Article Text

Abstract
Objective We aimed to determine the association between meteorological factors and sudden sensorineural hearing loss (SSNHL) audiogram configurations.
Design Retrospective review of medical records from 1 October 2007 to 31 December 2018.
Setting A tertiary hospital.
Participants 510 patients with SSNHL who had data on the exact date of SSNHL onset and underwent audiological evaluation within 14 days were included.
Primary and secondary outcome measures Daily values of meteorological factors, including maximum and minimum temperature, mean temperature and its day-to-day change, diurnal temperature range, atmospheric pressure, mean and maximum wind speed and relative humidity, and seasonal distributions.
Results Among the 510 patients (259 women (50.8%); mean (SD) age, 46.4 (15.5) years), 108 (21.2%) displayed ascending patterns, 143 (28.0%) displayed descending patterns, 129 (25.3%) displayed flat patterns and 130 (25.5%) displayed profound patterns of audiograms. The diurnal temperature range on the day of SSNHL onset in patients with profound patterns was significantly higher than that in patient with ascending (mean difference (MD), 2.2°C; 95% CI, 0.7°C to 3.7°C; p=0.001) and descending (MD, 1.5°C; 95% CI, 0.1°C to 2.9°C; p=0.031) patterns. The relative humidity was the highest on the day of SSNHL onset in patients with ascending patterns and showed a significant difference compared with that in patients with profound patterns (MD, 8.0%; 95% CI, 0.7% to 15.3%; p=0.026). Seasonal distribution did not differ among patients with different audiogram configurations.
Conclusions Profound audiogram patterns correlated with high diurnal temperature range, while ascending audiogram patterns correlated with high relative humidity in patients with SSNHL. No correlation was observed between seasons and audiogram configurations.
- otolaryngology
- neurotology
- audiology
Data availability statement
Data are available upon reasonable request. The meteorological data are available on the website of National Climatic Data Center (http://www.ncdc.noaa.gov/). Data of the enrolled patients will be shared by request from any qualified investigator.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Meteorological factors are associated with the incidence and prognosis of sudden sensorineural hearing loss (SSNHL); however, there are limited data on its correlation with audiogram configurations of SSNHL.
This study included patients diagnosed with SSNHL within 14 days after SSNHL onset to mitigate recall bias from the retrospective design.
This study was conducted at a single tertiary hospital that receives patients from all over the country.
Introduction
Sudden sensorineural hearing loss (SSNHL) is an otological emergency defined as hearing loss occurring over a relatively short period of time with no identifiable cause. SSNHL affects 5–27 individuals per 100 000 people annually, with approximately 66 000 new cases per year in the USA alone.1 Although various theories have been proposed, such as vascular impairment, viral infection, rupture of the labyrinth membrane and immune-mediated disorder, the aetiology of SSNHL is unclear.2–4
Vascular impairment is a widely accepted theoretical mechanism for SSNHL. The inner ear is supplied by the labyrinthine artery, which is a functional end artery that terminates in two branches supplying the cochlea and vestibular organ. The cochlea is susceptible to ischaemic injury through various vascular insults, such as thromboembolism or vasospasm.5 Further, shunting from the periphery cannot compensate for disturbances in the blood supply to the cochlea because the labyrinthine artery is a terminal artery and is positioned intraosseously. Animal models have shown that impairment in microcirculation of the cochlea leads to immediate loss of function of the organ of Corti.6 Moreover, the clinical characteristics of SSNHL are similar to those of other ischaemic vascular diseases7—symptoms develop abruptly without any preceding signs and only one side of the ear is affected in general. Many studies have reported that diseases of vascular origin, such as acute myocardial infarction,8 stroke9 and migraine,10 are correlated with meteorological factors. However, studies have drawn inconsistent conclusions regarding the correlation between SSNHL and meteorological factors.
The audiogram configuration of SSNHL can be categorised into five distinct patterns: ascending, descending, flat, profound and others.11 Each audiogram pattern is considered to be the result of different pathogenetic mechanisms.12 This study aimed to investigate the association between meteorological factors and different audiogram configurations of SSNHL.
