Article Text

Abstract
Introduction The first years of school are critical in establishing a foundation for positive long-term academic, social and well-being outcomes. Mindfulness-based interventions may help students transition well into school, but few robust studies have been conducted in this age group. We aim to determine whether compared with controls, children who receive a mindfulness intervention within the first years of primary school have better: (1) immediate attention/short-term memory at 18 months post-randomisation (primary outcome); (2) inhibition, working memory and cognitive flexibility at 18 months post-randomisation; (3) socio-emotional well-being, emotion-regulation and mental health-related behaviours at 6 and 18 months post-randomisation; (4) sustained changes in teacher practice and classroom interactions at 18 months post-randomisation. Furthermore, we aim to determine whether the implementation predicts the efficacy of the intervention, and the cost effectiveness relative to outcomes.
Methods and analysis This cluster randomised controlled trial will be conducted in 22 primary schools in disadvantaged areas of Melbourne, Australia. 826 students in the first year of primary school will be recruited to detect between groups differences of Cohen’s d=0.25 at the 18-month follow-up. Parent, teacher and child-assessment measures of child attention, emotion-regulation, executive functioning, socio-emotional well-being, mental health-related behaviour and learning, parent mental well-being, teacher well-being will be collected 6 and 18 months post-randomisation. Implementation factors will be measured throughout the study. Intention-to-treat analyses, accounting for clustering within schools and classes, will adopt a two-level random effects linear regression model to examine outcomes for the intervention versus control students. Unadjusted and analyses adjusted for baseline scores, baseline age, gender and family socioeconomic status will be conducted.
Ethics and dissemination Ethics approval has been received by the Human Research Ethics Committee at the University of Melbourne. Findings will be reported in peer-review publications, national and international conference presentations and research snapshots directly provided to participating schools and families.
Pre-Results Trial registration number Australian New Zealand Clinical Trials Registry (ACTRN12619000326190).
- community child health
- child & adolescent psychiatry
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations
Provide the first efficacy trial findings for a whole-class mindfulness intervention delivered across the first 2 years of primary school, with embedded process and economic evaluations.
Large population-based sample, specifically targeting schools in disadvantage areas of Melbourne, Australia.
Use of multi-informant and blinded outcome measures consisting of child, parent and teacher-reported measures across multiple domains proposed to change through a mindfulness intervention.
Unable to determine potential biological benefits (ie, reduced stressed related cortisol) of the intervention.
Introduction
The first years of school are critical for establishing firm foundations for positive child social, psychological and academic development.1–3 Childrens’ ability to regulate their attention, emotions and behaviour, and to follow classroom instructions during this period predicts school adjustment, participation and success.3–6 Similar to other countries,7 8 data from the Australian Early Development Census (AEDC) found that 22.4% of children commence school developmentally vulnerable. These vulnerabilities are highest in regards to (commonly relate to) behavioural and emotional difficulties, with children in disadvantaged areas three times more likely to experience these difficulties.9 Children who transition poorly into school are at increased risk for a host of detrimental outcomes, including behavioural and emotional problems, poor peer and teacher relationships and low academic performance. These difficulties can persist throughout their schooling years,2–4 10 and impact on long-term educational, economic, social, physical and mental health outcomes.11 12 Thus, identifying evidence-based approaches to help children develop attention and emotional regulation skills is critical in proactively supporting children’s mental health and academic performance.
Contemplative practices such as mindfulness, and other contemplative practices, have rapidly gained popularity in both practice and research and have potential to be used in classrooms to help children transition to school and to support ongoing learning.13–15 Mindfulness is broadly defined as the awareness that arises from paying purposeful attention to the present moment, non-judgmentally, with acceptance or curiosity.16 17 Numerous mindfulness-based programmes have been developed for children and adults to build attention, self-monitoring, self-regulation and mental flexibility.13 14 18–20 Such programmes propose that individuals can become more ‘mindful’ by learning and practicing mindful skills and activities.
