Article Text

Abstract
Objectives To explore population patterns of sex-based incidence and prevalence of peripheral arterial disease (PAD), guideline-directed best medical therapy prescriptions and its relationship with all-cause mortality at 1 year.
Design A retrospective cohort study.
Setting Anonymised electronic primary care from 787 practices in the UK, or approximately 6.2% of the UK population.
Participants All registered patients over 40 with a documented diagnosis of peripheral arterial disease.
Outcome measure Population incidence and prevalence of PAD by sex. Patterns of guideline-directed therapy, and correlation with all-cause mortality at 1 year (defined as death due to any outcome) in patients with and without an existing diagnosis of cardiovascular disease. Covariates included Charlson comorbidity, sex, age, body mass index, Townsend score of deprivation, smoking status, diabetes, hypertension, statin and antiplatelet prescription.
Results Sequential cross-sectional studies from 2010 to 2017 found annual PAD prevalence (12.7–14.3 vs 25.6 per 1000 in men) and incidence were lower in women (11.6–12.4 vs 22.7–26.8 per 10 000 person years in men). Cox proportional hazards models created for PAD patients with and without cardiovascular disease over one full year analysed 25 121 men and 13 480 women, finding that following adjustment for age, women were still less likely to be on a statin (OR 0.69; 95% CI 0.66 to 0.72; p<0.001) or antiplatelet (OR: 0.87; 95% CI 0.83 to 0.90; p<0.001). Once fully adjusted for guideline recommended medical therapy, all-cause mortality was similar between women and men (adjusted HR (aHR) 0.95, 95% CI 0.87 to 1.03, p=0.198 for all patients, aHR 1.01, 95% CI 0.88 to 1.16, p=0.860 for those with cardiovascular disease).
Conclusions Women with a new diagnosis of PAD were not prescribed guideline-directed therapy at the same rate as men. However once adjusted for factors including age, all-cause mortality in men and women was similar.
- peripheral vascular disease
- sex
- drug therapy
- epidemiology
- mortality
Data availability statement
The data that support the findings of this study are available from IQVIA Medical Research Data but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of IQVIA.
Data availability statement
No additional data available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A large primary care database.
Investigation of antiplatelet therapy as well as statin therapy.
Electronic patient records do not record why a patient is not on an antiplatelet or statin, for example, patient choice, poor compliance or a prescription error.
Use of prescriptions rates as is only a proxy for patients taking their prescribed medication, and not confirmation of patient adherence.
Introduction
Peripheral arterial disease (PAD) affects the blood supply to the lower limbs. PAD is estimated to occur in 15%–20% of people over 70 and, together with diabetes mellitus, is the leading global cause of lower limb amputation.1 2 The scale of severity ranges from asymptomatic (found on screening or incidentally), pain on walking or tissue loss and pain at rest.3
The majority (90%) of patients diagnosed with PAD experience mild or no symptoms and are managed non-operatively.4 Even so, excess mortality associated with a diagnosis of PAD is similar to that of coronary heart disease and stroke, due not only to systemic cardiovascular disease but higher rates of lung disease and malignancy.5 6
In common with other cardiovascular conditions guideline-directed best practice recommendations,7 that is, prescribing an antiplatelet and statin, is associated with reduced risk for all-cause mortality, myocardial infarction and stroke in the PAD cohort.8 There is now a large volume of evidence showing fewer women at risk of cardiovascular events are prescribed these medications, especially statins.9 At the same time studies have confirmed that statins are equally as effective at reducing all-cause mortality in women and men.