Patients and methods
Study population
This retrospective cross-sectional study included patients who were diagnosed with SSNHL at the Otorhinolaryngology Department in our hospital between 1 October 2007 and 31 December 2018. The diagnostic criteria for SSNHL were unexplained hearing loss of ≥30 dB at more than three consecutive pure-tone frequencies occurring within a 72-hour period. Patients who underwent audiological evaluation within 14 days of SSNHL onset were included. Patients with known causes of hearing loss, including middle ear disease, Ménière’s disease, acoustic neuroma and large vestibular aqueduct syndrome, were excluded. The medical records of all patients were thoroughly reviewed. Data on demographics, clinical parameters and date and geographical location of SSNHL attacks were collected. Laboratory results at the time of hospital admission were recorded, including complete blood count, coagulation panel and biochemical test results. All patients were treated with intravenous steroids (methylprednisolone 40 mg/day) for 5 days. Patients who did not achieve complete recovery received intratympanic steroids (methylprednisolone 20 mg every 2 days) on days 6, 8, 10, 12 and 14 in different combinations with blood flow-promoting drugs, vasodilators, vitamins and diuretics. Written informed consent that authorised the use of personal medical data in the study was obtained from all patients. The study was conducted in accordance with the Declaration of Helsinki.
Auditory evaluation
Pure-tone audiometry was performed on the day of inclusion and at the end of treatment on the 14th day. The pure-tone average was calculated from the air conduction thresholds at 500, 1000, 2000 and 4000 Hz in the affected ear. Initial audiogram configurations were classified as ascending (the average threshold of 250–500 Hz was 20 dB higher than 4–8 kHz), descending (the average threshold of 4–8 kHz was 20 dB higher than 250–500 Hz), flat (similar threshold across the entire frequency range) and profound (flat configuration with hearing threshold >90 dB) patterns. The level of recovery was evaluated according to Siegel’s criteria as follows: (1) complete recovery: final hearing <25 dB, (2) partial recovery: >15 dB gain and final hearing 25–45 dB, (3) slight improvement: >15 dB gain and final hearing >45 dB; and (4) no improvement: <15 dB gain and final hearing >75 dB. The overall recovery is the sum of complete recovery, partial recovery and slight improvement.
Meteorological data
According to the date and geographical location of SSNHL attacks, meteorological data on daily maximum and minimum temperature, daily mean temperature and its day-to-day change, diurnal temperature range, atmospheric pressure, mean and maximum wind speed and relative humidity were obtained from the National Climatic Data Center (http://www.ncdc.noaa.gov/). Seasons were defined as spring (1 March–31 May), summer (1 June–31 August), autumn (1 September–30 November) and winter (1 December–28/29 February).
Statistical analysis
Categorical variables are presented as frequencies and percentages, and continuous variables are presented as mean±SD. Meteorological factors were compared between the different audiogram patterns using one-way analysis of variance with the Scheffé post hoc test. Comparisons of clinical characteristics and recovery rate between the profound and non-profound groups were performed using unpaired t-test and the Pearson Χ2 test or Fisher’s exact test, as appropriate. Effective sizes and 95% CIs were presented to describe the magnitude of the differences between the groups. The level of statistical significance was set at a two-tailed p value of <0.05. All statistical analyses were performed using SPSS software (V.24.0) and GraphPad Prism software V.7.0.
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, conduct, reporting or dissemination plans of our research.
Results
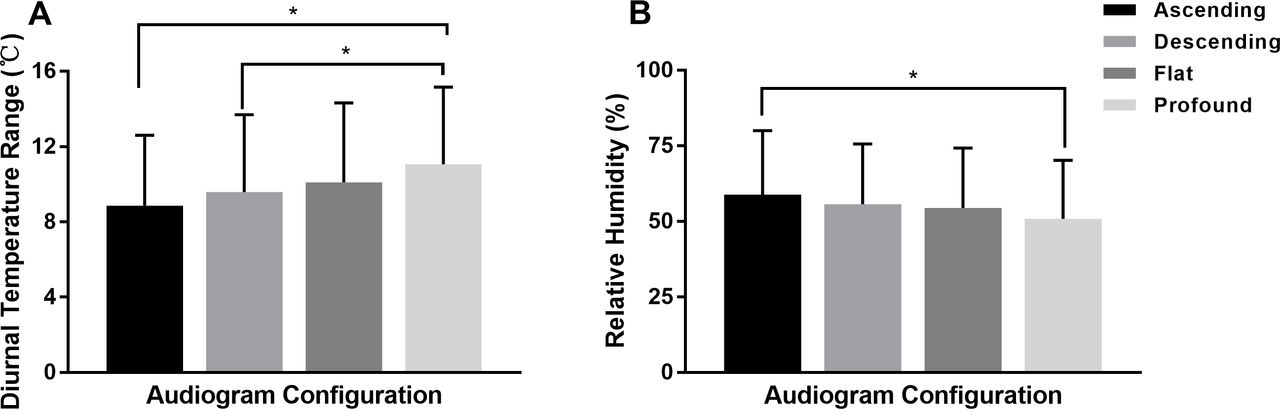