The interest in mindfulness-based interventions has been matched with studies, reviews and meta-analyses examining the effectiveness of these interventions.13 14 21–25 Studies find that interventions can have positive effects on attention, executive functioning, social behaviour and mindfulness in children and adults. However, reviews have also raised numerous concerns.13 14 25 26 Comparison groups are often weak or non-existent, selective samples are used, measures rely predominantly on self-report, methods are inconsistent (making it difficult to directly compare study effects), and programmes are often poorly defined and vary in their components, resulting in programmes that are often quite different. Only a limited number of rigorous randomised control trials (RCTs) have examined the impact of mindfulness interventions using objective outcome measures assessed over time. Further, systematic reviews have identified very few studies that have been conducted with children under 8 years,13 14 and to our knowledge, no large-scale rigorous studies exist at the early primary school level.
Even for the school-based interventions with stronger evidence, it is unknown whether their effectiveness can be maintained when implemented at large scale. Many mindfulness programmes involve the use of electronic/smart devices (eg, audio recorded instructions), which the teacher is expected to facilitate/lead, and children are expected to engage in. Little emphasis is given to equipping teachers with the theoretical and practical knowledge underlying the activities, or on providing strategies for incorporating mindfulness into their day-to-day teaching practices. Yet teacher pedagogy and student–teacher relationships are critical for learning.27 For example, a recent mindfulness intervention study following children from preschool to school suggested that observed executive functioning and later vocabulary and literacy benefits only emerged when teachers embedded these skills within their usual classroom practices over a long period of time, well beyond the standard 8–12-week period of most mindfulness interventions.28
Given the complexity of implementing interventions in schools,29 it is also important to understand the quality, fidelity and dosage of the mindfulness intervention that children are exposed to, especially when promising interventions are implemented at scale.30–32 When mindfulness programmes are poorly implemented or taught without appropriate theoretical and practical training, a range of unintended and adverse consequences can occur.15 Further, it is critical to determine the financial and time costs required to achieve positive outcomes, to ensure that the limited time and resources that schools have available are well spent. There are clear gaps between the levels of interest, evidence and investment in mindfulness-based interventions and best practices for doing so. Addressing these gaps will have both national and international implications for the use of mindfulness intervention within early primary school classrooms.
Addressing the lack of empirically based mindfulness programmes for early years education, the intervention used in this study directly trains teachers on mindfulness theory and practice and provides a structured approach for embedding mindfulness activities into everyday teaching practices to improve student outcomes. Initial support for the intervention was established through a pilot RCT involving 109 children from six classrooms in four preschool centres in disadvantaged areas of Melbourne, Australia. Preliminary data at immediate postintervention, indicated intervention children had better immediate attention/short-term memory (measured via the Corsi Block Tapping Task, effect size Cohen’s d=0.29; Digit Span Forward Task, d=0.24), behaviour regulation (measured via less is more, d=0.34) and mental health-related behaviours (measured via the Teacher Strengths and Difficulties Questionnaire—externalising, d=0.45), compared with control children. Qualitative data demonstrated that teachers believed that the programme was effective for themselves, their children and their colleagues, and reported parents wanted to know more about the programme and the activities. They also continued to embed mindfulness into their classroom after the programme finished.
The current study uses a rigorous RCT cluster design to build on these promising findings to examine whether the same intervention remains effective when implemented within early primary school classrooms at larger scale. We will provide an in-depth examination of child, teacher and school level factors that promote and reduce the intervention’s success. We will also consider the costs and economic benefits of the intervention. We hypothesise that the intervention will be associated with:
Improvements in child immediate attention/short-term memory assessed via blinded direct assessment 18 months post-randomisation (primary outcome).
Improvements in executive functioning measured via blinded direct assessment of inhibition, working memory and cognitive flexibility, 18 months post-randomisation.
Improved socio-emotional well-being, emotion-regulation and mental health-related behaviours, reported by parents and teachers, 6 and 18 months post-randomisation.
Sustained changes in teacher practice and classroom interactions assessed via blinded observations at 18 months post-randomisation.
Furthermore, we hypothesise that the quality and dosage of implementation will predict the efficacy of the intervention, and the intervention will be cost effective relative to outcomes.
