Article Text

Abstract
Purpose The Scottish Diabetes Research Network (SDRN)-diabetes research platform was established to combine disparate electronic health record data into research-ready linked datasets for diabetes research in Scotland. The resultant cohort, ‘The SDRN-National Diabetes Dataset (SDRN-NDS)’, has many uses, for example, understanding healthcare burden and socioeconomic trends in disease incidence and prevalence, observational pharmacoepidemiology studies and building prediction tools to support clinical decision making.
Participants We estimate that >99% of those diagnosed with diabetes nationwide are captured into the research platform. Between 2006 and mid-2020, the cohort comprised 472 648 people alive with diabetes at any point in whom there were 4 million person-years of follow-up. Of the cohort, 88.1% had type 2 diabetes, 8.8% type 1 diabetes and 3.1% had other types (eg, secondary diabetes). Data are captured from all key clinical encounters for diabetes-related care, including diabetes clinic, primary care and podiatry and comprise clinical history and measurements with linkage to blood results, microbiology, prescribed and dispensed drug and devices, retinopathy screening, outpatient, day case and inpatient episodes, birth outcomes, cancer registry, renal registry and causes of death.
Findings to date There have been >50 publications using the SDRN-NDS. Examples of recent key findings include analysis of the incidence and relative risks for COVID-19 infection, drug safety of insulin glargine and SGLT2 inhibitors, life expectancy estimates, evaluation of the impact of flash monitors on glycaemic control and diabetic ketoacidosis and time trend analysis showing that diabetic ketoacidosis (DKA) remains a major cause of death under age 50 years. The findings have been used to guide national diabetes strategy and influence national and international guidelines.
Future plans The comprehensive SDRN-NDS will continue to be used in future studies of diabetes epidemiology in the Scottish population. It will continue to be updated at least annually, with new data sources linked as they become available.
- EPIDEMIOLOGY
- DIABETES & ENDOCRINOLOGY
- Health informatics
Data availability statement
The SDRN-EPI team welcomes external collaborative research proposals that use the research data platform. SDRN-EPI are not data custodians and are not permitted to directly provision data externally. However, the component datasets can be obtained by data governance trained bone fide researchers through the Public Benefit and PrivacyPanel for Health and Social Care. See https://www.informationgovernance.scot.nhs.uk/pbpphsc/ for how to apply.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The cohort has nationwide coverage with >99% of all those with diabetes in Scotland. This includes 472 648 individuals from 2006 to 2020.
The cohort is updated annually with extensive linkage to existing healthcare data sources, negating requirements for de novo data collection.
Furthermore, it is extendable, with new datasets being easily linked as they are created using the national Community Health Index number.
The underpinning research data platform facilitates the use of a verifiable research pipeline, as it provides both the originating and cleaned data with a controlled and documented provenance pathway.
Limitations include the need for cleaning raw data values manually entered at the clinical interface; however, this cleaning is performed consistently during the database creation and not by each research analyst.
Introduction
In Scotland, a standardised electronic health record (Scottish Care Information-Diabetes (SCI-diabetes)) has been in use for patient care in diabetes since the late 1990s, gaining nationwide coverage by mid-2000s. The record uses a unique healthcare identifier, the Community Health Index (CHI) number, which is also used on all other administrative health datasets in Scotland.1 By linking these datasets together, we sought to generate a nationwide cohort of people with diabetes, updated annually with those newly diagnosed, and rich in a wide range of data.2 Such a population-wide cohort provides invaluable information for a range of stakeholders. Uses of such data include but are not limited to (1) understanding current disease prevalence, healthcare burden and trends in disease incidence to inform resource allocation, (2) studying disease aetiology, for example, determinants of complications of diabetes including in relation to sex, ethnicity and social deprivation, (3) evaluation of new developments in care, for example, flash glucose monitors, (4) studying the real-world observational pharmacoepidemiology of diabetes drugs on outcomes, (5) understanding the natural history of disease, for example, the progression rates to type 2 diabetes in those with prior gestational diabetes, (6) building prediction tools for decision making, such as cardiovascular disease risk scores, and many more.
