Article Text

Abstract
Objectives To examine how drug shop clients’ expenditures are affected by subsidies for malaria diagnostic testing and for malaria treatment, and also to examine how expenditures vary by clients’ malaria test result and by the number of medications they purchased.
Design Secondary cross-sectional analysis of survey responses from a randomised controlled trial.
Setting The study was conducted in twelve private drug shops in Western Kenya.
Participants We surveyed 836 clients who visited the drug shops between March 2018 and October 2019 for a malaria-like illness. This included children >1 year of age if they were physically present and accompanied by a parent or legal guardian.
Interventions Subsidies for malaria diagnostic testing and for malaria treatment (conditional on a positive malaria test result).
Primary and secondary outcome measures Expenditures at the drug shop in Kenya shillings (Ksh).
Results Clients who were randomised to a 50% subsidy for malaria rapid diagnostic tests (RDTs) spent approximately Ksh23 less than those who were randomised to no RDT subsidy (95% CI (−34.6 to −10.7), p=0.002), which corresponds approximately to the value of the subsidy (Ksh20). However, clients randomised to receive free treatment (artemisinin combination therapies (ACTs)) if they tested positive for malaria had similar spending levels as those randomised to a 67% ACT subsidy conditional on a positive test. Expenditures were also similar by test result, however, those who tested positive for malaria bought more medications than those who tested negative for malaria while spending approximately Ksh15 less per medication (95% CI (−34.7 to 3.6), p=0.102).
Conclusions Our results suggest that subsidies for diagnostic health products may result in larger household savings than subsidies on curative health products. A better understanding of how people adjust their behaviours and expenditures in response to subsidies could improve the design and implementation of subsidies for health products.
Trial registration number NCT03810014.
- health economics
- infectious diseases
- quality in health care
Data availability statement
De-identified data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
Subsidies for malaria testing and treatment were randomly assigned to clients, thus increasing confidence that we are identifying their causal impact on expenditures.
Drug shop expenditures were collected during exit interviews minimising the risk of recall bias
Test results and medication purchases were not randomly assigned, thus their impacts cannot be interpreted causally
The study was conducted in only 12 drugs shops in one part of Western Kenya, focusing specifically on malaria; this affects the generalisability of the results.
Introduction
In many low-income and middle-income countries, people continue to suffer high morbidity and mortality from diseases such as malaria, diarrhoea, pneumonia and HIV that are both preventable and treatable.1 In 2021, there were 241 million cases of malaria and 627 000 deaths, primarily in sub-Saharan Africa.2 Diarrhoea is responsible for approximately 1.5 million deaths, while lower respiratory infections such as pneumonia are responsible for 489 million cases and 2.49 million deaths.3
The treatment of these illnesses can place substantial financial burdens on poorer households.4–11 These costs to patients can include both indirect costs such as productivity losses and direct costs such as those related to prevention, diagnosis and treatment.6 11 A significant proportion of the direct costs of treatment are from spending on medications.5 10 12 For example, the recommended first-line treatment for malaria, a class of medications known as artemisinin combination therapies (ACTs), is more expensive compared with older, less effective malaria treatments.13 While ACTs are generally available for free or at heavily subsidised prices at public health facilities, they are more expensive at private drug shops where many people first seek care for malaria.13–15 Overall, studies have found that households in sub-Saharan Africa spend between US$0.23 and US$36.56 per episode of malaria (2016 US dollars) in direct costs, comprising medications, consultation, diagnostics and hospitalisation and indirect costs for transportation.7 Direct costs of malaria in Africa are estimated to be 12 billion US dollars per year worldwide.16
Subsidies can help make medications more affordable and accessible.17 Previous studies have shown that subsidies increase uptake of health products, such as insecticide-treated bed-nets to prevent malaria,18 19 water treatment solutions for diarrhoea-prevention20 and HIV self-testing.21 However, subsidies for health products also raise concerns about whether the product will be used or used appropriately, and whether the subsidised price may anchor people’s price expectations thus hampering future uptake of unsubsidised products.17 22 23
