Article Text

Abstract
Introduction A considerable literature implicates prenatal stress as a critical determinant of poor psychological functioning in childhood and beyond. However, knowledge about whether the timing of prenatal stress differentially influences the development of child outcomes, including psychopathology, is virtually unknown. The primary aim of our study is to examine how the timing of prenatal stress differentially affects early childhood regulatory functioning as a marker of psychopathology. Our second aim is to examine the mediating effects of maternal physiological and psychological factors during pregnancy. Our third aim is to examine the moderating effects of postnatal factors on child regulatory functioning. Our project is the first longitudinal, prospective, multimethod study addressing these questions.
Methods and analysis Our ongoing study recruits pregnant women, oversampled for intimate partner violence (a common event-based stressor allowing examination of timing effects), with data collection starting at pregnancy week 15 and concluding 4 years post partum. We aim to have n=335 mother–child dyads. We conduct a granular assessment of pregnancy stress (measured weekly by maternal report) in order to reveal sensitive periods during fetal life when stress particularly derails later functioning. Pattern-based statistical analyses will be used to identify subgroups of women who differ in the timing of their stress during pregnancy and then test whether these patterns of stress differentially predict early childhood self-regulatory outcomes.
Ethics and dissemination Due to the high-risk nature of our sample, care is taken to ensure protection of their well-being, including a safety plan for suicidal ideation and a safety mechanism (exit button in the online weekly survey) to protect participant data privacy. This study was approved by Michigan State University Institutional Review Board. Dissemination will be handled by data sharing through National Institute of Child Health and Human Development Data and Specimen Hub (DASH), as well as through publishing the findings in journals spanning behavioural neuroendocrinology to clinical and developmental psychology.
- non-accidental injury
- community child health
- adult psychiatry
- child & adolescent psychiatry
- perinatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- non-accidental injury
- community child health
- adult psychiatry
- child & adolescent psychiatry
- perinatology
Strengths and limitations of this study
High-frequency assessment of the timing of prenatal stress (ie, weekly assessments) and the timing of postnatal stress (ie, every 3 months).
Multimethod and multisystem assessment of maternal prenatal stress, including assessing psychological and physiological stress, as well as child self-regulation.
Pattern-based statistical analyses to identify subgroups of women who differ in the timing of their stress experiences during pregnancy as differential predictors of infant and early childhood self-regulatory outcomes.
Maternal physiological and psychological factors as potential mediators and postnatal risk and resilience factors as potential moderators.
Power concerns may prevent examination of the role of individual stressors on maternal physiological and psychological functioning and child outcomes.
Introduction
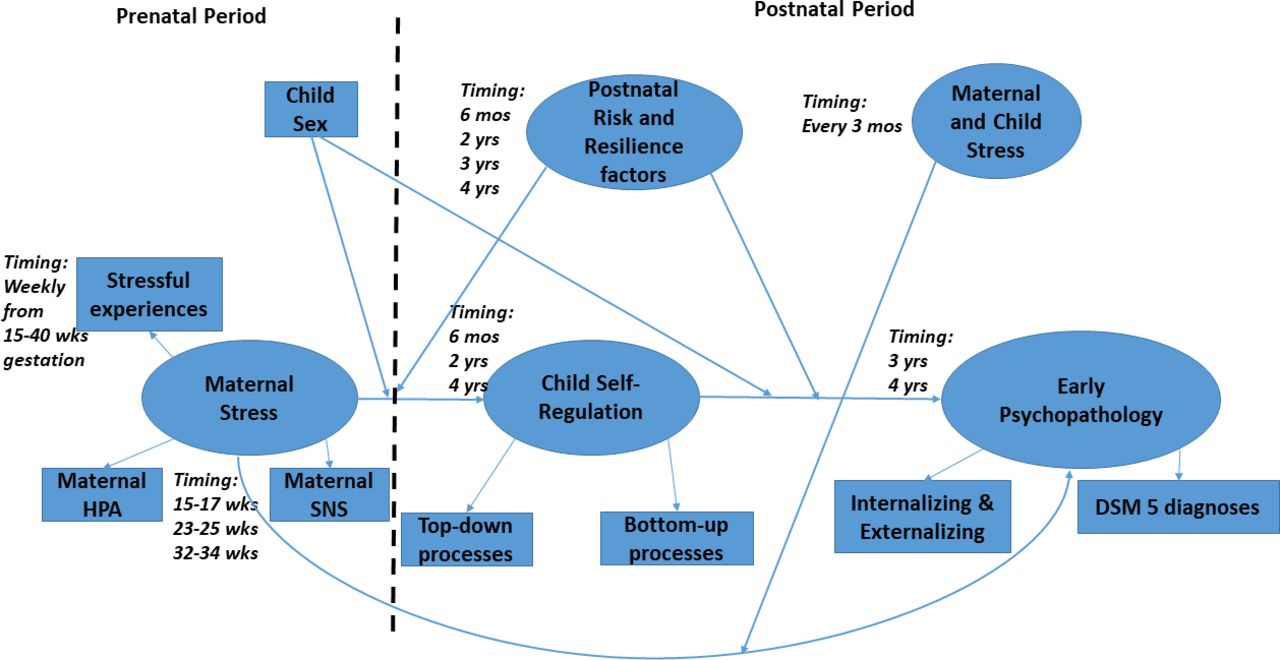
A growing body of research documents the pervasive and persistent effects of prenatal stress on offspring developmental functioning,1 but whether or not the timing of prenatal stress matters for infant regulatory functioning is, as yet, mostly unknown. The prenatal period involves rapid fetal brain development, rendering it a particularly vulnerable period to a host of environmental insults.2 3 Furthermore, because early brain development unfolds in a non-linear fashion with discernible stages,4 it is likely that the brain is more or less vulnerable to being affected or ‘programmed’ by stress during some periods of prenatal life. That is, although many studies have identified the prenatal period as a time of particular vulnerability to stress, the ‘prenatal period’ is surely not unitary. The focus of the Michigan Prenatal Stress Study is to identify how prenatal stress at different time points during pregnancy differentially programmes fetal development and subsequently shapes postnatal child development. From a developmental perspective, we are particularly interested in the child’s emerging capacity for self-regulation. Self-regulation is the foundation for positive, healthy development, whereas self-regulatory deficits may underlie child behaviour problems, including child psychopathology.5 6 The scientific premise of our study is that the neural systems involved in the development of self-regulation have different sensitive periods of susceptibility to prenatal stress (and potentially early postnatal stress), making knowledge about the timing of stress absolutely essential for understanding its effects on child self-regulation and early psychopathology (see figure 1).

