Article Text

Abstract
Objectives To determine the pooled effectiveness and feasibility of telerehabilitation in patients with COVID-19.
Design Systematic review and meta-analysis of randomised controlled trials (RCTs).
Data sources PubMed, CINAHL, Science Direct, PEDro, Google Scholar and Cochrane Library databases were systematically searched to the end of March 2022.
Eligibility criteria and outcomes RCTs investigating the effects of telerehabilitation in the management of patients with COVID-19 were included. The outcomes of interest were functional capacity, cardiopulmonary exercise tests, quality of life and other variables where data are available.
Data extraction and synthesis Two reviewers screened, extracted data and performed methodological quality assessment independently. The revised Cochrane Risk of Bias tool was used to assess the risk of bias. Review Manager V.5.4 and Stata V.14.0 software were used for statistical analysis. Mean difference (MD) with 95% CI and the corresponding p value were used to determine the treatment effect between groups. A fixed-effect model was used for all variables as no significant heterogeneity was observed.
Results Four studies with 334 patients with COVID-19 were included. The pooled result of telerehabilitation showed statistically significant improvement on 6-minute walking test (MD 75.50; 95% CI 54.69 to 96.30; p=0.48), 30-second sit-to-stand test (MD 1.76; 95% CI 1.47 to 2.04; p=0.30), Borg Scale (MD 2.49; 95% CI 2.16 to 2.83; p=0.28) and level of dyspnoea (MD 6.26; 95% CI 5.42 to 7.10; p=0.66). The overall treatment completion rate was 88.46%, and the most common reason for withdrawal after randomisation was lost to follow-up or uncooperativeness.
Conclusions The findings showed that telerehabilitation interventions could improve functional capacity and exercise perception among patients affected by COVID-19 and can be implemented with a high completion rate and minimal adverse events. However, more studies are required to investigate the effects on cardiopulmonary function, quality of life, anxiety, depression and other variables.
PROSPERO registration number CRD42021287975.
- COVID-19
- REHABILITATION MEDICINE
- RESPIRATORY MEDICINE (see Thoracic Medicine)
- Telemedicine
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. All data generated or analyzed for this study are included in this published article and its supplementary information files.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
STRENGTHS AND LIMITATIONS OF THIS STUDY
This is the first systematic review and meta-analysis to investigate both the effectiveness and feasibility of telerehabilitation in patients with COVID-19.
Some studies might be missed due to language bias and limited database searching.
The number of studies and sample sizes included in this systematic review was limited and no subgroup analysis was performed.
Introduction
COVID-19 is a highly infectious respiratory disease, which can lead to respiratory, physical and psychological dysfunctions.1 2 COVID-19 has clinical manifestations of cough, shortness of breath, chest pain, fatigue and severe viral pneumonia with respiratory failure and/or death. Respiratory rehabilitation improves symptoms of dyspnoea, relieves anxiety, reduces complications, minimises disability, preserves function, and improves the quality of life both in the acute phase and after discharge.2–4 Telerehabilitation is the provision of rehabilitation services through telecommunication networks or the internet offering remote treatments to the people in their homes or from a distance.5 6 Since COVID-19 emerged and caused a huge burden on the health system, many patients are not able to receive their face-to-face treatments and also people with chronic or long-standing health conditions are unable to continue their follow-up as usual and professionals cannot attend all of the consultations. Moreover, the highly contagious nature of the disease forced searching for another treatment approach, that is, telerehabilitation to be used widely for the treatment of patients with COVID-19.6 7 Telerehabilitation can be provided with applications via chat or video calling, virtual reality, live talks, telephone, internet with or without supervision, and at hospital or health centre.6 8–11 Scientific literature has explored the effectiveness of these treatment approaches in different chronic pathologies like diabetes mellitus, chronic lung disease, multiple sclerosis, cardiovascular disease and respiratory conditions, such as chronic obstructive pulmonary disease (COPD) or cystic fibrosis.6 12
Respiratory telerehabilitation plays an important role in the recovery of patients from COVID-19. A randomised controlled trial (RCT) aimed to evaluate exercise capacity, lower limb muscle strength (LMS), pulmonary function, health-related quality of life (HRQOL), and dyspnoea found that remotely delivered rehabilitation improves functional exercise capacity, LMS, and physical HRQOL but no improvements reported in pulmonary function tests and mental aspect of quality of life.3 A systematic review on rehabilitation of patients in post-COVID-19 infection suggested that respiratory rehabilitation interventions improve pulmonary function, physical and psychological efficiency, and quality of life,13 but this study had limitations due to the lack of RCTs included in the review. Another systematic review was done to evaluate the impact of home-based telerehabilitation among community-dwelling elderly people reported an average 81%±11 intervention completion rate14 but it has limited evidence for home-based telerehabilitation. Another recent systematic review that examined the effects of pulmonary rehabilitation on patients post-COVID-19 reported an improved exercise capacity measured by 6-minute walking test (6MWT).15 However, this study lacks evidence on lung (pulmonary) function tests, level of dyspnoea and quality of life.