In the case of malaria, the goal of increasing the availability and affordability of ACTs, particularly in the private retail sector where many people first seek care for malaria, led to the Global Fund’s Affordable Medicines Facility for malaria (AMFm) pilot programme.24 25 The programme negotiated reduced prices for ACTs from manufacturers and subsidised the cost of the medication for first-line buyers in seven African countries. Although successful in increasing both the availability and use of ACTs,26–28 the pilot—and its successor, the Private Sector Co-Payment Mechanism—raised concerns that highly subsidised ACTs could result in inappropriate use of the medication by those who do not have malaria.29 This in turn could result in delays in appropriate management of the illness, wastage of valuable medications or subsidy funds, and spread of drug resistance.30 31 Indeed, studies have documented that both clinicians and patients engage in presumptive malaria treatment of fevers as well as treatment of non-malarial fevers with antimalarial treatments.32 33 As a result, research has focused on combinations of subsidies for malaria testing and treatment to induce appropriate use of health products, while also making treatment more affordable29 34 35
While this previous work concentrated on how subsidies affect individuals’ testing and treatment behaviour, less is known about how these behavioural changes affect people’s expenditures at the drug shop. This is important for a more comprehensive understanding of the impact of subsidies on households. In this study, we examine how malaria testing and treatment subsidies affect drug shop clients’ expenditures. We also explore the relationship between malaria test results and number of medications purchased on client expenditures. We aimed to test the following hypotheses: (1) Clients randomly assigned to receive subsidies for malaria testing and malaria treatment will spend less at the drug shop than clients randomly assigned to not receive these subsidies; (2) Clients testing positive for malaria will have lower expenditures than clients testing negative for malaria, as a positive test result reduces uncertainty about the disease diagnosis and (3) Each additional medication purchased will be associated with higher client expenditures. The results of this study have implications for the design of future interventions that rely on subsidies to increase uptake and appropriate use of health products.
Methods
Study context
We used data from a survey conducted with 836 clients visiting 12 drug shops in 2 subcounties of rural western Kenya. Both subcounties included in the study have a similar malaria burden, predominantly Plasmodium falciparum with perennial transmission. The study was conducted over 18 months between 28 March 2018 and 30 October 2019, capturing the different malaria transmission seasons in the region. The survey was conducted as part of a randomised controlled trial designed to assess the impact of conditional ACT subsidies and subsidies for malaria rapid diagnostic tests (RDTs) on uptake of malaria testing and on the targeting of ACTs, described in more detail elsewhere.36
At the time of the study, malaria diagnostic testing was primarily available at formal health facilities. However, many individuals in Kenya seek treatment from the private retail sector : a 2016 ACT watch survey showed that 70.6% of all antimalarials in Kenya were distributed through the private sector, with 37% being through unregistered pharmacies. In these venues, RDT availability is limited—at the time, it was 16% and 9.5% in registered and unregistered retail outlets, respectively.13 The ACT watch survey also found that median RDT price in the private sector was US$1.00 and median ACT cost for an adult dose was US$1.31. Price data were collected in Kenya shillings and converted to US dollars based on official exchange rates during the data collection period (June-August 2016).13 The ACT prices likely reflect continued government subsidies through the Co-payment Mechanism which, following AMFm, allowed countries to set their own subsidy levels (in Kenya, this was a 70% subsidy for all pack sizes).37
Sampling
The study population for this study included any individual visiting the outlet with a malaria-like illness on randomly selected days, including children >1 year of age up to 17 years if they were physically present and accompanied by a parent or legal guardian. The client was defined as the sick individual if they were 18 years or older, or as the parent/legal guardian of the sick individual if the latter was under the age of 18.
