Article Text

Abstract
Introduction In Germany, an efficient and feasible transition from hospital to home for older patients, ensuring continuous care across healthcare settings, has not yet been applied and evaluated. Based on the transitional care model (TCM), this study aims to reduce preventable readmissions of patients ≥75 years of age with a transitional care intervention performed by geriatric-experienced care professionals. The study investigates whether the intervention ensures continuous care during transition and stabilises the care situation of patients at home.
Methods and analyses Randomised controlled clinical trial, recruiting between 25 April 2018 and 31 December 2019 in one German hospital in the city of Regensburg. The intervention group is supported by care professionals in the transition process from hospital to home for up to 12 months. Based on TCM, the intervention includes an individual care plan according to a patient’s symptoms, risks, needs and values. The plan is advanced in the domestic situation via personal visits and telephone contacts. All necessary care actions regarding, for example, mobility, residence adjustments, or nutrition, are initiated to be executed by ambulant care services, and are monitored, evaluated and adapted if necessary. In supervising the care plan, the care professionals do not administer active care services themselves but coordinate them. Patients and their caregivers are actively engaged in the care planning and execution. In contrast, the control group receives only usual discharge planning in the hospital and usual ambulatory care.
The primary outcome is the all-cause readmission rate assessed using health insurance data within a follow-up of up to 12 months after hospital discharge. Secondary outcomes include care quality, mobility, nutritional and wound situation, and health-related quality of life. They are assessed at baseline, after 1 month, 3 months, 6 months, and at the end of study visit. Additionally, the economic efficiency of the intervention will be evaluated.
Ethics and dissemination Ethics approval for the trial was obtained from the Ethics Committee of the Friedrich-Alexander-Universität Erlangen-Nürnberg. Results will be published in peer-reviewed, open-access scientific journals and disseminated at national and international research conferences and through public presentations in the geriatric and healthcare community.
Trial registration ClinicalTrials.gov identifier: NCT03513159.
- geriatric medicine
- quality in health care
- risk management
- clinical trials
- internal medicine
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- geriatric medicine
- quality in health care
- risk management
- clinical trials
- internal medicine
- public health
Strengths and limitations of this study
The findings of the trial will help to define so far missing recommendations for the implementation of efficient transsectoral care for older patients in the German healthcare system.
Transitional care professionals in the study offer a potential long-term benefit for home-dwelling patients, supporting them for up to 12 months.
The intervention is highly individualised to each participant’s needs and situation, but overall addressing and evaluating the importance of a broad spectrum of aspects, such as mobility, nutrition and care quality.
In case of readmission of a participant, the care professional promotes continuity of care and information transfer from the ambulant care setting back into the hospital, but due to the setting, this conclusion can only be drawn for the hospital of the study.
Patients with cognitive deficits might profit from our intervention; however, only individuals with a Mini-Mental State Examination Score of at least 22 points are included to ensure that participants are able to benefit from the self-management approach of the TCM.
