Article Text

Abstract
Introduction Daily multidisciplinary rounds (DMRs) consist of systematic patient-centred discussions aiming to establish joint therapeutic goals for the next 24 hours of intensive care unit (ICU) care. The aim of the present study protocol is to evaluate whether an intervention consisting of guided DMRs, supported by a remote specialist and audit/feedback on care performance will reduce ICU length of stay compared with a control group.
Methods and analysis A multicentre, controlled, cluster-randomised superiority trial including 30 ICUs in Brazil (15 intervention and 15 control), from August 2019 to June 2021. In a parallel assignment, ICUs are randomised to a complex-intervention composed by daily rounds carried out through Tele-ICU by a remote ICU physician; development of local quality indicators dashboards coupled with monthly meetings with local leadership; and dissemination of evidence-based clinical protocols versus usual care. Primary outcome is ICU length of stay. Secondary outcomes include classification of the unit according to the profiles defined by the standardised resource use and the standardised mortality rate, hospital mortality, incidence of healthcare-associated infections, ventilator-free days at 28 days, patient-days receiving oral or enteral feeding, patient-days under light sedation or alert and calm, rate of patients under normoxaemia. All adult patients admitted after the beginning of the study in each participant ICU will be enrolled. Inclusion criteria (clusters): public Brazilian ICUs with a minimum of 8 ICU beds interested/committed to participating in the study. Exclusion criteria (clusters): units with fully established DMRs by an intensivist, specialised or step-down units.
Ethics and dissemination The study protocol was approved by the institutional review board (IRB) of the coordinator centre, and by IRBs of each enrolled hospital/ICU. Statistical analysis protocol is being prepared for submission before the end of patient’s enrolment. Results will be disseminated through conferences, peer-reviewed journals and to each participating unit.
Trial registration number NCT03920501; Pre-results.
- telemedicine
- quality in health care
- intensive & critical care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) is the first, large, multicentre cluster-randomised trial performed in a middle-income country evaluating if a complex-intervention delivered mainly by TELE-intensive care unit (ICU) physician and aiming to optimise the care of critically ill patients impacts clinical outcomes.
TELESCOPE trained general board-certified ICU physicians to deliver TELE-ICU consultancy and provide performance feedback to the attending team and managers.
TELESCOPE used a baseline period as reference for randomisation, by using a minimisation algorithm in order to achieve balance between arms and decrease within cluster variability.
TELESCOPE intervention occurs only inside the ICU and an expected limitation is that length-of-stay depends on factors outside the ICU, such as ward bed availability.
Introduction
Healthcare demand for critically ill patients admitted to intensive care units (ICUs) has been expanding worldwide, causing great social impact.1–3 Several factors have contributed to it, such as population ageing,4 a higher prevalence of chronic diseases, among others.3 5 Brazil is especially sensitive to this issue as it experiences great regional disparities and population ageing without adequate control of the main health determinants.6–9 Such situation has resulted in a large number of frail elderly, who often require critical care due to acute aggravations in chronic conditions.10–12 This scenario combined with the risk of spending a significant amount of money with suboptimal return for the society, justifies seeking efficient care for severely ill patients.13
Daily multidisciplinary round (DMR) is an approach that optimises the ICU care.14–16 DMRs consists of systematic patient-centred discussions aiming to establish joint therapeutic goals for the next 24 hours of ICU care.14 In different studies, DMR has been associated to better clinical outcomes.15 16 However, full implementation of DMR is still challenging, since DMR must contain several attributes in order to maximise its results: its multidisciplinary character; proper settings; time and team standardisations; definition of roles; use of guiding tools; reduction of interruptions and focus on documented objectives.14
Telecommunication use for healthcare practice, the prototype for what telemedicine has become, has been described since the advent of telecommunication.17 The availability of high-speed data traffic has expanded the boundaries of Telemedicine, allowing the emergence of the first trial with critically ill patients in 1977.18 In recent years, the use of Telemedicine in critically ill patients, known as tele-ICU, has gained relevance.19 Specifically in the USA, the number of ICU beds with some form of Telemedicine coverage has reached at least 15%.20 21 There is a variety of possible tele-ICU applications, such as second opinion consultations in specific cases, monitoring of vital signs, real-time performance and DMR conducted by a remotely located medical specialist.22 23 However, the benefit of tele-ICU lacks high quality scientific evidence, particularly outside high-income countries.24 25 Furthermore, most of the studies published so far address Telemedicine in ICUs using vital signs monitoring and a continuous response system in a costly way.26 Thus, little is known about the use of Telemedicine focused primarily on supporting DMR, which is understood to be both effective and more feasible from the economic perspective.