Methods
Pre-registration
The study is registered with the Australian New Zealand Clinical Trials Registry.
Patient and public involvement
No patient involved.
Design
This is a cluster RCT with an embedded process and economic evaluation (see figure 1). This will inform the benefits of the intervention compared with current practice, identify for whom and under what conditions the intervention is beneficial, and provide an indication of the cost-benefits of the intervention. Results will be reported per the Consolidated Standards of Reporting Trials guidelines for non-pharmacological interventions.33

Graphical representation of key study components.
Participants
All foundation children (ie, the first year of primary school, ages 5–6) at participating schools with parental consent will be invited to participate in the data collection, provided the child and parents have sufficient English language abilities to complete the measures. Although this will affect generalisability, most measures have not been validated for other languages. Children without consent will still be exposed to the intervention as part of their school’s well-being approach but not complete the measures.
Sample size
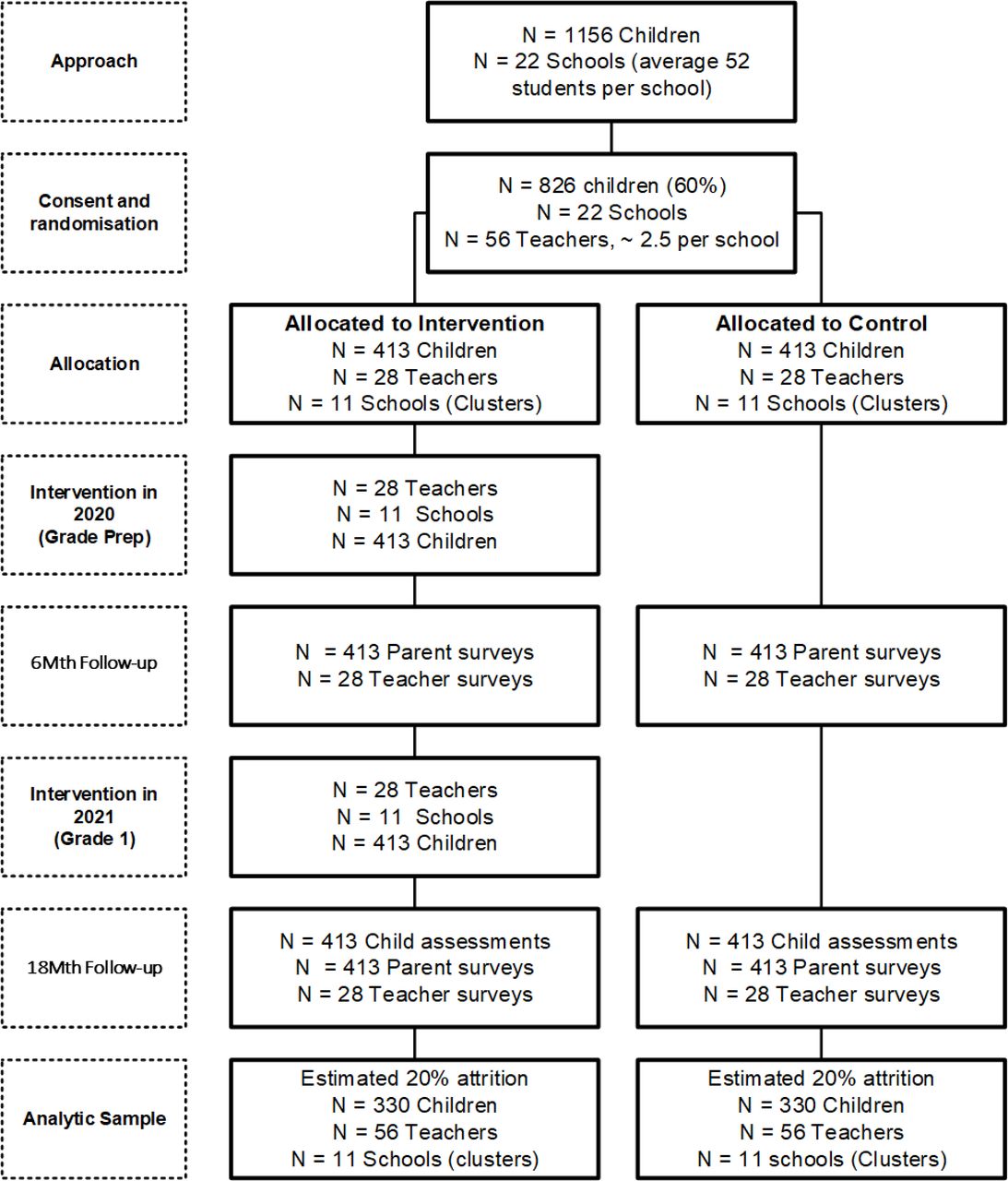
The estimated sample size across all stages of the study are shown in figure 2.

