Article Text

Abstract
Introduction Obesity is a global health issue that impacts quality of life. A calorie-restricted diet with high-intensity consultation provided via the internet may be an effective way to lose weight. The objective of this study was to assess the effectiveness of a practitioner-guided, mobile internet-based low-energy dietary intervention in overweight and obese populations in China.
Methods and analysis This open-label randomised controlled trial enrolled 220 overweight and obese adults aged 18–70 years who met the inclusion criteria. Participants were assigned to the control group (n=110) or trial group (n=110). The trial group will be enrolled in the MetaWell programme, a weight loss programme using diet replacement products, wireless scales and a mobile phone app. Participants in the control group will receive paper material containing a sample diet for weight loss. The follow-up period will be 1 year, and measurements will occur at 3, 6 and 12 months. Dual-emission X-ray absorptiometry and abdominal quantitative CT will be performed to estimate the percentage of overall body fat and areas of visceral and subcutaneous fat, alongside several cardiometabolic measurements. The primary outcome of this study is the change in body mas index (BMI) at 6 months after enrolment. A mixed-effects model will be used to compare BMI and body fat changes between the two groups.
Ethics and dissemination This study was approved by the ethics committee of the Hospital of Chengdu Office of the People’s Government of the Tibetan Autonomous Region. Advertisements for recruitment will be sent via official accounts using WeChat. The results will be disseminated via publications in academic journals and our clinic. Our study group will maintain contact with the participants to inform them of the study findings.
Trial registration number ChiCTR1900021630.
- protocols & guidelines
- clinical trials
- nutrition & dietetics
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, this is the first study to evaluate the effectiveness of a programme combining a mobile phone app, diet replacement product, wireless scale and high-intensity guidance from professionals for weight loss in overweight and obese individuals.
For more precise results, this study will use dual-emission X-ray absorptiometry to evaluate body fat, unlike most studies that use bioimpedance spectrum analysis to evaluate the amount of body fat, which may underestimate the body fat of participants.
Since the effects of subcutaneous adipose tissue (SAT) and visceral adipose tissue (VAT) on health are different, we will use quantitative CT to evaluate the changes in SAT and VAT during the intervention period.
The follow-up period may be insufficient to observe the long-term effects of this weight loss programme.
Introduction
Obesity has become a global public health issue in recent years. According to the WHO, more than 1.9 billion adults worldwide were overweight in 2016, a number which has nearly tripled since 1975.1 Obesity is associated with a poorer health-related quality of life, including physical impairments such as back pain,2 as well as an elevated risk of cardiovascular diseases, diabetes, hypertension and elevated mortality. In China, the Chinese Residents Nutrition and Chronic Disease Status Report 2015 revealed that the prevalence of overweight and obesity was 30.15% and 11.9%, respectively.3 The economic burden caused by overweight and obesity in China in 2010 alone was estimated to be US$12.97 billion.2
Dietary interventions are a commonly used strategy for weight loss. Guidelines for managing overweight and obese adults recommend a calorie-restricted diet that limits daily energy intake to 1200–1500 kcal/day for women and 1500–1800 kcal/day for men, thereby providing an energy deficit exceeding 500 kcal/day.4 Despite modification of dietary patterns, in-person high-intensity consultations provided by a trained practitioner can significantly promote the effectiveness of a weight loss programme.5 However, in middle-income countries such as China, high-intensity face-to-face consultations are impractical. With the development of information technology, commercial programmes that provide individualised feedback via the Internet to help patients lose weight have emerged. Evidence suggests that long-distance, internet-based high-intensity interventions are effective.4 A meta-analysis of internet-delivered interventions providing personalised feedback for obese adults revealed that those receiving Internet-delivered personalised feedback lost 2.13 kg more weight.6 The effectiveness of various dietary interventions and food replacement programmes for weight loss are well documented, although they involve face-to-face interventions or human contact.6–9 However, evidence from randomised trials combining internet-delivered programmes enhanced by monitoring of body weight using electronic scales is scarce. Furthermore, to the best of our knowledge, no trials to date have assessed the effectiveness of an online intervention that includes food replacement and remote weight monitoring.
