Article Text

Abstract
Introduction Studies of adolescent mental health require valid measures that are supported by evidence-based theories. An established theory is the dual-factor model, which argues that mental health status is only fully understood by incorporating information on both subjective well-being and psychopathology.
Objectives To develop a novel measure of adolescent mental health based on the dual-factor model and test its construct validity.
Design Cross-sectional analysis of national health survey data.
Setting and participants Nationally weighted sample of 21 993 grade 6–10 students; average age: 14.0 (SD 1.4) years from the 2014 Canadian Health Behaviour in School-aged Children study.
Measures Self-report indicators of subjective well-being (life satisfaction, positive and negative affect), and psychopathology (psychological symptoms and overt risk-taking behaviour) were incorporated into the dual-factor measure. Characteristics of adolescents families, specific mental health indicators and measures of academic and social functioning were used in the assessment of construct validity.
Results Proportions of students categorised to the four mental health groups indicated by the dual-factor measure were 67.6% ‘mentally healthy’, 17.5% ‘symptomatic yet content’, 5.5% ‘asymptomatic yet discontent’ and 9.4% ‘mentally unhealthy’. Being mentally healthy was associated with the highest functioning (greater social support and academic functioning) and being mentally unhealthy was associated with the worst. A one-unit increase (ranges=0–10) in peer support (OR 1.19; 95% CI 1.15 to 1.22), family support (OR 1.32; 95% CI 1.28 to 1.36), student support (OR 1.20; 95% CI 1.17 to 1.24) and average school marks (OR 1.18; 95% CI 1.10 to 1.27) increased the odds of being symptomatic yet content versus mentally unhealthy. Mentally healthy youth were the most likely to live with both parents (77% vs ≤65%) and report their family as well-off (62% vs ≤53%).
Conclusions We developed a novel, construct valid dual-factor measure of adolescent mental health. This potentially provides a nuanced and comprehensive approach to the assessment of adolescent mental health that is direly needed.
- epidemiology
- mental health
- statistics & research methods
- child & adolescent psychiatry
- public health
Data availability statement
Data may be obtained from a third party and are not publicly available. The HBSC Data Management Centre coordinates the work with the HBSC data, and is the Data Bank for the HBSC-study. The centre distributes data in accordance with the HBSC data access policy. Web: http://www.hbsc.org/.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study builds on an existing literature base by being the first to operationalise the dual-factor model in a large, national sample of Canadian adolescents.
The dual-factor measure developed in this study can be used to increase our understanding of adolescent mental health and can be applied in future cross-national initiatives.
This study relied on secondary data, and its restriction to available indicators collected as part of the Health Behaviour in School-aged Children study. As a result, single items were used to measure positive and negative affect, instead of full scales.
Reliance on self-report data may be subject to social-desirability bias, particularly for overt risk-taking behaviours.
Introduction
Adolescent mental health has been identified as a critical research priority in Canada.1 WHO defines mental health as ‘a state of well-being in which every individual realises his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community’.2 While this definition has been criticised for decontextualising mental health,3 it clearly illustrates the complexity involved in operationalising a measure of mental health status. Studies in the field of mental health require valid measures that are supported by evidence-informed theories, and go beyond the simplicity of unidimensional indicators of morbidity. One theory with known utility is the dual-factor model, which argues that mental health status is only fully understood by incorporating information on both subjective well-being as well as psychopathology.4 5 In this study, we developed a measure of adolescent mental health based on this dual-factor model, and tested its construct validity.