{kind=link}
{kind=link}
Consolidated Standards of Reporting Trials participant flow chart—estimated numbers.
Given the hypotheses of the trial and measures collected in our pilot study as well as in published meta-analyses,13 14 we anchored our sample size calculations on detection of a minimum effect size of 0.25 SD between the treatment and control groups at 18 months post-randomisation in a two-arm parallel trial with 80% power and a two-tailed 5% type I error. The sample size applies across all measures collected at 18 months post-randomisation, based on the number of SDs rather than on the actual outcome distributions.
To account for the clustering effect within classes (Intracluster Correlation Coefficient=0.02) and schools (ICC=0.02), and an attrition rate of 20% by the end of the study, our planned sample size is 413 children per condition (826 total). To achieve this, we estimate we will recruit 22 schools to participate (11 per condition). This assumes an average of 2.5 foundation year classes at each school, and 65% of parents providing consent for data collection (16 per class, 40 per school). The final number of schools will be dependent on student population, the number of classes within each school and class size of the recruited schools.
School selection and recruitment
Primary schools from metropolitan Melbourne, Australia, with disadvantaged student populations will be recruited. This will be determined by approaching schools with a high proportion of children starting primary school developmentally vulnerable in ‘emotional maturity’ and ‘social competence’ domains as defined by the AEDC. The AEDC is a national census completed every 3 years by classroom teachers for children in the first year of primary school, including 2015 and 2018.34 Data are available for >98% of Australian children during data collection years. Therefore, the AECD provides accurate estimates of the number of children with developmental vulnerabilities for/at each school. Where AEDC data are not available, other government or administrative datasets that measure school disadvantage will be used to select eligible schools.
The school recruitment approach is similar to those used in previous school-based longitudinal studies and intervention trials conducted by members of the research team.35–39 Australian schools are clustered into three sectors: government (69%), Catholic (19.2%) and independent (11.8%). To balance representation with study time and resources, we will include government and Catholic schools.
Although Department of Education and Training (DET) and Catholic Education Melbourne (CEM) have provided approval for research within schools, each school’s leadership has independent responsibility to approve which projects they choose their schools to participate in. Drawing on the DET and CEM network of schools, we will first present our study at each area’s school leadership network meetings or similar engagement event, providing background on the study and an overview of what would be expected of the school, teachers, parents and children. Principals will be able to indicate interest in participating in the study without fully committing. By doing this, we limit the burden of approaching schools in which school leadership do not wish to participate. If an enough schools’ express interest, we will proceed with selection and randomisation. Based on our prior experiences working with primary schools in the region, we estimate that 87 (75%) will express interest in being a part of the study, with the main reason for declining being time commitments and participation in other research projects. If additional schools are needed, we will directly contact remaining schools in the area until the number of required schools has been achieved.
Recruitment will be stratified by school sector type to ensure a representative sample from both sectors. Of those selected, we will approach the school’s principal to ascertain their consent to participate (see online supplementary file 1). If the principal declines, we will contact the next randomly selected school on the list, repeating until we reach the required sample size.
Supplemental material
We will then meet with all foundation and grade 1 teachers at participating schools to describe the purpose and requirements of the project, expected time commitments, and recruitment process and answer any questions they may have. The teachers will be provided with an information sheet detailing their expected involvement, a consent form (see online supplementary file 2) and a brief survey.
