Article Text

Abstract
Introduction Frailty refers to a multifaceted age-related loss of physiological reserve. Aside from the immediate challenges it presents, it is also associated with various adverse health outcomes. Given our ageing population, the healthcare and societal costs resulting from frailty present a significant and growing public health challenge. Rapidly accumulating evidence suggests that resistance exercise combined with protein supplementation can reverse frailty in older adults. However, translation of these findings into practice has proven difficult, due to either a lack of clarity regarding the interventions used or the use of interventions not suitable for widespread implementation. There remains an absence of evidence-based programmes suitable for delivery to frail older adults in the community.
Methods and analysis This paper outlines the protocol for a study to examine the effect of a novel programme of exercise and protein supplementation. This intervention has been developed by an expert consensus group, specifically for delivery to frail older adults in a group setting in the community. The study will take the form of a within-subjects non-randomised trial. Participants will be assessed at baseline, then following an 8-week period of regular activity, then following the 8-week intervention. Frailty (according to the Fried Frailty criteria) will be the primary outcome measure, along with a range of secondary outcome measures (including physical performance measures, body mass composition, psychosocial assessments and frailty-related biomarkers). If shown to be feasible to implement and effective at reversing frailty, the Diet and Exercise for FRAILty (DEFRAIL) intervention may facilitate more widespread participation in resistance exercise for frail older adults.
Ethics and dissemination This study received ethical approval from the Research Ethics committees of both the Health Service Executive South-Eastern Area and Waterford Institute of Technology. Its findings will be disseminated through journal publications, conference presentations and other forms of public engagement.
Trial registration number ISRCTN46458028; Pre-results.
- geriatric medicine
- rehabilitation medicine
- sports medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Novel exercise and protein intervention, specifically designed for frail older adults by expert consensus, with a focus on suitability for real-world implementation.
Inclusive eligibility criteria.
Comprehensive assessment of frailty and associated measures.
Single-site study.
Non-randomised study design.
Introduction
Frailty refers to a loss of physiological reserve and increased vulnerability to external stressors.1 It is known to be associated with ageing but is not an inevitable consequence of the ageing process. In addition to conferring increased mortality risk on older adults,2 frailty is accompanied by a range of adverse health outcomes, including falls, fractures and functional impairment.3 It impairs quality of life,4 results in earlier institutionalisation5 and increases healthcare usage, with healthcare-associated costs for frail older adults multiple times that of the non-frail.6 7
For these reasons, the prevention or reversal of frailty has the potential to significantly benefit older adults and society as a whole. As a result, much effort has gone into identifying a cost-effective means of countering frailty, with a growing consensus emerging. A recent systematic review concluded that the combination of resistance exercise and protein supplementation is ‘the most effective and easiest to implement intervention to delay or reverse frailty’.8 In the majority of studies included, the exercise component was delivered as part of a multicomponent exercise programme, that is, including aerobic, balance and flexibility training, in the form of a group class.9–11 This concurs with the findings of another systematic review,12 which found group interventions to be more effective than those performed individually, as well as providing better value for money, particularly for very frail older adults. There is also strong evidence that such interventions are most effective when combined with a nutritional intervention, with a focus on protein supplementation.13 14
This growing evidence base has resulted in incorporation of recommendations for strength training into physical activity guidelines for older adults by a number of public health bodies, including the recently revised UK government physical activity guidelines.15 This has been complemented by international guidelines advocating a higher target protein intake of at least 1.2 g/kg bodyweight/day for older adults engaged in regular exercise.16 Unfortunately, despite these recommendations, uptake of exercise programmes17 and levels of dietary protein-intake18 among community-dwelling frail older adults remains poor. Despite a willingness among older adults to engage in regular exercise,19 one of the main barriers reported is a lack of ‘age appropriate programmes’.20
To better understand this issue, exercise interventions reported in the literature were analysed using the Frequency, Intensity, Time, Type, Volume, Progression (FITT-VP) framework of the American College of Sports Medicine Guidelines for Exercise Testing and Prescription.21 This process revealed some important barriers to translating the evidence base for resistance exercise and protein into practice. Unfortunately, many studies provide incomplete information on the exact nature of their programmes, while others are impractically time-consuming, labour-intensive or costly to implement on a wider scale (table 1). In order to bridge the gap between research and clinical practice, it became clear that it would be necessary to design and implement a novel intervention, suitable for the majority of frail older adults and deliverable in a community setting.