The MetaWell programme (Weijian Technologies, Hangzhou, China) is a commercial weight loss programme in China that integrates prepackaged food, online guidance and a wireless home scale and has been proven to be effective in a previous retrospective study. The results demonstrated that at 120 days after programme initiation, 62.7% of participants had lost at least 5% of their initial weight.10 However, further investigations of the effects of this type of intervention on body composition, fat distribution and improvements in metabolic issues, such as abnormal blood pressure and insulin resistance, warrant further investigation.
We will conduct a randomised controlled trial to determine the effects of a practitioner-guided, mobile internet-based low-energy dietary intervention on body weight, body composition, body fat and metabolic profiles in overweight and obese Chinese populations. Further, we aim to evaluate the safety profile of the programme. This trial was commenced on 11 April 2019.
Methods and analysis
Overview of study design
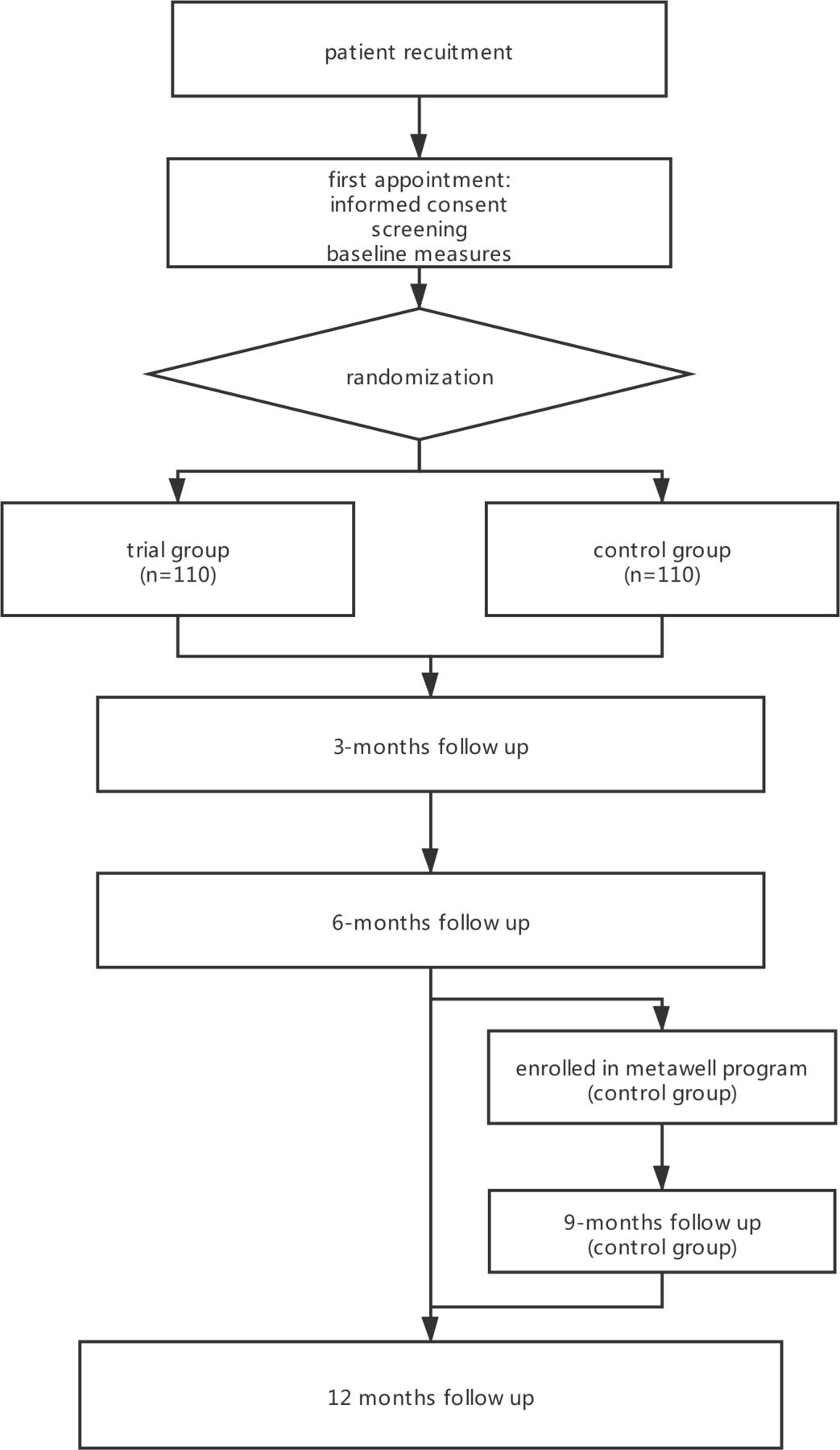
This trial is a single-centre, open-label, randomised controlled trial that aims to explore the effects of the MetaWell programme on weight loss, fat loss distribution, and cardiometabolic parameters. A total of 220 individuals aged 18–75 years living in Chengdu city, Sichuan Province, China, will be enrolled and randomly assigned at a 1:1 ratio to the intervention and control groups. This study uses a two-arm parallel design with an extended follow-up period of 1 year. The flowchart and schedule of this study are presented in figure 1 and table 1. Participants will receive a Metawell programme or general diet education. The intervention and follow-up periods will be 6 months. For ethical purposes, the participants in the control group will also receive the Metawell programme, and an extended follow-up will be conducted during the 9th (only for participants in the control group) and 12th month after enrolment.
Study schedule
Flowchat through the study
Recruitment and informed consent