Randomisation
Potential participants were approached by a research assistant posted at the shop and invited to participate in the study. Participants were randomised to one of four study arms, following a 2×2 factorial design, each with a different combination of two different RDT prices and two different subsidised ACT prices (conditional on a positive test result). The ACT subsidy was for artemether lumefantrine (AL), the type of ACT most sold in Kenya. Participants were offered a scratch card with masked arm assignment, which randomised them to one of four study arms. The target sample size for the study was 832 participants, which provided at least 80% power to detect each of the anticipated effect sizes for the main outcome of RDT uptake.36
Intervention
The consumer RDT price was either Ksh20 (50% subsidy) or Ksh40 (no subsidy) while the AL was either free (100% subsidy) or between Ksh10 and Ksh40 (67% subsidy) depending on whether the sick individual was a child or adult. At the time of the study, the exchange rate was approximately US$1=Ksh100. No AL discount was offered for individuals with a negative test or those without a test. If the client chose to be tested, the RDT was performed by the research assistant who presented and explained the result to the client. If the sick individual tested positive, they could show their RDT cassette and scratch card to the shopkeeper for an AL discount according to their arm assignment.
Data
Clients were surveyed at two points during their drug shop visit. They were first surveyed before they entered the drug shop to collect demographic and household information on the sick individual and the client (if they were responding on behalf of a minor participant), information about the illness, including any treatment actions that had already been taken, and the clients’ plans for what medication(s) they were going to buy and how much they expected to spend. Clients were then randomly assigned to one of four study arms. If they chose to get tested, the RDT result was also recorded by the research assistant. The client then completed their transaction at the drug shop. As the client was exiting the drug shop, they were once again surveyed to ask about what medication(s) they chose to purchase for the malaria-like illness (the interviewer also asked to see the packages to verify), and how much they spent at the shop. Additional details about the study design, including sample size calculations and the number of potential clients approached, randomised and analysed can be found in the paper describing the main study results.36
Dependent variable
Our main dependent variable was the client’s expenditure at the drug shop. We combined the amount that clients reported spending on drugs with the cost of the RDT if they chose to get tested. We either added the unsubsidised value of the RDT (Ksh40) or the subsidised value (Ksh20) depending on the arm to which they were randomly assigned.
Independent variables
Our independent variables included a dummy variable for whether the client was randomised to receive a free AL if they tested positive (relative to a 67% subsidised AL) and a dummy variable for whether they were randomised to receive a 50% subsidised RDT (we did not look at the interaction between the two subsidies as previous research showed no statistically significant interaction effect on RDT uptake36). We included interactions of each subsidy with a dummy variable for whether the client tested positive for malaria to examine variations in the effects of the subsidies by test result.
We used information on whether the client purchased any medications and the different types of medications they reported buying to construct a variable that captured the total number and types of medications they purchased (this included the free AL if they were eligible). We categorised the medications that they purchased as either AL, other antimalarials (eg, quinine, sulfadoxine pyrimethamine (SP), artemisinin injections), antibiotics (eg, amoxicillin co-trimoxazole, metronidazole), painkillers (for example diclofenac acetaminophen) and all other medications (which included cold and influenza medications and anti-histamines among others). These categories were precoded into the questionnaire and the interviewer could check off the appropriate boxes but there was also an ‘other’ category where the interviewer could write in the name of the medication. We went through these written-in medications to manually re-categorise some of the responses to one of the other categories, as appropriate.
In order to account for confounding due to demographic differences, we included, as control variables, the sick individual’s gender and age category, corresponding to the AL dosing categories (0–3 years, 4–8 years, 9–14 years and older than 14), the highest level of education completed by the client (less than primary, completed primary or completed secondary), household size and a dummy variable for whether the household was in the lower 40th percentile of the sample for wealth. The wealth index was calculated using polychoric principal component analysis based on the following household assets: water source, wall material, floor material, roof material, toilet type, cooking fuel type, cows, sheep, goats, pigs, donkeys, electricity, televisions, refrigerators, radios, mobile phones, motorcycles, cars/trucks and bank accounts.