Historically, mental health research has used disease-based models that focus on identifying symptoms of mental illness, which encompass internalised (eg, anxiety and depression) and externalised (eg, behavioural problems) psychopathology.5 This approach considers mental health to be present in the absence of mental illness, the latter defined as a group of diagnosable conditions found in the Diagnostic and Statistical Manual of Mental Disorders-5 that cause changes in our mood, thinking and behaviour.6 This line of thinking is consistent with the traditional medical model, which categorises individuals as either sick or well, with a focus on treating the sick. Yet, contemporary thinking suggests that the absence of mental illness is necessary, but not sufficient to ensure optimal mental health.5 7 It is possible to be free of mental illness, but not fully mentally healthy.8
The field of positive psychology has put a focus on the importance of positive psychological factors (ie, subjective well-being or happiness) in the optimisation of mental health.4 5 The hedonic and eudaimonic approaches to conceptualising well-being are commonly used to study such factors.9 According to the hedonistic research tradition, subjective well-being is captured through experiences of positive emotions and feeling good about one’s life, and can be measured with three components: life satisfaction, the presence of positive affect, and the absence of negative affect.10 In contrast, the eudaimonic approach to well-being focuses on an individuals interactions with their environment, and refers to self-actualisation (living up to one’s potential), finding meaning and purpose in life and functioning well.11 Subjective well-being is an important predictor of future mental health and mental illness.12
In response to criticisms raised about traditional deficit models12 and the emergence of positive psychology,13 Keyes developed a measure of mental health that combines self-reported hedonic (emotional) and eudaimonic (social and psychological) measures of well-being. Mental health is placed on a continuum from ‘flourishing’ to ‘languishing’, with those in the middle labelled as ‘moderately mentally healthy’.14 This approach has been criticised for considering mental health and mental illness as opposite ends of a continuum. An increase in one dimension is not necessarily associated with a decrease in the other.7 Illustratively, there are youth who report high levels of well-being, despite displaying symptoms of mental illness.15
Building on such criticism, the ‘dual-factor model’ of mental health was proposed based on the premise that mental health is a complete state composed of two unique, but correlated, dimensions.4 This measure uses ratings of subjective well-being and psychopathology to classify people into four categories: (1) ‘mentally healthy’ (high subjective well-being and low psychopathology), (2) ‘symptomatic yet content’ (high well-being, despite high psychopathology), (3) ‘asymptomatic yet discontent’ (low psychopathology, but low subjective well-being) and (4) ‘mentally unhealthy’ (low well-being and high psychopathology) (figure 1).4 5 16 According to this model, optimal mental health requires a positive sense of well-being in addition to the absence of clinically significant, active mental illness.7

The dual-factor model of mental health.
In previous studies among elementary and high school-age youth, 57%–68% were mentally healthy (also referred to as ‘flourishing’, ‘positive mental health’, ‘complete mental health’ and ‘well-adjusted’), 9%–20% were symptomatic yet content (also referred to as ‘externally maladjusted’ and ‘ambivalent’), 4%–21% were asymptomatic yet discontent (also referred to as ‘vulnerable’, ‘dissatisfied’ or ‘at risk’), and 7%–20% were mentally unhealthy (also referred to as ‘troubled’, ‘distressed’ and ‘languishing’).17–24 The mentally healthy group consistently had the highest functioning in terms of academic performance (eg, higher Grade Point Average (3.18 vs ≤2.95, p<0.01)),4 5 21 social relationships (supportive relationships with peers, family and teachers),4 5 18 25 behaviour (eg, behavioural engagement at school (Cohen’s d effect sizes ≥0.48))5 21 and physical health.5 17 Asymptomatic yet discontent youth would be identified as mentally healthy using traditional disease-based approaches. Yet, they display reduced functioning compared with the mentally healthy group and report similar academic struggles as those with high psychopathology.26 The symptomatic yet content group had better social functioning and academic engagement21 and higher self-worth than the mentally unhealthy group.5 20 The mentally unhealthy group had the worst outcomes of the four groups (eg, lowest self-worth, greatest external locus of control, poorest physical health, most social problems),4 with the exception of some cross-sectional studies that found no significant differences in academic achievement between the mentally unhealthy and symptomatic yet content groups.5 21 However, longitudinal findings suggest that the mentally unhealthy group is at greater risk of future academic decline.20 27
A dual-factor measure provides a potentially useful, nuanced and comprehensive understanding of adolescents’ mental health status.4 5 18 21 Such a measure is less likely to overestimate or underestimate an individual’s mental health than measures that rely on a single dimension.12 The ability to identify four unique mental health groups provides new opportunities to increase understanding of the factors and circumstances that influence mental health.
