Article Text

Abstract
Introduction The use of peripheral indwelling arterial catheter for haemodynamic monitoring is widespread in the intensive care unit and is recommended in patients with shock. However, there is no evidence that the arterial catheter could improve patient’s outcome, whereas the burden of morbidity generated is significant (pain, thrombosis, infections). We hypothesise that patients with shock may be managed without an arterial catheter.
Methods and analysis The EVERDAC study is an investigator-initiated, pragmatic, multicentre, randomised, controlled, open-label, non-inferiority clinical trial, comparing a less invasive intervention (ie, no arterial catheter insertion until felt absolutely needed, according to predefined safety criteria) or usual care (ie, systematic arterial catheter insertion in the early hours of shock). 1010 patients will be randomised with a 1:1 ratio in two groups according to the strategy. The primary outcome is all-cause mortality by 28 days after inclusion. A health economic analysis will be carried out.
Ethics and dissemination The study has been approved by the Ethics Committee (Comité de Protection des Personnes Île de France V, registration number 61606 CAT 2, 19 july 2018) and patients will be included after informed consent. The results will be submitted for publication in peer-reviewed journals.
Trial registration number NCT03680963.
- adult intensive & critical care
- health economics
- clinical trials
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The present project will be the first, multicentre, randomised, non-inferiority, controlled trial assessing the benefits and harms of the usual, systematic use of an arterial catheter, as compared with a less invasive strategy (no arterial catheter insertion unless absolutely needed) in patient with shock.
Blinding is not possible, nonetheless, we choose a solid, objective and patient-centred primary endpoint, mortality at day 28.
As the use of an arterial catheter is recommended in the care of patients with shock, cross-over is possible but very strict conditions to allow cross over will be applied.
The study is sufficiently sized to allow concluding to the non-inferiority but also, possibly, to the superiority of the tested, less invasive intervention.
The pragmatic design and the involvement of medical, surgical and mixed intensive care units, as well as academic tertiary care hospitals and community hospitals, will allow generalising the results.
Introduction
Background and rationale
The insertion of an indwelling arterial catheter (IAC) is a common practice in intensive care units (ICUs) patients around the world. In the USA, up to 38% of ICU patients may receive it.1 A European point-prevalence study performed in 1417 ICUs showed that 44% of ICU patients underwent an arterial catheter insertion.2
The reasons for this widespread use of the arterial catheter are that it allows continuous measurements of blood pressure (BP), a key physiological variable that drives organ perfusion, and facilitates blood sampling for laboratory testing while avoiding repeated vascular punctures.1 3 4 Therefore, despite the lack of high-level evidence of the benefits it could bring to ICU patients, the arterial catheter insertion is commonly recommended to manage patients with septic shock or other kinds of shock.5–8
One observational study showed, an increased mortality associated with arterial catheter use among patients receiving vasopressors, while adjusting for a propensity score to receive or not an arterial catheter.9 More recently, in a large cohort of ventilated patients who did not require vasopressor support, Hsu et al observed no difference in day 28 mortality after propensity score matching to receive or not an arterial catheter between patients with and without one. They observed shorter ICU and hospital stay among patients with no IAC in the full matched cohort and, also when the survivors were separately analysed.10 The authors concluded that randomised controlled trials were mandatory to investigate the impact of the arterial catheter use on patients’ outcomes.
Morbidity related to the arterial catheter
Vascular complications associated with the IAC are temporary arterial occlusion (≈20%), permanent ischaemia (≈0.1%), haematoma (≈14%) and pseudoaneurysm (≈0.1%).11–13 Local infectious complications or colonisation have an incidence close to 11 per 1000 arterial catheter days and bloodstream infections an incidence of 1.7 per 1000 (95% CI: 1.2 to 2.3) arterial catheter days.13
Moreover, some authors suggest that the presence of an arterial catheter, since it facilitates blood sampling, may increase the number of unnecessary blood samples drawn, therefore favouring anaemia and red blood cell transfusion during the ICU stay.10 14–16
In addition, one may speculate that the time needed to insert an arterial catheter, during the first golden hours of resuscitation, could delay urgent treatments and procedures (therapeutic prescription such as fluid expansion or antibiotics, nurses work overload, transport to imaging facility or operating room).