Statistical analysis
We first conducted a descriptive analysis and present summary statistics on the sample in terms of proportions and means/medians. We then examined graphically the difference between what clients expected to spend at the drug shop and what they actually spent. Spending expectations were based on people’s response to the question ‘Approximately how much do you expect to spend?’ We graphed the difference between expected and actual expenditures for everyone, and separately by RDT result, using a kernel density plot.
We also graphically examined mean drug shop expenditures (and 95% CIs) by clients’ AL subsidy randomisation (free AL vs 67% subsidised AL if they tested positive), their RDT subsidy randomisation (50% subsidy vs no subsidy) and, among those who chose to get tested, their malaria RDT result (positive vs negative).
We then performed ordinary least squares regression analysis to understand (1) how AL and RDT subsidies, interacted with RDT results, were associated with drug shop expenditures and (2) how medication purchases were associated with expenditures, and whether the relationship varied by the sick individuals’ RDT result. We adjusted our standard errors for clustering by drug shop outlet using STATA’s ‘cluster’ command. For these regression analyses, our sample only includes clients who chose to get an RDT (818 clients, or 98% of the sample chose to purchase the RDT). To simplify interpretation, we present the results of these regressions in terms of linear predicted values and marginal effects (with 95% CIs) using the ‘margins’ command in STATA. Missing values were addressed using listwise deletion.
To better understand the relationship between medication purchases and client expenditures, we used a kernel density plot to examine expenditures by the number of medications purchased and mean expenditures by those who purchased two or fewer medication vs those who purchased three or more drugs. Both these analyses were separated out by the sick individuals' RDT result and were limited to individuals in the highest AL dosing category (older than 14) to keep AL drug costs consistent across the sample. All analyses were conducted using STATA V.15.1.38
Patient and public involvement
The patients or the public were not involved in the design, or conduct, or reporting of the study.
Results
Sample characteristics
Table 1 presents demographic characteristics of the 836 sick individuals, as well as summary statistics on the client responding to the survey (who was also the sick individual in N=589 (70%) of cases and was the parent/legal guardian of a child younger than 18 in the remaining cases). Of those 836 sick individuals, 388 (47%) were female, and 607 (73%) were above the age of 14 (the highest AL dosage group). Most clients had at least a primary school education (N=677, 81%) and were most commonly self-employed (N=353, 42%) or farmers (N=184, 22%). While nearly everyone had piped water or obtained water from a protected source (N=807, 98%), very few people had access to an improved latrine (N=51, 6%).
Summary of study participants’ demographic characteristics and treatment behaviours (N=836)
In terms of malaria treatment behaviours, most clients said that they planned to buy whatever drug the pharmacist recommended (N=518, 62%), while only 161 (19%) clients planned to buy AL. Nearly all clients chose to purchase an RDT (N=818, 98%) and 174 of those (21%) tested positive for malaria. Overall, 203 (25%) clients purchased AL. Consistent with the randomisation, approximately half the clients were eligible for free AL if they tested positive for malaria, and half were eligible for the RDT subsidy.
Among the 533 clients who responded to the question of how much they expected to spend at the shop, the median amount given was Ksh100 or US$1 (this is approximately the cost of an unsubsidised ACT at a drug shop). The median amount people actually spent was Ksh110 (US$1.1) despite subsidies for RDTs and AL available to most clients. As shown in figure 1, of the 64% (533/836) of clients who had an expectation of how much they would spend, many (N=247, 47%) spent within Ksh50 of what they expected to spend, with similar results regardless of their RDT result.