Since the occurrence of the pandemic, various studies have been published regarding the use of telerehabilitation in different pathologies including COVID-19. To the best of our knowledge, there is no systematic review that investigates the pooled efficacy and feasibility of telerehabilitation interventions in patients with COVID-19. Therefore, this study aimed to determine the pooled effectiveness and feasibility of telerehabilitation interventions in patients with COVID-19.
Methods and analysis
This systematic review and meta-analysis was reported according to the PRISMA (Preferred Reporting Item for Systematic Review and Meta-analysis)16 guidelines and has been registered at the International Prospective Register of Systematic Reviews with ID No. CRD42021287975. The protocol version for this systematic review was already published.17
Search strategy
PubMed, CINAHL, Science Direct, PEDro, Google Scholar and Cochrane Library database were searched, and articles published from the occurrence of the pandemic to the end of March 2022 were included. Search results of Cochrane Library were accessed from the original journals where articles were published. Multiple combinations of search terms determined by the Medical Subject Headings (MeSH), entry terms and keywords of COVID-19, telerehabilitation and efficacy and feasibility related words were used. In addition, manual search of the references of the included studies was conducted to identify additional studies. Two reviewers searched studies from each database independently, and any disagreement between them was resolved by a consensus or by a third reviewer. The detailed search strategy of PubMed using MeSH terms and entry terms was presented in table 1. The search strategy of other databases was presented in the online supplemental file 1.
Supplemental material
PubMed search strategy
Inclusion criteria
RCTs comparing telerehabilitation with any/no rehabilitation programme in patients with COVID-19 in the acute or long-term (follow-up) phase were included in this systematic review. Telerehabilitation is defined as any rehabilitation programme delivered by physiotherapy professionals via telecom/internet network services to patients with COVID-19. Telerehabilitation for COVID-19 might include aerobic training (such as walking, fast walking, jogging, swimming, etc); progressive strength training, secretion drainage or ventilatory techniques; aerobic, flexibility, and strengthening exercises for upper and lower extremities, and breathing/respiratory exercise; and other physical training programmes.8 9 18 Only studies in which interventions were delivered by a physiotherapy professional were considered. Studies focusing on patients having mild to moderate COVID-19 symptoms and confined in their home were included in the study. Studies that did not have enough statistical information to be extracted, descriptive reviews, guidelines, observational studies, systematic reviews, protocols, opinions, editorials, comments and conference abstracts were excluded. Two reviewers independently assessed the titles and abstracts, and only full-text published RCTs in the English language were included.
Outcome measures
The primary outcomes of interest were functional capacity (such as 6MWT), cardiopulmonary exercise tests (such as level of dyspnoea, pulmonary function test) and quality of life (such as Short Form-12, Short Form-36, EuroQol-5 Dimension). Secondary outcomes of interest were anxiety and depression scales, sleep quality, mortality rate and smoking cessation. Feasibility outcomes of interest were intervention completion rate, the reason for withdrawal, adverse events, service satisfaction and cost-effectiveness. Other potential contributing factors for feasibility like information communication technology (ICT) skill and experience, age and medical condition were also analysed where data are available.
Data extraction
Two reviewers independently extracted the data on a standard worksheet and disagreements were solved by a consensus or with the consult of a third reviewer. The detailed characteristics of the included studies and data related to the outcomes of interest were extracted. In studies where relevant data were missed or further explanation is needed, the corresponding author was contacted through email.
Methodological quality assessment
The risk of bias in the included studies was assessed using the Revised Cochrane Risk of Bias tool for RCTs.19 The reviewers reached concurrence on the final score of all the included studies. Two reviewers rated independently and a third reviewer addressed any discrepancy that arose.
Data analysis
Review Manager V.5.4 (Cochrane Collaboration) and Stata V.14.0 software were used to conduct the meta-analysis. Mean difference (MD) with 95% CI and the corresponding p value were used to determine the treatment effect between groups. Heterogeneity among included studies was assessed using the I2 test. First, a fixed-effect model was used for data analysis. When I2>0.5 or p<0.1, it is considered that there is significant heterogeneity among the included studies,2 20 and a random-effect model was used in this case. In this study, a fixed-effect model was used for all variables as no significant heterogeneity was observed.