While previous research supports a dual-factor measure in adolescents, the majority of studies have been conducted from selected populations in the Southeastern USA.17 19 21 The one existing Canadian study generated evidence supporting the validity and potential utility of a dual-factor measure based on a sample of 407 students in grades 3–6 (mean age 10.5 years, (SD=0.7)) from Alberta, Canada.4 However, no studies have operationalised a dual-factor measure among older Canadian adolescents or in a population representative sample. The generalisability of previous findings is unknown as the study samples had exposures that could influence mental health (eg, environmental, cultural and economic) that are not representative of those experienced by the Canadian adolescent population. It is important to validate a dual-factor measure in adolescent populations because adolescence is a key stage of heightened social and emotional development, and a peak period of onset for mental health problems.28
Study objectives
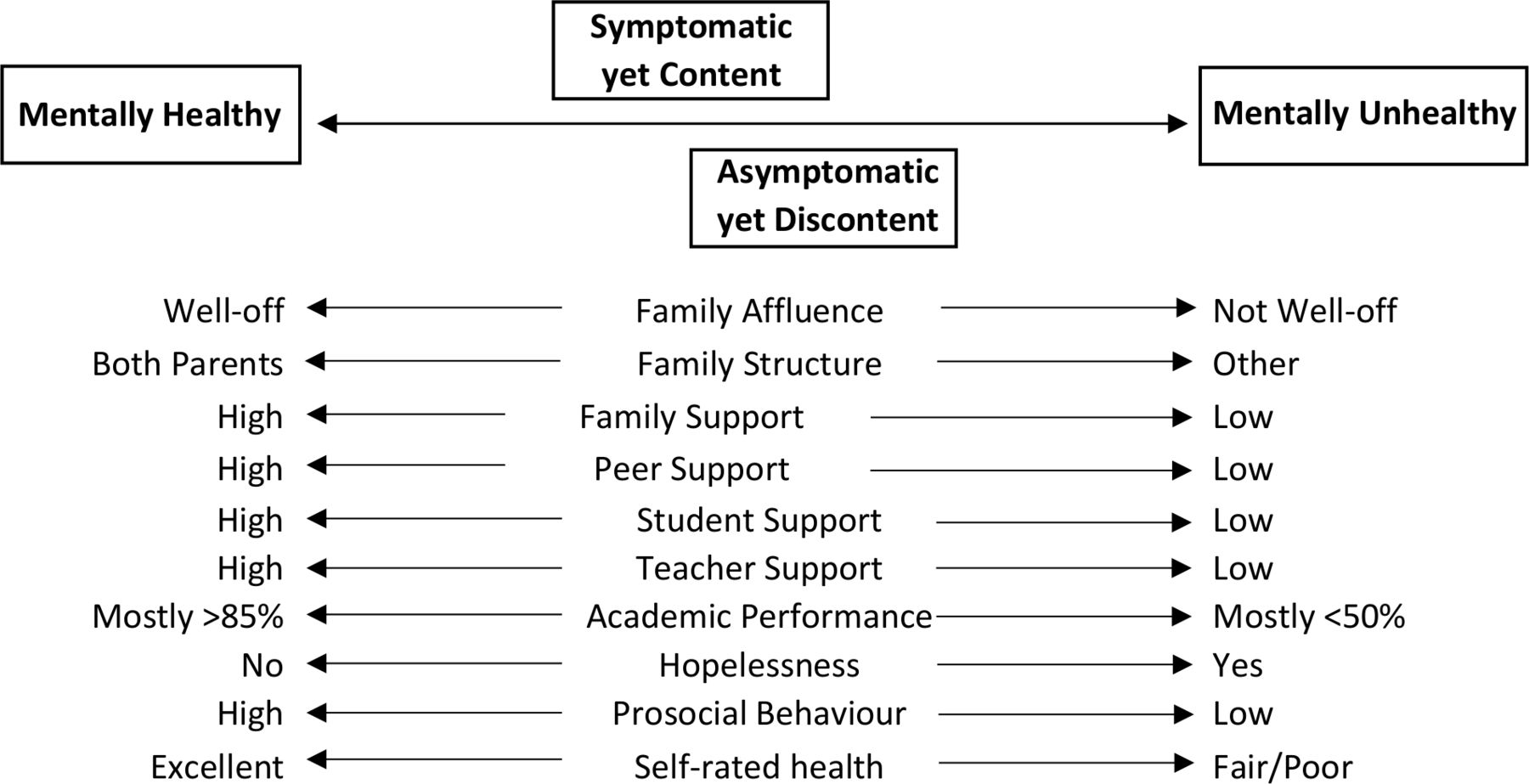
We developed a novel measure of adolescent mental health status based on the dual-factor model in a large, national sample of young Canadians aged 11–15 years. Our study objectives were: (1) to develop a measure based on the dual-factor model, by combining indicators of subjective well-being and psychopathology; (2) to test the measure’s construct validity by examining whether the mental health groups differed in predictable manners based on family characteristics and academic performance, social support, and mental health indicators known to be associated with mental health (figure 2).29 30 Consistent with the dual-factor model, belonging to the ‘mentally healthy’ group was expected to be associated with indicators of positive functioning (greater social support and academic performance), living with both parents, higher self-reported family affluence, and better self-rated health. Conversely, we expected poorer functioning, lower self-reported family affluence and worse self-perceptions of health would be associated with belonging to the ‘mentally unhealthy’ group. Based on previous study findings the symptomatic yet content group was expected to report greater social support,19 21 and similar academic functioning5 21 compared with the asymptomatic yet discontent group (figure 2). Our focus on social and academic functioning was guided by a key component of the WHO’s definition of mental health: the effective functioning of an individual.2 The overall goal of this study was to develop an evidence-based measure that could be applied robustly in the field of adolescent health research.

{kind=link}
{kind=link}
Expected associations between study variables and mental health status according to the dual-factor model.
Methods
Data Source