Introduction
Considerable medical progress and improved living conditions in the last decades have enabled an increasing life expectancy, leading to a marked ageing of the population in Europe.1 Expanded life expectancy is, however, often accompanied by multimorbidity, poorer quality of life, loss of function, polypharmacy and inconsistencies in care,2 3 resulting in increased hospital admissions.4 Moreover, in Germany, approximately 30% of hospital patients who are ≥70 years old, show a hospital-associated impairment in activities of daily living (ADL) and health-related quality of life at hospital discharge.5 Mobility and nutritional status are especially prone to deteriorate during hospital stays in older patients6 and can lead to rehospitalisations. In addition, patients with chronic wounds (eg, diabetic feet) run the risk of poor wound healing and wound care during transition from hospital to home. Moreover, the Diagnosis-Related Groups hospital payment system, promoting a shortening of hospitalisation days to reduce costs, enhances the risk for early unplanned rehospitalisations.7 As reported in 2015, in 20% of Medicare beneficiaries in the USA, readmissions occur within 30 days of discharge and in 34% within 90 days, leading not only to additional loss of independence of patients, but also to additional costs for the healthcare system.8 9 Thus, the USA instituted the Hospital Readmissions Reduction Programme holding hospitals accountable for unnecessary rehospitalisations.10
In Germany, as opposed to the mostly private sector healthcare of the USA, healthcare builds on a socialised compulsory insurance system. Generally, citizens either join a public or private health insurance fund. Public healthcare organisation and financing are under joint self-government of physicians, health insurances, hospitals and insurees, and are performed by private and public providers. This led to the development of fragmented, rigid, consolidated structures with separate in-hospital and ambulatory care programmes and reimbursement options, causing particular problems to bridge the gap between hospital and ambulatory care efficiently and from one source. To address deficiencies in the transition process from inpatient to home-setting, the German government amended a law in 2012 to improve healthcare structures and to strengthen the patients’ rights for discharge planning (§39 SGB V). However, hospital discharge planning is not sufficient to guarantee the patients’ readaptation and well-being at home after hospital discharge.11 12 It has been reported that the implementation of actions initiated by discharge teams could not be verified at home, arranged adaptations not audited and interruptions in the continuity of care not identified.13 14 Family physicians point to an unmet need for medically competent contact persons inside hospitals to efficiently communicate medical issues regarding patients transferring from hospital to home.15 Relevant information might be lost, provoking health deterioration and conceivably preventable readmissions.15 16
A distinct need for action was declared in Germany for older people with multimorbidity, notably for people 80 years of age and above. They experience increased vulnerability through complications, secondary diseases, chronic conditions, heightened risks of autonomy loss as well as a loss of self-help capacity facing increased hospitalisations.17
Applying transitional care programmes aiming at patients with high risk for poor outcomes and readmissions, such as older people with multimorbidities and complex chronic diseases can reduce preventable readmissions by up to 75%.18–24
The most rigorously tested model that has consistently demonstrated effectiveness to promote safe, timely and appropriate transfer between settings comprising education interventions, pre-discharge evaluation and patient-centred care at home, is the transitional care model (TCM).21 22 25–27
This is the first large randomised controlled trial in Germany that aims to evaluate an efficient and feasible care transition from hospital to home for older geriatric patients ≥75 years of age, based on TCM,22 and not disease oriented. It integrates discharge planning in the hospital with ambulant healthcare providers such as family physicians and ambulant care services to sustain patient care continuity across settings. The study investigates geriatric patients in a semi-rural setting in southern Germany, so cultural aspects could influence the transitional process from hospital to home.
Since academically educated advanced nurse practitioners are only starting to be trained in Germany, the intervention is performed by geriatric-experienced care professionals embedded in a team combining complementary expertises. As the care professionals find and guide the path for patients for better care, they are called ‘pathfinders’.
Objectives
The main objective is to improve geriatric care at the transition from hospital to home, reflected by a reduction of the all-cause readmission rate within a follow-up of up to 12 months after hospital discharge (primary outcome) in a randomised controlled trial. We hypothesise that the TCM-based intervention performed by geriatric-experienced care professionals will achieve a readmission reduction by improving the care situation of the patients at home and according to their housing and caregiving situation, contributing to a stable or improved state of their mobility, functionality, nutrition, wound healing, independence and health-related quality of life while reducing costs.
The effects of the intervention will be analysed and its efficacy and feasibility evaluated to be able to make recommendations on which parts or activities of this TCM-concept intervention might be implemented in the German healthcare system.