{kind=link}
Conceptual and measurement model for the Michigan Prenatal Stress Study. DSM, Diagnositc and Statistical Manual of Mental Disorders - Edition 5; HPA, hypothalamic-pituitary-adrenal; SNS, sympathetic nervous system.
Prenatal programming effects
Mammalian fetuses are embedded in the mother’s biopsychosocial environment, and because fetal stress is problematic to assess on its own, maternal mental and physical stress are often used as proxies. In particular, mother’s hypothalamic-pituitary-adrenal (HPA) axis and sympathetic nervous system (SNS) functioning may affect fetal/child stress physiology and emerging self-regulation. Cortisol released from the adrenal glands exhibits a natural circadian rhythm, with high levels in the morning that decline to an evening nadir. Superimposed on this circadian rhythm is the cortisol that is released in response to acute stressors, which is typically subject to negative feedback loops that quickly bring circulating cortisol levels back to the prestress baseline. When confronted with stressors, the SNS is also rapidly activated to stimulate peripheral organs, including the adrenal medulla. Subsequent adrenal secretion of epinephrine and norepinephrine further heightens physiological activity, including cardiovascular function, to elicit the ‘fight-or-flight’ response. Although some studies suggest that healthy pregnancy is associated with a blunting of the HPA axis and SNS responses to stress,7 8 these systems can become hyper-responsive in the face of chronic stress. This is detrimental to the mother and the fetus because maternal adrenal hormones such as cortisol, epinephrine and norepinephrine readily cross the placenta to reach the fetal compartment, including the fetal brain.9–13 Frequent exposure to high levels of maternal adrenal hormones potentially derails early brain development, with consequences for later infant and child stress regulation,14 15 and places the child at risk for a number of other problematic outcomes.16–18
The effects of prenatal stress on child outcomes are now well established. For example, a recent meta-analysis of 71 studies19 found that the association between maternal prenatal depression and anxiety (often used as proxies for prenatal stress, with caveats noted below) and child behavioural/socioemotional outcomes had an average OR of 1.66 (95% CI 1.54 to 1.79), suggesting that children with prenatally stressed mothers were 1.5 times more likely to have behavioural and emotional problems. However, how the timing of prenatal stress influences child outcomes is much less clear. Differential prenatal stress timing effects have so far been documented in two types of research.20–26 The first includes longitudinal, prospective studies that usually define stress as maternal mental health symptoms, and the second type includes retrospective studies of highly intense, rare events during the pregnancy (eg, 9/11 attacks, Chernobyl nuclear disaster). However, the methodological approaches used in these studies, including the lack of frequent assessment of stress and/or the retrospective approach, limit the precision of findings related to timing of prenatal stress. While this and other prior research demonstrate that prenatal stress impacts fetal development/programming, our study proposes two major innovations and significant contributions that build on the prior work. First, we are assessing prenatal stress in a granular fashion by assessing stress weekly, with a range of stressors from chronic (eg, poverty) to episodic (eg, intimate partner violence (IPV)). We oversampled for pregnant women exposed to IPV because it is a common traumatic stressor during pregnancy.27 The episodic stressor assessment (eg, weekly exposure to IPV and other episodic stressors) allows us to examine the timing of prenatal stress as an event-based stressor that will vary in its week-to-week occurrence within and between women. Second, we have implemented innovative and multimodal methods of assessing prenatal stress: (1) self-rating via smartphones with weekly questions sent by text/email to our pregnant participants, (2) three in-person interviews about women’s stress and mental health functioning, and (3) the collection of mother’s saliva to assess both circadian and acute laboratory stress-induced levels of cortisol and alpha-amylase as markers of the HPA axis and SNS, respectively. Thus, our study is building a theoretical model focused on a biopsychosocial pathway from the timing of mother’s prenatal stress to child self-regulation, understood to be the basis for developmental success or problems, as mediated by the mother’s psychological and physiological functioning.