Data for this study were obtained from the 2014 Canadian Health Behaviour in School-aged Children (HBSC) study.31 32 The HBSC study is a cross-sectional, general adolescent health survey of grade 6–10 students that is conducted in 4-year cycles in association with WHO. The sample was stratified within each province/territory by language of instruction, public/Roman Catholic designation and community size. Schools were then randomly selected using a systematic sampling approach. In most cases school administrators selected two classes at each grade to participate. In some provinces (eg, Prince Edward Island) and the territories, all students within the targeted grades were invited to participate. Private, special and on-reserve schools (<7% of eligible student population) were excluded from the sampling frame.33 Sampling weights were created within grades to ensure that each province and territory was proportionally represented.
A self-report questionnaire was administered to students, typically by teachers, during regular classroom time. For a student to participate, consent had to be obtained from the school jurisdiction, school principal and parent. The 2014 Canadian dataset includes information on 29 837 grades 6–10 students (typically ages 11–15), from 369 schools covering all 13 provinces and territories.
Patient and public involvement
The student voice was intentionally honoured in the development of the HBSC survey, but students did not contribute specifically to the development and conduct of this study.
Study variables
Creation of the dual-factor measure of mental health involved assessment of subjective well-being and psychopathology.
Subjective well-being (life satisfaction, positive and negative affect)
Life satisfaction was measured using the Cantril Ladder; involving referral to a picture of a ladder that students used to rate how they feel about their life from 0 (‘worst possible life’) to 10 (‘best possible life’).34 This simple scale correlates well with other measures of emotional well-being.35 Positive affect was assessed using the item: ‘Please show how much you agree or disagree with the following statement: ‘I am full of energy’. Responses were measured on a 5-point Likert scale (‘strongly agree’ to ‘strongly disagree’). This item is included in positive affect scales, such as the Geriatric Depression Scale-15.36 Negative affect was assessed using the following two items: (1) ‘I often feel lonely’, and (2) ‘I often feel helpless’ (five response options: ‘strongly agree’ to ‘strongly disagree’). The two items describing negative affect were strongly correlated (r=0.66) and were averaged into a single negative affect score. The feeling lonely item is from the Positive and Negative Affect Schedule for Children scale,37 and feeling helpless is in the Implicit Positive and Negative Affect Test,38 two validated negative affect scales.