Methods
Trial design and study setting
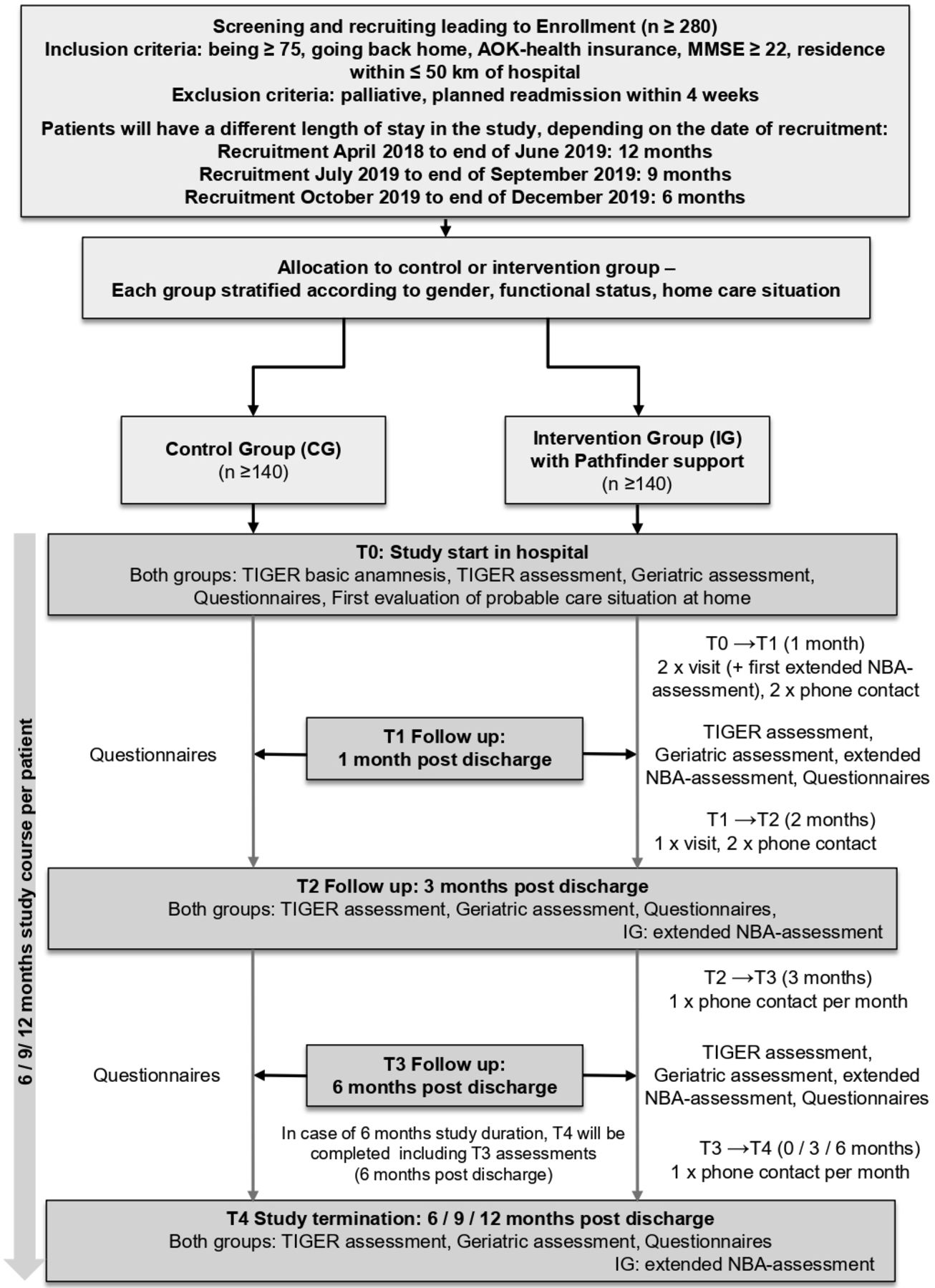
The Transsectoral Intervention Programme for Improvement of Geriatric Care in Regensburg (TIGER) study is a randomised controlled clinical trial with an intervention and a control group (see figure 1). It takes place at the St John of God Hospital, Regensburg (‘Barmherzige Brüder Regensburg’, BBR), Germany, in the city of Regensburg and surroundings. Since the effectiveness and feasibility of the application of a transitional care intervention itself will be evaluated in the study, the intervention is focusing on one hospital setting. The timeline of the overall TIGER project is depicted in figure 2.

