Article Text

Abstract
Setting Children especially those <5 years of age exposed to pulmonary tuberculosis (TB) are at a high risk of severe TB disease and death. Isoniazid preventive therapy (IPT) has been shown to decrease disease progression by up to 90%. Kenya, a high TB burden country experiences numerous operational challenges that limit implementation of TB preventive services. IPT completion in child contacts is not routinely reported in Kenya.
Objective This study aims to review the child contact management (CCM) cascade and present IPT outcomes across 10 clinics in western Kenya.
Design A retrospective chart review of programmatic data of a TB Reach-funded active, clinic-based CCM strategy.
Results Of 553 child contacts screened, 231 (42%) were reported symptomatic. 74 (13%) of the child contacts were diagnosed with active TB disease. Of those eligible for IPT, 427 (90%) initiated IPT according to TB REACH project data while 249 (58%) were recorded in the IPT register with 49 (11%) recorded as a transfer to other facilities. Of the 249 recorded in the IPT register, 205 (82%) were documented to complete therapy (48% of project initiation children).
Conclusion Our evaluation shows gaps in the routine CCM care cascade related to completeness of documentation that require further programmatic monitoring and evaluation to improve CCM outcomes.
- tuberculosis
- community child health
- paediatric infectious disease & immunisation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
One of the first attempts to assess isoniazid preventive therapy completion of therapy outcomes in Kenya.
Ten sites were visited to retrospectively collect programmatic data after a TB REACH initiative to expand child contact management.
Data regarding index cases and child contacts transferred to another facility were not available.
Introduction
Worldwide, tuberculosis (TB) is one of the top 10 causes of death and remains the leading infectious disease killer.1 Children—particularly those under 5 years of age—exposed to infectious pulmonary TB disease are at higher risk of severe disease and progression to death.2 It is estimated that 60%–80% of children with prolonged contact to a bacteriologically positive index case become infected with TB.2 3
WHO recommends that children under age 5 or living with HIV of any age exposed to bacteriologically positive TB should be screened and started on appropriate treatment—either isoniazid preventive therapy (IPT) if asymptomatic or active TB disease treatment.4 IPT decreases disease progression by approximately 90%.2 5 Operational challenges in the child contact management (CCM) care cascade—identification, screening, treatment initiation and completion of therapy—continue to exist in high TB burden settings.6 7 Only 27% of eligible children received IPT in 2018 globally.1
Kenya is one of 14 high TB burden countries with the highest burden of TB, multidrug-resistant TB and TB/HIV coinfection.8 Given the high burden of active TB disease, prioritising TB prevention is difficult with limited staff and resources. In 2018, only 34% of child contacts <5 years initiated IPT.9 Few African studies report varying degrees of IPT completion of therapy (COT) ranging from 12% to 76%.10–12 IPT COT outcomes among exposed child contacts have not been previously reported in Kenya.
At the Academic Model Providing Access to Healthcare (AMPATH) Partnership at Moi Teaching and Referral Hospital in Eldoret, Kenya, a previously described active, clinic-based child contact screening package funded through TB REACH Wave 2 was expanded across 10 sites in western Kenya in 2013 in an effort to improve CCM.13 Prior to the screening package, fewer than 1% of child contacts identified and documented by healthcare workers (HCWs) in a child contact register underwent clinical review with treatment decisons.14 In the first year of the screening package, 86% of child contacts were brought in for evaluation and 89% of IPT-eligible child contacts were initiated on the recommended 6 months of IPT.13
For this retrospective chart review of routine programme data, we visited 10 Wave 2 TB REACH treatment sites in western Kenya to retrospectively assess, for the first time, IPT and TB disease treatment outcomes for exposed child contacts as well as reasons leading to IPT deferral.
Methods
Study design
We conducted a retrospective chart review of routine programme data of IPT and TB disease treatment outcomes in exposed child TB contacts under age 5 at 10 sites across western Kenya. Our aim was to assess the final step of the CCM care cascade.