Among the 510 patients (259 women (50.8%); mean (SD) age, 46.4 (15.5) years) who met the inclusion criteria, 108 (21.2%) displayed ascending audiogram patterns, 143 (28.0%) displayed descending patterns, 129 (25.3%) displayed flat patterns and 130 (25.5%) displayed profound patterns. Each meteorological factor on the day of SSNHL onset was analysed. Only the diurnal temperature range and relative humidity showed significant correlations with specific audiogram configurations (table 1). The average diurnal temperature range on the day of SSNHL onset in patients with profound patterns was significantly higher than that in patients with ascending (mean difference (MD), 2.2°C; 95% CI, 0.7°C to 3.7°C; p=0.001) and descending (MD, 1.5°C; 95% CI, 0.1°C to 2.9°C; p=0.031) patterns. The diurnal temperature range on the day of SSNHL onset was higher in patients with profound patterns than in those with flat patterns, but the difference was not statistically significant (figure 1A). The relative humidity was the highest on the day of SSNHL onset in patients with ascending patterns and showed a significant difference compared with that in patients with profound patterns (MD, 8.0%; 95% CI, 0.7% to 15.3%; p=0.026; figure 1B). In addition, there was no significant difference in seasonal distribution among the four pattern groups (table 1).

{kind=link}
(A) Comparison of the diurnal temperature range between different audiogram configurations. (B) Comparison of relative humidity between different audiogram configurations.
Comparison of meteorological factors and seasonal distribution between different audiogram configurations
The percentage of patients aged >60 years (MD, 19.6%; 95% CI, 10.5% to 29.2%; p=0.000), those with vertigo (MD, 28.0%; 95% CI, 18.1% to 37.3%; p=0.0.000), those with diabetes (MD, 8.7%; 95% CI, 1.6% to 17.1%; p=0.014), those with stroke (MD, 3.9%; 95% CI, 0.2% to 9.7%; p=0.047) and those with coronary artery disease (MD, 7.3%; 95% CI, 2.3% to 14.1%; p=0.002) was significantly higher in the group with profound patterns than in the other groups. The mean prothrombin time (MD, −0.6 s; 95% CI, −1.2 to −0.1 s; p=0.006) was significantly shorter and the mean concentration of fibrinogen (MD, 19.5 mg/dL; 95% CI, 1.8 to 40.8 mg/dL; p=0.008) was significantly higher in the group with profound patterns than in the other groups (table 2).
Clinical characteristics of patients with profound and non-profound patterns
Response to treatment in 373 patients who underwent pure-tone audiometry on the 14th day after therapy was measured. The overall recovery rate was significantly lower in the group with profound patterns than in other groups (MD, −11.8%; 95% CI, −21.9% to −1.1%; p=0.031; table 3).
Response to treatment in patients with profound and non-profound patterns
Discussion
Weather conditions have long been recognised as an important factor in the deterioration of physical health since the time of Hippocrates (approximately 400 BC).13 Many studies have evaluated the association between SSNHL and weather and seasons. Mees et al14 found that the incidence of SSNHL was significantly affected by atmospheric pressure. Herbert et al15 also reported that the disease occurred more often at times of low pressure. Two retrospective studies from Korea demonstrated that the mean and maximum wind speeds were significantly and positively correlated with SSNHL onset.16 17 Concerning the seasonality of SSNHL, the results varied largely across studies.17–19 However, some studies have failed to establish a correlation between meteorological factors and the incidence20–22 and recovery rate of SSNHL.23 These studies mainly focused on the incidence and prognosis of SSNHL. Moreover, there are limited data on the relationship between the audiogram configurations of SSNHL and meteorological factors. This study showed that profound patterns were correlated with a high diurnal temperature range, while ascending patterns were correlated with high relative humidity. The study results did not indicate any correlation between seasons and audiogram configurations.