Child self-regulation
Self-regulation has been described differently by various researchers.5 6 28–31 In our research, we use self-regulation as the overarching term for multisystemic, inter-related and transactional intrinsic developmental processes that help children modulate their cognitive, affective and behavioural response to internal and external experiences.29 Self-regulatory capacity develops from infancy to early childhood and can be differentiated into top-down cortically mediated components and bottom-up subcortically mediated components.6 Each of these components underlying self-regulation has a typical developmental pattern beginning during prenatal life. During early childhood, day-to-day experiences with parents shape children’s self-regulatory capacities and help them learn to self-regulate in times of external and internal distress.32 If these parental experiences are suboptimal, due to depression, life stress and family violence, the child’s developing capacity for self-regulation may be impaired. Between ages 3 and 5, children typically develop increased capacity for independent self-regulation. Thus, it is at this age that early signs of psychopathology, such as internalising/externalising behaviours and early diagnoses, become evident based on deficits in one or more aspects of self-regulation.6 33 This is also the earliest age when externalising and internalising behaviours demonstrate continuity with psychopathology across later childhood and adolescence.34 35 In the extant literature on the effects of prenatal stress on early childhood functioning, child outcomes are typically limited to HPA axis activity and subjective maternal report of child behaviour problems/psychopathology. Importantly, our conceptualisation of child self-regulation as an early marker of child psychopathology includes an assessment of six domains of self-regulatory functioning (HPA axis stress reactivity, SNS stress reactivity, heart rate variability (HRV), impulsivity, negative affectivity and executive functioning) using multiple methods including salivary analytes, heart rate monitoring, behavioural observation, child tasks and maternal report.
Postnatal factors as moderators
Finally, the effects of the prenatal stressors on early psychopathology must be considered in the context of postnatal risk and resilience factors. Prenatal stress can increase sensitivity to the postnatal environment.36 37 In fact, the timing and severity of prenatal stress may predispose offspring to be particularly vulnerable to postnatal environmental stressors due to effects on offspring stress physiology, including the HPA axis and SNS.3 Furthermore, allostatic overload due to chronic stress during early childhood is linked to a variety of mental health problems.38 39 Typically, postnatal stressors are measured only annually or biannually by researchers. However, given the rapid development of self-regulation during the first 4 years of life, we believe that assessing in smaller epochs will provide more complete data about postnatal stressors. This, in turn, will facilitate a better understanding of when and what types of stress lead to early psychopathology. In the extant literature, interactions between prenatal and postnatal stress are rarely addressed, and when done so, the typical assessment of stressors is limited to one or two specific stressors prenatally and the same ones postnatally, rather than broadly assessing a range of possible stressors at both time periods. Our study addresses these limitations by assessing postnatal stressors every 3 months, as well as assessing the same broad range of chronic and episodic stressors that we assess during pregnancy. At our postnatal visits, we also assess, using questionnaires and observational methods, a range of resilience factors such as sensitive parenting, maternal coping strategies and maternal social support that are likely to reduce the effects of prenatal stress on child regulatory processes.