Related costs
Studies that specifically examined the cost related to arterial catheter use in ICU patients are lacking. However, one can speculate that this cost is high for hospitals when considering the time and resources needed for an arterial catheter insertion (on average 20 min of physician and 20 min of nurse time)17 and maintenance, the high number of patients undergoing arterial catheter insertion, the cost associated with catheter-related infections and perhaps undue lab tests and transfusions.18–24
Alternatives to the use of the arterial catheter
Alternatives to invasive BP measurements
Non-invasive BP (NIBP) measurements through automated oscillometry and brachial cuff are widely used, even in shocked, unstable patients.25 It is the first-line monitoring used during pre-hospital care, in the emergency department and often at ICU admission, before an intra-arterial catheter can be inserted in optimal conditions.
Notwithstanding some artefacts, oscillometric mean BP measurement is accurate to a few mm Hg.26 This point is of crucial importance since generally intensivists pay great attention to mean BP, as it represents the perfusion pressure of most organs, and mainly rely on it to track response to therapy in shocked patients.27
With modern oscillometric devices, recent prospective studies have shown that mean and diastolic BP measurements with an arm cuff NIBP device fulfilled the Internation Oragnisation for Standardisation (ISO Standard,28–30 that is, reported a mean bias of 5 mm Hg or less when compared with the intra-arterial reference, even in hypotensive, unstable ICU patients receiving continuous intravenous vasopressors. Remarkably, arm NIBP detection of a mean BP <65 mm Hg was associated with a high area under the receiver operating characteristics curve (AUCROC) of 0.90–0.98.28 29 31 32 Moreover, changes in arm NIBP have sufficient accuracy to provide good detection of a significant increase in intra-arterial mean BP, enabling identification of BP responders to urgent therapies (AUCROC of 0.89–0.98 for a 10% mean BP increase cut-off).31 In addition, arrhythmia did not alter the performance of the tested devices. It should be noted however that oscillometric arm NIBP measurements still remains challenging in very obese patients, even when the cuff size is optimal.30 33
Alternatives for arterial blood analysis
Central venous lines allow the safe infusion of drugs potentially toxic to the peripheral veins, such as vasopressors and hyperosmotic solutions. For these reasons, they are often used when caring for ICU patients,1 2 and their risk/benefit ratio seems to favour patients’ safety when compared with the use of peripheral venous lines.34
Blood drawn from superior vena cava catheters can be used to estimate arterial blood gases and lactate concentration with variously appreciated accuracy but of potential clinical value.35–38 As recently reported by our group in a large cohort of ICU patients with circulatory failure, the analysis of central venous blood combined with finger pulse-oximetry readings (SpO2) provides useful prediction of arterial pH, arterial carbon dioxide tension (PaCO2) and lactate concentration.39 In short, when the estimation of arterial values from central venous blood analysis predicts values within the normal range, this helps ruling out blood gas or lactate abnormal values with high probability.
In summary, a number of arterial punctures and arterial blood drawings can be avoided by simply checking SpO2 and analysing central venous blood. This does not prevent prescribing arterial puncture in some cases, depending on the clinical situation and the clinician’s confidence. Of note, central lines may be safely used to sample blood for other purposes than blood gases or lactate monitoring, as safely done for decades in cancer/haematology patients.40–43
Methods and analysis
Study design
The study at hand will be an investigator initiated, pragmatic, multicentre, randomised, controlled, open, two-parallel-group, non-inferiority clinical trial with 1:1 assignment of interventions.
Patient and public involvement
Patients and the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Blinding and randomisation
Although blinding is not possible due to the nature of the assessed intervention, the primary endpoint is objective (mortality at day 28).
We deliberately decided not to perform a cluster randomised trial. This design is prone to the risk of selection bias. Moreover, there are few centres in the study (medical, surgical and mixed ICUs, as well as academic tertiary care hospitals and community hospitals), which could lead to chance imbalance.
As the need for arterial catheter insertion is rooted in intensivists’ mind when caring for patients in shock, there is a real risk that patients assigned to the non-invasive arm will frequently be switched to the invasive arm (with arterial catheter insertion). To prevent this kind of contamination bias, the study scientific committee has set reasonable and consensual safety boundaries that will fix in which circumstances the insertion of an arterial catheter will become an inescapable need (in terms of vasopressor requirement for instance (see the ‘Interventions’ section).