However, building a cohort and underpinning a research data platform from electronic healthcare records, as distinct from study-specific data collections as in a clinical trial, for example, brings several challenges. A key issue is how best to organise and control the vast amounts of data received from various sources, each with differing levels of consistency and historical meta information. Another issue is that there will, in such data, be errors, and extensive data cleaning may be required. There is also a need to provide metadata to users on such extensive datasets, and the data must be held in a way that provides security and privacy. For a wide range of end-users of the database, data must be centrally provisioned in a common, consistent format that ensures the efficiency of the analytic code and provides a scalable, standardised structure for organising data in a way that can answer different research questions concurrently across teams of individuals. Such abstraction of data resources also enables common approaches to be adopted in downstream processes, including cohort generation, data analysis, automatic manuscript generation using R markdown3 and implementation of reproducible research frameworks.
In this paper, we (the Scottish Diabetes Research Network Epidemiology SDRN-EPI Group) provide a detailed description of the SDRN-diabetes research platform where SCI-Diabetes data (the spine of the database) have been linked to other data. We present details of the resulting cohort, the SDRN-National Diabetes Study (NDS) cohort summarising the data content in the cohort and its characteristics.
Cohort generation and characteristics
Data sources/diabetes data
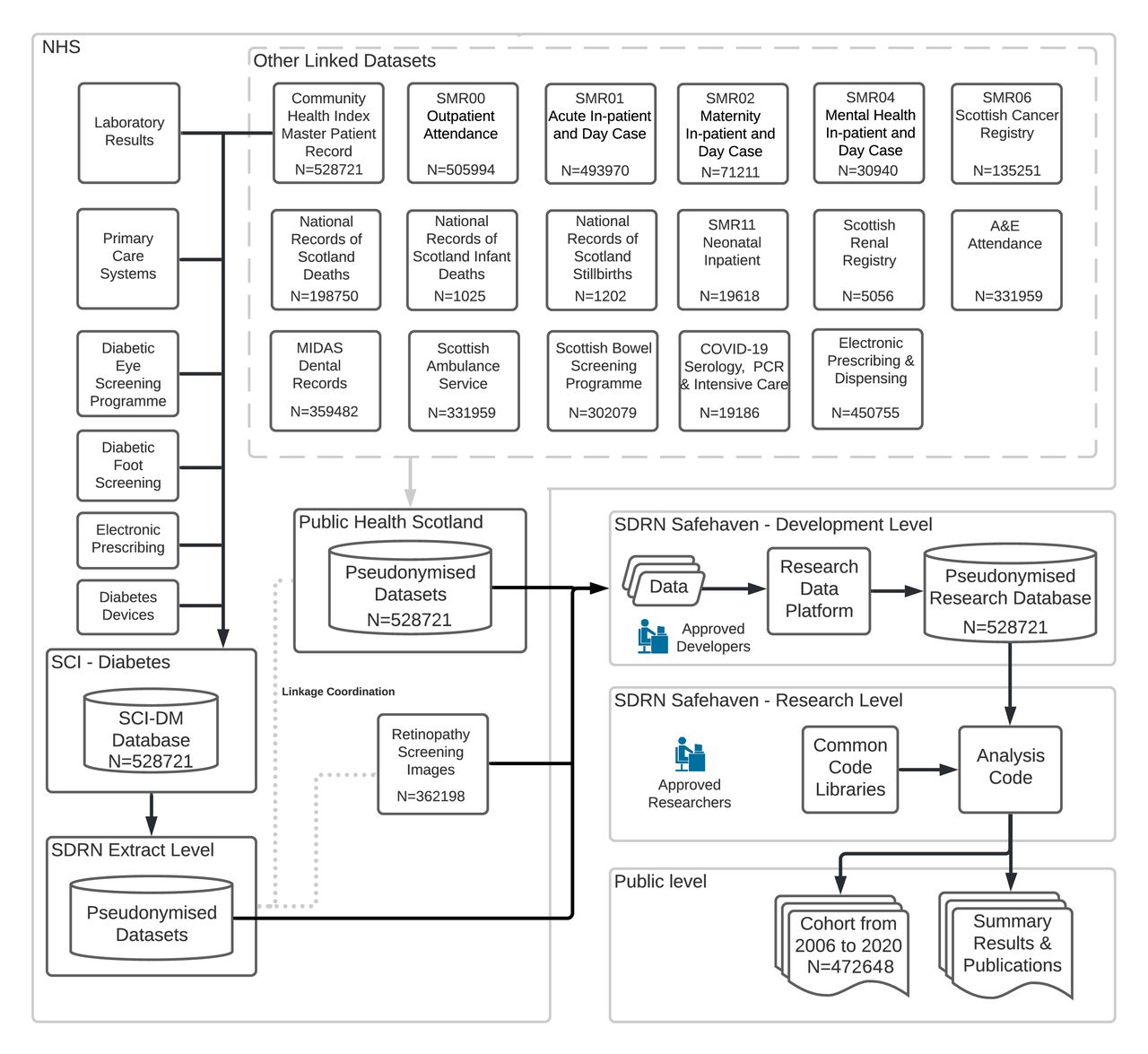
As shown in figure 1, the main source of diabetes data comes from NHS Scotland’s national patient record for diabetes care called Scottish Care Information-Diabetes (SCI-Diabetes). SCI-Diabetes itself is used for delivering patient care in most specialist and some primary care settings, including hospital, adult and paediatric diabetes clinics, podiatry clinics, dietetic clinics, inpatient review, community diabetes and so on. All newly diagnosed persons coded with diabetes in primary care have a record created in SCI-Diabetes. For patients registered on the system, there is an automated nightly feed into SCI-Diabetes of key retrospective and prospective information relevant to diabetes care, including all prescribed drugs