Psychopathology (internalised and externalised symptoms)
Internalised symptoms were measured using the 4-item HBSC psychological symptoms subscale (Cronbach’s alpha=0.79) of an existing subjective health complaints scale.39 Students reported how often they experienced the following symptoms in the past 6 months: ‘feeling low (depressed)’, ‘irritability or bad temper’, ‘feeling nervous’ and ‘difficulties in getting to sleep’. Responses to the four items (0= ‘rarely or never’ to 4= ‘about every day’) were summed to create a total symptom score.
Externalised symptoms were assessed using an overt risk-taking scale that includes the following behaviours: frequency of alcohol consumption, lifetime drunkenness history, lifetime smoking history, use of alternative tobacco products, physical fighting, non-helmet use on a bicycle and caffeinated energy drink consumption (Cronbach’s alpha=0.75).40 This scale has been positively associated with reductions in health including reduced life satisfaction and emotional well-being, and worse self-reported general health status.40
Variables used to test the dual-factor measure
The construct validity of the dual-factor measure was assessed by examining whether variables known to be associated with mental health,29 30 differed between the mental health groups of the dual-factor measure in the expected manner (figure 2). These variables included family characteristics (family structure and affluence), specific indicators of mental health and measures of social support and academic functioning.
Demographics and family characteristics
Age in years at the time of survey completion was categorised as ≤11, 12, 13, 14 or ≥15 years old. For biological sex, youth self-identified as either ‘male’ or ‘female’. Relative family affluence (five categories recategorised into ‘well-off’, ‘average’, ‘not well-off’) was measured using the item: ‘How well off do you think your family is?’. Family structure was based on the adults who lived at the youth’s primary residence (‘both parents’, ‘mother and partner’, ‘father and partner’, ‘mother only’, ‘father only’, ‘other’).
Mental health indicators
Feeling hopeless (‘yes’ or ‘no’) was assessed using the item: ‘During the past 12 months, did you ever feel so sad or hopeless almost every day for two weeks or more in a row that you stopped doing some usual activities’. Persistent sadness and hopelessness are criteria for, and strong predictors of clinical depression.41 Prosocial behaviour was measured using a five-item scale (α=0.87)32 capturing whether youth engage in behaviours that put others before themselves (0= ‘definitely not like me’ to 5= ‘definitely like me’). Self-rated health status was assessed using the item ‘Would you say your health is…?’ (‘excellent’, ‘good’, ‘fair’ or ‘poor’).
Social support
Peer support was measured using a four-item scale (α=0.92), describing whether adolescents believe they have friends they can count on and talk to about their problems and sorrows.32 Family support was assessed using four items describing whether students believe their family is available and willing to help them in times of need (α=0.91).32 The composite measures ranged from 0 to 16 (item response options: 0= ‘strongly disagree’ to 4= ‘strongly agree’).
Academic functioning
Student support was measured with a three-item scale (α=0.80), that gauged students’ perceptions of their peers within the school environment (eg, students in their class are kind and helpful and enjoy being together) (response options: 0= ‘strongly disagree’ to 4= ‘strongly agree’).32 The items were summed to get a composite score ranging from 0 to 12. Teacher support was assessed using a nine-item scale (α=0.90).32 Four of the items related to the students perceptions of how their teachers felt about them, and the remaining five items related to how the students feel about their teachers (response options: 0= ‘strongly disagree’ to 4= ‘strongly agree’). The composite score ranged from 0 to 36, with a higher score reflecting greater teacher support. Academic performance was measured using five categories describing the students average marks during the past year (1=‘mostly letter grades below C/below 50 %/or level 1’, 2=‘mostly Cs/between 50% and 59%/or level 2’, 3= ‘mostly Bs and Cs/between 60% and 69%/or level 3’, 4=‘mostly As and Bs/between 70% and 84%/or level 3 and 4’, 5=‘mostly As/above 85%/or level 4’).
Analysis
All analyses were conducted using SAS V.9.4 (SAS Institute). A thorough description of the analysis decisions can be found elsewhere.42 The dual-factor measure was developed and described in adolescents with complete data on the indicators used to create the measure (n=21 993 (weighted n=22 166)). For the regression analyses, the sample was further restricted to those with complete data on all variables previously described (n=20 146 (weighted n=20 262)).