Breakdown of exercise interventions used in various studies using FITT-VP framework
The aims of this research project are translational in nature. We aimed to address this important gap by designing a novel programme, combining exercise and protein supplementation, that can be easily replicated in a non-clinical setting by non-medical professionals. We now plan to deliver this intervention in a community setting and to evaluate its ability to reverse frailty and improves other related measures in frail older adults.
Methods and analysis
Intervention development
Modified Delphi process
Given the multidisciplinary expertise required to develop a novel intervention to reverse frailty, a modified Delphi process was felt to be a suitable approach (figure 1). This is ‘a well-recognised consensus method used to determine the extent of agreement on an issue’.22 The aim was to design a programme of exercise and protein supplementation by expert consensus that would be (1) acceptable to individuals across a range of degrees of frailty, (2) deliverable by non-specialists in a non-clinical setting as a group class and (3) effective at reversing frailty. This approach allowed us to combine the available evidence-base with clinical experience from a range of relevant disciplines, including Geriatric Medicine, Sport and Exercise Science, General Practice, Sports Medicine, Geriatric Nursing, Physiotherapy and Nutrition and Dietetics (see acknowledgements for details).
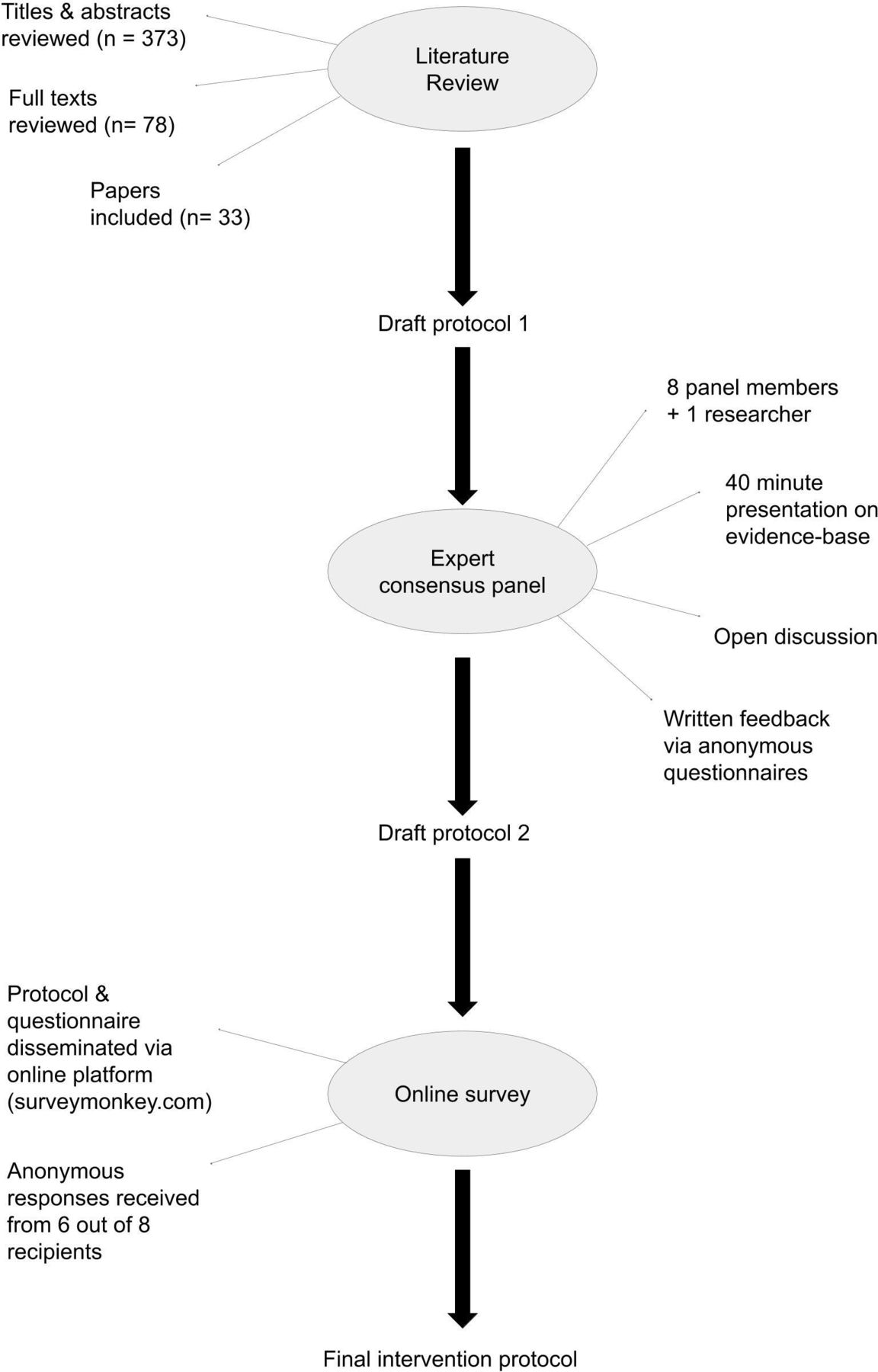
Stages of modified Delphi process.