from all primary care practices. Key data items including laboratory tests relevant for diabetes management and retinopathy screening and grading outcomes are uploaded to the system via direct data transfer via web services from NHS laboratory data stores and the National Retinopathy screening programme. There are various dashboards and interfaces enabling clinicians to enter data and gain summaries of individuals and their overall clinic or regional population.
{kind=link}
Scottish Diabetes Research Network data flow. SCI-DM, Scottish Care Information-Diabetes; SDRN, Scottish Diabetes Research Network.
We estimate that the coverage of the diabetes non-temporary population with a diabetes diagnosis residing in Scotland by SCI-Diabetes is more than 99%. All general practices nationwide contribute data to the SCI-Diabetes database. Furthermore, in a validation study, we queried all national hospital admission records and prescribing databases in 2018/2019 for any evidence of diabetes and then established whether all such persons have a record in SCI-diabetes. There were just 3228 people (<1% of the total including people on SCI diabetes who were alive at any point in 2018/2019) with evidence of diabetes but not on SCI-Diabetes. Confirming diabetes registration is an essential step for a person’s diabetes care since it forms the basis for invitation to the national retinal screening programme. Since 2% or less of retinopathy screening invitations are rejected on the basis of an incorrect assignation of diabetes where the person does not have diabetes, the positive predictive value of registration is 98%, and specificity is high.4
Other linked datasets
Primary care is free at the point of delivery in Scotland. On registering with a primary care physician, all patients in Scotland are assigned a CHI number, which is used as the key identifier on all health record systems across the country. This allows linkage of the primary SCI-Diabetes patient datasets to other key sources of data for research purposes, for example, the Scottish Morbidity Records that cover inpatient and outpatient attendances, maternity and birth hospital data and cancer registry data. Also linked are dispensed drugs and devices, intensive care unit and microbiology data, births and deaths data from National Records of Scotland (NRS). See figure 1 for a full list of datasets. Online supplemental table 1 provides a listing of key variables available in the database.