Development of the dual-factor measure of mental health
Indicators for subjective well-being and psychopathology were transformed into Z-scores with a mean of 50 and SD of 10, following precedent.19 21 Z-scores were created after stratifying by age group and gender, based on differential reporting by age and between boys and girls on the scales being considered.4 As a result youth were classified as high or low on the two dimensions relative to their peers of the same age and gender. The subjective well-being score was created by summing standardised scores for life satisfaction and positive affect, then subtracting standardised negative affect scores. Low subjective well-being was defined as a Z-score <40, based on common guidelines for identifying meaningful cut-offs.43 High psychopathology was defined as a Z-score ≥60 on either of the internalised or externalised symptoms scales, based on commonly used guidelines for determining clinically significant symptoms on other psychopathology scales.21 The dichotomous subjective well-being and psychopathology scores were then used to categorise youth into the four mental health groups defined according to the dual-factor model (figure 1).4 5
Testing the construct validity of the dual-factor measure
Frequency distributions were used to describe family characteristics and indicators of mental health, by mental health group. Spearman’s correlation coefficient was used to examine the correlation between indicators. Differences by mental health group were examined using Rao-Scott χ2 tests then multivariable, multinomial logistic regression was used to estimate ORs and associated 95% CIs. The latter produced adjusted estimates describing relationships between academic and social functioning and mental health status. The ORs represent the odds of belonging to one mental health group relative to another, associated with a one-unit change in the academic or social functioning variable. Regression models were also adjusted for age and sex. All models applied sampling weights and adjusted for clustering by school using random effects. To assist in comparisons, continuous covariates were rescaled to range from 0 to 10.
The Markov Chain Monte Carlo method44 of multiple imputation was used to assess potential bias resulting from missing data (35% of the full sample was missing one or more item). Effect estimates were generated based on ten imputed data sets using the full sample (n=29 837). The imputation model included all variables previously described in addition to the following: ethnicity, specific learning exceptionalities (attention deficit hyperactivity disorder (ADHD), learning disability, behaviour, language/speech impairment), frequency of going to bed hungry because there is not enough food at home and body satisfaction. These auxiliary variables were included because they are correlated with the incomplete variables in the analysis model, and could improve the prediction of missing values.45 The multinomial regression results generated from the imputation model were consistent with those from the complete-case analysis.
Results
The sample used to develop the composite measure of mental health (n=21 933 (weighted n=22 166)) was 53% female and an average age of 14.0 (SD=1.4) years old (table 1). Over half of the adolescents reported being from a well-off family, nearly three-quarters lived with both parents and 81% were born in Canada. The proportion of youth who fell into each of the four mental health categories was 67.6% mentally healthy, 17.5% symptomatic yet content, 5.5% asymptomatic yet discontent and 9.4% mentally unhealthy.
Description of the sample
Mental health status according to the dual-factor model differed by family structure and socioeconomic status, and specific indicators of mental health in the expected manner, providing support for the dual-factor measure as construct valid (table 2). The correlation between indicators was weak (rs=−0.23, p<0.001 for self-rated health and hopelessness) to negligible (rs=0.002, p=0.74 for prosocial behaviour and hopelessness).46 Mentally healthy youth were the most likely to live with both parents and report their family was well-off. They were much less likely than the other groups to report having felt hopeless in the past year (14% vs ≥41%) and were the most likely to engage in prosocial behaviour and rate their health as excellent. In contrast, mentally unhealthy youth were the least likely to live with both parents, and most likely to report that their family was relatively not well-off. Nearly 80% of the mentally unhealthy group reported feeling hopeless, and they were the group most likely to rate their health as fair or poor. When each pair of mental health groups was compared, all distributions were significantly different (Rao-Scott χ2, p<0.05), with the following exceptions: family structure in symptomatic yet content vs asymptomatic yet discontent youth (p=0.70), and prosocial behaviour in asymptomatic yet discontent and mentally unhealthy youth (p=0.48).