Methods and analysis
Aim and objectives
The TELE-critical Care verSus usual Care On ICU PErformance (TELESCOPE) trial aims to answer to the following research question: Does a complex intervention offered by tele-ICU, focused on DMR attended by remote intensivists, improve ICU efficiency of adult general units in Brazil?
Primary goal
To evaluate whether an intervention consisting of guided DMRs, supported by a remote specialist (intensivist) through Telemedicine and audit/feedback on care performance will reduce ICU length of stay (LOS) compared with a control group.
Secondary goals
To evaluate whether an intervention consisting of guided DMRs, supported by a remote specialist (intensivist) through Telemedicine and audit/feedback on care performance improves indicators of ICU performance compared with a control group.
Study design and setting
The TELESCOPE trial is a national, multicentre, controlled, open-label, cluster-randomised trial. The study tests the effectiveness of DMRs conducted by an intensivist through Telemedicine in Brazilian ICUs. Approximately 15 000 patients are expected to be recruited for a period of 18 months in 30 Brazilian ICUs (figure 1). The main characteristics of the TELESCOPE trial, according to WHO standards, are summarised in the Synopsis table (table 1). The three versions of the protocol are listed in the project control version table (table 2).

Geographical distribution of the 30 intensive care units in Brazil participating in the TELE-critical Care verSus usual Care On ICU PErformance trial.
Synopsis (WHO trial registration data set, as originally submitted)
Project version control
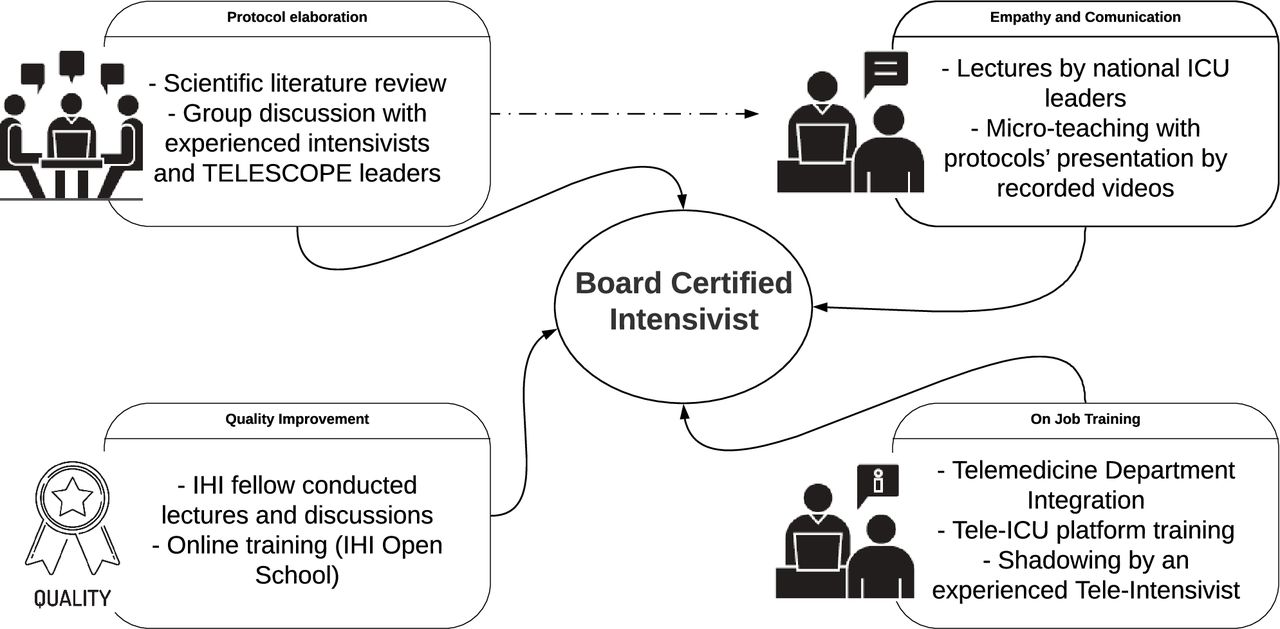
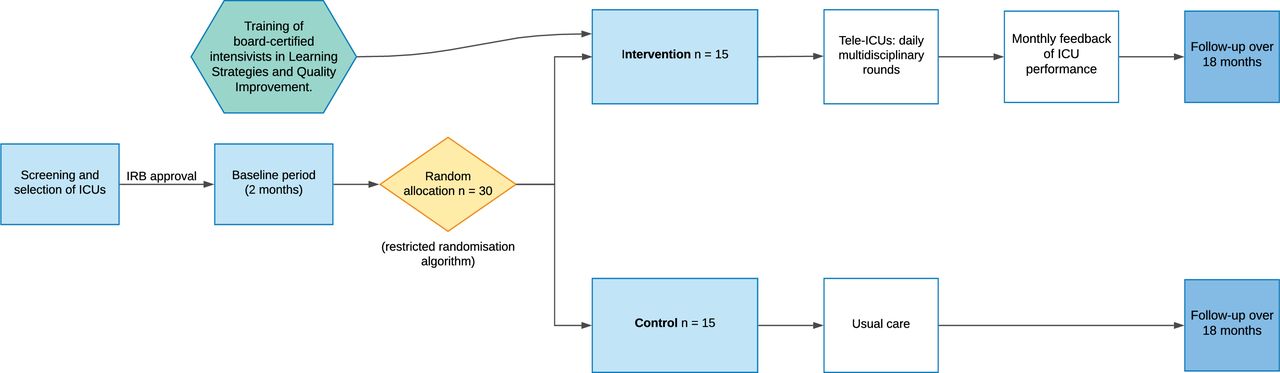
After a 2-month observation period (baseline period) in which performance indicators for eligible ICUs is collected without any intervention (with the purpose of obtaining data for randomisation and characterisation of the initial ICU status), the ICUs eligible for the study are randomised to either receive DMRs conducted by an intensivist through Telemedicine, from Monday to Friday, in addition to a monthly discussion of care performance indicators performed through virtual meetings (Intervention Group), or receive the unit’s usual care (Control Group) (figure 2). ICU board certified physicians receives a multicomponent training before starting the tele-ICU DMR, comprising empathy and communication and quality improvement (figure 3). The study protocol was registered in the ClinicalTrials.gov (NCT03920501). The study protocol follows the recommendations of the Standard Protocol Items: Recommendations for Interventional Trials 2013 Statement (online supplemental file 1).27
Supplemental material