Setting
Kenya is a low-income and middle-income country with a TB incidence of 292 per 100 000 in 2018.9 The TB REACH active, clinic-based child screening package was implemented in TB clinics throughout western Kenya in 2013. The 10 TB clinics were located in urban (Eldoret, Webuye, Busia, Bungoma, Kakamega) and rural (Chulaimbo, Khunyangu, Kapenguria, Teso, Turbo) regions. As part of the TB REACH care programme, HCWs were asked to interview patients with active TB regarding child contacts and track the interview results in the CCM register. HCWs diagnosed TB in children based on the Kenyan National TB Programme (NTP) guidelines.15 In Kenya, the majority of TB in children is diagnosed clinically. This is due to the fact that facilities often lack personnel and supplies to conduct gastric aspirates.
Data collection and analysis
Data for the CCM programme were previously collected by TB clinic staff in the NTP child contact registers and project-specific child contact tracing forms. In 2016, members of the study team visited all 10 sites and collected data to assess IPT and TB disease treatment outcomes for child contacts screened between July 2013 and December 2014. A child was considered initiating treatment if the project tracking form for that child so indicated. IPT and TB disease outcomes were then retrospectively collected from the local facility registers (child contact register, IPT and Treatment of disease registers). Treatment outcomes that were recorded from the registers included (1) completion—indication in register that the child completed IPT or TB treatment (2) deferral—indication in register that the child’s caregiver deferred treatment (3) transfer to another facility—indication in register or on TB REACH child contact tracing form that child transferred to another facility or (4) diagnosed with TB disease while on IPT. It is important to note that registers did not include detailed information about treatment follow-up visits such as adherence to medication or side effects.