In the end, we opted for a classical individually randomised trial and worked at limiting group contamination.
Randomisation will be electronically centralised via a dedicated website, stratified on centres, invasive mechanical ventilation (yes or no) and vasopressor dosage, namely <or ≥0.18 µg/kg/min of continuous intravenous norepinephrine (ie, 0.36 µg/kg/min of continuous intravenous norepinephrine tartrate) or of epinephrine or of the sum of both medications’ dosages at the time of enrolment.
The statistician in charge of the project will determine permutation blocks, the size of which will not be known by the investigators.
Study time points definitions
Patients will be declared enrolled in the study once consent obtained.
Date and time of randomisation will determine the beginning of the intervention period (Study H0). Study outlines are provided in figure 1.
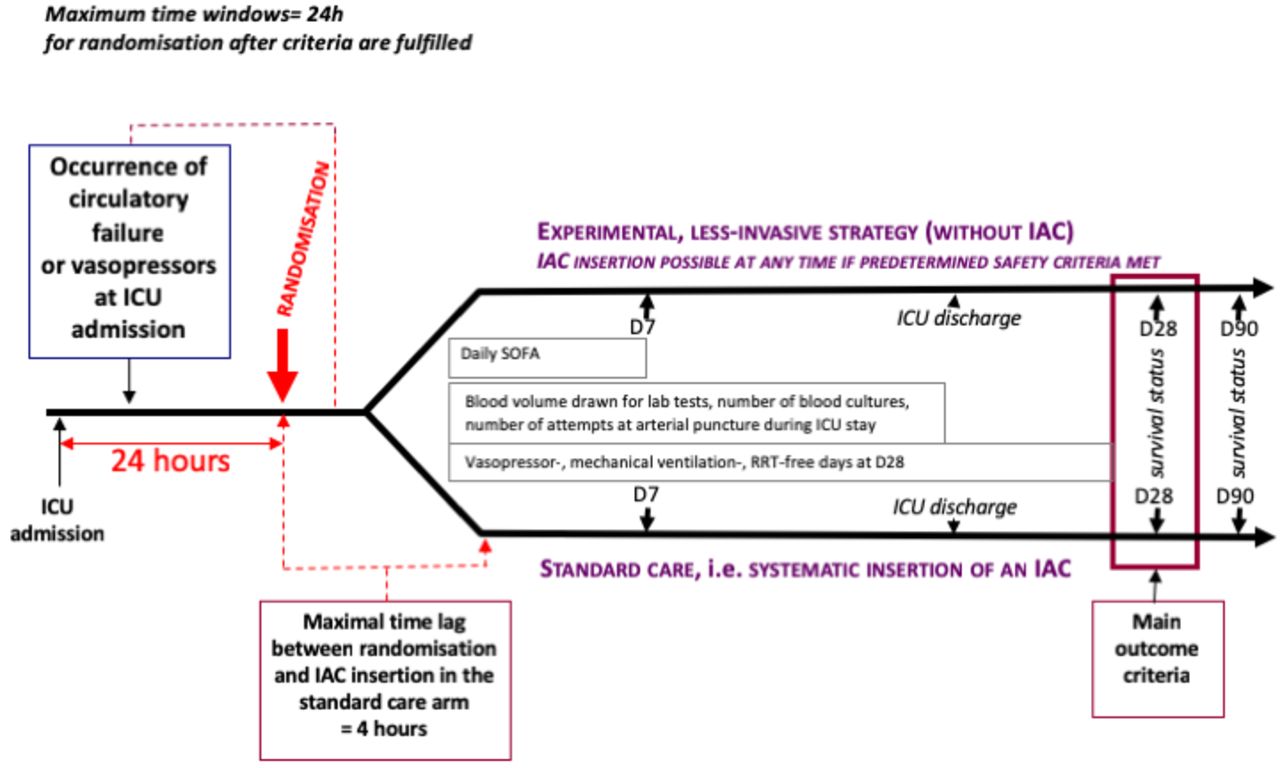
{kind=link}
Study outline. IAC, indwelling arterial catheter; ICU, intensive care unit; SOFA, Sequential Organ Failure Assessment.