Trial timeline, randomisation, intervention and follow-up. ICU, intensive care unit; IRB, institutional review board.
{kind=link}
{kind=link}
{kind=link}
Illustration of the multicomponent training of board-certified intensivists to act in the intervention arm. ICU, intensive care unit; IHI, institute for healthcare improvement.
Intervention
Intervention group (TELE-ICU)
Trial intervention consists of:
DMR led by remote intensivists—Discussions are conducted by an intensivist located in a remote centre (tele-intensivist) and the local multidisciplinary team (doctor, nurse and physiotherapist). DMRs takes place from Monday to Friday, in predetermined hours (mostly during the mornings), using Telemedicine equipment and approach every patient admitted to the participating ICUs. The main objective of DMR conducted by a tele-intensivist is to discuss diagnostic hypotheses, active problems and create a treatment plan until the next DMR. Tele-intensivists make recommendations based on updated scientific evidence, suitable to the local context. Clinical protocols in texts and videos formats (developed and used during the tele-intensivists training period) were made available to physicians and multidisciplinary team of the ICUs in the intervention arm, right after randomisation and establishment of a DMR routine. Electronic forms for patient follow-up serves as a guideline (Index) and are filled out by tele-intensivists. According to the current regulation (national resolution from the Brazilian Federal Council of Medicine - CFM, CFM Resolution 1643 of 2002), tele-intensivists does not act directly on patients, but are rather mediated by the local team. Therefore, the local healthcare practitioners implement the treatment plan. Indicators of adherence to recommendations made by tele-intensivists are registered. Tele-intensivists do not write medical prescriptions, nor gives direct orders to the local care team for procedures or interventions. DMRs may be postponed, interrupted or suspended in case of urgency/medical emergency situations that may hinder participation of local doctors (table 3).
Management of ICU performance—The variables collected for the trial (table 1) are presented aggregately in reports available for each coordinator of the participating ICUs as well as for tele-intensivists. Data from case report forms (CRFs) (REDCap, Vanderbilt University Medical Center, Tennessee, USA) are used to automatically feed dashboards in real-time, specially developed for this purpose (R Studio/Shiny, Boston, Massachusetts, USA). In addition, monthly remote meetings between the local ICU team and the respective tele-intensivist are organised to discuss these indicators and to establish possible improvement action plans.