Supplemental material
Student recruitment and consent
Before we begin student recruitment at each school, we will work with each school to publicise the trial, raising parental awareness and interest in the study through notifications in school newsletters, posters on classroom doors and sending advance-notice postcards to the homes of eligible children. Teachers will then send a recruitment pack to each family. The pack will contain an information sheet detailing the study, a consent form (see online supplementary file 3), a brief survey and an envelope. Parents will be asked to return the completed consent forms and survey in the sealed envelope to a secure box in the child’s classroom.
Supplemental material
Consent for the study will be specific to the data collection. Because the intervention focuses on embedding simple play-based activities into teachers’ daily practice and classrooms, it would be unethical and impractical to have children without consent be removed from the classroom, when teachers are implementing the mindfulness-based activities and games. Children are commonly/frequently exposed to similar changes in teacher practice following teacher professional development (PD) or when teachers make explicit decisions to implement a new pedagogical approach or well-being curriculum in their classroom.
Randomisation
After the parent and teacher surveys have been completed, schools, stratified by school sector, will be randomised to control or intervention in block sizes ranging from two to four. To reduce the potential for contamination effects, the randomisation will be conducted by a researcher independent of the study team, and group allocation will be concealed from research team members involved in the direct outcome assessments. All intervention schools will complete a memorandum of understanding, agreeing not to share the intervention resources with control schools, and control schools will not have access to the intervention training or manual.
Mindfulness intervention
Training and troubleshooting support for the mindfulness intervention will be provided by the programme developer. Children will be exposed to the intervention across two consecutive academic school years, foundation and grade 1.
For intervention schools, foundation and grade 1 teachers will attend one PD day in 2020 and 2021, respectively, which will provide the theoretical and practical foundations of the programme and instructions for implementing the programme.40 Teachers will be provided with an implementation manual (available by request), which includes a schedule of activities, lesson plans, communication templates/examples, sample activities, parent homework sheets, audio/music and film suggestions and training slides. Participants will review the materials, watch examples, practice a selection of activities, and will be able to ask questions to ensure clear understanding of the programme and implementation.
Following the PD, the teachers will be expected to embed the 12-week intervention into their classrooms, using the manual to help them to learn, practice, incorporate and reflect on the activities and strategies. The mindfulness programme involves three core practice components: (1) mindful games/activities; (2) mindful routines/transitions/moments; (3) use of props/books/music/art, which can be used within the classroom and integrated with normal teaching activities. For each week, it is recommended that teachers:
Engage in two mindfulness activities per day at least four times per week, using suggested props, games or art/music and trying to anchor these around key routines or transition periods during the day (eg, on classroom arrival/departure, after lunch/recess, before a test/specialist class, snack or mealtimes, moving between classrooms).
Read suggested storybooks each week and discuss with children possible connections to mindfulness and related skills/concepts. The manual includes a list of popular children’s storybooks (commonly available in schools or easily accessed) with guidance for discussion.
Identify and embed spontaneous ‘mindful moments’ into their daily classroom routines, transitions and class time, such as using ‘slow motion’ walking to the library, or watching rain drops race down classroom window.
Teachers will also be asked to establish, if possible, a ‘mindful space’ in the classroom to provide an ongoing reminder and/or display of mindfulness tools, while also creating a place for children to engage in mindful activities during class time. The space may include a variety of mindful props (eg, mind jar), games (eg, rock balancing), activities (eg, mindful drawing) and storybooks. Intervention schools will be provided with all required props, books, games and other resources (eg, door/wall posters) to implement the key elements of the programme.
Throughout the 12-week programme, teachers will also be encouraged to:
Discuss the intervention’s implementation during their team’s regular meetings, led by participating teachers, to reflect on the intervention’s progress, implementation and support needs, providing peer support and a shared commitment to the programme. In year 2 of the study, foundation teachers will continue to participate in these meetings, providing their own reflections and experiences to the grade 1 teachers, potentially aiding sustainability through a train-the-trainer type approach.