Study design. MMSE, Mini-Mental State Examination; NBA, Neues Begutachtungs Assessment, an assessment to determine eligibility for benefits from the long-term care insurance in Germany31 ; TIGER, Transsectoral Intervention Programme for Improvement of Geriatric Care in Regensburg

{kind=link}
{kind=link}
Timeline of overall TIGER project. eCRF, electronic case report form; TIGER, Transsectoral Intervention Programme for Improvement of Geriatric Care in Regensburg.
Participant timeline
The study duration per participant is at least 6 months, and in the case of early recruitment (before end of June 2019) 12 months (see figure 1). Since recruitment was lagging, as also reported in other clinical trials engaging persons over 65 years,28 we prolonged the recruitment phase from initially planned 12 months to 20 months to reach the calculated sample size. The follow-up visit plan had to be adapted, since the end of the overall study intervention phase could not be prolonged proportionately due to project funding reasons. The intervention period is planned to end on 30 June 2020. In figure 1, the timeline for each participant according to his recruitment date is illustrated with all visit times T0–T4. The schedule of intervention and control group assessments is presented in table 1.
Visit plan and standardised assessments of participants
Eligibility criteria
Male and female patients from all wards of BBR, aged 75 years or older, and being insured by the statutory health insurance AOK (Allgemeine Ortskrankenkasse) Bavaria are eligible for this study. Patients need to reside within a radius of 50 km distance to the hospital, return to their home environment after discharge and reach a Mini-Mental State Examination (MMSE)29 result of at least 22 points. Although patients with less than 22 points in the MMSE might also benefit from the intervention, we chose this threshold to ensure that participants will be able to benefit from the self-management approach of the TCM, and to fill out questionnaires themselves. Exclusion criteria are palliative care situation (defined by the statement ‘therapeutic goal: palliative’ (instead of curative) in the medical report) and planned readmission to the hospital within the next 4 weeks.
Recruitment process
A TIGER-specific IT tool supported screening for potential participants according to the eligibility criteria age, health insurance and residence within a 50 km radius electronically in all wards via the patient management system of BBR. All patients admitted between April 2018 and December 2019 were scanned by this tool. Potential participants identified by this tool were visited in person by the TIGER staff who assessed all other eligibility criteria and informed about the project. Patients in BBR fulfilling all eligibility criteria and present caregivers were then provided with the participant information brochure and informed consent form (ICF) (see online supplemental file 1). Patients were given at least 1 day to read the provided information and informed consent form and receive further information on the project. After signing and dating the informed consent form, the MMSE29 was performed as a last inclusion criterion for recruitment.
Supplemental material
Randomisation
Stratified block randomisation was performed with the following three strata1: (1) gender (male/female), (2) mobility (can walk at least four stair steps: yes/no)30 and (3) living condition (lives alone: yes/no). These strata were chosen because of their potential to influence the overall need for care and study outcomes.
The randomisation blocks varied between 2, 4 and 6 to guarantee a minimum of predictability for the randomisation. When receiving a recruitment number for a newly recruited participant in the electronic data acquisition and electronic case report form (eCRF) System (secuTrial®), the stratification questions had to be answered, the inclusion criteria affirmed and the exclusion criteria denied in the eCRF file. Then, the randomisation into intervention or control group was performed automatically by the eCRF system.
Study staff and training
Academically educated advanced nurse practitioners are not available yet in Germany. The study is thus performed by geriatric-experienced care professionals called ‘pathfinders’, consisting of a registered nurse, a case manager, a head nurse and an occupational therapist, to combine and exchange if needed multiple expertises when addressing the broad spectrum of care need aspects, such as care quality, mobility and nutrition. Each pathfinder of the TIGER project is exclusively responsible for his TIGER participants. They are supported by the study physician. The staff is divided into pathfinders supporting the intervention group participants, and study nurses assessing the control group participants (see also table 1). To prevent contamination between the intervention and the control group in the hospital, all patients receive usual care as far as the non-TIGER hospital staff is concerned. Additional actions in the intervention group are initiated by the pathfinders.