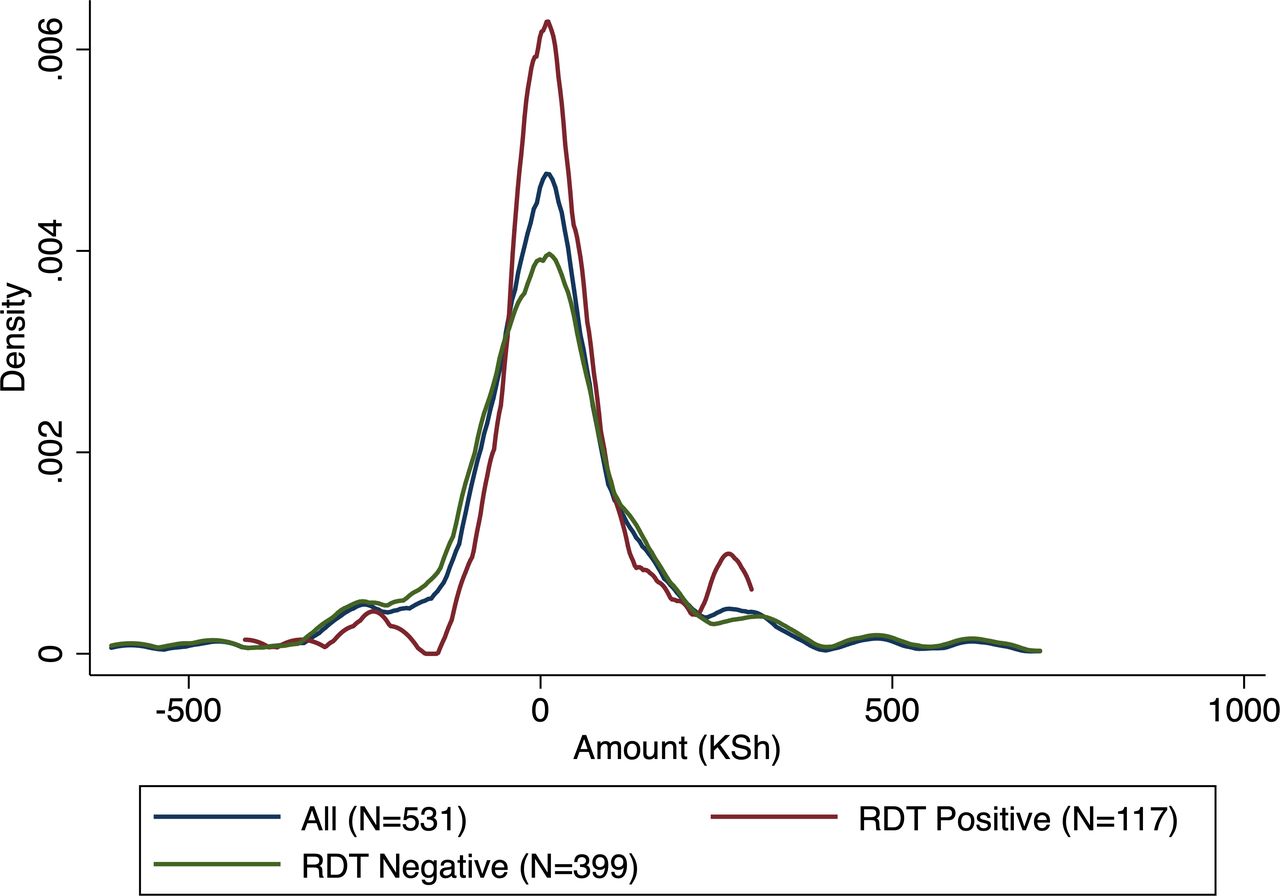
Difference between expected and actual expenditures (kernel density graph) by test result, for N=533 who reported an expected amount. N=303 people said that they ‘didn’t know’ how much they expected to spend, 2 people had missing data on actual expenditures, 15 people were not tested. RDT, rapid diagnostic test.