Data were deidentified and entered into a password-protected Microsoft Excel database. Descriptive analyses were conducted in STATA version 14.2.430.
Patient and public involvement
Given that this was a retrospective analysis of a care programme, we did not have contact with any patients. Results from this analysis were disseminated with members of the Kenyan NTP.
Results
Out of the 553 child contacts reviewed in the registers who were brought in for screening at the 10 TB clinics, 249 (46%) were male and 319 (58%) were exposed to an index case who was their parent. A total of 545 of the child contacts had an age listed and median age was 3 years. A total of 231 (42%) were symptomatic defined as the index case reporting that the child contact had one or more of the following—cough, weight loss/failure to thrive, fever or fatigue. Seventy-four (13%) of the child contacts were diagnosed with active TB disease (table 1).
Demographics of exposed child TB contacts <5 years of age who were screened
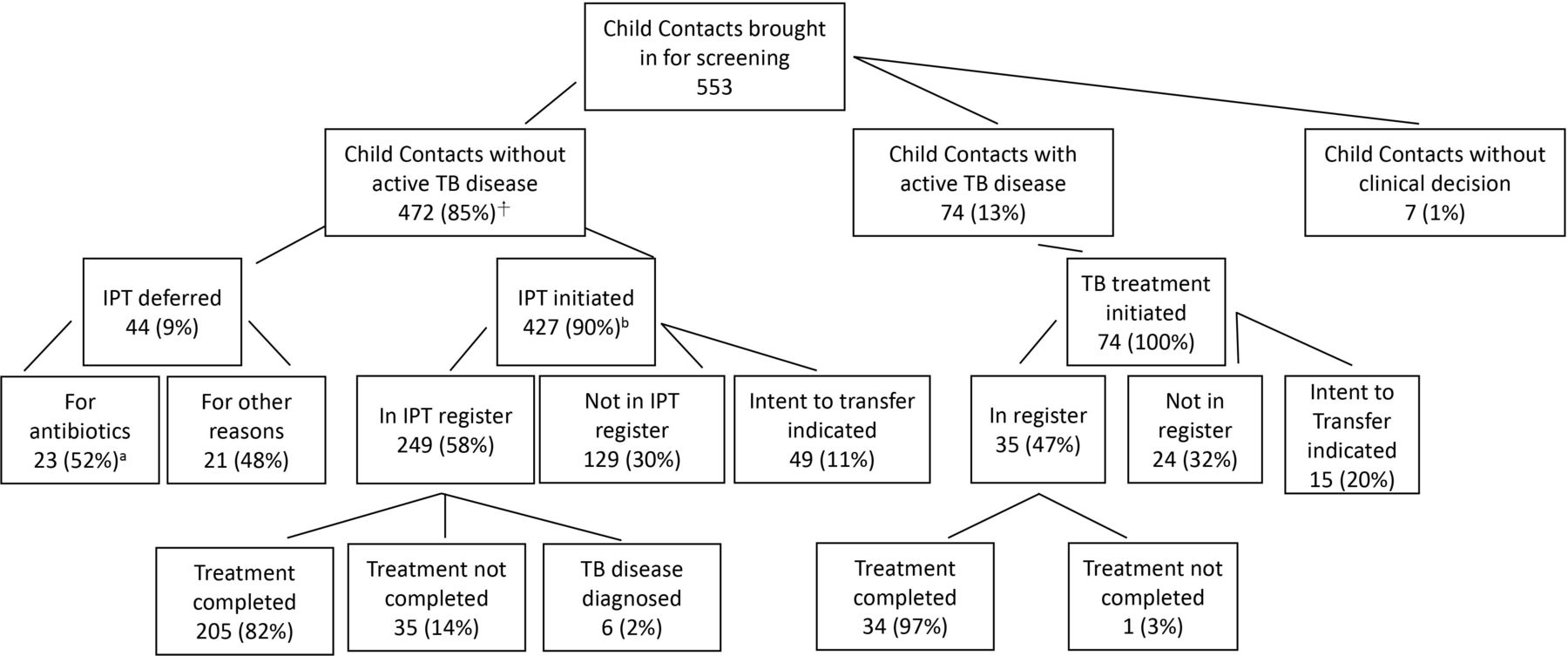
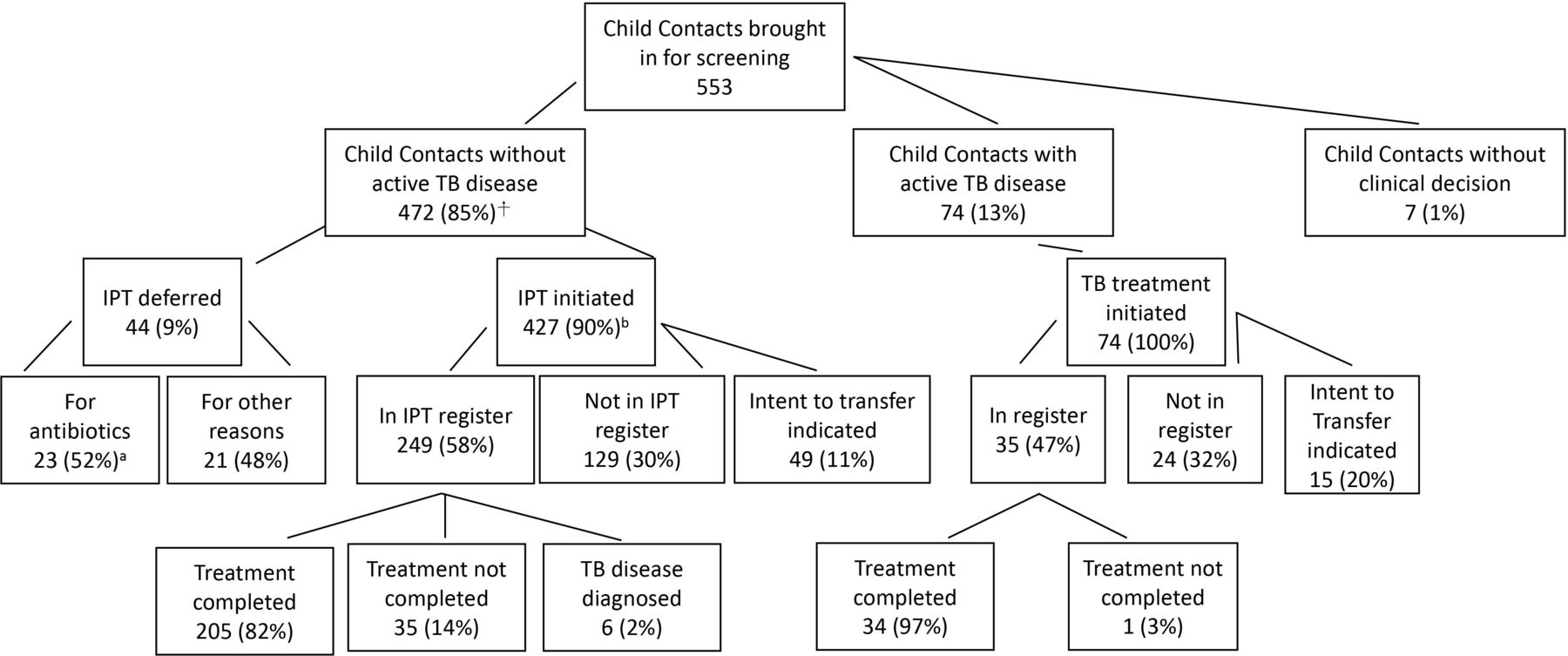
Of the remaining child contacts without active TB disease, no clinical decision was reported for 7 (1%). Of the remaining 472, 427 (90%) were documented on the child contact tracing forms to have initiated IPT. According to personal communication with HCW staff, IPT initiation documented on the project forms was only done so if the child was sent home with an initial course of treatment. Only 249 (58%) were recorded in the IPT register. Forty-nine (11%) had a plan to transfer documented on the child contact tracing form. Of the 249 recorded in the IPT register, 205 (82%) completed therapy; however, this is 48% completion if considering those who had documentation of IPT initiation initially on the child contact tracing forms (figure 1).
