Article Text

Abstract
Objectives To determine the prevalence of undiagnosed hepatitis C virus (HCV) and HIV cases in a population sample tested in the emergency room (ER) and to evaluate linkage-to-care.
Setting Canadian university hospital.
Participants Adults born after 1945 who consulted at ER for any condition and on any shift were included. Patients unable to opt-out were excluded.
Interventions ER nurse confirmed patients’ eligibility and provided them with the option to opt-out. A physician met patients with a new diagnosis. Linkage-to-care was assessed 3 months postdiagnosis. Patients newly diagnosed with HCV were considered linked if they had an HCV RNA test, genotype, liver fibrosis evaluation, and if indicated, treatment prescription. Patients newly diagnosed with HIV were considered linked to care if they had an HIV serology confirmation test, viral load, CD4 cell count and started antiretroviral therapy.
Primary and secondary outcome measures Primary objective: to determine the prevalence (overall and undiagnosed cases) of HIV and HCV among the patients who consult the ER. Secondary objectives: to determine the proportion of patients who opt-out, assess the adherence of emergency staff to the offer of testing, determine the proportion of patients linked to care at 3 months.
Results Among 6350 eligible patients informed of the screening programme, 62.1% of patients were tested for at least one virus (HIV: 3905; HCV: 3910). 25% patients opted-out, 12% were not tested for organisational reasons, 0.3% (18) patients were HCV-HIV coinfected. Overall prevalence of HCV and HIV cases were 1.9% and 1.2%, respectively. Prevalence of new cases was 0.23% (95% CI 0.12% 0.45%) for HCV and 0.05% (95% CI 0.01% to 0.20%) for HIV. Among the new cases, only two HCV-infected and one HIV-infected patients were linked-to-care 3 months postdiagnosis.
Conclusions Identification of new cases of HCV and HIV through universal screening at the ER and linkage-to-care were both low.
Trial registration number NCT03595527; Results.
- HIV & AIDS
- hepatology
- accident & emergency medicine
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first Canadian study to evaluate emergency room screening for hepatitis C virus (HCV).
A large number of patients were cotested for HIV and HCV, without regard to their risk factors.
Risk factors were evaluated among the patients newly diagnosed positive in order to evaluate the added benefit of universal screening.
Linkage to care was evaluated among the patients newly diagnosed positive.
Testing was performed in an urban tertiary care hospital, which can limit generalisability to other settings.
Introduction
To achieve WHO goal of zero transmission of HIV and elimination of hepatitis C virus (HCV) by 2030, it is essential to increase screening.1 2 It is estimated that 14% of HIV-infected and 44% HCV-infected Canadians do not know their status.3 4 Except for pregnant women who are universally tested for HIV, Quebec current screening system is based on the identification of risk factors (targeted screening) and may be currently missing a significant proportion of cases.
There are two approaches about screening. The ‘opt-in’ approach consists in informing the patient that the test is available and asking him if he wishes to be tested. The ‘opt-out’ option consists in informing the patient that he will be tested unless he declines the test. Several studies have demonstrated the acceptability of the latter approach with a higher screening rate than with the ‘opt-in’ option.5 6
Since 2006, the Centers for Disease Control and Prevention advocated integrating HIV testing into the care of all patients aged 13–64.7 In 2012, this was supported by the US Preventive Service Task Force, thereby promoting emergency room (ER) screening.8 Universal HIV testing is considered cost-effective in settings where the prevalence of undiagnosed HIV infections is ≥0.1%.9 Prevalence of new cases varies according to the overall prevalence of the population tested as well as the ease of access to screening outside the ER. A systematic review in 2017 reported a prevalence of new HIV cases of 0.4% (95% CI 0.21% to 0.64%) in 10 opt-out studies.10 The nine studies from the USA reached the cost-effectiveness thresholds (0.14%–1.65%) while the Singapore study reported a prevalence of only 0.06% of new cases.10 In Canada, British Columbia public health has recommended HIV screening for all patients presenting at the ER or admitted in three Vancouver hospitals since 2011.11 Between 2012 and 2016, the prevalence of new cases in the ER was 0.2%, reaching the cost-effectiveness threshold in the epicentre of HIV epidemic in this province.11
Given the ease of coscreening for HIV and HCV, studies of universal screening for HCV in the ER have been carried out and show a great variability in the prevalence (0.5%–14%) and identification of new cases (0.2%–9.4%) (table 1).12–23 Since 2013, the US Preventive Service Task Force has recommended a once in a life-time screening for HCV in adults born between 1945 and 1965 (‘baby boomers').24 In 2020, this recommendation was enlarged to a once in a lifetime screening for HCV for all adults, except in settings where the prevalence of HCV infection is less than 0.1%.25 This screening can take place in any context of care including the ER. This is not recommended in Canada, although some expert groups have endorsed baby boomers cohort screening.26–28
Non-exhaustive list of publications on non-targeted HCV screening in the ER
The aims of this study were to assess the feasibility of routine screening for HIV and HCV using an ‘opt-out’ approach in the ER of the Centre hospitalier de l’Université de Montréal (CHUM) and determine whether the positivity rate of new HIV and HCV infections would inform the long-term implementation of such screening.