During the introductory meeting, the current evidence base was presented to attendees, along with an initial draft exercise programme, to provide a basis for discussion. Areas where a lack of clear evidence existed were highlighted and discussed. Time was given to open debate regarding any other elements that attendees felt required further discussion. An anonymous questionnaire, using a range of question formats to explore these issues, was distributed to all attendees. Following this meeting, the results of the standardised anonymous feedback and group discussion were used to modify the initial draft programme. This revised draft was distributed electronically to all panel members, with an online survey (www.surveymonkey.com) used to receive further anonymous feedback. Examples of programme elements that were decided by consensus at this stage were: a class duration of 60 min; three classes per week; an 8-week programme duration; a focus on resistance over aerobic/balance exercises; 10–12 participants and two instructors per class.
Additionally, there was consensus that the exercise programme should be supplemented by additional dietary protein, in-keeping with international guidance that older adults engaged in exercise or otherwise physically active should aim for a higher daily protein intake (≥1.2 g/kg body weight/day).16 A decision was taken to opt for a commercially available milk-based supplement. To decide on the preferred preparation, an informal taste test was conducted among attendees to one of the Geriatric Medicine clinics of a large regional teaching hospital (n=11). This included three flavours of protein-supplemented milk and four varieties of a flavoured milk preparation (without protein supplementation). The outcome was one of broad satisfaction with each preparation (protein supplemented milk/flavoured milk), with a range of preference of flavours within each product group. As a result, protein milk was chosen as the most appropriate product, to be consumed as two doses of 250 mL two times per day. The first portion is to be consumed with breakfast and the second immediately after the exercise class (on ‘training’ days) or with lunch (on ‘non-training’ days).
This approach was based on a number of factors. This preparation was felt to represent the optimal balance between protein content, palatability, availability and cost. The dosing regimen is based on the evidence that distributing protein supplementation across the two typically protein-inadequate meals of the day, namely breakfast and lunch, may achieve greater overall stimulation of muscle protein synthesis.23 Additionally, consuming the second dose immediately after the classes on ‘training days’ is predicated on evidence of increased benefit with protein intake in the postexercise period in older adults.24 25 The 250 mL dose would provide an additional 12.5–14 g of additional protein (depending on flavour), in a similar range to the 20 g supplement advised by one paper.24 A nutritional breakdown of the plain flavoured protein milk is provided in table 2.
Nutritional information for Avonmore protein milk (plain flavour)
Pilot
Following the above steps, the final stage in the development of the intervention was a 4-week pilot, using potential recruits who were found to be insufficiently frail for inclusion in the main study. Examples of changes to the programme that were incorporated as a result of feedback from these individuals included: provision of transport; limitation of equipment to resistance bands and chairs; removal of several exercises that were unsafe or overly challenging; and reduction from four stations to three. This is described in greater detail below in ‘patient and public involvement’ (PPI).
Study design
The Diet and Exercise for FRAILty (DEFRAIL) trial will take the form of a non-randomised, single-group, pretest/post-test study, with repeated measures at three time-points over an 18-week period (see figure 2). This trial design was chosen as it was felt to be feasible to deliver, will offer all participants the opportunity to avail of the intervention, and will provide a monitored control period. Participants will undergo a baseline assessment, followed by 8 weeks of regular activity (during which time, participants will be advised to make no change to their diet or usual level of physical activity). After this period, they will be assessed again, before commencing the DEFRAIL intervention (attendance of >60% will be required for inclusion in the final analysis). Following completion of this 8-week programme, they will undergo a final assessment (see figure 2 and Standard Protocol Items: Recommendations for Interventional Trials figure). This will allow comparison of changes in outcome measures over the control period with changes over the intervention period. Due to constraints on the numbers of participants per class, the intervention will be conducted multiple times over the course of several months to achieve the desired sample size. Participants will not be monitored beyond the postintervention time point in the current study.
