Article Text

Abstract
Introduction In the UK, over 7000 amputations are performed each year because of diabetes. Up to 80% of these are preceded by a foot ulcer and could therefore be prevented with improvements in ulcer care. Peripheral arterial disease is an important risk factor for the development of diabetic foot ulceration. However, its diagnosis in diabetes is challenging due to the presence of neuropathy and arterial calcification. Commonly used bedside tests either have low sensitivities or little supporting evidence to justify their use. Duplex ultrasound (DUS) has good correlation to angiography findings but a full scan is difficult to learn and time consuming to perform. We have previously demonstrated that a focused DUS of the distal anterior and posterior tibial arteries at the ankle (podiatry ankle duplex scan (PAD-scan)) can be readily learnt by novices and performed rapidly and accurately. The primary aim of this study is to determine the diagnostic accuracy of the PAD-scan and other commonly used bedside tests in detecting arterial disease in diabetes.
Methods and analysis The study will include 305 patients presenting to diabetic foot clinics at two centres. Arterial assessment will be performed using the following index tests: the PAD-scan, pulse palpation, audible handheld Doppler, Ankle Brachial Pressure Index, Toe Brachial Pressure Index and transcutaneous pressure of oxygen. Patients will then undergo a full lower limb arterial DUS by a blinded vascular scientist as a reference test.
Ethics and dissemination Approval was gained from NRES Committee London (REC reference 17/LO/1447). Findings will be disseminated by various methods including international presentations and publication in a peer-reviewed journal.
Trial registration number ClinicalTrials.gov Registry (NCT04058626).
- diabetic nephropathy & vascular disease
- vascular surgery
- diabetic foot
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Provides a direct ‘head-to-head’ diagnostic accuracy comparison for commonly used bedside tests and the novel focused point-of-care ultrasound scan (podiatry ankle duplex scan).
Includes ‘high risk’ diabetic patient population, in whom the detection of arterial disease is potentially most challenging.
Blinded reference standard.
Appropriately statistically powered.
One potential limitation of this work is that it focuses on a population with advanced disease and a high prevalence of peripheral arterial disease. However, these are also the most challenging group of patients to diagnose and where evidence is most lacking.
Introduction
Diabetic foot complications that affect up to 25% of people with diabetes at some point in their life are associated with high rates of amputation and mortality.1 2 Ulcers are also challenging to manage, necessitating intensive treatment which costs the National Health Service (NHS) an estimated £1 billion per year.3 However, it has been suggested that up to 80% of diabetic amputations are preventable4 and that meaningful impact can still be made.
Neuropathy and peripheral arterial disease (PAD) are the most important risk factors for the development of foot ulceration.5 With rising prevalence of PAD in western populations, there has been a shift of pattern from neuropathic to ‘neuroischaemic’ ulceration.6–8 The prompt and accurate detection of PAD in the ulcerated foot is time critical as time to revascularisation is a determinant of ulcer healing and limb salvage.9 10 This serves as an important target for improving ulcer care due to the confounding effects of neuropathy and arterial calcification, the detection of PAD in diabetes is challenging. Symptoms, such as claudication and rest pain are often masked by the presence of neuropathy. Furthermore, physical examination and bedside screening tests such as Ankle Brachial Pressure Index (ABPI) are hindered by the presence of calcified, incompressible blood vessels. Limited evidence suggests that Toe Brachial Pressure Index (TBPI) and transcutaneous pressure of oxygen (TcPO2) may be superior to ABPI measurements.11–13 However, TBPI may also be influenced by the presence of digital artery calcification and TcPO2 can be time consuming to perform and may not be feasible in real world diabetic foot practice, reportedly used 6.2% and 0.8%, respectively.14 Interpretation of audible Doppler arterial signals using handheld Doppler devices is the most commonly used bedside test, but this is also limited by significant interobserver variation and poor sensitivity in detecting PAD.15 16 Currently, there is a scarcity of robust evidence to support the use of any one test.11
The limitations of current bedside tests highlight a need for a more accurate and reliable non-invasive screening tool for the detection of arterial disease. The lack of evidence highlights the need for a comparative diagnostic accuracy study to identify the best screening strategy.