{kind=link}
Summary of child contact management outcomes in 10 TB clinics in western Kenya July 2013–December 2014. IPT, isoniazid preventive therapy; TB, tuberculosis. ⍏Percentage denominators represent the box immediately preceding; a6 returned and completed IPT; b1 child unknown.
Of the 74 child contacts diagnosed with TB disease, 100% had documentation of initiating TB treatment in the contact tracing form. Only 35 (47%) were found in the facility’s TB treatment register and 15 (20%) had an intent to transfer documented on the child contact tracing form. Of the 35 documented in the register, 34 (97%) completed therapy; however, this is only 46% completion if considering those who had documentation of TB treatment initiation initially on the child contact tracing form (figure 1).
Forty-four child contacts deferred IPT: 23 (73%) children initiated antibiotics for presumed upper respiratory infection, 3 (10%) had TB previously, 4 (13%) had already received IPT at another facility and 1 (3%) deferred to await an X-ray that was not available at the time of screening. None of the 24 children who deferred for reasons other than previous treatment or had TB previously were documented to have ever returned to start their IPT.
Discussion
Our assessment of a CCM screening package in western Kenya reveals several interesting findings. The TB REACH-funded programme used child contact screening forms that documented IPT initiation in child contacts that otherwise did not appear in the national IPT registers. In fact, 90% of eligible child contacts were reportedly initiated on IPT according to the programme’s forms, while only 58% were documented to have initiated IPT in the NTP registers. Personal communication with staff at the sites visited confirmed that child contacts were started on IPT if documented on the programme form. These rates of initiation are much higher than the most recent IPT initiation rate of 34% from 2018 and further suggests that an active, clinic-based CCM strategy may be an effective model for successful management of child TB contacts.
In the exploration of the fourth component of the CCM cascade—completion of therapy, we found that 48% of children documented to initiate IPT in our project child contact tracing forms had documentation of COT in the national databases. This suggests several potential systemic and logistical gaps. Once a child completed their clinical assessment and a treatment plan was determined, the following possible paths can occur: (1) the child may have started treatment at the clinic with documentation in a NTP register, (2) the child may have started treatment but was not registered (and therefore not counted and COT cannot be tracked), (3) the child may have been transferred to another clinic with a lack of clarity about if and where registration occurred or (4) the HCW documented intent to initiate IPT and treatment was never initiated. Each of these scenarios determines the likelihood of documentation of COT.
Eleven percent of the children fell into the third category above—stated transfer. We had no ability to verify the transfers, a problem also experienced by the Kenyan NTP in the setting of an evolving electronic reporting system. The 40% of children who were documented as initiating IPT by our project data capture, but not recorded or reported in the NTP registers, raises questions of what happened to the children—never started, started not recorded in register, or transferred? Given that HCWs reported that IPT initiation was only documented on project forms if the child was sent home on treatment, this suggests that children were started not recorded or transferred to another facility. Additionally, integration of grant-funded programmes into existing NTP data collection mechanisms is challenging and confusion can exist regarding the need for double entry of data versus entering data only in one location. It might be that a HCW did not complete the register after they completed the TB REACH child contact tracing form as this could seem like duplication. This is an important consideration for project teams to discuss with stakeholders and front-line HCWs. We also recommend that programmes assess data from both programmatic reporting tools and NTP registers periodically during the project. This would have allowed us to recognise the discrepancy in initiation and completion outcomes and investigate further in real time.