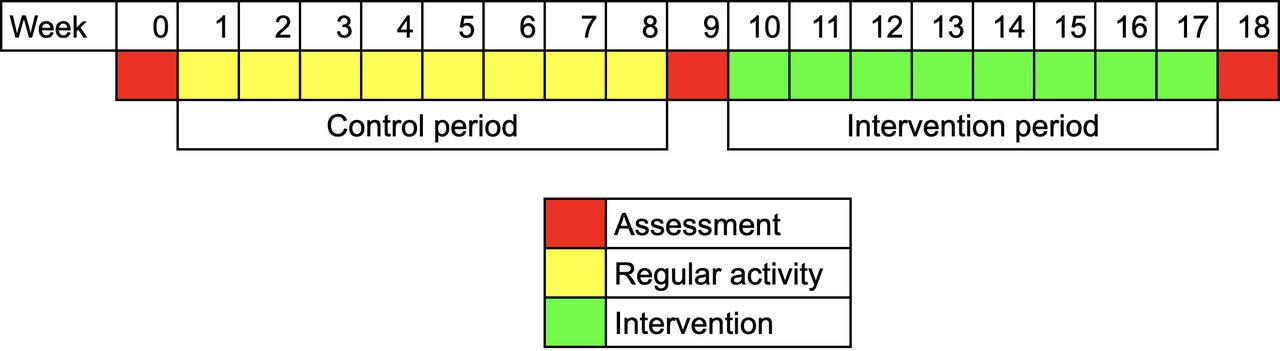
Non-randomised, single-group, pre-test/post-test study design.
Inclusion and exclusion criteria
The eligibility criteria are as follows:
≥ 65 of age.
Considered frail by the multidisciplinary team (MDT), that is, a score ≥5 on the Rockwood Clinical Frailty Scale (CFS),26 a 9-point scale ranging from ‘very fit’ (1) to ‘terminally Ill’ (9).
Able to mobilise without assistance (use of a mobility aid is acceptable).
Not currently participating in any research that could impact on the outcome of this study.
Recruitment
Sample size
Allowing for a 15% loss to follow-up and 5% mortality over the course of the intervention, this study aims to recruit a total of 24 participants. Each participant will provide control and intervention data, to achieve a power of 90% and a level of significance of 5% (two sided) for detecting a difference of 1 in the mean Fried Frailty criteria, between the intervention and control periods.
Identification
Convenience sampling of attendees to specialist clinics in the Geriatric Medicine department of a University hospital will be performed, where a Rockwood CFS score is routinely determined by a member of the MDT. Suitable candidates will be contacted no earlier than 24 hours later and, if agreeable, a detailed participant information leaflet will be sent by post to their address (online supplemental file 1). A subsequent follow-up phone call will be made no earlier than 48 hours later, to answer any outstanding queries. If agreeable to participation after this process, an appointment will be arranged for them to attend for initial assessment.
Supplemental material
Assessments
All assessments will be conducted in the Fitness Laboratory of the Waterford Institute of Technology Arena, a sports facility affiliated with a third-level education institution. Written informed consent will be obtained prior to commencement (online supplemental file 2).
Supplemental material
Primary outcome measure
The primary outcome measure will be the Fried frailty criteria,27 a cumulative score out of a maximum of five for the presence or absence of the following criteria: weight loss, self-reported exhaustion, reduced physical activity, weakness (reduced hand-grip strength) and slow gait speed. The values used to determine these criteria have been widely modified in the research setting,28 so the specific cut-offs to be used in this study are outlined in online supplemental file 3. A score of 3–5 is considered frail, 1–2 prefrail and 0 robust. This was chosen as it is the most widely cited assessment tool for phenotypic frailty29 and has been used to assess the effect of health interventions on frail older adults.30
Supplemental material
Secondary outcome measures
A range of secondary outcome measures related to frailty have been chosen (see table 3). Some are aimed at detecting physical and functional changes, such as assessment of body mass composition using bioelectrical impedance analysis and physical performance measures like the Timed ‘Up & Go’ test31 or the 30 s sit-to-stand test.32 Others provide a psychosocial perspective of the individual’s well-being, assessing cognition (Montreal Cognitive Assessment)33, mood (Geriatric Depression Scale-Short Form)34, pain (Pain Numerical Rating Scale)35 and quality of life (CASP-19 (Control, Autonomy, Self-realisation and Pleasure - 19 item) scale).36 Finally, a selection of biomarkers known to be associated with frailty has been chosen to examine the effect on underlying physiological processes related to the development or potentiation of frailty. Many of these are soluble biomarkers involved in inflammatory pathways (C reactive protein,37 interleukin-6 (IL-6),37 38 IL-8,38 IL-10,39 Tumour Necrosis Factor-alpha37 and interferon-gamma)40 but also include a measure of renal function (Cystatin C).41 For these analyses, non-fasting blood samples will be taken at each assessment visit. An additional clinical measure of arterial stiffness will be carried out, in the form of carotid-femoral pulse wave velocity.42
Secondary outcome measures
In order to monitor both adherence with the nutritional intervention and its effect on dietary intake, 3-day food diaries will be recorded by participants during the control and intervention periods. A dietitian will confirm accurate documentation of portion sizes, followed by analysis using the Nutritics.com online platform. This will allow assessment of the effect of the nutritional supplementation on the intake of a range of macronutrients and micronutrients.