Contact the research team for additional implementation support, trouble shooting, or advice/coaching, if required.
Share examples of mindful activities, artwork and discussions with parents, enabling connections and modelling between school, home and ongoing support.
Following the 12-week intervention, we will conduct a 1-hour meeting with teachers to allow reflection on learnings from the past 12 weeks and to help develop an ongoing implementation plan if they chose.
Outcome data collection and research assistant blinding
Outcome assessments will be conducted 6 (end of foundation for the children) and 18 months (end of grade 1) post-randomisation. At each occasion, parents and teachers will be asked to complete surveys. Children will complete face-to-face direct assessments at baseline and 18 months post-randomisation during school hours by trained research assistants blinded to the school’s group allocation.
Measures
Measures are summarised in table 1, which have chosen to attempt to measure proximal and distal outcomes that align with our intervention’s theory of change, which have been informed by our pilot findings and existing systematic reviews.13 14 17
Description of measures and timepoints
The primary outcome is labelled as child visuo-spatial short-term memory, as measured by the Corsi Block Tapping Forward Raw Score at 18 months post-randomisation.41 We have referred to this as short-term memory, however, previous psychological and cognitive sciences research have also used forward block span as a measure of immediate attention (the same applies for Digit Span Forwards and verbal short-term memory), with such terms often used somewhat interchangeably. Other research highlights difficulties in separating short-term memory and immediate attention conceptually and experimentally, hence they strongly overlap.42 43
The study includes secondary outcomes across multiple domains. Examining multiple outcomes aligns with the UK Medical Research Council guidelines for interventions that are complex in nature and likely to result in possible impact across a diversity of domains.44 It is particularly important that sufficient data are measured to enable comparability across mindfulness-based school programmes, as programmes frequently vary in their content, setting and target population. Because of the wide variety of measures, while each outcome will be analysed individually, findings and interpretations will consider the consensus of evidence for the data provided. This will involve careful examination and consideration of the magnitude, direction and statistical significance of the responsiveness estimated for each outcome. Due to the increased potential for false-positive findings arising through analysis of multiple outcomes, patterns will be interpreted cautiously and in context with one another, rather than in isolation.
Process evaluation
The implementation and process evaluation will use a mixed-methods approach, drawing on data collected via teacher surveys and teacher interviews. It will explore the intervention’s theory of change and the extent to which the dimensions of implementation impact the programme’s effectiveness, as well as the enablers and barriers to its implementation.29 Fidelity, quality and adaptation of the intervention’s activities over the 12-week manualised implementation will be examined via fortnightly surveys completed by intervention teachers. Sustainability, enablers and barriers of the intervention will be examined via teacher interviews and surveys at 6 and 18 months post-randomisation. Factors will be examined at the student, teacher and school levels where appropriate.
The well-being practices of the control schools will also be examined to document any practice similarities (ie, the presence of mindfulness practices/elements or other social-emotional learning (SEL) programmes) and differences (eg, the use of mindfulness audio-recorded sessions vs pedagogy-based approaches) when compared with our intervention.
Economic evaluation
Costs associated with the intervention training and delivery will be prospectively and retrospectively recorded, including costs for delivery, material/prop resources required by the schools, and time spent on the programme. Resources used in training and ongoing support will be prospectively recorded by the research team, and all intervention teachers will prospectively record time and resources used in intervention delivery and report these through the process evaluation. Teacher surveys will include retrospective report from control teachers of time and resources used on SEL related activities.
Using surveys, teachers in intervention and control schools will retrospectively report in-school additional support at 3 and 18 months post-randomisation, and at each time point parents will recall out-of-school health and education service use over the previous year.
Resource use will be presented in natural units as well as valued in 2021 Australian dollars using local (state) and national unit cost estimates (eg, education department salary scales, Medicare Benefits Schedule).45 Costs will be presented as costs per student from a government payer perspective.