Methods
Objectives
The primary objective of this cross-sectional study was to determine the prevalence (overall and undiagnosed cases) of HIV and HCV among the patients who consult the ER of the CHUM. The secondary objectives were to (1) determine the proportion of patients who ‘opt-out’; (2) assess the adherence of emergency staff to the offer of testing; (3) determine the prevalence of undiagnosed cases of HCV among baby boomers and (4) determine the proportion of patients linked to care at 3 months.
Setting
The study took place at the CHUM, a 772 beds, university hospital localised in downtown Montréal, in the near vicinity of Montreal Gay Village, multiple homeless shelters and needle-exchange/supervised injection sites facilities. This ER is not serving a significant amount First Nations and foreign-born patients.
Patient and public involvement
Patients and public were not involved in the recruitment and conduct of the study.
Eligibility criteria
Patients aged 18–73 (ie, adults born after 1945 at the time of the study) who consulted at ER for any condition and on any shift were supposed to be advised that, unless they refuse, they would be tested for HIV and HCV (opt-out). Patients unable to opt-out for language barriers, psychiatric reasons or having an unstable physical condition were excluded.
Interventions
Before starting the inclusion period, preparatory meetings were held with the study staff (ER managers, physicians and nurses) to clarify the study procedures and answer their questions. During the study, a research nurse was regularly present to support the ER staff on all shifts.
On initial contact with potential candidates, the ER nurse confirmed their age, assessed them for known HIV or HCV infection and provided them with the option to opt-out. Patients could be tested for only one virus if they were known positive for the other or if they refused one test. Where possible, blood samples were taken concurrently with other blood tests as required by the patient’s medical condition. If no blood work was required, the patient could have blood sampling specifically for this screening study. In extreme circumstances, priority was given to patient care and recruitment into the study was suspended.
HIV Ag/Ab combo tests and anti-HCV tests were performed on the ARCHITECT (Abbott). Positive HIV tests and indeterminate HCV tests were confirmed at the Laboratoire de Santé Publique du Quebec.
Patients had generally left the ER once their results were available. A study nurse disclosed negative results directly to the patient over the phone or in person for admitted patients. If not reached by these methods, a letter was sent. For patients with a positive test result, the nurse evaluated if the patients were known to be positive. Patients were considered known to be positive if they self-reported to be positive or if the laboratory reported a previously known infection. For participants with either a new diagnosis of HIV or HCV, or with an indeterminate test for HCV, which required additional HCV RNA testing, the study nurse made multiple attempts to reach the patients, using the same methods of communication as for negative patients, and she scheduled an on-site visit with the study infectious disease specialist.
Following disclosure of a positive result, patients signed an informed consent form, were asked about their risk factors and history of HIV/HCV testing, referred to a treatment team, and followed up by the research team for 3 months to assess linkage-to-care. Patients with new HIV diagnosis were considered linked to care if they had had an HIV serology confirmation test, viral load, CD4 cell count and had started antiretroviral therapy. Patients with new HCV diagnosis were considered linked if they had had an HCV RNA test, genotype, liver fibrosis evaluation, and if indicated, treatment prescription.