Intervention
The main elements of the DEFRAIL intervention are outlined below in figures 3 and 4, and table 4. It is composed of an 8-week exercise programme (supervised multicomponent group exercise class) accompanied by a nutritional supplement (protein milk, 250 mL two times per day). A more detailed description of the intervention can be found in the Participant Logbook (online supplemental file 4). The 8-week duration was chosen as the optimal balance between efficacy, based on previous similar work (ranging from 643 to 12 weeks),13 and adherence in clinical practice, realistic for future replication outside of the research setting.
Supplemental material
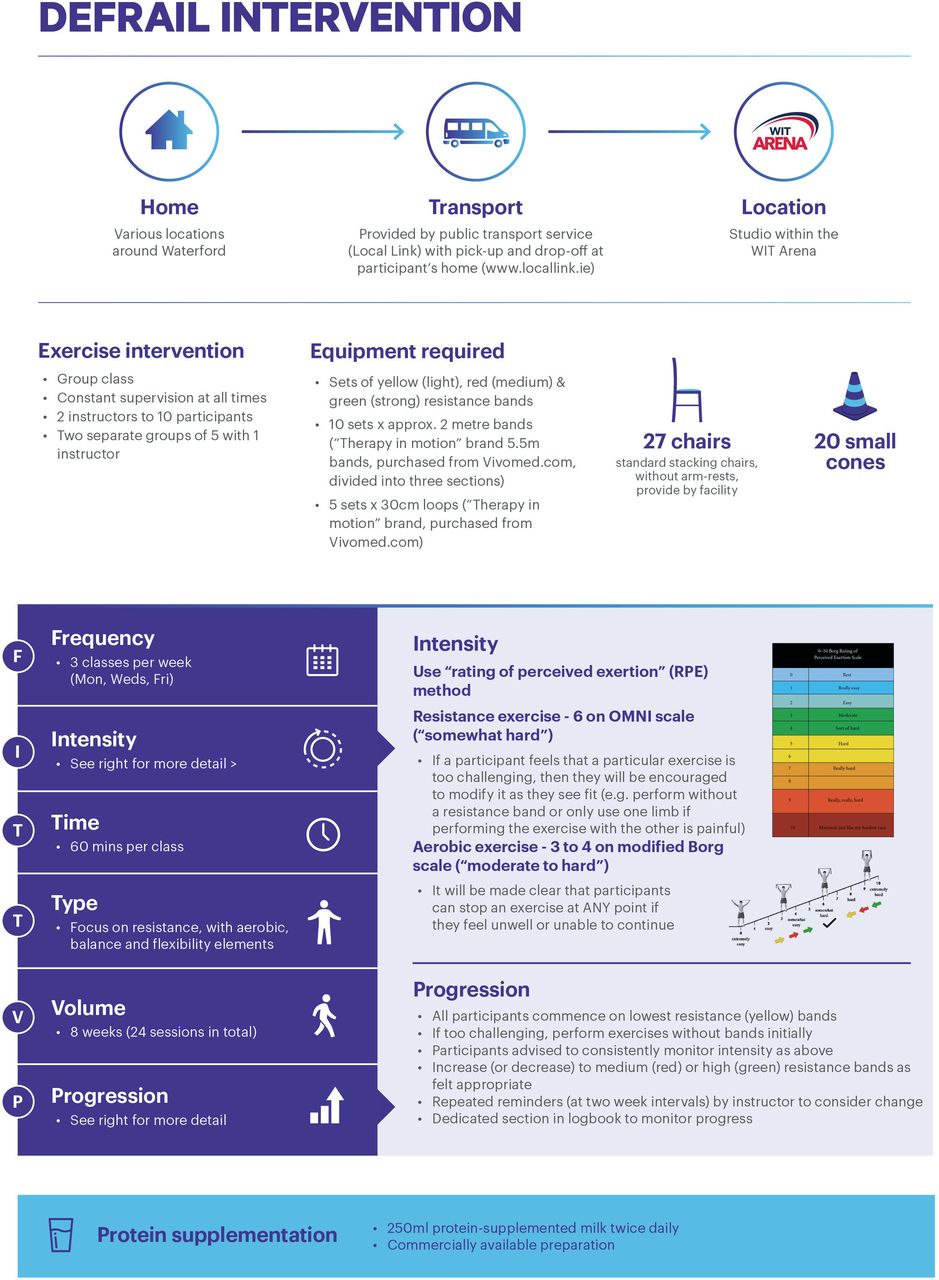
DEFRAIL intervention (1 of 2). DEFRAIL, Diet and Exercise for FRAILty; WIT, Waterford Institute of Technology.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
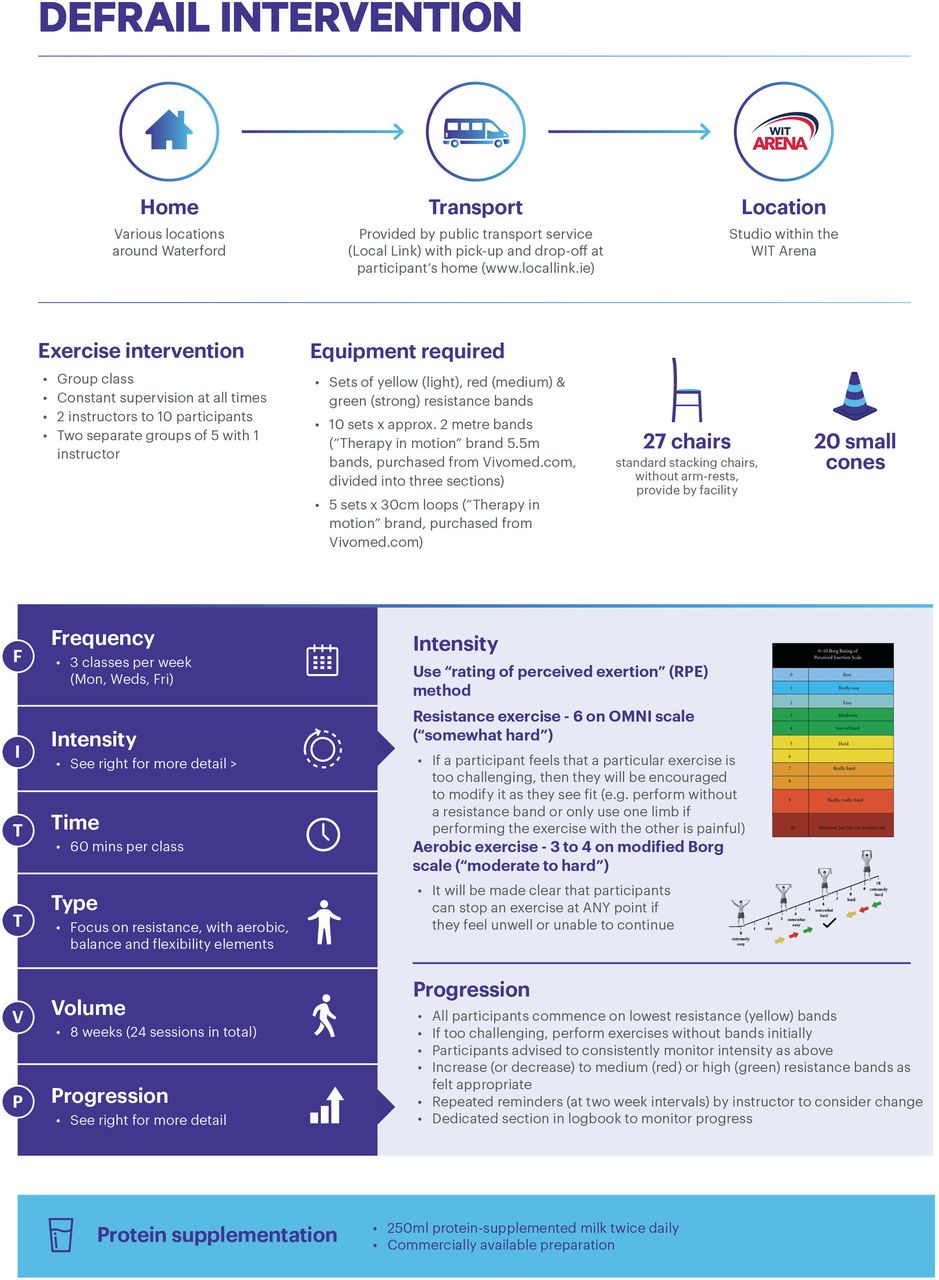
DEFRAIL intervention (2 of 2). DEFRAIL, Diet and Exercise for FRAILty.