Point-of-care arterial duplex ultrasound (DUS) may provide an alternative solution to diagnosis. A full lower limb arterial DUS scan has an accuracy comparable to the gold standard of angiography17 but is too time consuming to perform and technically challenging to learn due to the difficulty of scanning proximal tibial vessels,18 thus limiting its utility as a bedside test by front line staff. Focused scanning of the anterior and posterior tibial arteries at the ankle can provide information regarding the upstream state of the vasculature. We have given this focused DUS the acronym PAD-scan (podiatry ankle duplex scan). The PAD-scan allows for direct vessel visualisation and selective sampling of the Doppler signal from a region of interest to detect arterial disease (figures 1 and 2). This reduces the chance of mistakenly sampling collaterals and allows for more granular waveform analysis by sampling from a region of the vessel with low calcification. We have previously demonstrated that the PAD-scan can be readily learnt and accurately performed by front line staff.19

(A) Performing the PAD-scan in clinical practice (the persons depicted are not patients and the photo was taken with the participant’s knowledge and consent). (B) Schematic of PAD-scan, which involves scanning the distal anterior and posterior tibial arteries. PAD-scan, podiatry ankle duplex scan.
{kind=link}
{kind=link}
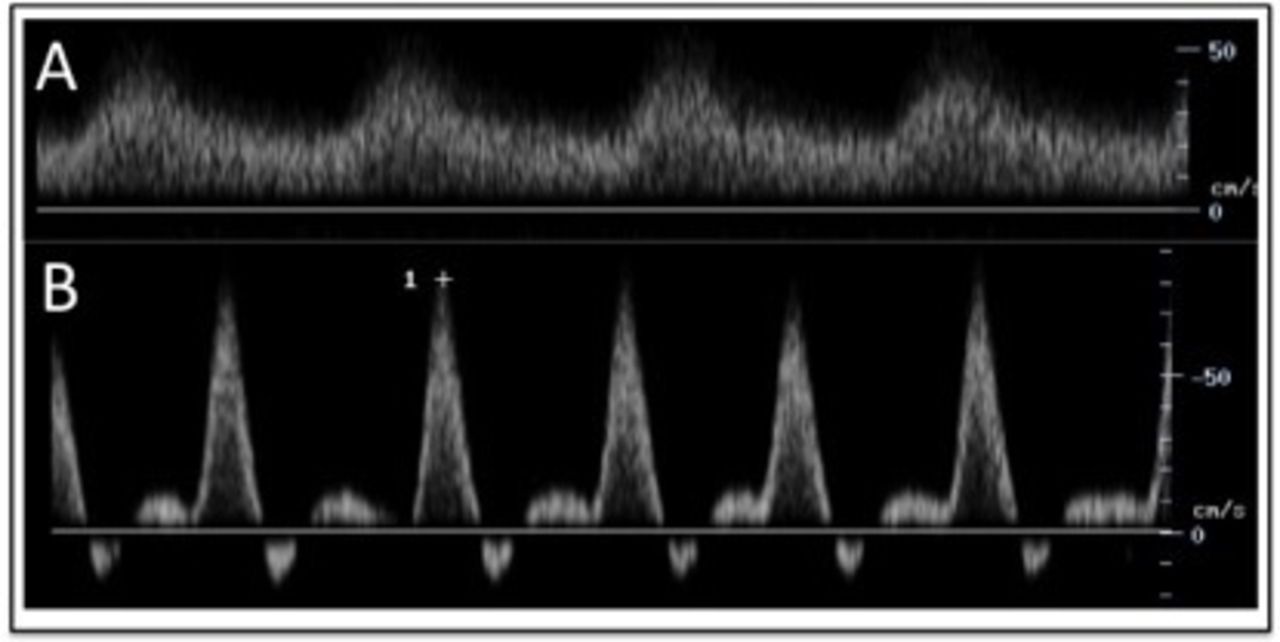
(A) An ‘abnormal’ monophasic arterial spectral waveform. (B) A ‘normal’ triphasic waveform.
