Article Text

Abstract
Objectives Obstructive sleep apnoea (OSA)/hypopnoea syndrome is associated with serious and major multiorgan morbidities, particularly in its most severe forms. However, no severe OSA screening instruments are available for high altitude residents that enable adequate identification and clinical prioritisation of such patients. We aimed at developing a severe OSA prediction tool based on the clinical characteristics and anthropometric measurements of a clinical referral cohort living at 2640 m.a.s.l.
Design Cohort-nested cross-sectional study.
Setting Sleep laboratory for standard polysomnography (PSG) in Colombia.
Participants A predictive model was generated from 8718 participants referred to the PSG laboratory. Results were subsequently validated in a second cohort of 1898 participants.
Primary outcome To identify clinical and anthropometric variables associated with severe OSA (>30 events/hour) and to include them in a binary logistic regression model.
Results The significant variables that were retained with the presence of severe OSA included Body mass index (BMI), Age, Sex, Arterial hypertension and Neck circumference (BASAN). The area under the receiver operating characteristic curvefor the BASAN index was 0.69 (95% CI: 0.68 to 0.70) in the derivation cohort and 0.67 (95% CI: 0.65 to 0.69) in the validation cohort, whereby a BASAN index ≥2 had a sensitivity of 95% and a specificity of 17% to detect severe OSA.
Conclusion An objectively based approach to screen for the presence of severe OSA, the BASAN index, exhibits favourable sensitivity characteristics that should enable its operational use as a screening tool in a Hispanic population with a clinical suspicion of OSA and living at high altitude.
- sleep medicine
- altitude medicine
- hypertension
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified participant data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study used data drawn from a large patient cohort attending a sleep laboratory at high altitude in which all patients had a polysomnography for a definitive diagnosis of obstructive sleep apnoea (OSA)/hypopnoea syndrome.
We described a rigorous approach to evaluate variables that are used in multiple tools for the diagnosis of OSA and identified a logistic model that uses simple variables with favourable performances for the diagnosis of this disease.
There was a possibility of a confounding bias and omission, as with any observational study.
Introduction
Obstructive sleep apnoea (OSA)/hypopnoea syndrome has a very high prevalence around the world1–3 and has been associated with significant increases in the risk of hypertension,4 coronary artery disease,5 6 stroke7 8 and sudden death.9 Furthermore, highlanders suffering from OSA have a higher prevalence of pulmonary hypertension, which therefore prioritises the detection of OSA in a timely fashion in high altitude residents.10–12 OSA has also been associated with a higher rate of traffic accidents, cognitive behavioural disorders and alterations in the overall quality of life. This ultimately results in an increased all-cause mortality and, as such, is considered a major public health problem.13 Standard overnight in-laboratory polysomnography (PSG) is the diagnostic test of choice for this condition, but it requires a significant resource infrastructure. Unfortunately, in most countries, a limited availability of PSGs precludes timely referrals and diagnoses for a large majority of these patients. These issues have fostered efforts aimed at developing clinical instruments that reliably predict the risk of OSA14 15 and to allow for rational prioritisation of high-risk patients. Two types of instruments have gained wide implementation. The first type is based on a mix of subjective reporting by the patients and objective office-based measures and includes the Epworth Sleepiness Scale (ESS),16 the Berlin questionnaire,17 snoring, tiredness, observed apnoea, blood pressure (STOP);18 STOP, body mass index (BMI), age, neck circumference, gender (STOP-Bang);19 and more recently, the neck, obesity, snoring, age, sex (NoSAS).20 21 The second type is based on simplified objective screening tools (No-Apnoea).22–24