The positive association between profound patterns and the diurnal temperature range suggests that vascular factors may play a role in this subtype of SSNHL. The correlation between SSNHL and vascular disease is described in various studies. A prospective study by Lin et al24 reported that the risk of stroke within 5 years was 1.64 times higher in patients with SSNHL compared with those without SSNHL. In another 5-year follow-up study, Kuo et al25 collected data from 11 115 patients with stroke and 33 345 matched patients without stroke and reported that the incidence of SSNHL was approximately twice as high among patients with stroke than among those without stroke. In a previous study, the rapid change in ambient temperature had an effect on the overall stroke risk, and the effect was more immediate on ischaemic stroke than on intracerebral haemorrhage and subarachnoid haemorrhage.9 The change in temperature was also observed to be associated with an increased risk of overall and non-ST-elevation myocardial infarction.8 The effects of temperature change on SSNHL with a profound pattern and vascular-related diseases were similar. This similarity provides complementary evidence supporting that sudden hearing loss with a profound pattern is most likely of vascular origin, and the change in temperature may serve as a triggering factor for the interruption of microcirculation in the inner ear. When the temperature change overwhelms the adaptive capacity of the body, the sympathetic nervous system and renin–angiotensin system are activated, thereby resulting in vasoconstriction of the inner ear, accompanied by hyperviscosity, and leading to thromboembolism in some cases.
In addition, to vascular factors, the association between recent viral infection and SSNHL is established in a study.26 The seasonal pattern of viral infection is usually the result of its transmission under favourable meteorological conditions. Therefore, the virus-inducing SSNHL theory cannot be ruled out. Recent studies have reported that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a possible trigger of SSNHL. SARS-CoV-2 infection can promote microthrombosis in the inner ear by endotheliitis and cytokine activation.27
In addition, endolymph hydrops may be involved in the pathophysiology of SSNHL with an ascending pattern. The audiogram configurations mimic those observed in Ménière’s disease. Schmidt et al reported that high humidity was strongly associated with a higher prevalence of initial attack and symptom exacerbation in Ménière’s disease.28 In this study, the relative humidity was significantly higher on the day of onset in patients with ascending patterns. These findings further support the fact that SSNHL with an ascending pattern and Ménière’s disease have a shared pathophysiology of endolymphatic hydrops.
This study also found that the risk factors of vascular-related diseases overlap with the characteristics of patients with profound patterns, including older age; presence of vertigo; and history of diabetes mellitus, stroke and coronary artery disease. Moreover, a shorter prothrombin time and higher concentration of fibrinogen were observed in the group with profound patterns, which is associated with higher coagulation activity and blood viscosity.29 These results reinforce the presence of an underlying vascular problem in patients with SSNHL with profound patterns. SSNHL with a profound pattern can be disabling and has a considerable negative impact on the patient’s quality of life. In this study, the recovery rate in the group with profound patterns was significantly lower than that in the other groups; therefore, there is a demand for an optimised treatment strategy. Given that vascular compromise may be the aetiology of SSNHL with a profound pattern, vasoactive and rheologic agents may be effective in the management of this particular group rather than of overall SSNHL. Some treatments based on vascular theory, such as fibrinogen/low-density lipoprotein apheresis29 and local hypothermia,30 have been tested and have shown positive results. Further clinical trials are required to provide higher quality evidence.
This study has several limitations. First, as a retrospective study, data on onset time were primarily extracted from the medical records, which is based on the patients’ self-report and may have introduced a recall bias. This study attempted to mitigate this limitation by including only those patients who were diagnosed with SSNHL within 14 days after SSNHL onset. Second, this study was conducted at only one hospital; therefore, more extensive multicentre studies are required.
Conclusion
The diurnal temperature range and relative humidity were associated with the audiogram configuration of SSNHL. A high diurnal temperature range on the day of SSNHL onset correlated with profound patterns, while high relative humidity on the day of SSNHL onset correlated with ascending patterns. However, there was no correlation between seasons and audiogram configurations.
Data availability statement
Data are available upon reasonable request. The meteorological data are available on the website of National Climatic Data Center (http://www.ncdc.noaa.gov/). Data of the enrolled patients will be shared by request from any qualified investigator.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board of Peking University People’s Hospital (reference number 2020PHB105-01).
References
Footnotes
Contributors JZ was tha guarantor and had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: YJ, LY and JZ. Acquisition, analysis or interpretation of the data: All authors. Drafting of the manuscript: JZ. Critical revision of the manuscript for important intellectual content: YJ, LY and XM. Statistical analysis: JZ and SJ.
Funding This work was supported by Capital’s Funds for Health Improvement and Research grant number 2020-2-4083.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.