Prospective studies and registry data have documented significantly poorer clinical outcomes in women being treated for symptomatic arterial disease such as acute stroke, heart attack, critical limb ischaemia and ruptured abdominal aortic aneurysm, with hypotheses citing older age at presentation, and less care provided in the years prior to needing surgery.10–12
This study was designed to provide: Estimates for the annual incidence and prevalence of PAD, annual incidence of all-cause mortality in patients with a diagnosis of PAD and the correlation of implementation of best practice (antiplatelet and statin prescriptions) using proxy measures, in patients with a new diagnosis of PAD, with adjusted risk of all-cause mortality at 1 year (all-cause mortality was used to ensure all causes of death associated with a diagnosis of PAD including malignancy and respiratory disorders were accounted for).6
Methods
We performed a retrospective analysis of a prospective primary care database using IQVIA Medical Research Data (IMRD), after identifying all patients over 40 with a documented diagnosis of PAD. This used data from The Health Improvement Network (THIN). Reference made to THIN is descriptive of the data asset licensed by IQVIA.13 IMRD database contains anonymised electronic health records contributed by 787 practices in the UK using Vision software. Approximately 6.2% of the UK population is covered by IMRD.14 IMRD contains data on patient demographics, lifestyle characteristics, medical diagnoses and prescriptions.
Practice eligibility criteria and quality assurance
Acceptable mortality reporting (AMR) is a quality assurance standard that ensures consistent recording of data in practices.15 To ensure reporting of quality data and to allow sufficient time for the recording of valuable patient information, practices qualified for inclusion from the later of the dates on which the practice achieved AMR reporting and a year after the practice employed the use of the Vision software system.
Annual incidence and prevalence of PAD
Estimates of incidence and prevalence of PAD were calculated for participants over the age of 40 (no upper age limit) registered with an eligible practice for more than a year before study entry (to ensure recording of all the important baseline covariates) and a documented diagnosis of PAD. Sequential cross-sectional studies were performed on 1 January each calendar year from 2010 to 2017 to calculate the annual prevalence of PAD and estimate incidence rates of PAD per 10 000 person-years.
Retrospective cohort study of factors associated with 1-year mortality
Participants aged 40 years and above with an incident diagnosis of PAD were included in the study. The study period was 1 January 2016 to 31 December 2016. Participants with a diagnosis of PAD were identified on 1 January 2016.
Exposure
PAD was assumed to be documented in a patient’s primary care record following one of the following: recorded reduced ankle-brachial pressure index, previous intervention for PAD, documented diagnosis following review of the patient or imaging by a vascular surgeon.
Individuals with a diagnosis of PAD (exposure) were identified using the relevant diagnostic Read codes (V.2). The Read clinical thesaurus is composed of hierarchically organised alphanumeric codes that describe a health-related concept.16 Read codes are a mechanism used by general practices in the UK for the recording of health-related information, including those practices involved in the THIN database. The relevant codes lists used in the present study were identified in the Read code thesaurus using the following key steps: (a) creation of a list of pertinent search terms; (b) a search of the Read code dictionary for relevant codes using the list of search terms; (c) a search of applicable additional codes from codes lists published in online Read codes repositories, or supplemental information of published research17; (d) rating each code in the list for relevance and deciding on the final set by consulting clinical experts (general practitioners and consultant specialists). A complete list of Read codes used in the study are included in the supplementary material (Read codes_online supplemental table 1).
Supplemental material
Outcome
All-cause mortality was defined as death due to any outcome. Mortality and date of death is reliably recorded in IMRD database and have been validated in previous studies.18 19 The 1 of January 2016 served as the index date. Exposed participants were followed from the index date to the exit date. The exit date was the earliest of (i) the outcome (1-year all-cause mortality), (ii) study end date, (iii) date of leaving the general practice or when the practice ceased contributing to the database.
Study covariates
The cohort was interrogated with specific reference to codes for comorbidity using the Charlson Comorbidity Index (CCI; scores are provided for varying severity of cardiovascular disease, dementia, chronic lung disease, liver disease, diabetes, renal disease, malignancy), sex, age at index diagnosis, body mass index (BMI), deprivation index (Townsend quintile), smoking, ethnicity, statins, antiplatelets, diabetes (insulin and non-insulin dependent combined), hypertension and existing diagnosis of cardiovascular conditions (cerebrovascular accidents, ischaemic heart disease, heart failure).