Supplemental material
Provisioning of data for research and its governance
Deidentified extracts of data from SCI-Diabetes containing a pseudonymised identifier are provided to the authorised group of research users, the SDRN-EPI group, via an approved, secured safe haven. For the same cohort of individuals, linked datasets are provided by the Public Health Scotland (PHS) Electronic Data Research and Innovation Service group. This is achieved by a transfer of CHI numbers with their pseudonymised identifier to PHS. Deidentified data containing the pseudonymised identifier and not the CHI are then provided to SDRN-EPI for merging. Regular transfer of data is scheduled from each source, with each provider performing extraction and deidentification before transfer into the SDRN-EPI Safe Haven environment. Deidentification includes pseudonymisation of the CHI number, removal of any identifiable data and reduction in granularity of key dates (eg, date of birth) by resetting each to mid-month.
Access to the Scottish NHS diabetes data sources is granted to the SDRN epidemiology research purposes by approval from the Public Benefit and Privacy Panel for Health and Social Care (reference 1617–0147). All data are held in a secure safe haven environment. All users are trained in data governance and as all processing and computation take place centrally, no export of data from the safe haven environment is permitted. The SDRN epidemiology group is not authorised to secondarily provision data externally; however, researchers who have obtained local R&D sponsorship may contact the SDRN administrator (administrator-sdrn@dundee.ac.uk) regarding collaborations that fall within the remit of the SDRN epidemiology governance structure.
Diabetes research data platform
The data transfer process results in several very large flat text data files containing longitudinal point-in-time data for various measures, diagnoses and interventions. On receipt of these data, the SDRN data manager ensures all meta information files are updated and correct. Subsequently, a new research database is generated with a three-stage build process converting the input data into a structured and strongly-typed relational database of longitudinal patient data. This data platform provides abstraction between research data and analysis. This is achieved by implementing two distinct software layers. The first layer performs extraction, transformation and loading (ETL) into a common data resource. The second, the analysis layer, enables research question-specific extraction and transformation from the common data resource. The data ETL is implemented in Python5 and R6 and takes disparate data sources, transforming them into a controlled, comprehensive, standardised relational research database with an accompanying electronic metadata dictionary. In the analysis layer, each database is designed to provide research question-specific longitudinal cohort datasets covering all areas of electronic health records through a standard interface with minimal latency. As the data layer is refreshed through time, the original analysis code is executed on the updated resource with minimal modification. The analysis layer is currently implemented in ‘R’, connecting to the data resource via Open Database Connectivity, with libraries and object-oriented code providing mechanisms for cohort definition and analysis dataset generation for the full gamut of epidemiological study designs.
It is useful for other researchers trying to implement such datasets from electronic health records to have a working example of how some of the challenges of the use of electronic health records have been addressed that may be of general use for others in the field. We provide a detailed specification of the database and its construction in the supplemental appendix. This includes an overview of the SDRN-NDS data model in online supplemental figure 1 and details of an object oriented library used for converting database data into a longitudinal research form in online supplemental figure 2.
Cohort characteristics
Altogether, the Diabetes Research Platform contains data on 528 721 individuals alive and with diabetes in Scotland at any time between 1 January 1984 and 8 April 2020, with data extracted between 3 August 2020 and 5 October 2020. The diabetes electronic health record in Scotland was used in some parts of the country since the mid-1990s but did not reach >95% coverage of the population of Scotland until 2006. For most analyses, therefore, we use the data from 2006 onwards which includes 472 648 individuals. Here, we describe the data from the cohort alive with diabetes anytime between 2006 and mid-2020 (the last date on which extraction from raw clinical data occurred).
Table 1 shows the prevalence of type 1 and type 2 diabetes from years 2006 to 2020. Mid-year population estimates were imported from NRS.7 Altogether, there were 472 648 individuals with diabetes who were alive with diabetes at any time between 2006 and 2020 who were included in the cohort. There are 4 million person-years of follow-up.