Patient and public involvement
No patient or member of the public was involved.
Results
A systematic review and meta-analysis of RCTs targeting virtual rehabilitation for patients with COVID-19 was conducted. We have made some minor changes concerning the initially published protocol of this systematic review. We have searched CINAHL instead of Web of Science due to the lack of full access to some important papers. The PubMed search strategy was also redesigned to get more papers done in the area. The PRISMA search and selection process is shown in figure 1.

Preferred Reporting Item for Systematic Review and Meta-analysis flow chart. RCT, randomised controlled trial.
Characteristics of included studies
Systematic electronic and manual search identified 2601 potential studies, and 62 full-text articles were retrieved. Four RCTs with a total of 334 sample sizes met the inclusion criteria and were considered for the final systematic review and statistical analysis.21–24 The main characteristics of the included studies are summarised in table 2.
Characteristics of the included studies
Telerehabilitation
All four included studies focused on the effects of telerehabilitation interventions delivered by a physiotherapist. In all studies, patients with acute SARS-CoV-2 infection aged from 18 to 75 years were included. The interventions focused on breathing control, thoracic expansion, aerobic and LMS exercises for 6-week duration in one study21 and breathing exercises based on an active cycle of breathing technique for 1-week and 2-week duration in two studies.23 24 Specific resistance and strength tonic exercises for the 1-week duration were delivered in another study.22 One study had three arms (study groups), and we took data from the control group and breathing exercise group. The control groups received education in one study21 and no specified interventions in three studies.22 23 Follow-up data were assessed and reported in only one study after 28 weeks.21
Outcome evaluation
Functional capacity was evaluated using 6MWT and reported in four studies21–24 and using a 30-second sit-to-stand test (30STST) and reported in three studies.22–24 The quantitative assessment of fatigue was measured using the Visual Analogue Fatigue Scale in one study.23 Borg Scale (BS) that measures perceived exertion was reported in three studies.22–24 Cardiopulmonary function was evaluated and reported in three studies. The level of dyspnoea was measured using modified Medical Research Council (mMRC) dyspnoea in one study21 and using Multidimensional Dyspnoea-12 (MD12) in two studies.23 24 Only one study reported other cardiopulmonary function tests and quality of life (both Mental and Physical Components) scores.21 In our original protocol, we considered analysing more primary and secondary outcomes including feasibility. Unfortunately, the data we got from the included studies are limited, which leads to limitations in the analysis of the results and some deviations from the prior published protocol. The summary of outcome data of the included studies was presented in table 3.
Summary of outcomes
Methodological quality
The methodological quality of the included studies was assessed using the revised Cochrane Risk of Bias tool. Review authors’ judgements about each revised Cochrane Risk of Bias item were presented as a risk of bias graph (percentages across all included studies) in figure 2 and risk of bias summary for each included study in figure 3. In all studies, randomisation and blinding of the outcome assessor were adequate according to the review authors’ judgement. No study can fully blind the therapist and participants due to the nature of the study.

Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.

Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
Effect of interventions
Statistical analysis of the pooled treatment effects was reported in the forest plots for all outcome variables of available data. All four studies reported improvement of 6MWT following breathing exercises and non-specific tonic strength and resistance exercises delivered from 1-week to 6-week duration. As shown in the meta-analysis forest plot (figure 4), four studies with 230 COVID-19 cases reported the effect of telerehabilitation on 6MWT, and pooled results showed statistically significant improvement following telerehabilitation (MD 75.50; 95% CI 54.69 to 96.30; p=0.48). There was no considerable heterogeneity (Q=2.46, df=3, I2=0%) observed in the studies, and the result was generated using the fixed-effect model.