Intervention framework
Control group (usual care)
No interventions are delivered to the ICUs randomised to the control group, except for the systematic data collection required for the comparisons described in the trial objectives. However, unlike in the ICUs of the intervention group, these data are not available for the care team nor to the coordination of the participating ICUs.
Sites
The list of potential units was retrieved from the national registry of health facilities (‘Cadastro Nacional de Estabelecimentos de Saúde’, in Portuguese), filtering those facilities with at least 8 ICU adult beds available.
Inclusion/exclusion
The ICUs are invited by electronic means for an interview in which the eligibility and feasibility criteria below will be verified.
Inclusion criteria for ICUs
ICUs of public or philanthropic hospitals.
ICUs with a minimum of eight ICU beds.
ICUs with on-site registered doctors and nurses.
Exclusion criteria for ICUs
ICUs that already presented DMRs, defined as:
Meetings (DMRs) ≥3 times per week, during weekdays, conducted by a certified intensivist and documented in medical records with fixed visit length (>5 min/patient), using some supporting tool (checklist or standard form), goal oriented, based on established protocols, including all the patients admitted to the ICU.
or
Monthly management of indicators (audit and feedback) with specific planning.
Specialised ICUs (ICUs admitting exclusively cardiac surgery, neurological, burned patients).
Step-down units or coronary units.
Patients
All consecutive patients that fulfil the inclusion criteria and none of the exclusion criteria will be enrolled.
Inclusion/exclusion
The patients admitted in the ICU who currently meet the following inclusion criteria are included:
Age≥18 years old.
Patients admitted to the ICU after the beginning of the trial.
Exclusion criteria for patients
Patients admitted to the ICU due to justice-related issues (since in such circumstances the ICU admission or discharge may be determined by law and not medical reasons).
Patients previously included in the TELESCOPE trial (for the analysis of the primary outcome).
Randomisation
The 30 ICUs are randomly assigned to either the intervention group (n=15) or the control group (n=15) using a restricted randomisation algorithm that minimises imbalance between treatment groups across the following baseline covariates at the ICU level: number of ICU beds, mean Simplified Acute Physiology (SAPS 3), mean ICU LOS, the standardised mortality rate (SMR), the standardised resource use (SRU) and a dummy indicator for Brazilian region where the ICU is located (South/Southeast x North/Northeast/Central-West).28 29 The randomisation unit will be the ICU to avoid contamination of the intervention. Only one ICU per hospital will be included in the trial. The randomisation is performed at three times, including 14 units during the first randomisation, followed by seven and nine units. We decided a priori to randomise at three times and the number of units at each randomisation was pragmatic, allowing for ethical approval and completion of the baseline period, respecting the minimum of eight units during first randomisation and minimum of six on subsequent randomisations.28 To ensure allocation concealment, the statistician responsible for the randomisation list receives only the ICU identifier code, being unaware of which unit it refers to. The allocation list is sent to the study coordinator, who informs the ICUs about the randomisation. The allocation will be maintained until the end of the study.
Blinding
The intervention is open, due to the nature of the study (Tele-ICU rounds, quality improvement meetings and delivery of evidence-based clinical protocols). The steering and scientific committees are blinded of the DMRs and monthly feedback/audit meetings.
Follow-up
Patients are followed up until hospital discharge by the healthcare worker responsible for data collection.
Outcomes
Primary outcome
At an individual level, the primary outcome of this trial is ICU LOS, measured in days, taking into account the time interval in hours between patients’ ICU admission and time of transfer to another care facility or another hospital or ICU death, as defined by the hospital’s system date and time. Date and time will be entered by the healthcare worker responsible for data collection.
Secondary exploratory outcomes
The secondary outcomes of this study include assessing the impact of interventions implemented through Telemedicine compared with a control group in the following outcomes:
Classification of the unit according to the profiles defined by the SRU and the SMR.30 The SRU reflects the observed/expected rate of resources used (estimated as ICU LOS for surviving patients), adjusted by patient’s severity of illness.31 32 The SMR reflects the observed / expected rate (according to severity score) of hospital deaths. The profiles are a combination of SMR (above or below median) and SRU (above or below median): Each unit can be assigned to one of four groups: ‘most efficient’ (SMR and SRU <median); ‘least efficient’ (SMR, SRU >median); ‘overachieving’ (low SMR, high SRU), ‘underachieving’ (high SMR, low SRU).31
In-hospital mortality, defined as death by any cause from date of ICU admission until the date of hospital discharge or death, whichever comes first.