Numbers of people with diabetes from 2006 to 2020 by diabetes type and overall annual prevalence
As shown, 8.8% of those in this cohort have been assigned as having type 1 diabetes. The type of diabetes can be recorded in SCI-Diabetes by multiple sources (primary care physician, secondary care physician, community nurse and so on). Thus, there is a longitudinal record of type for any given person within which there can be consistent or inconsistent type assignation. In the research data platform, we therefore employ an algorithm to check type against other data on prescriptions and date of diabetes onset. For type 1 diabetes, for example, misclassification might be defined by (1) extensive use of oral antidiabetic medication and (2) no continuous insulin therapy within 1 year of diagnosis. Those who are initially assigned as type 2 are reassigned to type 1 only if they have no contrary prescription history, 183 days of insulin prescribed in the year since diagnosis and an age of onset below age 30 years. The application of the algorithm resulted in a reassignment of 10.5% of people in the cohort with an initial label of type 1 being reassigned to type 2 and 0.8% of type 2 being reassigned to type 1. Most of this reassignment refers to those with already prevalent diabetes when the SCI-Diabetes record system was being established. As shown in online supplemental table 2, there is a much lower reassignment of type for incident cases in recent years. Of the cohort, 3.1% have other types of diabetes, as shown in table 2. These comprise, for example, secondary diabetes, gestational diabetes and monogenic diabetes.
Cohort demographics for people included in SCI-diabetes any time between 2006 and 2020 by diabetes type
A summary of the cohort demographics by diabetes type is provided in table 2. There is a slight excess of males for both types of diabetes. For non-fixed characteristics, we show the median and IQR of values in the cohort, having computed the within-person results over the years that they are observed in the cohort. The average age during the follow-up period is 47 years for type 1 diabetes and 71 years for type 2 diabetes. The average duration of diabetes during the follow-up period is 18 years for type 1 diabetes and 9 years for type 2 diabetes. The geographic distribution follows that of the overall population of Scotland, with the majority of the population residing in the central belt of Scotland between Glasgow in the West and Lothian in the East. The social class categorisation used is the Scottish Index of Multiple Deprivation.8 This categorises the deprivation score of the area the person lives in. As can be seen particularly for type 2 diabetes, there is a social class gradient with 47% being in the most deprived two quintiles, where 40% would be expected if there were no social class disparity in prevalence. There is substantial missingness for ethnicity, which is optionally self-assigned by the person with diabetes during outpatient and hospital encounters.
Clinical characteristics are summarised in table 3, including the median (IQR) frequency of each measure each year from 2006 to 2020 and the percentage of missingness. As shown for most of these measures, on average, people have at least one reading per year for each year of follow-up. Thus, the database is a very rich source of longitudinal trajectories of these characteristics in diabetes. There is a high level of missingness for low-density lipoprotein (LDL) cholesterol as the default is to measure total cholesterol first, and LDL cholesterol is then measured contingent on the total-cholesterol value. Height is not typically measured annually as expected for adults. For retinopathy, we show the grading on the photographs taken in the national screening programme for which only those aged 12 years and upwards are eligible. Those denoted as attending the eye clinic have previously had gradings to indicate either maculopathy or at least preproliferative retinopathy. Many person-years of follow-up are missing the albuminuria status and foot screening data in part because some point of care tests are not captured into the system, but this can also be caused by clinicians failing to arrange the tests and patients not having an adequate urine sample at their clinic visit. However, there is a high capture of estimated glomerular filtration rate (eGFR) with, on average, at least one measure each year in those with type 1 and 2 measures per year in those with type 2 diabetes.
Cohort summary clinical measurements from 2006 to 2020 by diabetes type
Patient and public involvement
The work of SDRN-EPI generating and using the national diabetes research platform is approved by the Public Benefit and Privacy Panel, which includes patient representatives. The Diabetes Informatics and Epidemiology team at the University of Edinburgh hosts a Patients Advisory Committee (PAC) that scrutinises and makes recommendations on the use of the data, priorities for research as well as advising on messaging key findings to the diabetes community. The SDRN also hosts PAC that comments and advises on specific research funding applications using the data.
Findings to date
The SDRN-Epi team have published more than 50 papers on the cohort from the National Diabetes Research Platform to date.9 These papers span a range of topic areas including evaluation of new technologies, modelling to underpin retinopathy screening intervals, complication risk prediction tools, observational pharmacoepidemiology, time trend analyses and much more. Several international collaborations have used the data. More recently, the database has been pivotal in generating data and an evidence base for COVID-19 prevention policies in people living with diabetes. We describe here a selection of the more recently published outputs from the platform.