Statistical analysis
The original goal was to perform 4000 tests for each virus. If a patient had multiple visits during the study period, only the first tests were used for analysis. The sample size was established according to the prevalence threshold of new diagnoses of HIV infection justifying the implementation of a routine HIV testing programme (0.1%).9 Assuming a prevalence of undiagnosed cases of 1/1000, a study of 4000 participants would lead to a 95% CI from 0.3/1000 to 2.7/1000. For HCV, assuming a prevalence of undiagnosed cases of 1/100, the 95% CI would be between 0.7% and 1.3%.
Descriptive statistics were used to calculate HIV and HCV prevalence of undiagnosed and overall cases and the proportions of ‘opt-out’, staff adherence to screening and linkage to care. Overall prevalence must be considered as an approximation, as not all patients of the denominator were tested (self-report, opt-out). A subanalysis was performed regarding prevalence of HCV new cases among baby boomers. Even if baby boomers are generally considered to be people born between 1945 and 1965, for HCV screening in Canada, this generation extends until 1975.29
Results
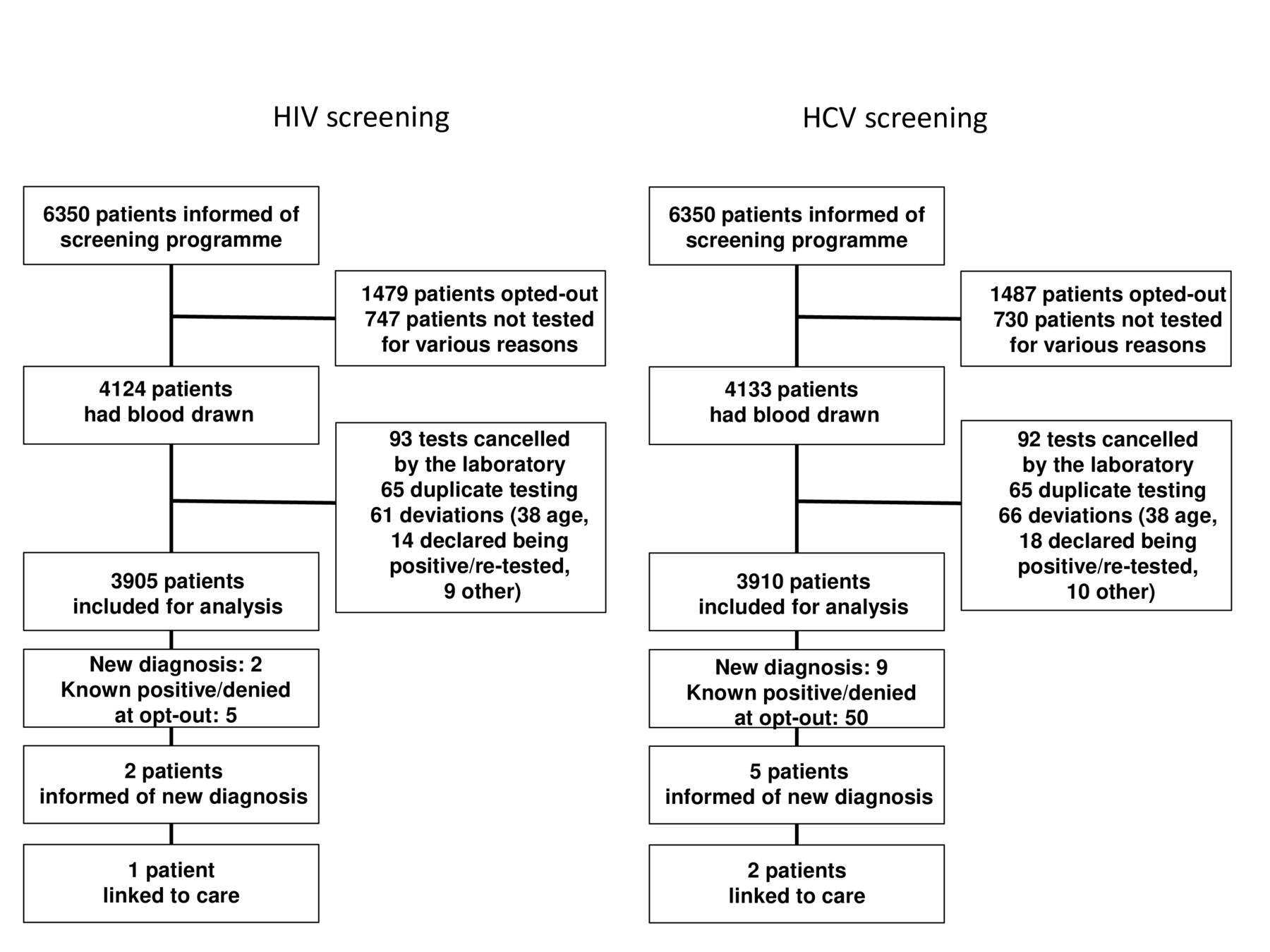
Between July 2018 and May 2019, 6350 patients were informed of the screening programme, which represents 21.5% of all patients aged 18–73 years seen in the ER during this period. Figure 1 shows the number of participants not included in the analysis and the reasons. Median age of participating patients was 41 yo (IQR: 30–56) and 53% were women. A quarter of the patients opted-out (women: 51%; median age 44 years (IQR 31–57)). In addition, around 12% were informed of the programme, did not opt-out, but were not tested. The two main reasons were patients who left the ER without being seen by the medical team, or physicians who discharged the patients before the nurses could draw the blood.

Enrolment and outcomes of screening. HCV, hepatitis C virus.