The staff was trained in a 4-week TCM programme, including sessions on therapeutic and care requirements regarding physical performance, mobility and functionality, nutrition, wounds, the discharge planning of BBR, current legislation aspects of social law, health insurance and welfare opportunities by respective experts. The intervention programme with the necessary assessments, as well as the documentation, were taught and a detailed protocol of operations provided. During the study, weekly case conferences take place with all members. Pathfinders can seek and will obtain further training in specific diseases or care management topics throughout the study.
The study begins inside BBR and continues after discharge in the participants’ homes for up to 12 months.
Intervention and intervention group
For the intervention group (IG), the pathfinders’ activities are based on the TCM.22 The authors described 9 distinct but interdependent components in their programme, which may be combined both before and after discharge to achieve the best results for the participants. The TIGER intervention is based on all 9 components of the TCM (see table 2). For the German hospital and home setting of this study, however, the modules needed some adaptation due to German healthcare settings, work law and local requirements, as described in table 2.
Adaptation of TCM modules to the TIGER study intervention group in German healthcare setting
Intervention
IG participants and their caregivers are accompanied by one pathfinder each in the process of hospital discharge, during the transition from hospital to home and for a minimum of 6 months up to 12 months after discharge (see figure 1). An individual care plan is developed by the designated pathfinder for each of the IG participants according to their symptoms, risks, needs and values (eg, physiotherapy, drug application and nutritional counselling) and in close collaboration with the care team (see table 2 ‘Collaborating’, including the family physician). All care activities for the IG participants are initiated by the pathfinder within the care team. The pathfinder coordinates, monitors, evaluates, adapts, if necessary, and documents the execution of the activities and the participants’ adherence. In developing the care plan, the pathfinders do not provide active care services themselves, but coordinate their execution by contacting ambulant services for the required service activities. For the project, it was essential to ensure that the pathfinders would not compromise the operational tasks of the usual ambulant services to be able to build a trusting relationship with these services. Participants and their caregivers are actively engaged in the care planning process. Progressively during the course of the intervention, self-management is promoted.
The family physicians of the IG participants are invited to actively take part in the study by the TIGER consortium partner Regensburger Aerztenetz, a network of family physicians in Regensburg, but this is no inclusion criterion. The IG participants are visited by the pathfinders and contacted by telephone. The individual care plan is regularly evaluated in the home visits (at least two times a month in the first month after discharge, at least once in a month in the second and third month after discharge) and telephone calls (at least two times in the first month after discharge and at least once in a month in all the following months until the end of study visit).
The pathfinders’ work is supported by a standardised questionnaire instrument based on the ‘Neues Begutachtungs Assessment’, an assessment to determine eligibility for benefits from the long-term care insurance in Germany,31 to identify individual care needs out of a broad range of possible care needs as well as to document and evaluate the needed or already initialised measures (for details on the spectrum of specified care needs see table 2).
In the IG, the standardised assessments (see section ‘Assessments of both groups’) take place at the beginning (T0), after 1 month (T1), 3 months (T2), 6 months (T3) and at the end of study (T4).
Control group
The control group (CG) receives usual hospital discharge planning by hospital staff not related to the TIGER study and usual ambulatory care after discharge. Usual discharge planning involves the first initiation of procurement of therapeutic adjuvants or appliances after hospital discharge, taking the hospital information, and if possible, a conversation with the patient and a caregiver into account. Medication for the first few days after discharge is supplied. No verifications of the arrangements at home are possible; the family physician of the patient is not contacted. No measures are initiated associated with the TIGER study.
The CG is assessed (see section ‘Assessments in both groups’) by the TIGER study nurses at the beginning (T0), after 3 months (T2) and at the end of the study (T4). It fills out the standardised questionnaires for participants also at T1 (after 1 month) and T3 (after 6 months) (see table 1).