Among the most widely used instruments is the ESS. However, this tool was created to measure diurnal sleepiness and not meant as a screening tool for OSA. Not surprisingly, its performance is clearly inferior to later instruments in this regard.24–26 Other frequently used instruments are the Berlin14–18 and STOP questionnaires, which primarily rely on self-reported symptoms. The Berlin questionnaire consists of 10 items related to snoring, non-restorative sleep, drowsiness while driving, apnoeas during sleep, arterial hypertension and BMI.17 It has a sensitivity and specificity of 80% and 46%, respectively, when the OSA is defined as having an apnoea–hypopnoea index (AHI) ≥5 events/hour. Furthermore, it has a sensitivity of 91% and specificity of 37% when OSA is defined as an AHI ≥15 events/hour.27 The STOP-Bang questionnaire is an eight-item survey that incorporates information about STOP, BMI, age, neck circumference and gender. For the diagnosis of OSA, a score ≥5 has a sensitivity and specificity of 85% and 53%, respectively; using a threshold of AHI >15 events, there is a sensitivity and specificity of 91% and 40%, respectively; and using a threshold of AHI >15 events/hour, there is a sensitivity and specificity of 95% and 35%, respectively.18 Conversely, we recently reported a two-item tool that is predicated on neck circumference and age. This tool has exhibited favourable screening capabilities as evidenced by an accuracy of 78.1%, 68.8% and 54.4%, respectively, for OSA ≥5, OSA ≥15 and OSA ≥30 events/hour.22
Approximately 2.3% of the world’s population lives between 2000 and 2500 m.a.s.l. This means that there are approximately 178 million people residing at such high altitude, with an additional 60 million people living between 2500 and 3500 m.a.s.l. (high altitude, class 3 of the mountain classification of the United Nations Environment Programme).28 The effects of altitude on sleep have been described since the beginning of the 20th century.29 These effects include a higher frequency of periodic breathing, central sleep apnoea, increased risk of oxyhaemoglobin desaturation events during sleep, frequent awakenings and a decrease in the proportion of slow wave sleep.30 These effects become apparent in non-acclimated people at altitudes of 2000–2500 m.a.s.l.28 30–32 Although these effects are mitigated with acclimatisation,33 34 an implementation of the aforementioned screening instruments may be underperforming. Thus, they may require the development of better tailored tools for sleep apnoea screening that are specifically designed for these populations and in whom the prevalence of respiratory disorders during sleep may be higher than at sea level. Our aim in this study was to develop a simple screening tool that enables the reliable detection of patients with severe OSA who are living at 2640 m.a.s.l. Moreover, this tool would be based on objectively assessed clinical characteristics and anthropometric measurements.
Methods
This was a cross-sectional study nested in a cohort of a sleep laboratory in the city of Bogotá, Colombia. Included in this study were adult patients (age >18 years) referred for a standard polysomnographic study due to a clinical suspicion of OSA and living in Bogotá, a city at 2640 m.a.s.l. Exclusion criteria were patients treated surgically (correction of the upper airways) or medically (continuous positive airway pressure or bilevel positive airway pressure) for OSA. Other exclusion criteria included craniofacial alterations, a history of other sleep or cognitive disorders, psychiatric or muscle wasting diseases, patients whose sleep studies revealed a proportion of central apnoeas >10% of all events, and those with other comorbidities in advanced stages (chronic obstructive pulmonary disease, cardiac insufficiency and severe arrhythmias).
Information was retrieved from the electronic databases containing the medical records of all patients who underwent a standard PSG between February 2007 and January 2017. A total of 10 478 eligible consecutively studied patients were identified. There were 8580 patients corresponding to the period between February 2007 and December 2014 who were used for the construction of the instrument. Another 1898 patients were then recruited from January 2015 to January 2017 whose data were used for tool validation.
Immediately before each PSG, age, sex, weight, height, BMI, neck circumference at the level of the cricoid cartilage, a history of arterial hypertension and blood pressure measurements were collected. Other collected data included the presence of daytime sleepiness, as measured by the ESS, sleep onset insomnia, maintenance insomnia, night awakenings, non-restorative sleep, sleepwalking, nightmares, leg movements, sweating, heartburn, dry mouth and the Berlin questionnaire.