The primary aim of this present study is to determine the ability of the PAD-scan, continuous handheld Doppler (audible and visual waveform assessment), ABPI, TBPI, TcPO2 and pulse palpation to discriminate between the presence and absence of PAD in diabetes, as compared with a reference standard of full lower limb arterial DUS.
The results of this study will improve the diagnosis of PAD in diabetes and inform referral pathways between primary and secondary care. Early detection, referral and management of PAD in the ulcerated foot will result in faster healing rates, reduction in hospital admissions, reduction in lower limb amputations and cost savings for the NHS. In the non-ulcerated foot, detection of PAD may alter foot care behaviours to reduce the risk of ulceration and allow for optimisation of best medical therapy to reduce overall cardiovascular risk.
Methods and analysis
Centre(s): St Mary’s Hospital (London, UK), West Middlesex University Hospital (London, UK).
Study status: This is an ongoing study that started recruiting on 4th March 2019.
Design
Inclusion and exclusion criteria
Diabetic patients aged over 18 years presenting to the diabetic foot clinics at our chosen centres will be eligible for the study. Patients with a known history of vascular imaging or intervention in the past 1 year will be excluded. Patients unable to provide informed consent will also be excluded.
Intervention(s) or method
Patient assessment
The clinical team responsible for care will perform a routine clinical assessment of each patient. Neuropathy will be tested for using a 10 g monofilament, 128 Hz tuning fork and proprioception at the first metatarsophalangeal joint. Assessment of ulcer size, depth and severity will be made using the validated University of Texas Score.20 21
Index tests
Pulse palpation and audible handheld continuous Doppler assessment will be performed by the podiatrist assessing the patient as part of their routine clinical assessment.
This present study focuses on diagnostic accuracy and not feasibility of frontline staff learning or performing the PAD-scan, which we have previously established. Therefore, two vascular scientists will perform all tests, one of the two will perform the index tests; PAD-scan, TcPO2, ABPI, TBPI and visual handheld continuous Doppler waveform assessment, the other will perform the reference full Duplex scan. Each scientist will be blinded to the findings of the other.
Pulse palpation
The dorsalis pedis (DPA) and posterior tibial artery (PTA) pulses will be palpated and classified as present or absent. Absence of either pulse will be considered diagnostic.
Continous handheld Doppler device (audible and visual waveform assessment)
The DPA and PTA will be interrogated using a continuous wave handheld Doppler device. The presence of a monophasic signal or the absence of a signal in either vessel will be considered diagnostic. Secondary analysis will also consider the inclusion of biphasic waveforms to the diagnostic criteria.
Ankle Brachial Pressure Index
A sphygmomanometer-cuff placed at the ankle and a handheld continuous wave Doppler device will be used to measure the systolic pressure of the DPA and PTA. The pressures of both arms will also be taken and the highest reading used to calculate the ABPI.22 ABPI of ≤0.9 will be considered diagnostic. Secondary analysis will consider the inclusion of ABPI>1.323 to the diagnostic criteria.
Podiatry ankle duplex scan
PAD-scan involves using an ultrasound machine to visualise the anterior and posterior tibial arteries at the ankle (figure 1), which supply the foot. Graphically displayed Doppler spectral waveforms are then assessed. PAD-scan is positive for the presence PAD in the presence of an occlusion, venous like slow flow, monophasic waveform, or a biphasic waveform with adverse features (slow rise time, spectral broadening, infilling of the spectral window and long forward flow in diastole) in either vessel scanned. All scans will be performed using the Mindray M7 (Shenzhen, China) Portable Ultrasound System with a linear 6–14 kHz transducer.