Rotation of resistance exercises
Classes of 10–12 participants will be supervised by two instructors, who will provide demonstration of exercises, supervision of technique and observation for safety purposes. During the 4-week pilot, each instructor underwent training to ensure accurate replication of the intervention. Regular reference to the logbook will be encouraged, to ensure adherence to the protocol.
Patient and public involvement
The involvement of older adults, the cohort for whom the intervention has been developed, was central to this study. Most significantly, a 4-week pilot was undertaken with prefrail participants (n=7). This gave an opportunity for ineligible candidates who had attended for assessment to participate in a truncated programme, the goal of which was to allow meaningful PPI in the development of the final intervention. To achieve this, group discussions were undertaken with participants during and after each class. This provided invaluable feedback on the user experience, along with advice or suggestions for modifications. The input of family members, some of whom attended these sessions, gave additional perspectives. The informal nature of these conversations, conducted in the setting of the classes themselves, were felt to encourage frank and honest responses. To complement this, phone interviews using standardised questionnaires were also carried out with all pilot participants on completion, in order to provide more structured feedback. Topics discussed included tolerability of the intervention, perceived enablers and barriers to participation, and any other issues felt to be of importance to the individual. This feedback led to a number of changes to the final study design, including addition and removal of specific exercises, changes to the timing and structure of classes and arrangements regarding transport for participants. The plan for dissemination of results to participants is to provide a summary of clinically meaningful outcome measures on completion.
Results
Data management
Data collection and storage
All data will be collected in paper format using a standardised data collection form and stored in a locked filing cabinet in the office of the primary researcher. The identity and personal information of all participants will remain confidential. Each study participant will be assigned a unique identifier (DF001, DF002, etc), under which all information will be stored, and the masterfile matching these details to their ID number will be stored on an encrypted and password-protected computer.
Statistical analysis
Paired t-tests and Wilcoxon signed-rank tests will be used to compare the changes over the control and intervention periods, depending on parametric or non-parametric distribution of data, respectively. Statistical analysis will be performed using IBM SPSS V26.
Discussion
The development of complex health interventions is challenging and many fail to be translated into clinical practice.44 Our goal in designing the DEFRAIL intervention was to produce a programme of exercise and protein supplementation that could have the greatest impact on frailty in clinical practice. To achieve this, we felt our intervention should incorporate a number of characteristics: be suitable for a broad range of levels of frailty, in order to be inclusive; be appropriate for group classes in a community setting with limited specialist equipment, to allow community integration; be deliverable by non-medical professionals with minimal training, to remove the bottleneck presented by limitations in health service capacity; incorporate flexibility, balance and aerobic elements to maximise enjoyment and provide ancillary benefits; be structured to minimise falls risk, in order to allow a feasible instructor:participant ratio while remaining safe; and include an approach to nutritional supplementation that was palatable, affordable and widely available. In order to achieve these aims, a number of compromises were necessary, as discussed below.
We have adopted the ‘rating of perceived exertion’45 approach to the setting of exercise intensity and progression, through the use of the OMNI scale,46 for resistance, exercises and the Borg CR10 (category-ratio 10) scale47 for aerobic exercises. This prioritises participation over rigid prescription, with subsequent individualised progression based on a participant’s subjective impression of the difficulty of exercises. In this way, classes following the DEFRAIL protocol are suitable for a broad range of older adults with varying degrees of frailty to participate side by side, in a manner representative of the general older population. We feel this is more appropriate than the use of a “percentage of one-repetition maximum” (%1RM) approach, that is, the maximum load under which an individual can complete one repetition of a particular exercise. Although still advocated by many for use in older adults, due to concerns that underdosing of exercise prescriptions may occur,48 49 in addition to presenting safety concerns, it also represents a barrier to engaging older, particularly frail, adults in strength training. This is because it requires the input of a trained professional at the outset and ongoing supervision over the course of the programme.
The method of nutritional supplementation (protein-supplemented milk) was also chosen in an attempt to achieve the optimal balance between efficacy and adherence. It is a preparation that it suited to adoption in clinical practice due to its widespread availability, low cost (compared with oral nutritional supplements), familiarity and palatability.