The most recently recorded variable prior to study entry was used. BMI in kg/m2 was categorised as underweight, normal, overweight obese or missing. Smoking status (self-reported) was categorised as never smoked, current smoker, ex-smoker or missing. Current users of a statin or an antiplatelet (clopidogrel or aspirin) were defined as those with an active prescription for the last 90 days prior to cohort entry.
Statistical analysis
Prevalence estimates were used to map PAD and all-cause mortality in the years prior to the study. The proportion of eligible participants with any record ever of PAD was calculated on 1 January each year from 2010 to 2017. Annual crude incident rates (overall and by sex) for PAD were calculated by dividing the number of newly diagnosed patients with PAD (numerator) by the total number of person-years at risk (denominator) for the given year. The crude incident rates for all-cause mortality in PAD (overall and by sex) were calculated by dividing the number of newly recorded deaths from any cause in patients with PAD (numerator) by the total number of person-years at risk (denominator) for the given year.
Cox proportional hazards models were used to estimate the HR and the corresponding 95% CIs of 1-year mortality among women with PAD compared with men with PAD. In the multivariable models, adjustments were made for Charlson comorbidity, sex, age, BMI, Townsend score of deprivation, smoking status, diabetes (insulin dependent and independent), hypertension, statin and antiplatelet prescriptions. Two separate models were created: (i) a model for participants with pre-existing cardiovascular disease (ischaemic heart disease, cerebrovascular accidents and heart failure) and a diagnosis of incident PAD; (ii) a model for participants without documented pre-existing cardiovascular disease, with an incident diagnosis of PAD.
Missing data
For categorical variables we created a separate category, ‘missing’, which was then included in the analysis. Numbers for missing data have been included in the tables.
Patient and public involvement
No patients were directly involved in the design of this study.
Results
Temporal trends in PAD incidence and prevalence, and all-cause mortality