Description of the mental health groups by family structure, relative family affluence and specific indicators of mental health
Construct validity was assessed further by examining the associations between self-reported social support and academic functioning, and mental health status (table 3). Belonging to the mentally healthy group was associated with the most positive functioning (higher peer, family, teacher and student support, and higher average marks) (table 3; online supplemental figure 1). Among youth with high psychopathology, being symptomatic yet content was associated with higher support and better academic functioning. A one-unit increase in family support for example was associated with increased odds of being symptomatic, yet content compared with mentally unhealthy (OR 1.32; 95% CI 1.28 to 1.36). In youth reporting low levels of well-being, the absence of psychopathology was associated with more positive functioning. Compared with the mentally unhealthy group being asymptomatic yet discontent was associated with better functioning on all variables considered except for peer support (OR 0.98; 95% CI 0.95 to 1.01). Consistent with the theory of the dual-factor model falling into the mentally unhealthy group was associated with the worst functioning of the four groups.
Supplemental material
Results of multivariable multinomial logistic regression examining the odds of being in one mental health group versus another, associated with a one-unit increase in variables describing social support and academic functioning
Discussion
This analysis provides epidemiological evidence in support of the construct validity of a dual-factor measure of adolescent mental health status. Development of the measure was guided by an evidence-based theory arguing that an individual’s mental health status cannot be fully captured without consideration of two unique, but related dimensions: subjective well-being and psychopathology.5 Following precedents,5 18 the two dimensions were used together to categorise students into four groups. Construct validity was supported by findings that the four groups differed in the expected direction on variables known to be related to mental health.29 30 Complete mental health is associated with functioning well, including realising one’s abilities, working productively and maintaining healthy relationships.2 The mentally healthy group was, therefore, expected to be the highest functioning.
The proportion of youth who fell in each mental health group was consistent with previous studies.5 17–19 21 47 With respect to family characteristics, mentally unhealthy youth were the most likely to be from less affluent families, consistent with findings that lower socioeconomic status is associated with increased risk of mental health problems in adolescents.48 They were also the most likely to be living in a home with fewer than two adults, which is in keeping with findings that children from single-parent homes are at greater risk of social maladaptation and poorer psychological well-being.49 Symptomatic yet content youth reported higher family affluence than the two groups with low well-being, consistent with findings that higher socioeconomic status is associated with greater psychological well-being.50 The proportion of youth in each mental health group reporting feelings of hopelessness, fair or poor self-rated health status and engagement in prosocial behaviour was significantly different, suggesting the composite dual-factor measure more accurately differentiates mental health status than the individual indicators. The specific mental health indicators and family characteristics examined were not strongly correlated, suggesting that the consistent associations between these variables and mental health status according to the dual-factor measure is not explained by some other underlying factor.
Academic and social functioning was associated with group membership in the expected direction.4 5 Belonging to the mentally healthy group was associated with the most positive functioning and belonging to the mentally unhealthy group the worst. The one exception was that greater peer support increased the likelihood of belonging to the symptomatic yet content group compared with the mentally healthy group. The primary peer group of symptomatic yet content youth was more likely to engage in maladaptive risk-taking behaviours, including illicit drug and alcohol use (data not shown). While adolescents in this group may report greater peer support than the mentally healthy group, such peer relationships appear to be of negative quality, and potentially harmful to their mental health.
Most of the adolescents with low psychopathology also reported moderate to high subjective well-being (68%). This group would have been identified as mentally health using only one of the unidimensional measures of mental health. However, there were a substantial portion who fell into groups performing favourable with respect to one measure and unfavourable on the other. The asymptomatic yet discontent group (5.5% of the sample) had poorer academic functioning and perceived less social support than the mentally healthy group supporting the theory that low psychopathology does not equate to optimal or complete mental health. Similarly, symptomatic yet content youth (17.5%) had poorer functioning than the mentally healthy group supporting the notion that subjective well-being alone is not sufficient to ensure optimal mental health. Using only one measure, this piece of information would be lost.