We will disseminate advertisements containing our contact information to recruit participants via various social media platforms through their official account on an instant messaging app (WeChat). Appointments will be made with overweight and obese individuals who are willing to participate in our study. A trained research nurse will provide the participants with detailed information about this study. After informed consent is signed, the initial screening for eligibility criteria and baseline measurements will be performed. The inclusion and exclusion criteria are as follows:
Inclusion criteria
Participant’s age is between 18 and 70 years old and 25≤body mass index (BMI)<40 kg/m2, with at least one condition from the following list: history of hypertension, systolic blood pressure >120 mm Hg or diastolic blood pressure >80 mm Hg; abdominal circumference >96 cm for men and >90 cm for women; fasting triglycerides>1.69 mmol/L; history of type 2 diabetes mellitus managed with lifestyle (not on insulin or oral medications) or fasting blood glucose >5.6 mmol/L; HDL cholesterol <1.04 mmol/L for men and <1.3 mmol/L for women.
Exclusion criteria
Participants with one or more conditions listed below are considered unsuitable for participation in the programme and will be excluded: history of coronary artery disease; diabetes mellitus managed with insulin or any oral hypoglycaemic pill for diabetes; glucose intolerance or fasting glucose ≥8 mmol/L; congestive heart failure; familial hypercholesterolaemia, including familial hypertriglyceridaemia; fasting low-density lipoprotein cholesterol >4.2 mmol/L; fasting triglycerides>6.8 mmol/L; current use of lipid-lowering agents; history of hypothyroidism, Cushing’s syndrome, eating disorders and/or gout in the past 6 months; confirmed episodes of hypoglycaemia, pregnancy, advanced liver disease, renal insufficiency or any other major chronic medical condition; and smokers who plan to quit smoking in the following 12 months. Participants with hypertension will be included only if they take <3 antihypertensive medications, do not change the dose of their blood pressure medications in the preceding month and have systolic blood pressure <160 mm Hg and diastolic blood pressure <100 mm Hg. Individuals who are unable to use smartphones will be excluded.