There was a plateau in the annual prevalence of PAD between 2010 and 2017 (figure 1). The annual incidence decreased from 19.4 per 10 000 person-years in 2010 to 17.0 per 10 000 person years in 2017. During this period, the annual prevalence and incidence remained lower in women. In fact, among women, the prevalence of PAD decreased from 14.3 per 1000 in 2010 to 12.7 per 1000 in 2017 while remaining stable among men (25.4 per 1000 and 25.6 per 1000 in 2010 and 2017, respectively). Incidence of PAD diagnosis has declined over time in women (12.4 per 10 000 person-years to 11.6 per 10 000 years) and men (26.8 to 22.7 per 10 000).
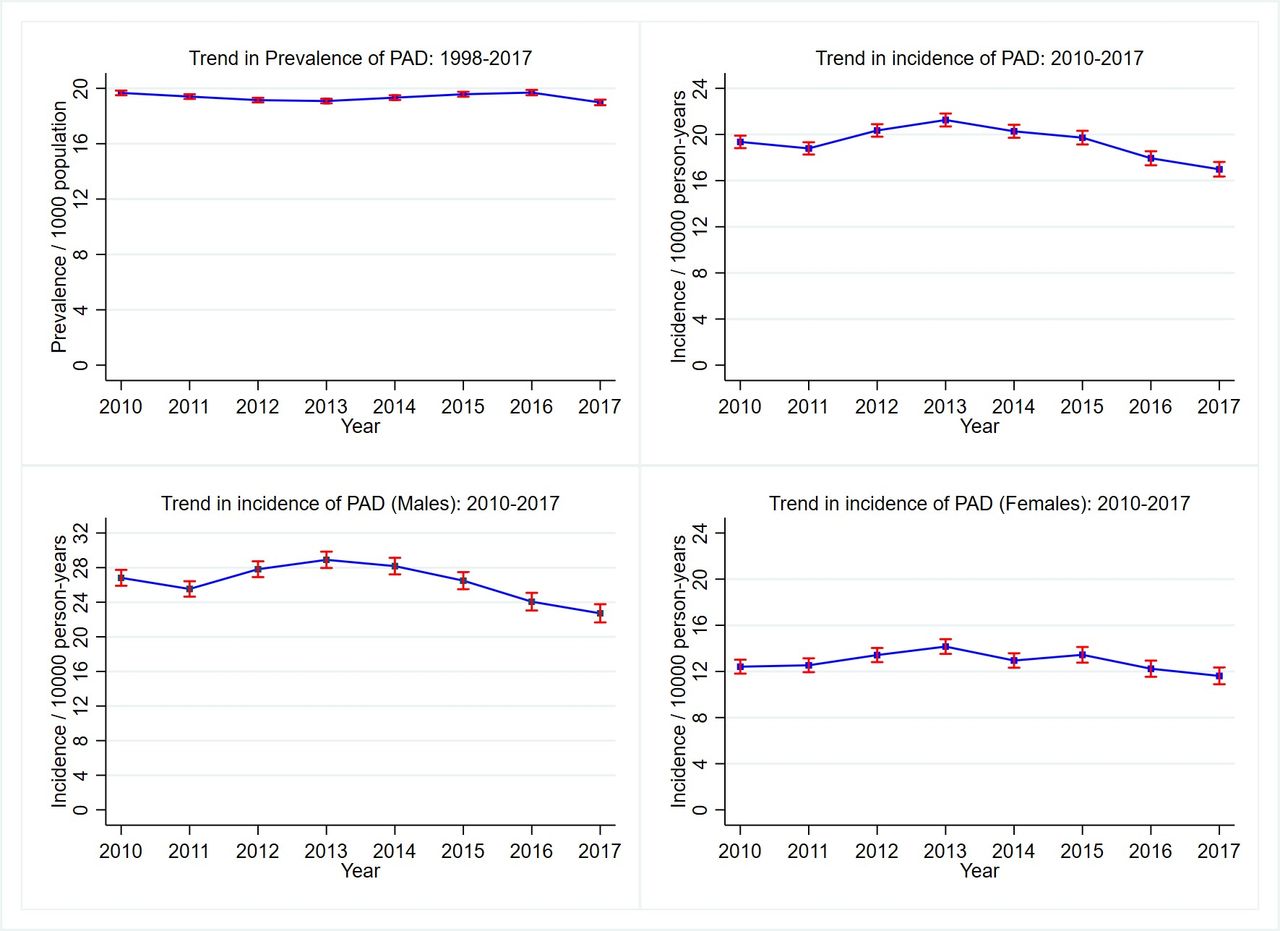
The changing prevalence and incidence of pad among UK adults aged 40 years and over, 2010–2017: sequential cross-sectional studies were performed on 1 January each calendar year from 2010 to 2017 to calculate the annual prevalence of PAD. Prevalence has remained relatively steady, whereas incidence has dropped. This appears to be accounted for by a drop in incidence in men over the study period, compared with women in which annual incidence has remained stable. PAD, peripheral arterial disease.
Between 2010 and 2017, all-cause mortality in patients with PAD remained stable at 7432.2 per 100 000 person-years in 2010 and 7273.3 per 100 000 person-years in 2017. Rates have been increasing in women, but decreasing in men (figure 2, online supplemental table 2).
Supplemental material

The annual incidence of all-cause mortality in patients with a diagnosis of PAD among UK adults aged 40 years and over between 2010 and 2017: sequential cross-sectional studies were performed on 1 January each calendar year from 2010 to 2017 to calculate the annual prevalence of PAD. Incidence has remained steady despite improvements in treatments and advances in evidence for early implementation of guideline-based therapy. PAD, peripheral arterial disease.
Cohort study
The analysis included 24 963 men and 13 343 women with a documented diagnosis of PAD in their primary care notes. Table 1 summarises the baseline demographic, lifestyle, surgical and medical characteristics of all study participants. Overall, baseline characteristics between men and women with PAD were similar. However, women were more likely to be slightly older at the time of diagnosis, with a median age of 76 years (IQR 67–83) compared with men at a median age of 73 years (IQR 66–80). Women were more likely to live in areas of greatest deprivation (16.2% vs 15.1%), be classified as severely obese (class 2/3 obesity, 10% vs 7.8%) or hypertensive (64.3% vs 59.9%).