Assessments in both groups
All study participants receive regular standardised assessments at visits T0–T4 using validated instruments (see table 1) to assess health and care degree, functionality and mobility, nutritional status, geriatric and cognitive situation, and domestic care situation. Since a comprehensive geriatric assessment is not mandatory in all wards at hospital admission of an older patient, it is administered in the TIGER study directly at recruitment and up to four times after discharge (depending on IG/CG and duration of participation: 6–12 months).
Additionally, health-related quality of life, personal psychosocial resources regarding health, wound-related quality of life, stress perception, as well as the burden of informal caregivers, are assessed by questionnaires to be filled out by the study participants autonomously. Table 1 gives an overview of when and which assessments are performed by the pathfinders and study nurses in the IG and the CG, respectively.
If the family physician of an IG participant agrees to participate in the study, he or she performs the geriatric assessments for the study (see table 1) at visits T1–T4 (see figure 1). Otherwise, the geriatric assessments at visits T1–T4 are performed by the study physician or pathfinders for the IG, and by the study physician or study nurse for the CG.
Outcomes
The primary outcome is the readmission rate, since the application of TCM in the USA has shown to reduce the readmission rate as a major negative outcome for geriatric patients leaving the hospital.25 27 Readmission rate is defined as the proportion of patients who have at least one unplanned readmission into any hospital (not rehabilitation clinic) within a follow-up of up to 12 months after hospital discharge, using anonymised data of the health insurance fund AOK Bavaria.
Secondary outcomes include care situation, care supply, and quality at home, functionality, and mobility, nutritional status, geriatric assessment-outcomes (depression and cognitive status, and ADL), questionnaires for participants outcomes (wound condition, health-related quality of life, psychosocial resources of participants regarding health and burden of informal caregivers), frequency of transfers into nursing homes. A detailed description of all assessment instruments and time points of data collection, including quotes, is depicted in table 1.
Another important secondary outcome is the efficiency of the pathfinder intervention. In a cost–cost analysis, costs of both groups (eg, intervention costs and healthcare costs) will be compared, to assess if the intervention leads to monetary savings. In an additional cost–utility analysis, costs of the intervention will be compared in both groups to non-monetary benefits (eg, higher quality of life).
Sample size
Based on international studies,21 25 27 it can be assumed that the implementation of a transitional care concept can reduce the readmission rate by 40%. An analysis of AOK Bayern data of 2018 points to a readmission rate of approximately 41.9% for people above 75 years of age in Germany. Thus, we expect the general readmission rate of 41.9% to drop by 40% to a readmission rate of about 25.1% by the intervention. We aim at determining this effect with a level of significance of 5% and a power of at least 80% with the intervention and control group of equal size. Therefore, 280 intention to treat participants in total are calculated to be sufficient to reach a statistically significant validation and statement based on the assumptions stated above, and taking a loss-to-follow-up rate of 15%–20% into account.
Data collection and monitoring methods
The recruitment period started with the first-patient-in on 25 April 2018 and ended on 31 December 2019. The pathfinders, study nurses and partly the study physician and/or participants’ family physicians collect the assessment and questionnaire data on paper forms at visits T0, T1, T2, T3 and T4, respectively, for each participant (see table 1) and before data entry into the eCRF. Any change in care setting, form or participation is documented in a standardised format (eg, necessary readmission with entry date and discharge date, commission to nursing home, participant’s wish to discontinue and death) for subsequent evaluation.
For monitoring data quality and completeness, double data entry is performed for the assessments. Data from the paper forms are entered into the eCRF by two different eCRF-trained research associates in two input forms. In case of differences between the two versions of data input, the original paper file is checked, and the entry corrected accordingly.
Once a month, the trial site, pathfinders and study nurses are monitored by the project coordinator. Trial conduct and recruitment are discussed, possible obstacles identified and other consortium partners are invited to the meetings if indicated. Problems in performance, quality, medical or other issues are analysed, solutions initiated and implemented. Consequent protocol of operations amendments are implemented, and new protocol versions distributed within the consortium. The ethics committee is informed on protocol amendments regarding ethical issues. Amendments are introduced into the clinical trials.gov file.