Sample size
Based on the Doctor referral of overweight people to low energy total diet replacement treatment (DROPLET) study,7 we hypothesised that the absolute difference in weight loss between the trial and control groups will be at least 4 kg in weight, with a SD of 9 kg. Therefore, 100 participants per group will provide more than 90% power to detect this difference with an alpha error of 0.05. The required sample size was determined to be 110 participants per group, considering an estimated 10% attrition rate.
Randomisation
All participants will be randomly assigned to the trial or control groups at a 1:1 ratio. A list of randomisation numbers will be generated using R, and the allocation results will be sealed in an opaque envelope. After completion of baseline measurements, the randomisation envelope will be unsealed by the practitioners responsible for participant allocation.
Interventions
The MetaWell programme is a remote weight loss programme that consists of a free mobile application combined with a wireless home scale, customised nutrition programme and weight management coach (figure 2). Once enrolled in the programme, participants will receive advice from the weight management coach certified by MetaWell and up to three MetaWell biscuits daily, along with a selection of healthy recipes (such as seaweed soup, skimmed milk, spiced beef, grains, vegetables, etc). The nutritional information of the biscuits is presented in table 2. Participants are required to measure their weight and urinary ketones daily. The weight management coach will measure, monitor, and evaluate participants’ body fat parameters and ketone production to adjust the programme and meal plan accordingly to ensure that the programme is effective and safe.
Nutritional information of Yufit biscuits

{kind=link}
{kind=link}
MetaWell program and a sample of recipe for participants.(a.Three main components form the closed loop system of Metawell programb. One out of seven sample recipes for participants,)
Trial group
After randomisation, the participants will be enrolled in the MetaWell programme (Weijian Technologie, Hangzhou, China). The programme comprises three stages: (1) weight loss stage (0–3 months), (2) continued weight loss transitioning to a weight maintenance stage (3–6 months) and (3) extended follow-up stage (6–12 months)
Weight loss stage (0–3 months)
After being assigned to the trial group, participants will download an app on their mobile phones and will be provided with a home scale, urine ketone testing strip and Yufit biscuits. Participants will be instructed on how to use the scale to monitor changes in body weight and fat. Participants will be randomly assigned to a particular practitioner. Participants will be required to monitor their body composition and urine ketone levels using a scale and test strip daily. Data will be uploaded to their mobile phones and transmitted to their practitioners. All practitioners have medical backgrounds and are trained by the MetaWell group. Practitioners will provide guidance on required dietary adjustments via the app and will make necessary adjustments to the participants’ daily diet based on their health condition, such as urine ketones, hypoglycaemia and rate of weight loss. The daily energy intake is typically 800–1200 kcal/day.
Weight maintenance stage (3–6 months)
After 3 months, the Yufit biscuits will no longer be used routinely in the diet. Participants will still be required to monitor their weight and upload the data. When noticeable weight regain is detected, the practitioner will initiate 2–3 days weight loss intervention using the same protocol as that in the weight-loss stage to maintain the participant’s body weight.
Extended follow-up stage (6–12 months)
After 6 months, practitioners will not provide advice but will instruct participants to monitor their body weight weekly and maintain their body weight autonomously.
Control group
Printed educational material containing general guidance on a routine diet and sample diet for weight loss (1500 kcal/day for men and 1200 kcal/day for women) will be provided to participants. Details are provided in table 3. Face-to-face education will occur only once, and participants will be instructed to follow this diet to lose weight and monitor their weight and urine ketone levels once a week. If their urine ketones become positive, participants will be informed to contact the study organisers. Their recent diet will be reviewed and advice on relevant dietary adjustments will be provided.
Diet sample for participants in the control group
After 6 months, participants in the control group will be enrolled in the MetaWell programme, including a 3-month weight loss stage and 3-month weight maintenance stage, as described above.