PSGs were performed during natural nighttime sleep at the patient’s usual bedtime. The PSG was performed using the Alice 5 and 6 digital systems (Philips Respironics, Pennsylvania, USA). Standard electroencephalography, electro-oculography, mandible and leg electromyography, nasal and oral airflow, electrocardiography, respiratory effort and oxygen saturation were included. The PSG was manually scored by a certified technician and reviewed by a physician certified in sleep medicine.
Sleep stages and respiratory events were scored according to the recommendations of the American Academy of Sleep Medicine (AASM) Manual for Scoring of Sleep and Associated Events 2007.35 36 The clinical diagnosis of OSA was defined by an AHI ≥5 events/hour of sleep, with symptoms of sleep fragmentation and daytime somnolence, according to the AASM. The severity of OSA was determined according to the AHI as follows: mild, 5–14.9; moderate, 15–30; and severe, greater than 30 events/hour of total sleep time. Hypopnoea was defined as a significant decrease in the baseline amplitude of a valid measure of breathing for at least 10 s during sleep, along with an oxygen desaturation of ≥3% or an arousal.37
Statistical analysis
Data are presented as mean±SD for quantitative variables and frequencies (absolute and relative) for qualitative variables. Bivariate analyses were initially conducted and the variables that were associated with OSA were identified. The independent variables included age, sex, weight, height, BMI, neck circumference, arterial hypertension, snoring, sleep apnoea, choking and fatigue. Other independent variables included daytime sleepiness, muscle weakness, insomnia, night awakenings, waking up to go to the bathroom at night, non-restorative sleep, sleepwalking, nightmares, leg movements, sweating, heartburn and mouth dryness. Finally, those variables that showed statistical significance and biological plausibility were included in the construction of the severe OSA prediction model. Cut-off values for continuous independent variables were derived from receiver operating characteristic (ROC) curves. Missing data were completed using multiple imputation procedures prior to statistical analysis.
The cohort of patients recruited from 2007 to 2014 served for development of the prediction model. Through logistic regression analyses, associations of the different variables with the crude and adjusted OSA outcomes were quantified. Based on these findings, the construction and fit of the model were explored, while identifying interaction, confusion and collinearity. A two-tailed value of p<0.05 was considered statistically significant. Validation of the instrument to test the goodness of fit and discrimination capacity was performed in a patient population different from that used to develop the model (the cohort recruited from 2015 to 2017). All statistical analyses were performed using the statistical packages SAS V.9.4 and STATA V.14, and Microsoft Office Excel 2016 was used to build the databases.
Patient and public involvement
No patients were involved.
Results
The data from 10 478 patients were included in the study, with 8580 (82%) serving to develop the model, and the remaining 1898 (18%) used for validation of the model. The patients identified themselves predominantly as Hispanics. The prevalence of OSA in this high-risk clinical referral population was 94.8%, with 49.2% having severe OSA. The mean age was 53.5±14.3 years, BMI was 30.1±6.3 kg/m2, neck circumference was 38.6±4.2 cm and 54.5% had arterial hypertension (table 1). Additionally, as the OSA severity increased, age, BMI, neck circumference, snoring and the prevalence of arterial hypertension also increased (tables 1 and 2). A weak correlation between BMI and neck circumference was observed (r=0.4). No significant differences emerged in ESS and the presence of OSA (ESS: 10.1±6.0) or absence of OSA (ESS: 10.2±6.1) (p=0.4). Variables, including age, BMI and neck circumference, were then dichotomised based on the optimal cut-off point obtained from ROC curves (figure 1), with determination of cut-offs of greatest discrimination carried out according to the Youden index. These cut-off points were 38.9 cm for neck circumference, 28.5 kg/m2 for BMI and 54.5 years for age. With these dichotomous variables, we proceeded to construct the various models (table 3).