The current study
Our primary research questions are as follows: First, how does the timing of prenatal stress affect infant and early childhood self-regulatory outcomes, such that some outcomes are affected by relatively early pregnancy stress and others are affected by mid-pregnancy and/or late-pregnancy stress? Second, how do maternal physiological and psychological factors mediate the association between the timing of prenatal stress and infant/early childhood self-regulatory outcomes? Finally, do postnatal risk and resilience factors moderate the effects of the timing of prenatal stress on infant/early childhood self-regulatory outcomes? As a corollary to this final research question, we also ask if the timing of postnatal risk and resilience factors plays a role in moderating the timing of prenatal stress on child outcomes.
In sum, addressing questions about the timing of prenatal stress will fill an important gap in the scientific understanding of how prenatal stress affects child self-regulation and early psychopathology. Delineating the association between sensitive periods during pregnancy and child outcomes will help future researchers better identify the cellular and molecular mechanisms, as well as the brain structures, underlying altered neurobehavioural development. Identifying sensitive prenatal periods during which exposure to stress may be particularly detrimental for children could also shape new recommendations for maternal risk screening during pregnancy as well as the timing of prenatal interventions. Ultimately, we expect our findings to contribute to optimally timed and therefore better informed preventative interventions for the millions of women and their children affected by very early-life stress.
Methods and analysis
Participants
Our longitudinal, prospective study is funded by the US National Institute of Child Health and Human Development and begins during early pregnancy and continues until the children are 4 years old. The Michigan State University Institutional Review Board approved this study in October 2016. Recruitment and data collection began in 2017, and the study is projected to complete data collection in 2026. Participants are recruited from three metropolitan areas in Michigan as early as possible in pregnancy, with the first laboratory assessment conducted between 15 and 17 weeks. Women are enrolled in the study if they meet these initial inclusion criteria: (1) English fluency, (2) 18–34 years old, (3) without endocrine disorders, cancer or cancer therapy that could affect stress system hormones,40 and (4) in a heterosexual romantic relationship for >6 weeks during the current pregnancy to increase the probability of relationship-related stressors in the sample. We are focusing recruitment on high-risk women with prenatal stress, including IPV and poverty (ie, below Medicaid cut-off), and thus have a sample with a range of both chronic and episodic stressors as well as risk and resilience factors. We expect to recruit 335 women: approximately 50% Black women, 45% White women and 5% of other racial/ethnic backgrounds, reflecting the demographics of the most at-risk women in our three metropolitan recruitment regions in Michigan (Lansing, Ann Arbor, Detroit). Women are recruited through existing relationships between the research team and various local organisations as well as by placing flyers in strategic areas targeting low-income and high-risk pregnant women (eg, recipients of government support). We also recruit from an Ob-Gyn Perinatal Registry affiliated with one of our universities, which annually enrols ~750–1000 pregnant women with a range of demographic risk, and by ads on Facebook and other social media in all three metropolitan areas. Assessments are conducted at offices near each of the three recruitment sites. The physical set-up and equipment used in the assessment offices are equivalent across all three sites.
Patient and public involvement
The public was not involved in the study design. However, we intend to disseminate this study widely, including sending study findings to the participants in our research through regular newsletters after data analysis is under way and results are ready for dissemination.
Design considerations
A comprehensive list of constructs and the timing of assessments are listed in table 1. Several unique aspects of our design are described below.