Of the children who programmatically were identified as starting on IPT and who entered the national registering system, 82% of the children identified within the NTP register as starting treatment had COT. This COT rate matches exactly the one found recently by Ngugi et al of IPT among children living with HIV at a national referral hospital in Kenya.16 These remarkably high COT rates also mirror the outcomes for Kenya for active TB disease. Methods for documentation of transfers for mobile populations are critical as well as training and supervision support around recording and reporting for programmes to understand fully what is happening to patient outcomes.
A major limitation to this evaluation is that we were not able to review data from surrounding facilities to crosscheck if child contacts were successfully transferred—this was due to the fact that the transfer facility was often not listed and the Kenyan electronic reporting system did not have complete IPT register data inputted. As reported in a systematic review regarding CCM implementation, there are numerous barriers throughout the CCM care cascade.17 Our study demonstrates that many additional steps exist beyond identification, screening, IPT initiation and IPT completion (in this case—transfer of care). As more and more programmes and researchers track the CCM care cascade, the reported gaps are actually important opportunities to conduct a deeper dive into the problem.
Another limitation is that this retrospective chart review was limited in rigour given that we were collecting data available in registers and programme forms. Additionally, a selection bias may exist with the child contacts reviewed in the registers. Parents/caregivers who brought child contacts in may be worried about their children’s health, which could explain the large number of child contacts who were reportedly symptomatic.
A final programmatic gap identified in our study was the outcome of children for whom IPT was deferred. Only 25% of child contacts who deferred for a course of antibiotics were brought back for IPT initiation. Tracking of child contacts in low-income and middle-income countries like Kenya requires further programmatic guidelines and infrastructure . The current lack of support leads to HCWs’ ‘non-decision’ regarding IPT and a missed opportunity for disease prevention.
Conclusion
This is one of the first attempts to report IPT completion of therapy outcomes among child contacts <5 years in Kenya. Our evaluation revealed potential gaps throughout the CCM care cascade—documentation of IPT initiation, transfer management and IPT deferral support. Our results also demonstrate the importance of integrating grant-funded monitoring and evaluation with routine reporting tools and that multiple reporting mechanisms can lead to confusion. Further support for programmatic monitoring and evaluation as well as revised guidelines for transfers and deferrals could lead to continued improvement in CCM outcomes.
Acknowledgments
We would like to thank all of the TB clinics’ health care workers in providing diligent attention to child contact management within their busy clinical services. We also acknowledge Dr Carol Bigelow for her statistical assistance.
Footnotes
Twitter @masinienos
Contributors JAA, EJC, EM and DS designed the study. JAA, DS and EJC collaborated to complete the data collection. JAA and DS completed the data analysis. EM provided CCM cascade expertise relevant to the Kenyan context. JAA, EJC, EM and DS wrote, edited and finalised the manuscript.
Funding The Child Contact Management (CCM) strategy was supported by the Stop TB Partnership’s TB REACH Initiative (Waves 2 and 5, Award Number N/A), which was funded by the Government of Canada. (Principal Investigator: EJC). The data collection was funded by the University of Massachusetts Office of Global Health Pilot Project program (Award Number NA). DS is partially supported by Institutional Development Award Number U54GM115677 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds Advance Clinical and Translational Research (Advance-CTR). DS is also partially supported by the Thrasher Research Fund (Award Number NA).
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Stop TB Partnership, or the Thrasher Research Fund.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval This study was deemed to be non-human subjects research by the University of Massachusetts Institutional Review Board. Retrospective data collection of the TB REACH-funded programme was approved by the Moi University School of Medicine Institutional Research and Ethics Committee and the Lifespan Institutional Review Board at Brown University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Deidentified participant data are available by contacting the PI (Orcid ID 0000-0001-5864-9011). Reuse would need to be discussed with the study team as well as the Kenyan National TB Program.