General characteristics of the cohort
Clinical and anthropometric variables associated with severe OSA (AHI >30 events/hour TST)
Cut-offpoints with greater discriminatory capacity (Youden index) for the variables associated with severe OSA
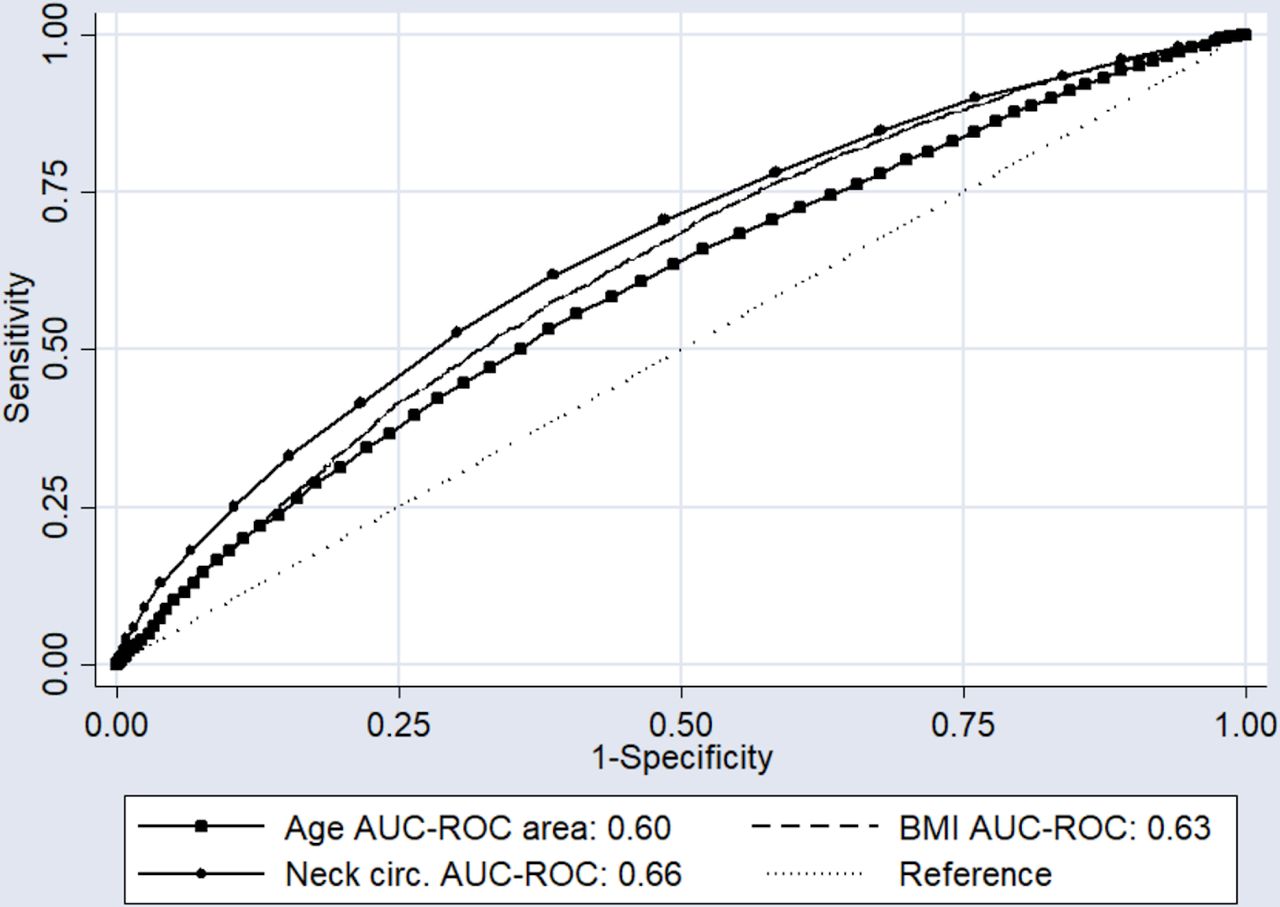
ROC curves for predictor variables in the derivation cohort. AUC-ROC (binomial exact) in the derivation cohort of age: 0.60 (95% CI: 0.59 to 0.61); BMI: 0.63 (95% CI: 0.62 to 0.64); and neck circumference: 0.66 (95% CI: 0.65 to 0.67). AUC-ROC, area under the receiver operating characteristic curve; BMI body mass index; circ., circumference.