Among the 6350 participants, 78 were positive for HIV: 71 self-reported being positive, 5 denied being positive, but were known to be positive in the laboratory informatics system, and 2 were newly diagnosed. For HCV, 118 patients were positive: 59 self-reported being positive, 50 denied being positive but were known to be positive and 9 were newly diagnosed. The overall HIV prevalence was therefore 78/6350 participants, or 1.2% (95% CI 1.0% to 1.5%) and the overall HCV prevalence was 118 cases/6350 participants, or 1.9% (95% CI 1.6% to 2.2%). The prevalence of new diagnoses was 2/3905 participants tested, or 0.05% (95% CI 0.01% to 0.20%) for HIV and 9/3910 participants tested (0.23%; 95% CI 0.12% to 0.45%) for HCV. New HIV diagnoses represent 2.6% of positive cases (2/78) while new HCV diagnoses represent 7.6% of positive cases (9/118).
People born between 1945 and 1965 represented 30.7% of the cohort (figure 2). This proportion increased to 46.5% when people born until 1975 were included. Seven of the nine new cases were born between 1945 and 1975 while only three were born between 1945 and 1965. The prevalence of new cases was therefore: 1945–1965: 0.25% (95% CI 0.09% to 0.73%), 1966–1975: 0.65% (95% CI 0.25% to 1.66%), 1976–2001: 0.10% (95% CI 0.03% to 0.35%).

{kind=link}
{kind=link}
Proportion of people tested for HCV and prevalence of undiagnosed HCV cases by birth cohort. HCV, hepatitis C virus.
Two new cases of HIV (100%) and five new cases of HCV (56%) were successfully reached to disclose the result. All the patients had recognised risk factors for their infection. Among HIV new diagnoses, a man had sex with men (MSM) with an HIV positive partner and a man had unprotected heterosexual relations in a country of high endemicity. Among HCV new diagnoses, three patients used/had used injection drugs and two had received at risk transfusions (geographical location or year of transfusion). Five patients were HCV RNA positive.
In terms of linkage to care, one out of two HIV-infected patients (50%) and two out of nine HCV-infected patients (22%) were linked to care at 3 months based on our criteria. The patient with newly diagnosed HIV and not linked to care left the consultation after disclosure of the diagnosis by the infectious disease specialist and did not answer our calls thereafter. Four of the nine patients with newly diagnosed HCV could not be reach after the ER visit. For the three remaining patients, one patient did not complete HCV RNA testing within 3 months, one did not complete fibrosis evaluation and one patient had medications prescribed after the 3 months follow-up period.