Subsidies, test result and expenditures
Figure 2 shows mean spending at the drug shop by whether the client was randomised to receive free AL if they tested positive for malaria, vs a 67% subsidised AL (figure 2A), whether they were randomised to receive a 50% subsidised RDT versus an unsubsidised RDT (figure 2B) and by whether those who got tested had a positive or negative result (figure 2C). We find similar spending levels by AL randomisation and by RDT result. However, adjusting for our control variables, those who were randomised to receive the subsidised RDT spent approximately Ksh23 less than those randomised to the unsubsidised RDT (95% CI (−34.6 to -10.7), p=0.002) (online supplemental table S1, Panel B). The association between client expenditures and the subsidies as well as with the control variables is displayed in online supplemental table S2.
Supplemental material

Mean expenditures by AL subsidy randomisation (A), RDT subsidy randomisation (B) and RDT result (C). Error bars indicate 95% CIs. AL, artemether lumefantrine; RDT, rapid diagnostic test.
Effect of medication purchases on expenditures
Table 2 presents results from a linear regression that examines the association between expenditures and AL subsidies, RDT subsidies and medication purchases, and also how these associations vary by the sick individual’s test result. Once we adjust for the number of drugs purchased, as well as all our other control variables, those who tested positive for malaria spent approximately Ksh70 less than those who tested negative for malaria (95% CI (−93.7 to -46.2, p<0.001). As before, those who were randomised to receive the free AL did not have lower expenditures relative to those who were randomised to the 67% ACT subsidy, and this did not vary by test result. Moreover, the RDT subsidy was associated with lower expenditures with larger effects among those who tested negative for malaria (though the difference between those who tested positive, and those who negative was not statistically significant). We also find that the number of medications purchased was associated with higher expenditures, but clients who tested positive spent approximately Ksh15 less for each additional medication than those who tested negative for malaria (95% CI (−34.7 to 3.6), p=0.102). Our sample size for this analysis included only 805 of the 818 clients who were tested for malaria, as 10 people had missing values for wealth, one had a missing value for patient gender and two had missing values for number of medications purchased.
Association between subsidies and spending at drug shop by RDT result
As figure 3 shows, despite lower spending per medication, total expenditures for clients who tested positive were, on average, the same as for those who tested negative likely because those who tested positive generally bought more medications (median=2, (IQR=2-3)) than those who tested negative (median=1 (IQR=0–2)). Many of those who tested negative did not buy any medications (34%) while almost everyone (98%) who tested positive bought at least one medication (this includes the free AL among the clients who were eligible for one). Moreover, online supplemental figure S1 shows that for those who bought two or fewer medications (nearly 80% of clients), spending was similar, regardless of test result. It is only for clients who bought three or more medications where a positive test result was associated with lower spending.

{kind=link}
{kind=link}
{kind=link}
Total spending by the number of medications purchased, separated by test result. Vertical lines indicate the median number of medications purchased for those who tested negative (blue) and those who tested positive (red). Sample is limited to those who were eligible for the adult AL dose (older than 14 years). AL, artemether lumefantrine; RDT, rapid diagnostic test.
Discussion
We analysed predictors of spending for individuals seeking malaria treatment at drug shops in Western Kenya and found three main results. First, people spent approximately what they expected to spend, despite receiving large subsidies for malaria testing and treatment. There are several possible explanations for this, including the fact that the AL subsidies were only available to those who tested positive (approximately 21% of the study sample) and that most clients chose to also purchase an RDT which was likely an extra, unexpected expenditure. Moreover, our evidence shows that those who tested positive bought more medications, on average, than those who tested negative so any potential savings from the AL subsidies were likely negated by additional medication purchases. Our results are consistent with previous research suggesting that people might use reference points for purchasing decisions, but also that financial constraints likely limit the amount that they are willing to spend.1 23 39 40
Our second main result is that being randomised to receive a free AL (conditional on a positive RDT) did not lower expenditures relative to being randomised to receive a 67% conditional AL subsidy, even for individuals who tested positive for malaria. On the other hand, clients randomised to the RDT subsidy had lower expenditures by approximately the value of the subsidy. For the AL subsidy, since individuals who did not get the free AL were still eligible for a 67% subsidy if they tested positive for malaria, the difference in AL prices between the two groups was relatively small (though still on the order of Ksh20–Ksh40). Even though the larger subsidy did not save people money, ACT subsidies may still be needed to encourage patients with confirmed malaria to buy ACTs rather than cheaper, less effective, medications.