Incidence of central line-associated bloodstream infection (CLABSI), as defined by the Centers for Disease Control and Prevention (CDC).33
Incidence of ventilator-associated event (VAE), as defined by the CDC.34
Incidence of catheter-associated urinary tract infection (CAUTI), as defined by the CDC.35
Ventilator-free days at 28 days, defined as the number of days from successfully weaning to day 28; patients who died before weaning were deemed to have no ventilator-free days.
Patient-days receiving oral or enteral feeding, defined as any amount oral or enteral diet.
Patient-days under light sedation or alert and calm (Richmond Agitation-Sedation Scale (RASS) = −3 to +1).
Rate of patients under normoxaemia (peripheral oxygen saturation (SpO2) between 92% and 96%).
Other exploratory outcomes
Other outcomes, considered merely exploratory, will be observed:
ICU mortality.
A 24-hour ICU readmission rate.
Proportion of mechanical ventilation (MV) use.
Early reintubation rate (<48 hours after extubation).
Accidental extubation rate.
Compliance to head of bed elevation for patient under MV.
Rate of central venous catheter (CVC) use and duration.
Rate of urinary catheter use and duration.
Adequate prevention of venous thromboembolism (VTE).
Rate of patients with adequate glycaemic control.
We will truncate the primary and secondary outcomes follow-up at 90 days.
Data collection
At the patient level, the following data is collected (table 4).
At the time of ICU admission
Patient data collection schedule
Identifier, date of birth, sex, main reason of ICU admission (adapted from Acute Physiology and Chronic Health disease Classification System-APACHE III),36 readmission status
Anthropometric characteristics, comorbidities (adapted from SAPS3),37 functional status (adapted from The Eastern Cooperative Oncology Group - ECOG).37
Respiratory, cardiovascular and renal support.
Diet and sedation status.
Presence of devices: CVC, arterial line, permanent catheters, urinary catheter, oro/nasotracheal catheter and traqueostomy.
Date and time of hospital admission.
Date and time of ICU admission.
SAPS 3 score.32
Sequential organ failure assessment score.38 39
Throughout the ICU admission
Documented goals from the DMR.
Documented discharge order status, defined as any mention to readiness to discharge or ICU transference order.
MV status and MV parameters.
SpO2 range for patients on oxygen therapy.
Head of bed elevation for patients under MV.
Spontaneous respiratory test, accidental extubation or reintubation events.
Need of vasoactive drugs and renal replacement therapy.
Continuous sedative infusion and light sedation strategy (reduction/daily interruption).
Daily value (categorised below, above or within −3 to +1 range) of the RASSfor patients undergoing continuous sedation at a predetermined time.
Adequacy of VTE prophylaxis: considered adequate when patient is bedridden without any of the following exclusion criteria: active bleeding, stress gastric ulcer, uncontrolled arterial hypertension (>180/110 mm Hg), coagulation disorder, allergy, kidney failure (Cl <30 mL/min), ocular or cranial surgery in last 2 weeks, and lumbar puncture in last 24 hours).
Presence of oral or enteral nutrition.
Glycaemic control: considered adequate if between 60 and 180 mg/dL.
Notification of healthcare-related infection episodes according to CDC criteria:
Date and time of withdrawal of CVC for patients undergoing CVC insertion.
Date and time of indwelling urinary catheter (IUC) insertion for patients submitted to IUC insertion.
Date and time of withdrawal of IUC for patients undergoing IUC insertion.
Documentation of decisions for limiting the life support considering any mention to withholding or withdrawing in the medical records.
At the time of ICU discharge
Date and time of ICU discharge.
ICU outcome: discharge to ward, hospital transfer, death.
At the time of hospital discharge
Date and time of hospital discharge.
Hospital outcome: hospital transfer, death.
Data collection and management
Trained healthcare workers collect data, without any involvement from the study committees and investigators. We developed a standard CRFs for the trial, with extensive validation and piloting aiming clarity and consistency.