Statistical methods
The primary outcome hospital readmission rate will be evaluated by Fisher’s exact test. The main analysis will be performed for the first 3 months follow-up of patients after discharge. In addition, a subanalysis will be performed with data after 6 months, 9 months and 12 months follow-up. Possible interactions with housing situation, availability of caring relatives and risk factors like care dependency or limitations in cognition will be analysed by multiple regression for a better understanding of the intervention’s impact on the hospital readmission rate.
Secondary outcomes (eg, quality of life and mobility) will be analysed by t-test, Fisher’s test, Mann-Whitney test or χ2 test, depending on distribution and number of cases. Subgroup analysis will be performed for primary and secondary outcomes, for example, for participants with or without caregivers, for participants with risk of malnutrition and for participants with different classifications from long-term care insurance.
Repeated measurements will be analysed by Analysis of Variance (ANOVA) or linear mixed model.
To deal with missing data, for the primary outcome, complete case analysis will be applied. In case of the secondary outcomes, either complete case analysis or, if appropriate and applicable, multiple imputation will be considered.
The analysis of possible financial benefits of implementing a pathfinder will be carried out by t-test. The main analyses will be performed using SPSS (IBM SPSS Statistics 26) and R.
Patient and public involvement
One of the TCM’s activities and a part of this study’s design is the engagement of patients and their caregivers in their own care planning, so every participant is actively involved in the construction of his/her own care planning and in the conduct of the study. Progressively during the course of the intervention, self-management of the participants is promoted.
Confidentiality
The signed ICF of the participants are stored in BBR separate from the assessed data of the participants, anonymised with the participants’ eCRF IDs. The list that contains both participants’ names and their eCRF IDs is stored on a stand-alone PC without internet connection, being deleted after the study. Original paper files are archived according to data protection regulations of Bavaria, Germany.
Ethics and dissemination
Research ethics approval
The ethical committee of Friedrich-Alexander Universität Erlangen-Nürnberg approved the study on 5 March 2018 (# 60–18 B) prior to first participant inclusion. The study will be conducted in accordance with the Declaration of Helsinki.
Harms
We expect no harm due to the study since all interventions are performed by experienced professionals, and medical as well as nursing care of participants remain proficient.
Access to data
The final anonymised trial data set will be available to the TIGER consortium. After completion of evaluation and dissemination by the TIGER consortium, the anonymised data set will be available to interested researchers on demand.
Ancillary and post-trial care
CG participants are provided at the end of study visit with a short explanation and feedback letter concerning the development of their health scores throughout the study regarding MMSE, Geriatric Depression Score,32 Mini Nutritional Assessment,33 34 as well as handgrip strength (see table 1) over time. Each IG participant receives a list of the contacted ambulatory services helpful during the intervention at the end of study visit.
Dissemination policy
The study was registered at clinical trials.gov. According to outcomes, the results will be published in peer-reviewed scientific journals and disseminated in the geriatric and nursing care specialised healthcare communities, to promote effective intervention activities for the process of introduction into regular healthcare.
Discussion
Local adaptations of the TCM were described as being necessary by the architects of the model themselves.35 The application of the TCM modules within the TIGER trial in Germany also needs adaptations, mostly contextual in nature (see table 2) or due to the German healthcare settings. For the module ‘Collaborating’, the family physicians for the intervention participants can actively take part in the study performing the geriatric assessments and having regular information exchange with the pathfinder on behalf of the joint participant. This integration of family physicians directly in the study design stresses their essential role not only in post-discharge management of the patient, but underlining the transsectoral importance of a collaborative team.