Our third main result is that the number of medications purchased was one of the strongest predictors of spending. Our finding that people who tested positive bought more medications than those who tested negative, and that actual spending was close to people’s spending expectations, suggests that people may adjust the number of medications they buy to keep their out-of-pocket costs close to what they expected to pay. For example, those who tested positive may have bought more medications than they had planned because they now received an AL subsidy, whereas those who tested negative may have bought fewer medications to account for the additional cost of the RDT purchase. This is contrary to what we might expect from a fever management perspective since having a positive diagnosis should reduce uncertainty about which medications might be needed to treat the illness (online supplemental table S2 summarises the different medications purchased by clients, separated by RDT result).
This study has several implications for subsidy design. First, our results suggest that while subsidies may help direct behaviour, they may not necessarily save people money especially if consumers change their spending patterns to account for savings. Second, our findings suggest that subsidies need to take into account how much people expect to spend particularly if people are being encouraged to buy things that they were not planning to otherwise. Lastly, our results suggest that subsidies may be more likely to save people money if they are not conditional on other factors. For example, subsidising RDTs saved people money regardless of their malaria status, resulting in lower expenditures among those who received the subsidy, whereas the free AL only benefitted those who tested positive for malaria. Thus, subsidies on preventive and diagnostic health products, which can be used by everyone, may be more widely beneficial than subsidies on curative health products, particularly since there is evidence that people are very sensitive to prices for preventive health products.17 29 40
There are some limitations to this study. We do not capture indirect expenditures (eg, spending on transport) which may be an important component of illness expenditures.6 11 Second, spending expectations were missing for a large percentage of sample (N=303, 36%) who simply said ‘I don’t know’ when asked how much they expected to spend. Third, AL was heavily subsidised in all arms of the study, thus it is difficult to identify the effect of AL subsides on expenditures. We also did not directly ask people how the subsidies and test result affected their purchasing decisions—for example, whether it induced them to buy more or fewer medications. Lastly, this study was conducted in only 12 drugs shops in one part of Western Kenya, focusing specifically on testing and treatment for malaria, and this could affect the generalisability of the results.
Nonetheless, to our knowledge, this is one of the first studies to capture spending expectations and to examine how subsidies, test results and medication purchases together affect client expenditures at retail drug outlets. Our results suggest that there is not necessarily a straightforward relationship between subsidies and expenditure and that a better understanding between people’s expectations and their behaviour could improve the design of subsidies for health products.
Conclusion
We found that subsidies for testing had a statistically significant effect on expenditures while subsidies for malaria treatment that were conditional on a positive test result did not. There was also little difference in expenditures between those who tested positive compared with those who tested negative for malaria (despite subsidies for treatment available only to the former). Our results suggest that people may adjust their purchasing behaviour to keep their expenditures close to what they expected to spend at the drug shop.
Data availability statement
De-identified data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval for this study was given by Duke University (Pro00100425) and Moi University (IREC/2018/292). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors IS participated in the conceptualisation, design, analysis, interpretation, drafting and revision of the manuscript. JL participated in the design and interpretation of the manuscript. DM participated in the design, interpretation and revision of the manuscript. AW participated in the design and interpretation of the manuscript. TV participated in the design, interpretation, and revision of the manuscript. ELT participated in design, interpretation and revision of the manuscript. WPO'M participated in conceptualisation, design, interpretation and revision of the manuscript. IS is the guarantor of the content and accepts full responsibility for the finished work and/or the conduct of the study, had access to the data, and controlled the decision to publishAll authors approved the final manuscript.
Funding The original study on which the present article is based funded by the National Institute of Allergy and Infectious Diseases (R01AI141444).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.