With two recent analyses, we were able to reassure policymakers in the National Health Service in Scotland that investment in free provision of continuous subcutaneous insulin infusion (CSII) pumps and flash monitors is having an impact on important outcomes. We showed10 that flash monitor initiation was associated with clinically important reductions in HbA1c, especially in those with worst glycaemic control; an average fall of 15.5 mmol/mol (1.4% units) in those with HbA1c>84 mmol/mol (9.8%) for example. We also showed a striking 40% reduction in diabetic ketoacidosis incidence with flash monitor use. With CSII use, we also observed marked falls in HbA1c, especially in those with high baseline HbA1c, an average fall of 21.0 mmol/mol (1.9% units in those with a baseline >84 mmol/mol within a year of exposure) that was sustained.11 CSII was associated with a 39% reduction in DKA rates and a 33% reduction in severe hospitalised hypoglycaemia. Such data are key inputs to health economic analyses that justify increasing provision for the use of diabetes technologies to improve health outcomes.
We have demonstrated increases in the number of women with existing type 2 diabetes before pregnancy achieving a successful term.12 However, there are marked increases in birth weight in women with type 1 and type 2 diabetes.12 Rates of stillbirth were 4 and 5 times those of the background population in women with type 1 and type 2 diabetes, respectively.12 We have further explored the importance of glycaemic control and adiposity in stillbirth.13
In a recent time trends analysis, we focused on trends in mortality under the age of 50 years, as overall mortality trends are overwhelmingly determined by cardiovascular disease trends in older persons.14 Yet, young deaths contribute enormously to overall years-of-life lost. We showed that absolute mortality has fallen, but the relative impact of type 1 diabetes on mortality below 50 years has not improved; the standardised mortality ratio relative to the background population was approximately stable at 3.1 and 3.6 in men and 4.09 and 4.16 in women for 2004 and 2017, respectively. Diabetic ketoacidosis or coma deaths accounted for 22% of deaths under age 50 years and the rate did not decline significantly in that period. The vast majority of such deaths (79.3%) occurred out of hospital, emphasising the need for community recognition and prevention of DKA. This work influenced the recent Scottish Government Diabetes Improvement Plan for the next 5 years with the launch of a new DKA national education campaign.15
During the first wave of the COVID-19 pandemic, we quickly produced a report for Government and Diabetes Charity stakeholders, later published as a manuscript, showing elevated relative risks of severe COVID-19 in those with type 1 (2.4-fold) and type 2 diabetes (1.4-fold).16 Before that, most estimations of the risks were simple descriptions of the proportions of hospitalised patients with diabetes. We showed that there was wide variation in risk in those with diabetes and that risk was highly predictable (C-statistic 0.89), and we produced a tool (https://diabepi.shinyapps.io/covidrisk/) to facilitate conversations on COVID-19 risk between clinician and their patients. The data we produced were pivotal in reassuring policymakers that the extreme social distancing programme (shielding) should not be mandated for the majority of those with diabetes.
SCI-diabetes SDRN data was the largest contributing dataset to a UK four nations approach looking at outcomes for diabetes retinal screening (DRS), and in particular for those with low-risk eye disease. Linked data on 354 549 people with diabetes has shown that it is safe to undertake retinal screening every 2 years rather than every year for those with two baseline reports of no retinopathy.17 This has led to a change in the National DRS policy in Scotland. SDRN data have also been the first comprehensive national data to demonstrate a reduction in amputation rates with a 29.8% reduction in all amputations for people with diabetes between the years of 2004 and 2008.18 In addition, SDRN data have allowed Scotland to be the first country to report on comprehensive national data on the incidence of foot ulceration at 1.1%, with first time ulceration at 0.7%.19 People with foot ulcers are 2–5-fold more likely to die than to undergo amputation, and those with high risk feet are 9-fold more likely to die than undergo amputation20 which has major implications for health planning.
Other examples of recent work include descriptions of:
Strengths and limitations
The strengths of this cohort are its large size (over 2 billion health data records from over 472 648 individuals to date), the nationwide coverage, the long period of follow-up, the frequency and, by definition, completeness of capture of data items given comprehensive coverage of electronic records. Other key strengths include the extensive data linkages to other datasets and that the data are regularly updated. A major strength is that this is built on existing healthcare data and does not require any de novo data collection.