Baseline cohort characteristics by sex for all patients ≥40 years old diagnosed with peripheral arterial disease (PAD) within the study time period, and those with an existing diagnosis of cardiovascular disease (CVD), defined as ischaemic heart disease, stroke or heart failure
Best medical therapy
Crude sex-based comparisons found fewer women were prescribed a statin or antiplatelet (table 1). Anticoagulation (warfarin or direct oral anticoagulant) was also prescribed less often in women. Even following adjustment for age, at risk women were still less likely to have a documented prescription for antiplatelets (OR 0.87, 95% CI 0.83 to 0.90, p<0.001) or statin (OR 0.69, 95% CI 0.66 to 0.72, p<0.001) than their male counterparts.
All-cause mortality at 1 year
Table 2 shows crude and adjusted models for 1-year mortality. Crude modelling suggested an increased risk of mortality in women in comparison to men (HR 1.16; 95% CI 1.07 to 1.26; p<0.001). However, this difference disappeared when adjusted for age (adjusted HR (aHR) 0.95; 95% CI 0.88 to 1.03; p=0.215). Once adjusted for all covariates sex itself was not associated with an increased risk of all-cause mortality (aHR 0.95; 95% CI 0.87 to 1.03; p=0.198).
Events, that is, deaths from any cause during study period by percentage, person-years and crude rate per 1000 person-years in patients aged >40 years old with a diagnosis of PAD, and those with diagnosis of PAD and CVD. Modelling was performed for sex and age, followed by model adjusted for Charlson comorbidity, sex, age, body mass index, Townsend score of deprivation, smoking status, diabetes, hypertension, statin and antiplatelet prescription
PAD without cardiovascular disease
In patients with a diagnosis of PAD but no record of cardiovascular disease (CVD), all-cause mortality was associated with a CCI of ≥2, older age, BMI <18.5, greater deprivation (Townsend quintile 4/5) and being a current or ex-smoker. An active prescription for a statin was also associated with survival at 1 year (aHR 0.70, 0.84–1.03; p<0.001). An antiplatelet prescription was associated with greater odds of survival but did not reach statistical significance (aHR 0.92; 95% CI 0.83 to 1.03; p=0.161) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Factors associated with all-cause mortality in all patients with a diagnosis of PAD and in patients with PAD and an existing diagnosis of cardiovascular disease: COX proportional hazards models were used to estimate the HR and corresponding 95% CIs of 1-year mortality using two separate models: (i) a model for participants with pre-existing cardiovascular disease (ischaemic heart disease, cerebrovascular accidents and heart failure) and a diagnosis of incident pad; (II) a model for participants without documented pre-existing cardiovascular disease, with an incident diagnosis of PAD. variable protective for 1 year mortality were similar between the two groups. BMI, body mass index; CVD, cardiovascular disease; PAD, peripheral arterial disease.
PAD with CVD
In this subgroup, active statin and antiplatelet prescriptions were both associated with protection from mortality at 1 year (HR 0.68, 0.59–0.78, p=>0.01), (HR 0.76, 0.67–0.86, p≤0.01). Increased risk was associated with a CCI score of ≥2, a BMI <18.5 and being a current or ex-smokers. Sex was not associated with a difference in all-cause mortality.
Discussion
The IMRD database includes a large number of UK general practice patients and is generalisable to the UK population, therefore it has been used here to extrapolate findings to the rest of the UK. We have focused on all-cause mortality rather than cardiovascular mortality alone, to ensure that other causes of mortality known to occur at higher rates in this cohort such as malignancy, respiratory and psychiatric conditions have been included.6 We have also included evaluation of antiplatelet prescriptions, rather than statins alone, as both are key components of best medical therapy recommended in this cohort.