Outcomes
The primary outcome of this study is the between-group difference in the change in participants’ BMI after 6 months of follow-up. The study has four secondary outcomes: (1) proportion of participants losing 5% of their body weight; (2) changes in total body fat and distribution of abdominal visceral adipose tissue and subcutaneous adipose tissue given that visceral adipose tissue is closely associated with health in obese patients and a decrease in body weight is not equal to a loss in body fat; (3) changes in systemic inflammation reflected by high-sensitivity C reactive protein (hs-CRP) preintervention and postintervention and (4) mid-term and long-term effectiveness of the MetaWell programme for improving systemic blood pressure, abdominal obesity, blood glucose and blood lipids.
The exploratory outcome of our study is the weight loss effect of the MetaWell programme at 1 year for participants in the intervention group. The safety outcomes of our study are changes in serum vitamin levels and changes in liver and renal function.
Assessment and follow-up
Eligible individuals who meet the criteria and consent to participate in the clinical trial will undergo a baseline assessment. Follow-up assessments will be performed at 3, 6, 9 and 12 months after enrolment. A summary of the follow-up assessments is presented in table 1. Group interventions will be masked in the data provided to the assessor to avoid bias. To ensure the quality and reliability of the data, all follow-up measurements will be performed by a nurse who is specially trained by our team or qualified lab.
Baseline information
All participants will complete a questionnaire on sociodemographic and medical information, including age, sex and medical and surgical history in baseline assessments.
Anthropometry
At baseline and during every follow-up assessment, body weight will be measured to assess weight changes. Measurements will be performed with an ultrasonic height-weight scale (DHM-200, Dinghengkeji, Hennan, China). Participants will be weighed barefoot and without greatcoats. Body height and weight will be recorded to the nearest 0.1 cm and 0.1 kg, respectively. To ensure measurement accuracy, the scale will be calibrated using a 20 kg standard weight every month. Waist and hip circumferences will be measured at every assessment. Measurements will be performed by two nurses trained by our study group. Waist and hip circumferences will be measured approximately 3 cm above the navel and at the widest part of the hip, respectively. Participants will be instructed to keep their arms down and relax during measurements. BMI and waist-to-hip ratio will be calculated.
Blood tests
At every follow-up visit, a 30 mL fasting blood sample will be collected from each participant using vacuum tubes, including procoagulation tubes, for various blood tests listed below:
Liver function, renal function, blood lipids and CRP: Elevated alanine aminotransferase (ALT) is the most commonly used biomarker of liver dysfunction. Given the association between obesity and non-alcoholic fatty liver disease (NAFLD) and based on reports that bariatric surgery can improve NAFLD in obese patients with weight loss,11 we will measure the liver function of participants at every follow-up. In addition to NAFLD, hyperuricaemia, hyperlipidaemia and body inflammation are closely linked to overweight and obesity. To investigate whether these symptoms will improve with weight loss, we will assess renal function and blood lipids at every follow-up to observe changes in ALT, urine acidity and blood lipids during the programme.
Blood glucose and insulin levels: Obese patients are more vulnerable to glucose intolerance.12 Although diabetic patients will not be enrolled in our programme, the effects of the weight loss programme on insulin resistance in participants will be measured. Fasting blood glucose and insulin levels will be measured. Homeostatic model assessment will be used for assessing insulin resistece (HOMA2-IR) and will be calculated using the HOMA2 calculator,13 and changes in HOMA2-IR will be analysed.
Haemoglobin and vitamin levels: Safety assessments of weight loss programmes are crucial, and there are many reports on the side effects of weight loss surgery.14 15 The most common symptoms are vitamin deficiency and anaemia. However, it remains unclear whether dietary interventions are associated with a lack of nutritional intake and similar side effects. Therefore, we will assess levels of haemoglobin and vitamins A, B6, B12 and 25-(OH)-D during the programme.
Questionnaires
To analyse the impact of our weight loss programme on general quality of life, physical activity and lifestyle, a set of questionnaires will be administered at every follow-up assessment. The short form (SF-36) health survey is a commonly used questionnaire to assess quality of life and has been validated in the Chinese population.16–18 To assess changes in physical activity and self-efficiency, the international physical activity questionnaire (IPAQ)19 and Weight Efficacy Lifestyle short-form questionnaire will be employed.20
Given that the feeling of hunger may impact the adherence and feelings of participants, a Visual Analogue Scale will be used to investigate the feeling of hunger at different time points before and after each meal in each participant.