List of measures and assessment timing
Timing of assessments
One of the most unique components of the research design is the strong attention to timing for the stress assessments. We assess stress weekly throughout pregnancy, beginning at approximately 15 weeks’ gestation. We assess the occurrence and perceived stress from multiple stressors, including psychological, physical and sexual IPV victimisation as well as perpetration; food insecurity; financial problems; neighbourhood violence exposure; non-violent family conflict; and overall stress level for the week. These are assessed by a questionnaire sent to our participants by text or email to a smartphone; if the participant does not have a smartphone, one is provided to her with minutes on a plan that she will be able to use for any purpose throughout the study period. Following the child’s birth, we continue to use the smartphones to assess these stressors, with the addition of child-focused stressors (eg, accidents, hospital/emergency room visit, saw someone get hurt, separated from loved ones for more than a few days) once every 3 months until the last assessment when the child turns 4 years of age. This frequent assessment of stress allows us to develop subgroups of participants who differ in the timing of their exposure to stress. This will allow us to determine the differential effects of stress timing on outcomes. Due to the rapid brain growth during fetal life,41 42 this high-frequency prenatal sampling is essential. Human brain maturation of course continues to occur postnatally, but does so over a longer period of time, thus we lengthened the epochs for assessment of stress to every 3 months. This is much longer than the weekly epoch we used in the prenatal period, but is much shorter than the 1–2 years between assessments typical for previous developmental studies. Similar to the prenatal period, we expect that in postnatal life there are likely specific epochs that involve higher levels of susceptibility to postnatal factors. This high-frequency sampling both during the prenatal and postnatal periods will allow us to examine how the timing of prenatal and postnatal stress might interact to produce differing effects on self-regulation and indicators of emerging psychopathology in 4 year-olds.
Maternal assessments
We are interested in understanding both physiological and psychological/behavioural mediators of the effects of prenatal stress on infant and child development. Thus, at all three pregnancy assessments, we assess both challenged and diurnal maternal salivary cortisol and alpha-amylase as markers of the HPA axis and SNS functioning, respectively.43 44 For the challenged HPA axis and SNS assessments, we use the Trier Social Stress Test45 and collect saliva at baseline, 5 min, 20 min and 40 min post-Trier. The women passively drool through a straw and the saliva collected in microcentrifuge tubes. At all prepartum and postpartum assessments, women report on their mental health,46–48 IPV,49 parenting,50–52 social support53 and life stress.54 All postpartum assessments include behavioural observations of parenting in a mother–infant/child-free play,55–57 as well as high-frequency HRV assessed in mothers during a baseline 2 min period when no task is occurring and during the mother–infant/child-free play interactions.58 59 We use the standard placement on the body for HRV assessment using three leads attached to the upper chest.
Multimethod approach to assess child self-regulation and early markers of psychopathology
We assess the children three times—first at 6 months, then at 2.5 and at 4 years of age. Because self-regulation involves both top-down and bottom-up processes with physiological, behavioural and emotional components, our child assessments involve multiple methods. We use behavioural observation of the fear and anger paradigms from the Laboratory Temperament Assessment Battery (LabTAB60 61) with the child’s reactions coded in 10 s epochs using standardised procedures. The emotion reactivity codes are latency to distress and intensity of facial, vocal and bodily distress. The regulatory behaviour codes are gaze aversion, looks toward mother, struggling, self-stimulation and tension release. Physiological markers of infant/child salivary cortisol and alpha-amylase, assessed using the LabTAB as the stressor, are collected at baseline, 5 min, 20 min and 40 min poststressor.62–64 Saliva collection from the child is done by the mothers using a swab to collect their child’s saliva and then placing the swab in a tube. In addition, a heart rate monitor worn by the children collects high-frequency HRV at resting baseline, while interacting with their mothers,65 and during the LabTAB stress tasks.66–68 The observational LabTAB stress tasks are done in a room away from the mother, with two exceptions when the tasks require maternal presence. For executive functioning, behavioural observations of impulsivity and effortful control are assessed. Impulsivity is assessed with a delay task (gift or snack depending on the age).69 70 Effortful control is assessed with an age-appropriate Stroop task.71–73 The mother remains in the room for the executive functioning tasks in order not to cause attachment distress for the child. Mothers report on the child’s temperament at each age74–76 and children’s behaviour problems.77–79 Finally, at age 4, we also use a semistructured diagnostic interview conducted with mothers over the phone to assess both symptoms and categorical diagnoses of child psychopathology80
Data analysis
We will use a pattern-based approach81 to identify subgroups of women who differ in the timing of stress, both in terms of levels and chronicity, during pregnancy. For example, some women may experience high levels of stress across all of pregnancy, whereas other women may experience high levels only during particular weeks. This is a data-driven approach in which subgroups are identified by patterns observed in the data. Such an approach differs from traditional variable-based models of stress in pregnancy that can obscure critical differential stress experiences under the modelling assumption that the level of stress and chronicity of stress are the same for all women and all stressors. Instead, this approach will take into account that stress exposure varies both between and within individual women across pregnancy.