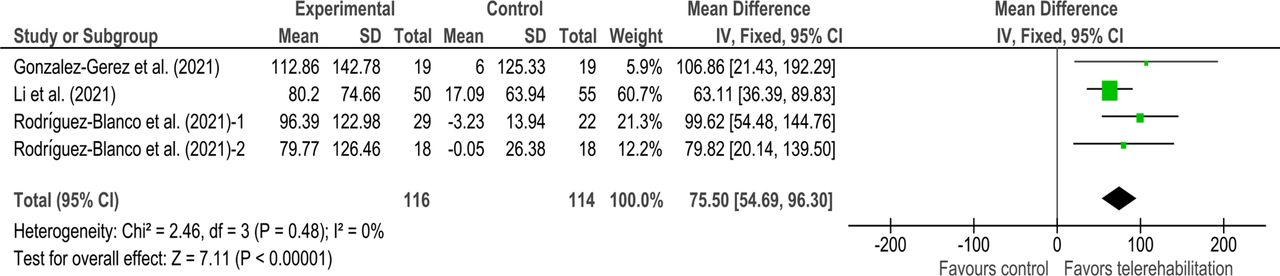
Forest plot showing the result of telerehabilitation versus control group for 6-minute walking test.
The 30STST was an effective, valid and reliable tool to assess peripheral muscle performance of lower limbs.25 Three studies with 125 cases reported that rehabilitation provided virtually was effective to improve 30STST. The forest plot (figure 5) showed the pooled effectiveness of telerehabilitation on 30STST was statistically significant (MD 1.76; 95% CI 1.47 to 2.04; p=0.30). Significant heterogeneity between studies was not observed (Q=2.4, df=2, I2=17%).

Forest plot showing the result of telerehabilitation versus control group for 30-second sit-to-stand test.
BS, which measures the entire range of activities that the individual perceives when exercising, was reported in three studies with 125 COVID-19 cases. The scores were multiplied by −1 because a higher score indicates a worse result on the test.23 26 BS was improved in all three studies after breathing exercises, specific tonic strength and resistance exercises delivered virtually. The pooled effectiveness (figure 6) was also significant (MD 2.49; 95% CI 2.16 to 2.83; p=0.28). No significant heterogeneity between studies was observed (Q=1.40, df=2, I2=22%).

Forest plot showing the result of telerehabilitation vs control group for Borg Scale.
Regarding cardiopulmonary function tests, one study reported the short-term effect of telerehabilitation on maximum voluntary ventilation and mMRC dyspnoea levels and reported no effects on forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC and peak expiratory flow pulmonary function parameters. Another two studies investigated only MD12 and found a significant effect after virtual breathing exercises. The pooled result (figure 7) was also significant (MD 6.26; 95% CI 5.42 to 7.10; p=0.66).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing the result of telerehabilitation versus control group for Multidimensional Dyspnoea-12.
Only one study reported data about quality of life (both Physical and Mental Components) using the HRQOL scale and found that pulmonary telerehabilitation was effective in improving only the physical component of quality of life. No outcome data are reported regarding our secondary outcomes of interest (such as anxiety, depression, sleep quality, mortality rate and smoking cessation) mentioned in the primary protocol.
Telerehabilitation feasibility
From a total of 334 enrolled cases, 45 (13.47%) were excluded for not meeting the inclusion criteria (21 cases), declining to participate (21 cases) and other unspecified reasons (3 cases). In all four studies, the median age of the participants ranges from 39±12 to 50.61±10.98 years and after randomisation, the overall intervention completion rate was 88.46%. From all four studies, three cases of hospitalisation due to worsening of the disease (all from the control group) and no serious adverse events like death were reported during the intervention period. Other factors that affect feasibility such as service satisfaction, cost, medical condition (comorbidity) and other variables were not reported in the individual studies.
Discussion
To our knowledge, this is the first systematic review and meta-analysis of RCTs focusing on the effectiveness and feasibility of telerehabilitation interventions among patients with COVID-19. A scoping review on telerehabilitation in participants with respiratory tract diseases, including COVID-19, by Taito et al included 23 studies where 22 of the included studies focused on stable COPD and received telerehabilitation at home; only one case series study focused on SARS-CoV-2 infection who received telerehabilitation at the hospital.27 Our systematic search identified only four full-text published RCTs implying that telerehabilitation is not well implemented for patients with COVID-19 and is in its infancy.
According to the present systematic review, telerehabilitation intervention programmes for patients with COVID-19 consist of mainly breathing exercises delivered at the home-based level. In the previous scoping review, aerobic exercises using a cycle ergometer or a treadmill, walking and muscle-strengthening exercises were the most used telerehabilitation programmes for respiratory tract infection.27 A recently published rapid review on the effectiveness of telerehabilitation in physical therapy included 53 systematic reviews, and cardiorespiratory rehabilitation was reported in 15 systematic reviews. The majority of conditions included were coronary artery disease, heart failure and COPD. The most common outcomes reported were related to clinical effectiveness as exercise capacity and HRQOL.28 In the present systematic review, the most common reported outcome was functional capacity measured by 6MWT and 30STST followed by cardiopulmonary function measured by the level of dyspnoea. It is uncovered that studies have faced limitations in assessing and reporting comprehensive outcome data which might be secondary to being virtual, and access to instrumental measurements might not be easy and possible.