Dietary assessment
Obese individuals enrolled in weight loss programmes tend to regain their weight 1 or 2 years postintervention.21 We hypothesise that this could be due to the failure of the programmes to change dietary patterns. Therefore, we plan to conduct dietary assessments at baseline and 6 months after enrolment to determine whether our programme alters the dietary patterns of participants and to examine the relationship between dietary changes and weight regain. A 24-hour dietary recall, which is the standard method for performing dietary investigations and is widely used globally,22–24 and short Food Frequency Questionnaires (FFQs) will be used. The FFQ used in this study was designed to conduct nutritional investigations in Chengdu city.25
Body composition
The main goal of weight loss is to reduce the amount of body fat. Therefore, to investigate the effect of our weight loss programme on body fat, dual-emission X-ray absorptiometry (DXA) will be performed using the GE Lunar Prodigy scanner26 to assess body composition. Total body fat, leg fat and upper body fat will be measured. The percentage of body fat will be calculated.
Visceral adipose tissue is closely associated with various symptoms, including hypertriglyceridaemia,27 cardiovascular diseases28 or metabolic syndrome.29 Considering the impact of visceral adipose tissue on human health, we will investigate changes in visceral adipose tissue with weight loss. We will use 16-slice spiral CT (TOSHIBA Aquilion 16, Japan) to scan and analyse slices between L2/L3 to evaluate the amount of visceral fat and subcutaneous fat in each participant using QCTPRO software.30 DXA will be performed at baseline, 6 months and 12 months. CT will be performed at baseline and 6 months. We will also measure the skinfold thickness of the triceps, subscapular crest and iliac crest at every follow-up assessment.31
A 24-hour blood pressure monitoring
Participants will be required to undergo 24 hours blood pressure monitoring at baseline and 6-month follow-up using a Welch Allyn ABPM 6100/7100 blood pressure monitor. Average and SD of blood pressure during the daytime and at night will be recorded.
Adverse events
Expected adverse events of the weight loss intervention include hypoglycaemia, menstrual disorder, constipation and dizziness. At every follow-up, participants will be asked if they have experienced the aforementioned side effects. All adverse events will be recorded.
Data management
Paper case report forms and reports of each measurement will be collected as original data. These data will be entered into an electronic data collection system. Every month, the missing data, outliers and other types of incorrectly entered data will be screened and reported in a monthly meeting of the main research group members. We will assess the raw material of any suspicious data and amend any incorrectly entered data. On conclusion of enrolment, a brief report on the data distribution of the two groups will be prepared to assess the efficiency of randomisation.
Statistical analysis
Analysis of primary and secondary outcomes
The intention-to-treat dataset will be used to analyse the primary and secondary outcomes performed by an independent statistician group. Changes in participants’ BMI (primary outcome) and the amount of body fat, abdominal visceral adipose tissue and hs-CRP (secondary outcomes) will be analysed using a mixed-effects model, which includes different intervention groups. Random effects will include repeat measurements on the same participant and individual differences among participants. The proportion of participants who lose 5% of their initial weight will be analysed using Cox regression, Kaplan-Meier survival curves and log-rank test. The data at 6 months will be considered as the main result. Changes in all outcome measurements between baseline and at 6-month follow-up will be analysed. Differences in changes will be assessed using a t-test or χ2 test.
Adjustment
Baseline BMI, sex, age and IPAQ scores of participants will be adjusted. Both adjusted and unadjusted analyses will be performed, and the adjusted result will be considered as the main result.
Comparison of baseline characteristics
After the enrolment of participants is completed, baseline characteristics will be compared between two groups using a t-test and χ2 test.
Sensitivity analysis
The differences in body weight changes of participants in the control group will be analysed using a t-test to confirm the effects of the Metawell programme.