Inclusion and non-inclusion criteria
Inclusion criteria are: age ≥18 years, existence of an acute circulatory failure defined by the presence of persisting hypotension (systolic <90 mm Hg or mean BP <65 mm Hg, for more than 15 min at ICU admission or within the following 24 hours; OR requirement of continuous intravenous vasopressor infusion) AND presence of at least one sign of peripheral hypoperfusion (alteration of mental status; skin mottling; oliguria defined as a urine output <0.5 mL/kg body weight for at least 1 hour; arterial lactate concentration >2 mmol/L; peripheral venous lactate concentration >3.2 mmol/L44; central venous oxygen saturation (ScvO2) <70%).
Non-inclusion criteria are: acute circulatory failure present for more than 24 hours, NIBP device failing to display a BP value or cuff placement impossible, patient undergoing extracorporeal membrane oxygenation, patient treated with vasopressor doses of more than 2.5 µg/kg/min of vasopressor (because it is the threshold indicating the insertion of an arterial catheter in patients assigned to the non-invasive group), severe traumatic brain injury (with a Glasgow Coma Scale score of less than 9), patient previously included in the trial, refusal to participate, body mass index above 40 kg/m2, pregnancy.
Interventions
Once included, the patient will be randomly assigned, for the 28 following days, to one of the following strategies:
(A) ‘Usual care’: An arterial catheter will be inserted within the first 4 hours after randomisation and will be maintained until day 28 or ICU discharge (whichever comes first), except in case of arterial catheter futility (see definition below), suspected or proven arterial catheter related infection or thrombosis (at the discretion of attending physician). After day 28, clinicians may choose to maintain or to remove the arterial catheter. If indicated, arterial blood will need to be drawn via the arterial catheter.
In case of arterial catheter removal for other futility criteria than decision of palliative care, an arterial catheter will be inserted within the 4 hours of new onset of circulatory failure.
(B)‘Non-invasive care’: No arterial catheter insertion will be allowed during the first 28 days, excepted if predefined safety criteria (indicating absolute need of an arterial catheter insertion) are reached: an arterial catheter will be inserted within the 4 hours of presence of safety criteria and the patient will be managed as if he/she were part of usual care group until day 28 or ICU discharge. Arterial blood drawn will be allowed via direct arterial puncture as frequently as indicated.
Criteria of arterial catheter futility (one or more criteria define futility) allowing arterial catheter removal at physician’s discretion:
The patient no longer needs vasopressor therapy for more than 4 hours, and exhibits no sign of hypoperfusion.
Medical decision of palliative care
Safety criteria indicating the insertion of an arterial catheter in patients initially randomised in the ‘no arterial catheter’ group
As undisputable criteria are lacking in the medical literature, criteria were consensually determined (Delphi method)45 after collecting the opinion of the anticipated investigators in each centre. After two notation rounds, the following criteria were retained: pulse oximetry monitor or NIBP can no longer display any reliable value; absolute need of one arterial blood gas measurement whereas five consecutive arterial puncture attempts have failed; patient placed under extracorporeal membrane oxygenation; need of vasopressor dosages of more than 2.5 µg/kg/min; patient undergoing high-risk surgery (left at the attending physician discretion) within the next 4 hours; in this last case, the arterial catheter should be withdrawn within the 4 hours after the patient returns in the ICU, unless one or several of the above-mentioned safety criteria are fulfilled.
Blood sampling technique
Regarding blood sampling for laboratory tests, to avoid unnecessary blood spoliation in both arms, we strongly encourage investigators and attending intensivists to properly assess the real need of each laboratory test they order. We discourage sampling for routine (daily or more frequent) monitoring or after changes in inspired oxygen fraction or positive-end-expiratory pressure for example. If blood gas discloses metabolic or respiratory disorder, we encourage the clinicians to order resampling only after a therapeutic intervention has been administered.
In addition, to decrease blood spoliation during sampling through any vascular catheter (arterial catheter for the invasive group, central venous line for the non-invasive group), we strongly suggest to discard at least two times, but not more than the catheter’s priming volume (3–5 mL) before sampling. For the centres using a closed system for reinfusion, they can continue to use it without discarding blood.