The findings of this systematic review and meta-analysis showed that compared with education only or no rehabilitation, the telerehabilitation interventions showed better effects on COVID-19-infected patients’ physical function, exercise perception and level of dyspnoea with a high intervention completion rate. Although we could not obtain conclusive evidence of other outcomes due to limited relevant information, our findings suggest that telerehabilitation interventions could be an alternative strategy for the delivery of rehabilitation services for patients with COVID-19. A previous systematic review about telerehabilitation on various disease conditions reported better or at least similar outcomes than the comparative interventions with high attendance and patient satisfaction rates.29 Another systematic review on the effectiveness and feasibility of home-based telerehabilitation for older adults included six RCTs and reported 81%±11 average intervention completion rate. The study suggested that home-based telerehabilitation can be a strategy for rehabilitation service delivery with acceptable feasibility comparable with conventional rehabilitation for older adults.14 Telerehabilitation provides the advantage that the therapy can be delivered wherever is most convenient for the patient and the therapist can prescribe a variety of interventions and be able to get feedback through the use of modern digital technology. Another advantage of telerehabilitation is that patients can attend from their home or care centre, which in turn reduces the load as well as the number of healthcare providers involved than the actual face-to-face setup.
Feasibility
In the present systematic review, the overall intervention completion rate was 88.46% (87.21% in the intervention group and 89.76% in the control group). This result appears to be higher compared with the previously reported results on home-based telerehabilitation in older people (80%) and telerehabilitation intervention for respiratory tract diseases (70%).14 27 The possible explanation for this higher completion rate might be the age of participants, which is less than 50 years in this study. This high acceptance and implementation of telerehabilitation for COVID-19 pandemic indicates that virtual rehabilitation interventions might be playing a greater role in the future.
The present systematic review revealed that most of the reasons for withdrawal from the intervention were people who were lost to follow-up or uncooperativeness and worsening medical condition or hospitalisation. In contrast, there was less emphasis on reporting other aspects of feasibility such as the specific reasons for withdrawal, cost-effectiveness, service satisfaction, ICT skill and other potential factors. A qualitative research review aimed to identify the barriers and recommendations with telehealth services for healthcare delivery during the COVID-19 pandemic included 30 studies. Accordingly, the most encountered barriers to telerehabilitation were infrastructure and internet access (20%), data privacy and security (13.33%), digital literacy (13.33%), reimbursement and liability (10%), and clinician and patient unwillingness (6.67%).30 In the present systematic review, no data related to barriers to telerehabilitation were reported because studies were RCTs focusing on effectiveness only.
The results of this systematic review and meta-analysis should be interpreted in the context of its limitations. First, only short duration of telerehabilitation interventions (1–6 weeks) was reported. Therefore, the final results might not be generalised to all COVID-19 cases like ‘Long COVID-19’. Second, some important studies may have been missed from our systematic review due to language bias and accessibility issues. We have included only English-language studies. The Web of Science database was excluded and Cochrane Library database search results were retrieved from individual journals due to accessibility issues. Third, there are a number of published and unpublished (ongoing) RCT study protocols on telerehabilitation interventions in patients with COVID-19. A robust comprehensive systematic review and meta-analysis on the effectiveness and feasibility of telerehabilitation for patients with COVID-19 could be available in the future.
Conclusions
In the present systematic review and meta-analysis, telerehabilitation interventions delivered in a home setting showed improvements on the physical functions measured by 6MWT and 30STST, exercise perception measured by BS and level of dyspnoea measured by MD12 comparable with those of education or no rehabilitation, with an acceptable intervention completion rate. These positive findings and the potential long-term effects of telerehabilitation on pulmonary function, quality of life, anxiety, depression and other outcomes, including long-term feasibility, should be investigated with a larger sample size and higher methodological quality studies in the future.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information. All data generated or analyzed for this study are included in this published article and its supplementary information files.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have made significant contributions to this systematic review. AAS developed the research question, wrote the first draft, designed the search strategy, performed data extraction and statistical analysis, edited the manuscript and controlled and managed the overall work. SBA developed the research question, revised the search strategy of databases, developed the data extraction form, performed data extraction and statistical analysis, and edited the manuscript. AAM revised the data extraction form and edited the manuscript. All authors have approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.