After identifying subgroups of women that differ in timing of stress during pregnancy, we will test whether these patterns of stress experiences differentially predict infant and early childhood self-regulatory outcomes. To do this, we will use the patterns identified as latent subgroups to test for group differences in our outcomes. We will also test maternal physiological and psychological factors as potential mediators of these associations. Finally, we will assess whether postnatal risk and resilience factors moderate these mediational processes, which include timing of postnatal stressors. To do this, we will construct bootstrapped CIs to test mediation and moderated mediation models.82
Power analysis
The mediation model for predicting the outcome variables will be used as a basis to determine the necessary sample size. As is the case for most studies on power analysis for mediational processes, we will focus on models for continuous variables. The sample size required for a power of 80% ranges widely, depending on the test used and the effect examined.83 To determine an approximate required sample size, we will focus on joint significance. We assume that our measures will stay at their current high levels of reliability (eg, 0.78–0.8984). Across the 16 conditions studied by Fritz and Mackinnon,83 the required sample sizes range from 58 to 530. For Sobel (conservative) test, the range is 42–667. Considering our variables have high levels of reliability, we are confident that our sample of 335 mother–child pairs will allow us to find effects with a power of 0.80 even when the effects are no larger than medium size. When using Baron and Kenny’s approach,85 smaller sample sizes suffice, or smaller effects become detectable. These sample sizes apply to manifest variable mediator analysis. To obtain a power of about 0.80, for an R2 of the dependent latent variable of 0.45 and a precision of 0.61, a sample of about 150 mother–child pairs is needed.86 Our proposed sample size of 335 allows us to discuss even smaller R2 values. For these, although the required sample size is larger, when latent variables have more than four indicators, the required sample is reduced.86 For additional latent variables (see figure 1), the required sample will increase in size. Therefore, and considering the complexity of our models, a proposed sample size of 335 allows us to estimate our models with sufficient statistical power.
Ethics and dissemination
Our study is about stress and involves women with a variety of stressors that include IPV, poverty and mental health problems. It is particularly important that we do everything possible to minimise the risks to our participants. Women sign informed consent before each interview and consent for their child at the postnatal interviews. As noted earlier, the Michigan State University Institutional Review Board approved this study, including consent, measures, procedures and risk management. We manage risks to participant safety in several ways. At each interview, the interviewer examines the depression scale for the self-harm question, and if it is endorsed, one of the licensed mental health practitioners on the study is alerted and the participant is assessed for suicidality and referred to appropriate mental health resources as needed. If during an interview, either the participant or the project staff is concerned about the woman’s safety, the interview is ended and we assess whether the woman is able to continue in the study in a safe manner. For the weekly and every 3-month assessments that are completed on the woman’s smartphone, we have installed an option to hit an ‘exit’ button on the phone that will remove her from the questionnaire website. This was a safety measure meant to protect the woman should she become concerned that someone was observing her or reading her responses. The risks to the child participants in this study are minimal. There is potential that project staff could observe or be told about incidents, such as maltreatment, that are mandatory reportable by state law to Child Protective Services. The staff is trained in guidelines about what types of incidents are mandatory to report and how to report, and when needed, appropriate actions are taken.
At the conclusion of the study, we will deposit the questionnaire data, observational codes and biomarker data in the Institute of Child Health and Development Health data repository (DASH - Data and Specimen Hub). We intend to publish the primary findings from the study in journals that span the disciplines in which we are working, including developmental psychology, clinical psychology, behavioural endocrinology and psychiatry. Other papers examining hypotheses that are less central to the primary aims will be published prior to completion of the entire study, as many of these will involve cross-sectional analyses of early waves of data or longitudinal examinations of only the early waves of data collection. As noted above, we will also disseminate findings to our participants through regular newsletters, once the data are prepared and analysed.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @AmyKNuttall
Contributors AAL, GAB, JL and MM conceptualised and designed this study and developed the primary aims and hypotheses. AKN primarily conceptualised the data analysis strategy to fit with the research design and hypotheses. AAL took the primary role in drafting the manuscript and final editing. GAB and MM edited the entire manuscript multiple times. JL wrote a section of the manuscript and played a final editing role. AKN wrote a section of the manuscript and edited the manuscript. All five authors are actively involved in the planning and conduct of the study described and all will be involved in interpretation and reporting of the findings for this study.
Funding This work was supported by the National Institute of Child Health and Development (grant numbers R01HD085990 and R01HD100469) to AAL, GAB and JL (with MM as site PI and AKN as Co-I), and AAL, GAB and MM (with JL and AKN as Co-Is), respectively.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.