Data are input using electronic CRFs in the Research Electronic Data Capture system - REDCap (REDCap, USA) via internet and hosted on a server at the Hospital Israelita Albert Einstein/São Paulo-Brazil. Medical data from tele-intensivist consultations is generated and stored using a specific platform developed by the Tele-ICU Department of the Hospital Israelita Albert Einstein/São Paulo-Brazil. Images and audio are never saved or stored. The electronic files are stored in the hospital’s servers in a controlled and secure environment to guarantee confidentiality. Furthermore, access to all documents is user and password controlled. To ensure data quality, the following procedures are performed:
All professionals responsible for data collection are trained before the beginning of the trial in order to guarantee clear definitions for accurate data collection.
A research nurse from the Coordinating Centre is available 24/7 to solve any problem and question about data collection.
Data input in the system are submitted to near real-time verifications to detect missing data, values outside expected and logic patterns.
Remote data monitoring is performed regularly to detect patterns of anomalies, consistency or credibility problems and other anomalies—according to pre-established queries created by the system. Any missing data or outlier is individually reviewed for inspection.
The coordinating centre reviews follow-up reports regularly to ensure their consistency and completeness.
Centre monitoring is performed while the study is being conducted. A trained professional is assigned by the coordinating centre to monitor the study participating centres. All the information obtained during the monitoring visits are strictly confidential.
Monitoring
Interim analyses
Since our intervention gathers the best available evidence for care of critically ill patients admitted to the ICUs, and we do not predict inherent risks in the performance of the trial, interim analyses are not planned. Therefore, a formal data monitoring committee was deemed unneeded. Adverse events are not expected to occur but could be reported by local researchers, data assistants and local doctors.
Intervention monitoring
Considering the study aim is to evaluate the impact of a complex intervention (composed by DMR, management of ICU performance indicators, and provision of clinical protocols), specific data (implementation indicators) will be collected and followed in order to ensure adherence to the protocol:
DMR rate per site/bed/day, and DMR duration (including individual and periodic feedback to each tele-intensivist).
Rate of recommendations made, and validated (accepted and not accepted)/DMR.
Monthly meeting on performance indicators reports: tele-intensivists will send to study team monthly reports including the executive summary (file sent to the leaderships of each study centre/intervention arm, before the monthly meeting) and the meeting record file (structured data about highlighted indicators, action plan, responsibility and due dates).
Access to the clinical protocols: absolute number of accesses to the video-protocols will be provided and followed.
Auditing
Trial conduct is subjected to audit by Einstein Research Integrity Committee, at any time, independently of the IRB and research team, the same way as any interventional studies performed at Albert Einstein Hospital (random selection).
Power/sample size calculation
We estimated a mean ICU length-of-stay of 8 (SD 10) days for general adult public ICUs in Brazil. We used data from published literature and reports from the online project ‘UTIs Brasileiras’.40 Using data from 20 ICUs (10 ICUs from Ranzani et al,41 10 ICUs from the ORganizational CHaractEriSTics in cRitical cAre-ORCHESTRA study,42 available in the ems R package), we estimated an intraclass correlation coefficient of 0.018. Considering a two-arm cluster trial with an ICC of 0.018, for a minimum difference of an average LOS of 1.5 days (8.0–6.5 days) and SD of 10 days, power 80%, alpha 5%, we would need a total of 30 clusters (15 intervention units and 15 control units) with an average cluster size of 500 patients per ICU over a period of 18 months. If we use a coefficient of variation of cluster size, estimated by the expected minimum and maximum method, we will maintain 80% power if the difference between the clusters minimum and maximum size is 150 patients. If needed, after the baseline period, we might review the sample calculation and simulate the power for secondary outcomes, using the data from the selected ICUs.
Analysis
All analyses will be thoroughly described in a statistical analysis plan (SAP), which will be concluded and submitted for publishing prior to database closure and the beginning of analyses. Primary statistical analyses will be performed according to the intention-to-treat principle. All outcomes at the patient-level will be performed using models that account for correlated data within each ICU (ie, ICU as a cluster) with generalised linear mixed models and adjusted by pre-specified covariates, as will be specified in the SAP. Prespecified secondary outcomes and subgroup analyses will not be adjusted for multiple comparisons. They should, therefore, be interpreted as exploratory. We prespecified three subgroups: type of admission (medical vs surgical), by tertiles of SAPS3 and MV status (invasive MV vs not-invasive MV). Subgroups will be analysed as an interaction term.
We will evaluate the calibration of the SAPS3 model with data from the baseline period. If necessary, we will recalibrate the model for the studied population. We plan to perform multiple imputation if missing data on core variables will be >5% and we will use standard steps for multiple imputation using chained equations. All analyses will be performed with programme R (V.3.4.1, the version will be updated at the time of analysis).