Randomised trials have already documented poorer adherence to medical therapies in women who have progressed to vascular surgery compared with men.20 21 This study has aimed to add to this by addressing the significant number of patients that do not proceed to surgical intervention. In those patients, the purpose of an antiplatelet and statin is the prevention of cardiovascular events and death. At least 85% of the cohort studied here will not undergo intervention for their PAD. Therefore, risk prevention is the mainstay of their management.
Although the data found that best medical therapy was associated with a survival advantage in patients at greatest risk (PAD and CVD), we have failed to show that women who did not have an active prescription at the time of the study were at any higher risk of all-cause mortality than their matched male counterparts. At the same time, the data show that regardless of outcomes, sex-based disparities in medical optimisation begin in primary care, making it a target for intervention to improve outcomes in the PAD population.
It must be noted that rates of guideline directed therapy in both men and women remain well below those we might hope for, despite them being at equal or higher risk of major cardiovascular events and death than those suffering from CVD alone.5 These patients have repeatedly been shown to be undertreated compared with their counterparts with other forms of CVD.22 A recent evaluation of initiation of recommended medical management for patients with PAD undergoing intervention in hospital demonstrated poor uptake of guideline recommendations such as measuring lipid levels and prescriptions of adequate medical therapy. The same study estimated that by optimising treatment for men and women, an absolute reduction for 10-year cardiovascular risk of 29% could be achieved.23 Community based studies of statin prescriptions using the same IMRD/THIN database found that even following high risk scoring only 50% of eligible patients went on to receive a prescription for a statin in primary care.14
Study limitations
Electronic patient records do not allow analysis of decision-making processes, for example why a patient is not on an antiplatelet or statin ie, patient choice, poor compliance or uncorrected administrative prescription error. This will be the focus of future assessments. We have attempted to account for prescribing confounders linked to survival in other vascular diseases (such as beta blockade) by performing a separate analysis for patients with CVD and cerebrovascular disease. We accept this cannot be completely accounted for. We have not identified the severity of PAD, or linked that to mortality directly. Although severity scores are available, they are not routinely documented in primary care. A key limitation in the guidelines is the lack of reference to alternative lipid lowering therapies. In this cohort, the number of patients on alternatives to statins was very small, but a larger study will be able to address this in the future. Finally, we have used prescription rates as a proxy for patients taking their prescribed medication but can only say that the patient filled at least one 3-month prescription in the year being studied. We cannot comment on actual patient adherence.
Conclusion
There are significant differences in prescribing practices for men and women with PAD in primary care. Research into the best ways of promoting best medical therapy in the whole community must be a priority to reduce the burden of all-cause mortality in this high-risk group.
Data availability statement
The data that support the findings of this study are available from IQVIA Medical Research Data but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of IQVIA.
Data availability statement
No additional data available.
Ethics statements
Patient consent for publication
Ethics approval
Use of IMRD is approved by the UK Research Ethics Committee (reference number: 18/LO/0441); in accordance with this approval, the study protocol was reviewed and approved by an independent Scientific Review Committee (SRC) (reference numbers: 17THIN061 and 17THIN062). IMRD incorporates data from The Health Improvement Network (THIN), A Cegedim Database. Reference made to THIN is intended to be descriptive of the data asset licensed by IQVIA. This work used de-identified data provided by patients as a part of their routine primary care.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
KN and DSL are joint senior authors.
Contributors RB: Study concept, study design, manuscript writing and final approval of the manuscript. KO: Analysis and contribution to manuscript. DK: Data extraction. KG: Data extraction. NA: Analysis and manuscript. KN: Study design and final approval of the manuscript, and study guarantor. DSL: Study design and final approval of the manuscript.
Funding The funding for this research was provided by the University of Birmingham research development fund (RB, award number NA). The authors of the study are supported by various grants from the National Institute for Health Research (NIHR) Applied Research Collaboration (ARC) West Midlands (award numbers NA). The views expressed here are those of the authors alone.
Disclaimer The authors have no disclosures or competing interests to declare.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.