Discussion
Our study demonstrates the feasibility of universal ER screening in Quebec. Despite the high-risk population served by the hospital, the number of new cases identified was low (two HIV and nine HCV). The overall prevalence of HCV in our study was similar to what is reported for the Montreal area (1.9% vs 1.5%) while HIV prevalence was higher than provincial estimates (1.2% vs 0.2%; no data available specifically for Montreal).30 31 This suggests that we have not underidentified the positive cases and that the number of undiagnosed cases in our environment is possibly lower than what is reported in the literature in Canada (HIV: 14% and HCV: 44%).3 4 The prevalence of new cases was similar to what was found in other ER universal screening studies, except for certain American studies (table 1).10 Our HIV results are also lower to what was observed in Vancouver (0.05% vs 0.2%).11 Our study also underlines the challenges of conducting universal screening in an ER: relatively low staff adherence to screening offer (21.5% of all potentially eligible patients presenting to the ER), significant opt-out proportion (25% of patients informed of the screening programme), and non completion of screening of patients who did not opt-out (12%), especially when patients leave before being seen by the medical team or are discharged by the physician before the nurses could draw the blood.
All patients newly diagnosed had well-known risk factors for HIV or HCV. Having not been diagnosed before, these patients have likely benefited from our screening programme. However, a systematic targeted screening based on risk factors rather than a non-targeted testing without regards to risk factors might have been more effective. During a cluster-randomised two-period cross-over trial conducted in eight ERs in France, nurse-driven targeted screening was offered after the completion of a short self-administered questionnaire.32 Targeted screening combined with diagnostic testing (intervention strategy) was compared with a control strategy involving physician-directed diagnostic testing alone. The intervention resulted in a higher proportion of new diagnoses among patients visiting the ERs (RR 3.7, 95% CI 1.4 to 9.8). The authors compared their results to a non targeted screening study performed in the same region and reported higher proportions of positive results in the targeted study (0.46% vs 0.14%) with a substantial reduction in the number of tests performed.32 33 On the other hand, some studies indicate that, even if the positive rate might be higher in targeted screening programmes, the absolute number of cases identified might be lower as less patients are tested or might be similar.34 35 Targeted screening reduces the number of tests to be performed and might potentially be less expensive than universal screening, provided that the strategy to identify cases, including staff requirements is not more costly than the tests avoided.
Baby boomers represented the majority of the new HCV cases, but only if the cohort was extended until 1975. Most cases were among patients born between 1965 and 1975 (figure 2). One argument regarding universal screening is the destigmatisation associated with this approach. The reasonably low proportion of opt-out in our study is in favour of this argument. Universal screening decreases memory biases associated to potentially remote risk factors.36 Cost-effectiveness of baby-boomers screening has been advocated for implementation, but this economical benefit is highly dependent of the prevalence of undiagnosed cases. With the limitation that we identified a low number of cases, the fact that all of them had some risk factors seems to support the Canadian Task Force recommendation to limit screening of baby boomers to those who are at risk of HCV.26
For HIV and HCV, linkage to care is critical. As the populations affected by these conditions are often vulnerable and marginalised, they face many barriers when trying to access care and their linkage is often difficult. In the present study, difficulties linking patients to care are consequently no exception (HIV: 50%; HCV: 22%). As some patients seen in the ER could not be traced back, the use of point-of-care tests could have been advantageous in order to improve results disclosure.37 ER screening can also be an opportunity to re-link to care patients previously diagnosed.38 Unfortunately, as this was not an aim of our study, we cannot comment on linkage to care of the previously diagnosed patients (76 HIV-infected and 109 HCV-infected patients).