This study adds to a growing body of literature pointing to the potential clinical relevance of using a dual-factor model of mental health.4 5 21 If the ultimate goal is to identify ways of protecting and fostering optimal mental health and functioning among adolescents, studies should be considering two dimensions of mental health. Mentally healthy youth according to the dual-factor measure are not only the highest functioning,5 19 21 they also appear to be the most stable over time, and least likely to experience future mental health problems.12 47
The main strength of this study is its novelty. It builds on an existing literature base by developing and testing the construct validity of a dual-factor measure of mental health in a large, national sample of Canadian adolescents. The study sample was representative of the Canadian population by immigration status and family structure, but adolescents from rural communities (population centre <1000) were under-represented (4.0% vs 19.3% of the Canadian population).51 The findings help address concerns about generalisability raised by previous studies on adolescents from select samples, most often in the Southeastern USA.5 21 Unique to this study, the cut-offs used to define ‘high’ and ‘low’ psychopathology and subjective well-being were calculated within strata defined by age group and gender. This approach prevented the grouping of mental health from being affected by the age and gender distribution of our sample. If differences in reporting by age group were not accounted for then the older adolescents in our sample would have an inflated likelihood of being categorised as mentally unhealthy compared with if the measure was developed in a sample of older adolescents. If duplicated across countries and cultures, including those in the HBSC network, it would provide further evidence of a robust measure with universal application to the study of mental health status in adolescent populations.
The analysis is limited, however, on its reliance on secondary data, and its restriction to available indicators collected as part of the HBSC study. As a result, single items were used to measure positive and negative affect, instead of the full scales,37 which may have more accurately captured those domains. The only available item for positive affect measured the adolescents’ energy level, which could be impacted by their physical health. Second, reliance on self-report data may be subject to socialdesirability bias, particularly for risk-taking behaviours such as alcohol use. Previous studies have overcome this limitation by using teacher report of externalised symptoms (conduct problems).5
Future studies operationalising a dual-factor measure should use validated diagnostic scales for assessing the presence or absence of well-being and psychopathology. This would allow the measure to be operationalised in smaller, non-representative samples. Keyes Mental Health Continuum suggests a diagnostic criteria for identifying well-being.8 Future studies could also consider other approaches to combining the two dimensions of mental health, such as a recent latent profile analysis described by Moore et al.52 A six group classification of mental health, combining the two dimensions has also been proposed.12
Conclusion
The results of this study support the construct validity of a dual-factor measure of adolescent mental health. Adolescents in each group reported unique patterns related to their level of social and academic functioning. Findings highlight the importance of integrated measures for accurately and comprehensively classifying mental health status. Measures that consider only one dimension imply the risk to overlook clinically relevant information. Application of the dual-factor measure in population health research increases our potential to understand and improve the mental health of adolescents.
Data availability statement
Data may be obtained from a third party and are not publicly available. The HBSC Data Management Centre coordinates the work with the HBSC data, and is the Data Bank for the HBSC-study. The centre distributes data in accordance with the HBSC data access policy. Web: http://www.hbsc.org/.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approval for the study was granted by Research Ethics Boards from both Queen’s University (GREB TRAQ #: 6010236) and PHAC/Health Canada (REB 2013-0022).
Acknowledgments
We thank members of the international and national HBSC team. The international coordinator of the HBSC survey is Dr Jo Inchley, University of St. Andrews, Scotland. The international databank manager is Dr Oddrun Samdal, University of Bergen, Norway. The Canadian principal investigators of the 2014 HBSC were Drs John Freeman and William Pickett, Queen’s University, and its national coordinator was Matthew King. We would also like to thank the Brock University, James A. Gibson Library Open Access Publishing Fund.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @colleendavison
Correction notice This article has been corrected since it first published. The acknowledgements section has been updated.
Contributors WP and CMD helped lead the HBSC survey in Canada, and provided access to the data. NK led the conception of the study and the writing of the manuscript, and performed the statistical analysis. WP and CMD critically reviewed the analysis and writing for important intellectual content, and assisted with editing and revision of the article. All authors read and approved the final manuscript.
Funding This work was supported by The Public Health Agency of Canada and the Canadian Institutes of Health Research (grant numbers MOP341188 and FRN-130379).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.