In the ‘usual care’ group, blood samples for laboratory tests will be drawn from the arterial catheter, as many times as necessary. Blood drawing through the central venous catheter is forbidden, excepted for ScvO2 measurements.
In the ‘non-invasive’ group, blood drawing through the central venous catheter is recommended for usual laboratory tests. Regarding the monitoring of oxygenation and acid-base homeostasis and of the lactate blood concentration, we encourage the attending intensivists and investigators to rely on SpO246 47 to assess oxygenation, and on predicted pH, PaCO2, and lactate derived from central venous blood analysis.39 For this purpose, formula to derive estimates of arterial blood parameters and abacuses giving probabilities of true arterial values below or above given thresholds for each predicted value will be provided to the sites. We developed a mobile application to automatically estimate arterial blood gas parameters from central venous parameters and SpO2 (available online: www.everdac.fr/).
Modalities of patients’ general management
In both group, patients will be managed following international and national guidelines, except for the arterial catheter insertion.
Outcome measurements
Primary outcome
All-cause mortality by 28 days after randomisation.
Secondary outcomes
To account for the potential bias brought by deaths occurring as the result of life-sustaining treatments withdrawal/withholding, as frequently encountered in ICUs, we will record such events from inclusion to Day 35 (ie, until 1 week after the primary time point).48
Cumulative incidence of death from inclusion through day 90.
Cumulative survival free of arterial catheter insertion, from inclusion through day 90.
Number of patients who underwent IAC insertion, in both groups.
Evolution of daily Sequential Organ Failure Assessment (SOFA)49 score during the first 7 days.
Daily amount of intravenous fluid given for rapid vascular volume expansion from day 1 to day 7.
Daily fluid balance from day 1 to day 7.
Duration of mechanical ventilation.
Ventilator-free days from day 1 to day 28 (for this purpose patients dying between randomisation and day 28 will be assigned a 0 value; for survivors at day 28, all the days free of invasive mechanical ventilation through an endotracheal tube within the 28-day period will be taken into account).
Proportion of patients treated by renal-replacement therapy between day 1 and day 28.
Renal replacement therapy-free days from day 1 to day 28 (for this purpose days without renal replacement therapy from day 1 to day 28 for survivors at day 28, and from day 1 to the date of death for patients dying before day 28, will be taken into account).
Proportion of patients treated by vasopressor between day 1 and day 28.
Vasopressor therapy-free days from day 1 to day 28 (for this purpose days without vasopressor therapy from day 1 to day 28 for survivors at day 28, and from day 1 to the date of death for patients dying before day 28, will be taken into account).
Mean daily blood volume drawn for lab testing during ICU stay.
Number of blood cultures performed during ICU stay.
Number of attempts at arterial puncture during ICU stay.
Evolution of blood haemoglobin level from day 1 to day 28.
Evolution of haematocrit from day 1 to day 28.
Number of red blood cell packs transfused from day 1 to day 28.
Number of transcutaneous arterial and venous puncture for lab tests, arterial catheter insertion and set up of monitor, blood drawing from the arterial catheter or other vascular line through ICU stay and time (min) spent by nurses and physicians (min) on these tasks during the first 3 days of the ICU stay (in a random sample representing 10% of the total number of included patients).
Number of arterial and central venous catheter insertion during ICU stay.
Numbers of arterial and central venous catheter-related infections during ICU stay, expressed as the incidence of new cases per 1000 catheter days, including local and catheter-related bloodstream infections as consensually defined.50 51
Numbers of local infections of arterial and central venous during ICU stay (number of new cases per 1000 catheter days).
Numbers of arterial and central venous catheter-related bloodstream infections during ICU stay, (number of new cases per 1000 catheter days).
Number of bloodstream infections during ICU stay, catheter related or not.
Duration of ICU stay.
Duration of hospital stay.
ICU mortality.
Hospital mortality.
Day 90 mortality.
Number of adverse events (AEs) of special interest (ischaemia and/or necrosis of finger(s) or toe(s); documented bowel ischaemia; occurrence or worsening of acute renal failure with need of renal replacement therapy; need of tracheal intubation in a patient previously not intubated; cardiac arrest; nerve injury of upper limb(s); skin lesions at cuff location or at arterial catheter insertion site; arterial thrombosis, haematoma, arterial pseudo aneurysm, haemorrhage at arterial catheter insertion site either during arterial catheter placement or later).