In our study, only 21.5% of patients seen in the ER were informed of the screening programme but this finding is comparable to results of similar studies in the ER context, given the high patient volume environment.39 Nursing participation is critical for a screening programme and recruitment was probably greatly influenced by the nurses’ willingness to participate in the project, with some participating more than others. This was difficult to quantify, but was clearly perceived by the research nurse supporting the ER team. ER overflow is a real challenge in Quebec and elsewhere, particularly in winter, during the respiratory viruses season. Consequently, it was stipulated in the protocol that, if the workload of a nurse was too heavy, clinical care took precedence over the study. In addition, some nurses might have had reluctance to discuss HIV and HCV screening with patients due to discomfort with these conditions or perceptions that patients were at low risk.40 A study conducted in California compared patients and nurses perspective regarding universal HIV and HCV screening in the ER and concluded that nurses often negatively misperceived patients experience regarding screening, a situation at risk of complicating implementation of screening programmes.41
Our opt-out rates compared favourably with the literature. A systematic review published in 2017 reported an opt-out of 56% among 75 155 patients tested for HIV while we observed an opt-out of 25% in our study.10 Of note, several of these studies required written consent, even for an opt-out, which was not our case. The absence of consent prevented us to collect detailed information on patients who opted-out. On the other hand, this allowed our evaluation to be as close as possible to the real conditions in which a universal screening programme would be conducted outside of a research project.
The main limitation of our study is generalisability. The CHUM is an urban university hospital for tertiary/quaternary care. Due to its geographical localisation, it serves a large population of people who inject drugs (PWID) and MSM, even for secondary care, and should be representative for these populations who include the majority of HIV and HCV cases in Canada. For example, in 2018, these two populations were representing more than half the new HIV cases in Québec (MSM: 51.1%; PWID: 5.8%; both: 1.6%) and PWIDs represent more than 85% of new HCV diagnosis in Canada each year.28 42 However, our population is less representative of First nations or foreign-born patients.
In conclusion, universal screening of HIV and HCV in the ER is feasible even if the strategy did not lead to the identification of a large number of cases. In the perspective of elimination of AIDS and HCV, each case is important and those we identified might not have had access to screening in other settings. With a CI barely including the cost-effectiveness threshold for HIV, universal screening might not be the ideal screening strategy for this infection in our setting and targeted screening should be evaluated. Considering the higher number of HCV cases identified, universal screening might be adequate, under the limitations that cost-effectiveness threshold has not been established for HCV and that the number of new cases is expected to decrease over time with the availability of HCV treatments and elimination efforts currently ongoing. Finally, cost-effectiveness threshold of coscreening for HIV and HCV is not established but is probably lower than screening for only one condition. These tests can easily be performed together; consequently reducing human resources and blood draw costs. In some setting, adding hepatitis B or syphilis screening might also be considered. In order to take large-scale decision on establishment of screening programmes, this co-screening cost-effectiveness threshold should probably be established.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The project was approved by the CHUM institutional review board (IRB). A waiver of consent was granted by the IRB for the screening portion of the project as it considered the study as the evaluation of a program. For the linkage-to-care portion of the project, participants signed an informed consent form. All research procedures have conformed to the principles embodied in the Declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge the participation of Danielle Navarre, Catherine Boucher, Chantal Morrisseau and Karell Bossé.
References
Footnotes
Contributors VM-L and CT led the project and reported substantial contributions to the conception, design, acquisition, analysis, interpretation of data and drafting the work. J-GB, IA, JL, JC, EJ, DH and GL contributed to the conception, design, analysis and interpretation of data for the work and critical revision of the manuscript (initial and revised versions) for important intellectual content. EJ and DH additionally contributed to data acquisition. All authors approved the final version of this manuscript and agreed to be accountable for all aspects of the work. VM-L is the guarantor.
Funding This study was funded by the Ministère de la Santé et des Services Sociaux du Québec (grant number : N/A), Gilead Sciences (grant number : N/A) and Merck (grant number : N/A). VM-L is funded by Chercheur-boursier clinicien Junior 1-FRQ-S.
Competing interests VM-L: research grants/consultant: Gilead Sciences, Merck, Abbvie, research material: Cepheids; J-GB: research grants: GlaxoSmithKline, Merck, and Gilead Sciences, consultant: ViiV Healthcare, Merck, and Gilead Sciences; CT: research grants: ViiV, Merck, Gilead Sciences, consultant: Merck, Gilead Sciences, ViiV. IA, JL, JC, EJ, DH and GL have no competing interests to disclose.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.