Ethics and dissemination
The project was approved by local Research Ethics Committee (institutional review board, IRB) of the coordinating study centre (Hospital Israelita Albert Einstein) (CAAE: 01523118.0.1001.0071) and by the local IRB from each one of the 30 ICUs (online supplemental file 2), following the Brazilian legislation. A specialist in regulatory process will oversee and support the local process. Any modifications in the protocol that might affect the development of the study and its potential benefits or safety, including changes in the objectives, design, study population, sample size, interventions or relevant management aspects, will require amendments to the protocol. Such amendments should be submitted to the IRB of the coordinating centre and all the IRBs at the participating centre for proper approval. There will be rigorous procedures of protocol version control.
Supplemental material
The need for patients’ written informed consent was waived in all 30 centres. For one centre, it was requested written informed consent for healthcare professionals involved in the tele-ICU visits. We obtained written agreement from the Director of each institution as well as by the ICU coordinator.43–46
Therefore, the set interventions are not specifically directed to the patients but to the whole cluster together: the ICU (intervention type A).47 In this type of interventions, there is only one decision to be made for each cluster and individual choice are not appropriated.47 In this sense, informed consent was proposed and signed in the cluster level. In the best interest of patients, medical teams and other professionals, the hospital director and the head of ICU (physician) were the responsible to sign the consent form. This proposal was approved by all the involved IRBs (coordinating centre and the IRBs of each one of the 30 participant hospitals).
All the information in the study will be stored (in paper and/or magnetic media) at the coordinating centre. All patient-level data will be anonymised, and will be accessed only by the data manager and statistician. Access to information from the participants (during the visits) will be restricted to the intensivists performing daily rounds via Telemedicine. All records with names or other identifiers will be stored separately from the study records. Information on patients will not be disclosed except for regulatory purposes.
The TELESCOPE study Steering Committee commits to publishing the study results, whatever they may be. The results of this study will be mainly disseminated through international scientific publication. The main result of this project will be reported in an article and substudies are planned. Results of this project are expected to be presented in major sessions at national and international congresses, especially in the field of intensive care medicine. Study results are expected to be promoted to the lay press and disseminated in various media outlets due to its impact on the health system.
Trial status
This paper presents the protocol for the TELESCOPE trial (original V.1.0, approved in 11 July 2018). The baseline period started on 01 June 2019. First randomisation and interventions started in 06 August 2019. At the time of first version of the manuscript submission, data collection for the trial was ongoing and due to be complete in the first semester of 2021.
Ethics statements
Ethics approval
This study will be conducted according to the resolution no 466/12 of the Brazilian National Health Council (http://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html). The study protocol has been approved by the Research Ethics Committee of the coordinating site (approval number: CAAE 01523118.0.1001.0071) and the Research Ethics Committees of all participant institutions (online supplemental file 2).
Acknowledgments
The authors would like to thank the central TELESCOPE team, data collection team of each participating ICU, as well as the Hospital Israelita Albert Einstein, the Brazilian Ministry of Health, and the Brazilian Research in Intensive Care Network (BRICNET) for their support in conducting the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rodrigobiondi
DTN and OTR contributed equally.
Collaborators Coordinating Center: Hospital Israelita Albert Einstein (HIAE), Executive Committee (Design and execution of the study, protocol preparation and revisions, preparation of the investigator’s brochure (IB) and case reform forms (CRF), organization of the meetings of the committee of representatives of the ICUs participating in the study, oversight of the clinical trials office (ARO) management activities, publishing of study reports): - Adriano José Pereira – intensivist. Intensive Care Unit, Hospital Israelita Albert Einstein - Principal Investigator/Study Chair. - Danilo Teixeira Noritomi - intensivist. Hospital Israelita Albert Einstein, São Paulo, SP. Senior Investigator. - Otavio Tavares Ranzani – intensivist and epidemiologist. - Maura Santos - Senior Nurse Steering Committee: - Adriano José Pereira – intensivist. Intensive Care Unit, Hospital Israelita Albert Einstein - Principal Investigator/Study Chair.