Incremental cost-effectiveness ratio (ICER): «Cost/Life day gained at 28 days’» between the two strategies.
Budget impact of the generalisation of the non-invasive strategy (if clinical non inferiority is demonstrated) in France on a 5 years’ time frame.
Patient-reported pain and discomfort related to the device used for BP monitoring
Data management
Data management will be performed by the INSERM CIC-P 1415. An electronic case report form (CRF) will be developed using the Clinsight software. Data will be managed in agreement with the INSERM CIC-P 1415 standardised operating procedures (SOP).
A blind review will be done prior locking the data-base.
Diagnosis-related groups (DRG) and reimbursement data for patient hospital stays from randomisation to day 28 will be obtained from an extraction from each hospital’s discharge database Programme de Médicalisation des Systèmes d'Informations (PMSI) at the end of the study.
Sample size calculation
The hospital mortality of patients with septic shock, the most prevalent cause of shock in the ICU, is around 30%–35% depending on initial lactate level.52 We speculated that the day 28 mortality would be lower, around 25% in the study cohort for several reasons: (1) Patients with shock other than septic shock can be included, and the mortality rates of haemorrhagic, hypovolaemic non-haemorrhagic and cardiogenic shock are highly variable depending on the cause; (2) The use of vasopressor is not mandatory for inclusion, so patients with short-lived hypotension (but with at least one sign of hypoperfusion) can be included; (3) Patients with very high vasopressor dosages are excluded and (4) Patients with severe traumatic brain injury are excluded, an exclusion policy which should lower the mortality rate of the haemorrhagic shocks of traumatic origin.
We assume that the mortality rate at day 28 will be 22.5% in the ‘non-invasive’ group and 25% in the control (invasive, usual care) group. With the non-inferiority margin set at 5%, power at 80% and alpha risk at 5%, the inclusion of 1010 patients is needed.
The 5% non-inferiority margin has been obtained through a consensus between the investigators and the methodologists of the study, considering that a 5% difference is the smallest value that would be clinically relevant between arms.
Data analysis and statistics
The intention to treat principle will be applied. Nevertheless, patients who would withdraw consent to study participation will be discarded, as required by the French legislation. No intermediate analysis will be performed. A 95% CI will be provided for each estimation.
Statistical analysis of the primary outcome
The between-group difference (experimental group minus usual care group) in rates of day 28 mortality will be estimated based on the two-sided 95% CI. The upper boundary of the 95% CI will be compared with the non-inferiority margin of 5%. If non-inferiority is demonstrated, the upper bound of the 95% CI will be compared with 0: if it is lower than 0, then a superiority conclusion will be drawn. As a sensitivity analysis, we will perform a multivariate logistic regression, to estimate the OR adjusted on the stratification variables and location of the arterial catheter (because the arterial catheter location, namely femoral vs radial site, may influence the rate of catheter-related infections and other complications).
Statistical analysis of secondary clinical outcomes
Day 90 mortality: the between-group difference in rates of day 90 mortality will be estimated. Survival analysis will also be performed on mortality using a Cox regression model providing that the assumption of proportional hazards is verified.
The effect of intervention on changes over time of SOFA, blood haemoglobin level, haematocrit, mean daily blood volume drawn for lab testing and daily maximum pain will be estimated using mixed linear models, after data transformation if necessary.
Durations of mechanical ventilation, ICU stay and hospital stay as well as ICU and hospital mortality will be analysed using a competing risk approach, with death as competing risk.
The incidences of patients treated by renal-replacement therapy or by vasopressor, and of patients with arterial and central venous catheter-related infections or bloodstream infections will be estimated using the competing risk approach, with death as competing risk.
The effect of intervention on number of blood cultures performed, number of attempts at arterial puncture, number of red blood cell packs transfused, number of arterial and central venous catheter insertion will be estimated using negative binomial models with duration of ICU stays as offset variable.
IQR and medians of free-days (Ventilator-free days, renal replacement therapy-free days, vasopressor therapy-free days) will be estimated in each group.