Furthermore, it is extendible, with new datasets being easily linked as they get created by using the national CHI number. An example of this was the rapid recent linkage to national virology to capture all SARS-CoV-2 tests done nationally.
Key strengths of the underpinning research data platform and attendant tools are that it encapsulates much of the required cleaning and complexity away from the end user. It presents metadata simply; it has in-built source code control, it allows rapid creation of the necessary longitudinal subsets of records for a given analysis and it facilitates the use of a verifiable research pipeline as it offers full traceability to originating precleaned data.
Limitations include the inherent limitations of basing a cohort on electronic health records. There will inevitably be incorrect raw data values entered at the clinical interface that require cleaning, along with changes to lab reference ranges within various health boards, incomplete metadata and inconsistent data due to new systems being introduced in the earlier years. Another challenge is that for key data concepts, the underpinning raw data source for example, assay method and normal range may change over time. For example, albuminuria status might be measured by albumin concentrations or albumin creatinine ratios at differing points in time, and how this is handled must be captured in the metadata. Another limitation is that we are dependent on the timescales of upstream data providers; ideally, we would like to refresh the data every few months, but currently, it typically happens annually. Since the cohort is limited to people with a current or previous diabetes diagnosis, any analysis requiring a non-diabetic comparative group will require further linkage to the general population without a history of diabetes. Finally, many cohort studies with dedicated data collection systems will use the health record as the gold standard or ‘ground truth’ against which to check the accuracy of their data. Here, we are using this gold standard health record itself as the data source and, therefore, must use internal consistency and validity checks, as exemplified by our diabetes type algorithm, to establish ground truth.
Data availability statement
The SDRN-EPI team welcomes external collaborative research proposals that use the research data platform. SDRN-EPI are not data custodians and are not permitted to directly provision data externally. However, the component datasets can be obtained by data governance trained bone fide researchers through the Public Benefit and PrivacyPanel for Health and Social Care. See https://www.informationgovernance.scot.nhs.uk/pbpphsc/ for how to apply.
Ethics statements
Patient consent for publication
Acknowledgments
We acknowledge with gratitude the contributions of people with diabetes, NHS staff and organisations (the Scottish Care Information-Diabetes development team and Steering Group, the Scottish Diabetes Group, the Scottish Diabetes Survey Group, the diabetes managed clinical networks) involved in providing data, setting up, maintaining and overseeing collation of data for people with diabetes in Scotland. Data linkage is performed by colleagues at Public Health Scotland. We acknowledge the financial support of NHS Research Scotland (NRS), through Diabetes Network. The NHS Research Scotland Diabetes Network (formerly Scottish Diabetes Research Network) receives funding from the Chief Scientist Office of the Scottish Government.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MetaMedTeam
Collaborators The SDRN-EPI team welcomes external collaborative research proposals that use the research data platform. Such proposals are welcomed by academic researchers, commercial entities and other stakeholders, for example, policymakers. There must be a valid scientific question in all collaborations, and no right of veto over the publication of results will be granted.
Contributors SP is Clinical Lead for SCI-Diabetes. SMcG, LAKB, PMcK and HC designed the platform. SMcG, LAKB and HC performed data transformation. SW, LAKB and HC obtained ethical and governance approvals. TC, JM, AB, AC, NS, JMcK, JP, SP, RL, KH, DMcA, GL and EP commented on database design and contributed to source data generation. SMcG and LAKB conducted the analyses in this manuscript. SMcG and HC wrote the initial draft of this manuscript. TC, JM, AB, AC, NS, JMcK, JP, SP, RL, KH, DMcA, GL, SW and EP edited the manuscript and revised it critically for important intellectual content. HC is responsible for the overall content as the guarantor. All authors approved the final version and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding Work described here has been supported by Chief Scientist Office Scotland (Ref. ETM/47) and by Diabetes UK (Ref. 17/0005627).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.