Seven models were generated by the stepwise forward logistic regression method, leading to the selection of the most parsimonious model, with a coefficient of determination of R2=0.09. This model included the following variables: male sex, age (≥55 for the general predictor model, >50 years for the male model and ≥55 for the female model), neck circumference (≥39 cm for the general predictor model, >41 cm for the male model and ≥36 cm for the female model), BMI (≥30 for the general predictor model, >28 kg/m2 for the male model and ≥30 for the female model) and the presence of arterial hypertension. For each of these variables, the ORs were calculated (tables 4–6). Finally, scores were assigned to each of the variables according to the value of the adjusted ORs (tables 4–6), assigning 2 points for each of the five variables present to obtain a score between 0 and 10 for the general predictor model and between 0 and 8 for the male/female specific models. Such variables were summarised with the acronym BASAN (BMI, Age, Sex, Arterial hypertension and Neck circumference), which is the proposed screening instrument for severe OSA.
General predictive model for severe OSA (most parsimonious)
Predictive model for severe OSA in men (most parsimonious)
Predictive model for severe OSA in women (most parsimonious)
Regarding the validation of the BASAN index in terms of discrimination and goodness of fit, an area under the curve (AUC)-ROC of 0.69 (95% CI: 0.68 to 0.70) was obtained in the derivation cohort, and 0.67 (95% CI: 0.65 to 0.69) in the validation cohort (figure 2). The fit of the model according to the Hosmer-Lemeshow test was good for all score categories of the scale, with a value of χ2=3.87 (p=0.42). The cut-off point of the BASAN index (general model) with greater discriminative capacity was ≥4 points, which showed a sensitivity of 82.1% and specificity of 40.4% with corresponding positive likelihood ratio 1.4 and negative likelihood ratio 4 to detect severe OSA. In contrast, a BASAN index ≥2 had a sensitivity of 95% and specificity of 17% to detect severe OSA in the validation cohort. Additional cut-off points with their corresponding sensitivities/specificities and Likelihood ratios (LRs) may be found in the online supplemental tables S1 and S2. The overall predictive properties of the BASAN index were remarkably similar and stable in both the derivation and validation cohorts.
Supplemental material

{kind=link}
{kind=link}
ROC curves of the general, female and male models to predict severe obstructive sleep apnoea in the derivation and validation cohorts. (A) General model in the derivation cohort. (B) General model in the validation cohort. (C) Female model in the derivation cohort. (D) Female model in the validation cohort. (E) Male model in the derivation cohort. (F) Male model in the validation cohort. AUC-ROC markers correspond to model total score (2 points per each predictor positive according to tables 5–7). AUC-ROC (binomial exact) general model in the derivation cohort: 0.69 (95% CI: 0.68 to 0.70); general model in the validation cohort: 0.67 (95% CI: 0.65 to 0.69); female model in the derivation cohort: 0.69 (95%CI: 0.67 to 0.70); female model in the validation cohort: 0.64 (95% CI: 0.61 to 0.68); male model in the derivation cohort: 0.65 (95% CI: 0.63 to 0.66); and male model in the validation cohort: 0.63 (95% CI: 0.59 to 0.67). AUC-ROC, area under the receiver operating characteristic curve.
The predictive model for severe OSA in men aged ≥50 years, neck circumference ≥41 cm, BMI ≥28 kg/m2 and arterial hypertension is shown in figure 2 and table 5. The model for women aged ≥55 years, neck circumference ≥36 cm, BMI ≥30 kg/m2 and arterial hypertension is shown in figure 2 and table 6. The scoring methods for men and women were similar, assigning a score of 2 for each positive predictor, for a maximum score of 8 points in both models (tables 5 and 6). In the male model, a score ≥2 had a sensitivity of 93% and a specificity of 20% to predict severe OSA, while in the female model, a score ≥2 had a sensitivity of 95% and a specificity of 17% to predict severe OSA. Higher scores had better specificities at the expense of sensitivity, as shown in the online supplemental tables S3–S6. The reader can use these tables to select cut-off points that better fit specific aims.