Statistical analysis of health economic outcomes
Cost-effectiveness analyses will follow standard recommendations for health economic analyses.
The time horizon will be 28 days and take into account two viewpoints (health insurance and health institutions). Only the direct medical costs related to the hospitalisations will be retained. The economic data will be derived from hospital microcosting of 10% of the patients in each centre and from the local collection of DRG and reimbursement data for hospital stays for patients up to day 28. The microcosting will be performed to count and time resources used in ICU for some specific steps: preparation and insertion of an IAC and set up of monitor, NIBP measurement by oscillometry, arterial and venous blood punctures and sampling, peripheral pulse oximetry readings (SpO2), transfusion (number of packed red blood cell transfused) and dressing changes. Staff resources (physician, nurse…) will be reported and timed separately. The equipment used for these steps will also be collected.
The ICER «Cost/Prevented death at 28 days’» will be computed and presented in cost-effectiveness plan and a cost-effectiveness acceptability curve will be drawn from a bootstrap simulation to show the probability that the studied strategy is cost-effective for a ceiling ratio. This ratio is determined as the maximum cost that decision makers are willing to pay for one prevented death at 28 days. The uncertainty of the ICER will be assessed using one-way deterministic sensitivity analyses (use of tornado diagram to present the results) and probabilistic sensitivity analysis (Monte-Carlo simulations).
A budget impact analysis will attempt to evaluate the potential savings in the wider use of the efficient strategy in terms of generalisation of the non-invasive strategy in France on a 5-year time frame and from the viewpoint of the health system (Hospital and Health Insurance).
Satistical analysis will be done with R software (version 3.6.3); Excel and TreeAge Pro softwares will be used for all health economic analyses.
Management of AEs
As this research is qualified as a low risk study in the meaning of the French law, all serious AE (SAE), in accordance with regulations in force, have to be reported by the investigator according with each procedure in place for reporting AE related to care in the institution.
The following AEs will be considered SAEs of special interest and are to be recorded in source documents and study CRF, whatever their relation to the study procedures and whatever the study arm the patient is assigned to:
Ischaemia and/or necrosis of finger(s) or toe(s).
Documented bowel ischaemia.
Occurrence or worsening of acute renal failure with need of renal replacement therapy (while there was no need of renal replacement therapy before this event).
Need of tracheal intubation in a patient previously not intubated.
Cardiac arrest.
Death of any cause.
Each AE, serious or not, related or not to the study procedure have to be recorded in source documents and study CRF.
For safety purpose, the following AEs that could potentially be related to the BP measuring method used, will be systematically collected in source documents and study CRF:
Nerve injury of upper limb(s).
Skin lesions at cuff location or at IAC insertion site.
Arterial thrombosis, haematoma, arterial pseudo aneurysm and haemorrhage at IAC insertion site either during IAC placement or later.
Monitoring and study safety
For this research that brings minimal risks (in the meaning of the French Law), we do not plan to set up an independent data safety and monitoring board.
Ethics and dissemination
The protocol has been approved by the Ethics Committee (Comité de Protection des Personnes Île de France V, number 61606 CAT2). The results of the study will be presented in national and international conferences, and published via a peer-reviewed journal.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @a6tole, @Quenot
Contributors GM and TB designed the study and wrote the first draft of the manuscript. GM, TK, DC, SE, MM, J-PQ, J-CL, FB, AM, SV, SBH, ET and TB also helped to design the study. GM, TK, DC, SE, MM, J-PQ, J-CL, FB, AM, SV and TB participated in the notations according to the Delphi method to fix inclusion and exclusion criteria and safety limits of vasopressor dosages. SBH designed the methods of the medicoeconomic study. ET and TB designed the statistical plan analysis. GM, TK, DC, SE, MM, J-PQ, J-CL, FB, AM, SV, SBH, ET and TB critically revised the manuscript for important intellectual content and approved the final version of the manuscript. GM, TK, DC, SE, MM, J-PQ, J-CL, FB, AM, SV, SBH, ET and TB gave their agreement to be accountable for all aspects of the work and ensure the accuracy and integrity of any part of the work.
Funding Funded by the French government (Programme Hospitalier de Recherche Clinique 2017, Number PHRCN-17-0326).
Disclaimer This funding source had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.