- Alexandre Biasi Cavalcanti – intensivist. Research Institute HCor, São Paulo, SP. Member of BRICNet – Brazilian Research in Intensive Care Network. - Ary Serpa Neto – intensivist. Hospital Alemão Oswaldo Cruz, São Paulo, SP. Member of BRICNet – Brazilian Research in Intensive Care Network - Danilo Teixeira Noritomi - intensivist. Hospital Israelita Albert Einstein, São Paulo, SP. Senior Investigator. - Eduardo Cordioli. Health Care Manager of the Department of Telemedicine of the Hospital Israelita Albert Einstein, São Paulo, SP - Fernando Gatti. Coordinator of the Hospital Infection Control Service of the Hospital Israelita Albert Einstein, São Paulo, SP 10. - Jorge Salluh. Intensivist. Professor in the UFRJ Graduate Program, Researcher of the Intensive Care Department, IDOR- Rio de Janeiro - Leonardo José Rolin Ferraz – intensivist. Intensive Care Unit, Hospital Israelita Albert Einstein - Lúbia Caus. Intensivist. Intensive Care Unit, Hospital Israelita Albert Einstein. - Luciano Azevedo – intensivist. Hospital Sírio-Libanês & Hospital São Paulo, UNIFESP, São Paulo, SP. Member of BRICNet – Brazilian Research in Intensive Care Network - Maura Cristina Santos. Senior nurse of the Department of Severely ill Patients, tele – ICU. Study Manager - Otávio Berwanger – epidemiologist. Hospital Israelita Albert Einstein, São Paulo, SP - Otavio Tavares Ranzani – intensivist and epidemiologist - Regis Goulart Rosa – intensivist. Adult Intensive Care Unit of the Hospital Moinhos de Vento, Porto Alegre, RS - Renata Albaladejo. Nurse specialist in Telemedicine - Rodrigo Biondi – intensive care physician- Thiago Domingos Correa – intensivist. Hospital Israelita Albert Einstein, São Paulo, SP. Member of BRICNet – Brazilian Research in Intensive Care Network Project Office: Composed by Main Researcher, Senior Researcher and Study Manager, Responsible for the trial planning, Responsible for organizing meetings with the representative committee of the ICUs participating in the trial, Responsible for producing semiannual progress reports for the Ministry of Health and the Ethics Committee, Responsible for the trial master file, Responsible for managing the trial financial resources (in partnership with the PROADI institutional office) and contractual issues with third parties and individual centers, Responsible for making recommendations for local investigators, Responsible for semi-annual monitoring (in partnership with ARO), providing feedbacks and decisions on visits to the centers, Responsible for data checking, Responsible for randomization. Representative Committee of ICUs participating in the trial: Ensure implementation of interventions at the center, Ensure data collection quality, Monitor trial and, if necessary, approve protocol changes or amendments/IB, ensuring the trial is conducted as efficiently as possible. Local Investigators: A local investigator will be appointed in each center (ICU coordinator or senior doctor at the ICU). He will oversee hired data collectors. In intervention on the ICUs, they will be responsible for ensuring the implementation of intervention proposed by a remote intensivist (Telemedicine), data collection / feeding, filling in the CRF (Case Report Form) and patient follow-up. Data manager: Responsible (together with Einstein’s technical Telemedicine team) for maintaining patient care system, data feeding and verification. Responsible to execute the Data Monitoring Plan. Sponsor (Brazil Ministry of Health): Approval of detailed study proposal, according to public interest, Project schedule development follow-up (quarterly face-to-face or virtual meetings; annual written report), Pre-publication consent (according to current legislation), No participation or interference in the analyses and results.
Contributors DTN, OTR and AJP developed the main study intervention. DTN, OTR and AJP developed the original concept of this study. DTN, OTR, MCdS, ASN, TDC, RA, LCDM, ABC, RSB, RGR, JIS, LCPA, GS, OB, EC, LJRF and AJP contributed to study design. DTN, OTR, MCdS, ASN and AJP wrote the first draft of the paper, and TDC, RA, LCdM, ABC, RSB, RGR, JIS, LCPA, GS, OB, EC and LJRF revised the first draft. The final manuscript was reviewed by all the authors. All authors read and approved the final manuscript.
Funding The Ministry of Health (Institutional Development Program of the Unified Health System-PROADI SUS) was the primary source of funding, including costs of physician services, purchase of equipment (hardware) for Telemedicine sessions, hiring of local professionals for data collection and travel expenses for training and monitoring. The same funding also covered costed related to the regulatory part of the study-data collection, monitoring, data curation and statistical support. The Hospital Israelita Albert Einstein allocated time of professionals and specialists who sat on the Trial Management Committee (TMC) of the study, as well as assign its Telemedicine service system.
Map disclaimer The depiction of boundaries on the map(s) in this article does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.