Another major challenge when translating the evidence base into practice is the lack of detail provided by authors when describing their interventions, such that accurate replication is difficult.50 To address this, we have provided a clear and comprehensive record of the DEFRAIL intervention in the form of a logbook for instructors and participants (online supplemental file 4). In addition, we have included an itemised breakdown in the form of a ‘Template for Intervention Description and Replication’ (TIDieR) checklist, which has been shown to improve implementation fidelity in complex community-based interventions.51
Due to its widespread use and ease of administration, the Rockwood CFS52 was used as the frailty screening tool in the inclusion criteria, while the Fried frailty criteria,27 a more analytical and objective assessment tool, was used as the primary outcome measure. As discussed, the Fried criteria is the most widely cited measure of phenotypic frailty29 so has a central place in the discussion around frailty. However, it has a number of recognised limitations for use in this setting, including the heterogeneity of its application due to various modifications.53 For this reason, a range of frailty-related secondary outcome measures will also be assessed, as listed above.
The lack of longer-term follow-up of participants is recognised as a limitation of this study but the need to do so in future work is acknowledged, with planned maintenance strategies in place.
Finally, a number of other limitations relate to the study design. These include the lack of randomisation, the single-site nature of this study, and the unblinded nature of the assessments. Additionally, the lack of comparative arms mean that it will not be possible to separate the effects of the various elements of this combined intervention. The resources available to the project and the accessible local frail population did not allow for a fully randomised, multiarm, multisite, blinded study. Following completion of this study, if it is proven to be effective, we would hope to undertake a larger multisite study with blinded assessments. This would involve randomisation of participants into multiple arms, in order to examine the relative contributions of its constituent parts. These include the exercise programme, the nutritional supplementation and the effect of social interaction as part of a community-based group activity.
Ethics and dissemination
This study received ethical approval from the Research Ethics committees of both the Health Service Executive South-Eastern Area and Waterford Institute of Technology. Its findings will be disseminated through various means, including journal publications, conference presentations and other forms of public engagement.
Reporting of adverse events
Given the pragmatic nature of the trial and the overarching aim of providing a reproducible intervention, medical oversight will not be provided for the intervention, despite the involvement of physicians in the design and conduct of the study. Instead, all adverse events are to be dealt with initially by the staff of the facility where the classes take place, with further medical review to be arranged as appropriate, via standard community or emergency medical services. However, all adverse events will be reported to the primary researcher and a detailed review of the circumstances will be conducted as necessary.
Status
This trial commenced on 13 May 2019 and is expected to be complete by December 2020.
Ethics statements
Acknowledgments
The members of the expert consensus panel were Prof. John Cooke, Prof. Ríona Mulcahy, Dr. George Pope (Geriatric Medicine), Dr. Michael Harrison (Sports & Exercise Science), Dr Noel McCaffrey General Practice, Sports Medicine), Maggie Bolger (Geriatric Nursing), Niamh Phelan (Physiotherapy), Emma Grant (Nutrition & Dietetics) and the coordinator was Dr. Pádraig Bambrick (Geriatric Medicine). Valuable advice on the approach to nutritional supplementation was provided by Dr. Linda Giblin and Dr. André Brodkorb of the Moorepark Teagasc Food Research Centre, Fermoy, Co. Cork. Statistical support was provided by Dr Fiona Boland of the Data Science Centre at RCSI. The classes will be delivered by four personal trainers, in rotation (two per class) (Anna Hawrylak, Barry O’Connor, Michelle Mullaly and Anna Flynn). We would like to acknowledge the advisory role of the participants of our pilot trial, all of whom provided constructive feedback on their experiences. This contributed significantly to the final design of the intervention and study. We would like to thank Michelle Collins and Kate Lennon at Glanbia Ireland for their financial and logistical support. This project is being carried out under the Strategic Academic Recruitment MD (StAR MD) programme of RCSI.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @pbambrick
Contributors The initial exercise intervention was designed by PB and NP, with revision by an expert consensus group. The assessment protocol was designed and trialled by PB and TB, as part of ongoing collaborative work. Food diary records will be assessed and analysed by EG. This manuscript was written by PB, with supervision, input and feedback at all stages by JC, RM and MH. All authors have read and approved the final manuscript.
Funding This work was supported by the Royal College of Surgeons in Ireland (RCSI) and Glanbia Ireland DAC.
Competing interests The protein-supplemented milk used in this study is a commercial product of one of the main funders, Glanbia Ireland DAC (Avonmore Protein milk).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.