Several cluster analyses were performed as shown in the online supplemental figures S1–S6 with similar discriminant capacity in all figures, except in the cluster of snoring patients where the model showed a higher AUC-ROC of 0.70 (online supplemental figure S6). We also obtained the percentiles for each quantitative predictor variable (age, BMI and neck circumference) for men and women according to the AHI (table 7), which may be used as a reference for a population living at moderate to high altitudes.
Percentiles of quantitative predictor variables according to AHI
Discussion
In the present study, a screening instrument for the presence of severe OSA was developed and validated in a large cohort of patients living at high altitude and clinically referred for PSG due to a clinical suspicion of OSA. Interestingly, we found five variables that were significantly related to the presence of severe OSA, namely male sex, age older than 50 years for men and 55 years for women, neck circumference greater than 41 cm for men and 36 cm for women, BMI greater than 28 kg/m2 for men and 30 kg/m2 for women, and the presence of arterial hypertension. Based on their relatively similar contributions to the risk of suffering from severe OSA, we attributed a similar scoring approach to each of the variables and constructed the BASAN screening instrument. The performance of this tool was obviously designed to screen rather than diagnose severe OSA, as reflected by the very high sensitivity and low specificity. The BASAN index was then validated in a subsequent relatively large cohort of nearly 1900 patients with virtually identical findings.
In our study, we found that patients with mild, moderate and severe OSA had mean BMI values of 28, 29 and 31 kg/m2, respectively, consistent with the AASM guidelines, which recognises the risk of OSA above a BMI of 30 kg/m2. However, our cut-off values were slightly different from those reported in studies conducted at sea level and are more consistent with our clinical empirical observations among high altitude residents. A similar BMI cut-off was also described in the Berlin questionnaire, and by Takegami and colleagues38 in the 4-Variable tool for screening patients with OSA. In contrast, the STOP-Bang scale recognises the risk of OSA starting at a BMI greater than 35 kg/m2, an age greater than 50 years and a neck circumference greater than 40 cm.19 Such values were different in our study, which found lower cut-off values than the majority of those reported in the literature. Therefore, our values may simply reflect the characteristics of the Hispanic population living at altitudes around 2600 m.a.s.l. This may further reinforce the concept that regional differences around the globe require careful tailoring and validation of any screening instrument to the population of interest, rather than assuming that one size fits all.
The clinical attractiveness of the BASAN index is first and foremost predicated on the fact that it was developed through a fairly parsimonious model, and that the five items retained are easy to measure and readily available in any clinical practice. Thus, the BASAN index should enable primary care clinicians to assign a probability of severe OSA among their patients living at high altitudes, a critically useful feature enabling prioritisation of care to those patients who require a more immediate diagnosis and treatment. However, the derivation and validation of the BASAN tool was conducted in patients with high pretest probability. For a disease like OSA, it is potentially more important that a screening test has a high sensitivity rather than a high specificity.14 Nevertheless, this approach is not unanimously endorsed, and an earlier study has shown that the strategy of different cut-off points for any screening instrument may be interesting depending on the specific aim to confirm or exclude OSA.39 In addition, in a population with an elevated prevalence of OSA, such as in a sleep laboratory, using a screening instrument that exhibits a high sensitivity, such as the BASAN index, might lead to increases in the false positive rate. While sensitivity and specificity are not altered by the prevalence of the disease, predictive values are largely dependent on disease prevalence in the population of interest.40 41 It is therefore possible that exploration of other cut-off values for BASAN that modulate between sensitivity and specificity may be of greater interest in clinical practices or regions in which a lower prevalence of OSA prevails, such as in primary care.