We experienced a considerable lag behind the planned recruitment. This encountered recruitment difficulty is also reported in other clinical trials that engage persons over 65 years of age. Discussed reasons for higher challenges of recruitment of this vulnerable patient group are their feeling unwell at recruitment, too long and detailed participant information sheets and not wishing to take advice from additional healthcare persons or to have visits at home.28
To address recruitment difficulties, we introduced from the beginning a face-to-face and stepwise approach of information provision of study content to participants, as recommended.28 Adaptations and optimisations of the recruitment process were implemented to maximise recruitment success. Thus, we expanded the included wards from originally three wards to all wards of the hospital, that could harbour eligible TIGER participants. In case the questionnaires for participants would be a too high burden and thus an impediment to participate, we allowed participants to take part and only join the assessments and intervention. Also, the recruitment schedule and follow-up visit plan were adapted. In our original study design, a follow-up of up to 1 year after discharge was targeted27 for a comprehensive evaluation, offering a long time benefit to the participants. Since a minimum follow-up of 6 months has been discussed as also being effective in reducing readmission rates significantly in patients over 65 years of age,21 36 37 while lowering healthcare costs, the adapted study design prolongs the recruitment phase (from 12 months to 20 months) allowing for a follow-up of at least 6 months for those participants recruited after June 2019 (see figure 1).
According to Greysen and colleagues,38 participants who are more fragile (poorer physical function, older age, suffering from multimorbidity, impairment in ADL, etc) are the ones who tend to present higher readmission rates. Since there is still a gap of knowledge on the efficiency of TCM concepts for geriatric patients significantly older than 65 years of age, it will be interesting to see which participants in the TIGER study profit most from the intervention. The detailed analysis of assessments of mobility and functionality, nutrition, geriatric issues and wound situation of the TIGER study will shed light on the most needed areas of intervention for this vulnerable patient group, even if the readmission rates of this patient group ≥75 years of age with chronic disease might not be reduced as much by the intervention as anticipated.
In general, this study shows a wide scope of combined qualitative and quantitative analyses of the care situation of geriatric patients, of influencing factors and of the impact of pathfinders activities on readmission rate. The study will provide important additional data on the TCM component implementation over different time periods ranging from 4 weeks to 12 months. On a national level, it will add knowledge concerning if and how a transitional care concept or parts of it can also be applied in Germany with its fragmented established structures in order to define necessary steps to improve continuous transitional care for the geriatric patient group analysed in this study.
For patients with cognitive deficits, further transitional care intervention studies need to be conducted.
In case of a positive evaluation regarding its scientific and health-economic outcomes, a prospective goal is to define clear implementation possibilities of pathfinder activities for the analysed patient group in the German healthcare system.
Acknowledgments
Principal investigator and project coordinator is the Institute for Biomedicine of Ageing. The Federal Association of Geriatrics reviews current projects in Germany, including geriatric patients who are discharged from hospitals for the project, and will disseminate results in interacting with healthcare stakeholders. The intervention takes place at BBR in collaboration with the Regensburger Aerztenetz. The health insurance fund AOK Bavaria will provide anonymous routine data for evaluation. Psychogerontological advice is provided by the chair for social medicine and prevention at University Medicine Greifswald. The scientific and health-economic evaluation will be performed by the Institute for Nursing Science at the University of Bielefeld, and the chair of health management at the University Erlangen-Nürnberg, respectively.
We thank the TIGER (Transsectoral Intervention Programme for Improvement of Geriatric Care in Regensburg) staff Sarah Blaimer, Teresa Freund, TG, Claudia Gradl, Sylvie Lamotte, Renate Roetzer, Christina Schrader and Manfred Seitz, and the study physician Stephan Theobaldy for their relentless recruiting efforts and ongoing finding of individual best care paths.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MR: project coordination, study supervision, improvements of study design and writing the original manuscript. JW: partaking in original study design and partaking in original manuscript writing. SB: drafting manuscript figures and revising the manuscript. TG: improvements in study design and revising the manuscript. MH, DvdH, AK, TK, OS, DV, KW and SW: partaking in original study design and revising the manuscript. EF: conceptualisation of study and study design, and revising the manuscript. CS: conceptualisation of study and study design, revising the manuscript and principal investigator.
Funding The project TIGER (Transsectoral Intervention Programme for Improvement of Geriatric Care in Regensburg) is funded by the Innovation Fund at the Federal Joint Committee of Germany (https://www.g-ba.de/english) with the funding number 01NVF17005.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.