Missing values
Missing values will be implemented using multiple imputation. Both preimputation and postimputation datasets will be analysed. The results of postimputation data will be considered as the main result.
Statistical description and software
The distribution of continuous, normally distributed data will be presented as means and SD. Other continuous data will be presented as medians and IQR. All analyses will be performed using R V.3.5. P values, 95% CIs and the different effects of the two interventions will be reported. Differences will be considered statistically significant at p<0.05.
Patient and public involvement
Patients and the public were not involved in the design, conduct, reporting or dissemination of our research.
Ethics and dissemination
This study conforms to the Declaration of Helsinki. The study has been approved by the ethics committee of the Hospital of Chengdu Office of People’s Government of Tibetan Autonomous Region (Reference ID for ethics approval: 2019-01). Before signing consent forms, participants will be well informed about the benefits and risks of participating in this programme. The trial was commenced on 11 April 2019.
There are two main audiences of this research: the overweight/obese population in China and professionals working in the weight loss field. The results of our study will be disseminated via publications in academic journals and our clinic. Our study group will maintain contact with participants to inform them of the study findings.
Discussion
This study aims to examine the effectiveness of an internet-based, low-carbohydrate dietary intervention programme for improving body weight, body composition, and general metabolic health. Although similar types of programmes have been performed in developed countries, there is a paucity of similar studies in China. In our study, DXA and quantitative CT (QCT) will provide more detailed and accurate data on changes in body fat during the intervention, which may clarify the benefits of a low-carbohydrate diet in obese patients.
In recent years, the effects of diverse dietary interventions on weight loss have been extensively examined. The findings indicate that patient adherence is the most crucial factor. A prepackaged diet replacement product provides a much easier plan to follow. The use of an internet-based platform allows professional practitioners to monitor patient status, have high-intensity contact with patients, and modify their weight loss plan in real time without the need for patients to attend specific facilities. These advantages may improve patient adherence and improve outcomes compared with traditional weight loss programmes.
The main purpose of losing weight is to reduce body fat and improve health and quality of life. Given that weight loss can be due to loss of water, lean mass or body fat, simply observing a reduction in body weight does not necessarily indicate a reduction in body fat and improvements in health outcomes. Accordingly, a key feature of our study is the ability to track changes in body fat. Bioimpedance spectrum analysis (BIA) is the most commonly used method for estimating the amount and percentage of body fat. However, one study reported that BIA overestimated total body lean mass in 93% of participants and underestimated total body fat mass in 90% of participants.32 In this regard, DXA is a more accurate measure of body fat compared with BIA.
To the best of our knowledge, this is the first study to evaluate weight loss resulting from a weight loss programme combining a mobile phone app, diet replacement product, wireless scale and high-intensity guidance from professionals. Moreover, we will employ DXA and QCT to accurately evaluate changes in body fat, visceral adipose tissue and subcutaneous adipose tissue. Nevertheless, this study has several limitations. First, participants enrolled in previous loss programmes tend to regain most of their weight within years. As the follow-up period is 1 year, we will be unable to thoroughly analyse weight regain in our participants. Second, the follow-up period of 1 year is also insufficient to assess the long-term benefits of this weight loss programme, such as reduced risk of cardiovascular events and diabetes onset. Therefore, we will consider a prolonged follow-up period of 2–3 years for participants that agree to stay in our programme in order to observe the long-term effects of our programme.
Ethics statements
Patient consent for publication
Acknowledgments
During the preparation stage of this study, Lin Weihua and Zhang Xiaoyong helped with the coordination between our study group and Metawell company.
References
Footnotes
Contributors XW, YW, LL, AL and FL-J designed the study. XW, YW, YG and CZ are the medical supervisors of this study and are responsible for enrolling participants. SW is responsible for the randomisation, data collection, management and drafting of this manuscript. XW, CZ, YW, LZ and FL-J reviewed and revised the manuscript. XW acts as a gaurantor for this study.
Funding This work was supported by Weijian Technologies.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.