Our large sample size allowed us to include heterogeneous subjects and to address the impact of such heterogeneities in the predictive capacity of the model. Furthermore, we assigned scores to the variables included in the model based on standardised B coefficients and ORs according to the most rigorous validity processes.42 The STOP questionnaire included 211 patients who underwent PSG to classify them as high risk and to then define the cut-off points of the variables according to their positive predictive values. These cut-off points were as follows: age >50 years, BMI >35 kg/m2, neck circumference >40 cm and sex; however, by not taking into account the negative predictive values, there are limitations in the discrimination capacity for each variable.17 43 Subramanian et al developed the neck circumference, airway classification, comorbidities, Epworth scale and snoring (NAMES) scale43 by enrolling 659 Hispanic and Caucasian adults living at altitudes close to sea level who were referred to a sleep laboratory due to a clinical suspicion of OSA. In their study, the cut-off points were defined according to the literature and expert opinions, an approach that may lead to suboptimal selection of cut-off points relative to the test candidate population. The NAMES scale achieved similar performance characteristics to the Berlin questionnaire,13 16 with AUC-ROCs ranging from 0.64 to 0.66 and sensitivities from 91% to 99% (higher than the ESS)44 and specificities between 9% and 27%. The addition of BMI and sex to this tool improved the detection of OSA, concluding that the NAMES scale is an effective and economic screening strategy in patients with moderate to severe OSA.43 The methodology used for the development and validation of our BASAN index enabled higher AUC-ROC. There was also an improved balance between sensitivity (82%) and specificity (41%) than with NAMES, as well as those of other instruments developed for OSA detection, including the Berlin, STOP and STOP-Bang questionnaires.44–46
Limitations and strengths
In the bivariate analysis, we did not find an association between ESS scores and OSA. This is consistent with the findings of most previous studies because the ESS was designed to evaluate daytime sleepiness, as it is one of the most common symptoms of OSA, and not to discriminate the severity of OSA.24 47–53 The frequent use of the ESS in our country to make decisions about the need for a PSG may have affected its a priori discriminatory ability, particularly when considering that our cohort had mean ESS scores of 10. Our study included a low proportion of patients without OSA, a factor that clearly limited our ability to develop a predictive model for mild OSA. Notwithstanding, the population of our study reflects the characteristics of Hispanics living at altitudes around 2600 m.a.s.l. who are usually referred for PSG. Furthermore, the BASAN index should allow for the detection of those patients at higher risk of severe OSA, who would be the priority group for referral to PSG. On the other hand, as with any observational and retrospective study, there is a risk of confounding bias and omission. To circumvent this risk, we adhered to the existing recommendations for the construction of logistic regression models.42
Conclusion
The BASAN index showed adequate discrimination and calibration for predicting severe OSA. The greatest utility of the BASAN index is in the selection of symptomatic patients living at high altitudes who are at the highest risk for morbidities and therefore should be a priority for a diagnostic PSG and treatment. Future implementation and validity corroboration of this instrument among primary care settings will be required.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Deidentified participant data.
Ethics statements
Ethics approval
The Institutional Review Board Investigation Subcommittee of the Universidad de La Sabana, Chía, Colombia, approved this study (Act No. 450 of 9 November 2018). According to resolution number 8430 of 1993, Ministry of Health of Colombia, this study is considered an investigation without risk. Therefore, national legislation personal data protection is required but not informed consent.
The study was approved by the institutional review board of the Ondina Clinic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @luisfgiraldo
Contributors HO, RL, LFGC and KH had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. HO, RL, LFGC, AB, CB, RB, LP, KH and DG contributed substantially to the study design, data analysis and interpretation, and the writing of the manuscript. HO and LFGC contributed substantially to data statistical analysis.
Funding This study was founded by Universidad de La Sabana, grant: MED-211-2016. DG is supported by National Institutes of Heath grants 1R01HL130984 and R56 HL140548.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer-reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.