Analyses will involve: (1) a cost-consequences analysis, which will compare incremental costs of the intervention (costs accrued in the intervention arm, from intervention and resource use over the period of follow-up, compared with costs accrued in the control arm) to all primary and secondary outcomes, expressed in their natural units of measurement; (2) cost-effectiveness, assessed against the primary outcome measure and presented as cost per point change in child attention. Impact of missing data will be assessed through multiple imputation (described below).
Statistical analysis
All participants and school demographic and baseline continuous outcomes will be presented as mean and SD (or medians and IQRs for skewed data), while categorical outcomes will be presented as absolute and relative frequencies by group. Statistical analysis will follow standard methods for cluster randomised trials and the primary analysis will be by intention to treat. Multiple imputation will be conducted separately in the two arms using chained equations applied to all outcomes simultaneously, including baseline measures as auxiliary variables. Fifty imputed datasets will be generated. All analyses will be conducted using Stata 15 or later.
The primary outcome is student visual-spatial short-term memory/immediate attention at 18 months post-randomisation. The effect of the intervention on the Corsi Block Tapping Forward raw score at 18 months compared with control children will be examined adopting a linear mixed model, which will include the stratification factor used during randomisation (school sector) as a fixed effect term and two random effect terms (school and class) to account for the clustering structure of the data. The effect of intervention on the primary outcome at 18 months will then be adjusted by the student baseline Corsi Block Tapping Forward score, age at baseline, gender, family socioeconomic status and child intelligence quotient (IQ), which will be included in the above model as fixed effect terms.
For all the outcomes collected at 18 months, the effect of the intervention will be estimated using generalised linear mixed models (linear or logistic according to the nature of the outcome), which will include control variables (ie, school sector, the corresponding outcome measure at baseline, age at baseline, gender, family socioeconomic status, child IQ and time of assessment) as fixed effect terms and the same random effect terms mentioned above. For outcomes collected at 6 months and at 18 months, the same generalised linear mixed models described above will be adopted, with the addition of a third random effect term (ie, student), to account for the repeated measures over time (the nature of the outcome), which will include control variables as fixed effect terms and the same random effect terms mentioned above with the addition of a third random effect term (ie, student), to account for the repeated measures within children.
Ethics and dissemination
Ethics approval was obtained from the Human Research Ethics Committee at the University of Melbourne (Ethics ID: 1853492), Australia, and approval for the study was provided by the Victorian Department of Education and Training and Catholic Education Melbourne. Active written consent will be provided by each child’s parent/caregiver, while all participating teachers will provide active written consent.
Once the study is completed, we will publish our findings in international peer-reviewed child health journals and present at national and international conferences. In addition, we will send participating schools and parents a short report of our findings. A copy of the report will also be sent to relevant government departments.
Annual school and parent newsletter: to maintain engagement throughout the study, we will send annual newsletters to all participating schools and families that will provide a progress update, and summary of any new findings which have been published.
A participating school seminar: recognising the time and resource contributed by participating schools, it is important findings are presented to schools in a timely manner. We will hold, and record, a half-day seminar at the primary institution within 6 months of the study’s completion to present findings and enable dialogue about implications.
References
Footnotes
Contributors All authors are investigators on the successful funding grant for this project, with JQL as the lead investigator. All authors have reviewed and approved this submitted version. JLQ was involved in the study’s design as well as the drafting and finalising of the study protocol. They will have overall responsibility for the study’s conduct. BD was involved in the study’s design as well as the drafting and finalising of the study protocol. They also designed the intervention. PK was involved in the study’s design as well as the drafting and finalising of the study protocol. JC was involved in the study’s design as well as the drafting and finalising of the study protocol. LG was involved in the study’s design as well as the drafting and finalising of the study protocol. FO was involved in the study’s design as well as the drafting and finalising of the study protocol. ES was involved in the study’s design as well as the drafting and finalising of the study protocol.
Funding This study is funded by an Australian Research Council Discovery Award (DP190100504). Associate Professor Sciberras is funded via a National Health Medical Research Council Career Development Fellowship (GNT1110688).
Competing interests BD developed the intervention but does not receive any commercial or non-commercial financial entitlements.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.