Toe Brachial Pressure Index
TBPI will be measured using the photoplethysmography method, employing an infrared sensor placed on the hallux and index finger. The highest upper limb reading will be used to calculate the TBPI. Values of <0.75 will be considered diagnostic for PAD.24
Transcutaneous pressure of oxygen
Prior to taking TcPO2 measurements, patients will be acclimatised for 20 min in the resting supine position with the room temperature maintained between 23°C and 25°C. Calibration will be performed and transducers placed on the skin after cleaning using double-sided adhesive rings and contact liquid.25 Measurements will be taken centrally (at the sternum or the deltoid if the patient has had a previous midline sternotomy) and on the dorsum of the foot using an automated machine equipped with Clark electrodes. Foot measurements will be repeated after 3 min of 30° leg elevation supported by a wedge. Readings of <40 mm Hg at resting supine position in the foot electrode will be considered diagnostic.26 Regional Perfusion Index (limb TcPO2 values normalised to central values; values<0.6 considered diagnostic) and change in TcPO2 on leg elevation (decrease of >10 mm Hg considered diagnostic) will also be calculated as secondary TcPO2 metrics of interest for PAD diagnosis.
Reference test
Intra-arterial digital subtraction angiography (DSA) has long been considered the gold standard for diagnosis of PAD. However, it is expensive, invasive and carriers a risk of complications. DUS has been shown to be comparable to DSA, making it a useful non-invasive alternative.17
Patients will undergo a full departmental DUS at their respective hospitals on the same day as the index tests by one of two blinded vascular scientists present in each clinic. PAD will be deemed significant when occlusions, or stenosis, or diffuse stenotic disease, individually or collectively, cause significant velocity change (peak systolic velocity ratio≥2) and flow disturbance locally and result in biphasic or monophasic signal distally. All scans will be performed using the Mindray M7 (Shenzhen, China) Portable Ultrasound System with a linear 6–14 kHz transducer.
Quality assurance
PAD-scan: For quality assurance, an external vascular scientist will review a random selection of 40 saved scans.
Reference test: Quality will be assured by acquiring a second DUS by an external vascular scientist in 20 individuals.
Statistical analysis and plan
Sample size and power calculations
Calculations were performed using the described sample size formula for estimating sensitivity.27 Calculations were based on a 95% confidence level (ie, an error of 5%), an estimated PAD prevalence of 50%28 and a predicted sensitivity of 90% for the PAD-scan as derived from our previous research. The estimated sample size required was calculated as 277 patients. From previous research undertaken, we anticipate an attrition rate of 10%. Therefore, the recruitment target for this study is 305 patients.
Statistical tests
Cross-tabulation of the index test results by the results of the reference standard will be made creating a ‘confusion matrix’. This will be used to determine diagnostic accuracy, expressed as sensitivity, specificity, predictive values and likelihood ratios. Receiver operating characteristic analysis will also be performed for each test. Agreement between tests will be analysed using the Cohen’s kappa statistic. Statistical modelling will also be performed to explore the effect of combining tests on diagnostic accuracy in order to identify the most accurate diagnostic strategy.
Interimanalysis and stopping rules
No interim analysis will be performed, and the data will be analysed when the target recruitment of 305 patients has been reached.
Patient and public involvement
Patient representatives were involved in the design of this project protocol. In particular they informed the recruitment process in order to ensure that it was acceptable to patients. After completion of the study they will also be invited to a roundtable discussion of our findings, allowing for integration of their perspectives with those of practitioners. They will also be involved in the dissemination of our findings via patient groups and the production of written and video summaries for patients.
Dissemination
The results of the study will be published a peer-reviewed journal and presented at international surgical and diabetes research meetings. Furthermore, to ensure that our findings reach all stakeholders including patients our results will also be presented at relevant patient group meetings as well as local and regional diabetic foot network meetings.
Acknowledgments
We would like to acknowledge our patient representatives Councilor Melvin Collins and Sister Elizabeth Pigott for their invaluable input and contribution to the drafting of this protocol.
References
Footnotes
Correction notice This article has been corrected since it was published. The article title has been revised.
Contributors PN and UJ were involved in the study conception, study design and acquisition of study funding. PN, UJ, MA, SP, MA and VB were involved in the design and drafting of this protocol.
Funding PN is funded by a National Institute for Health Research (NIHR) Academic Clinical Fellowship award for this research project. This research was also supported by a local Chelsea and Westminster Plus (CW+) Charity grant (Award number: 0051).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval NHS Health Research Authority (NRES Committee London- City & East Research Ethics Committee) approval gained on 21/12/2017 (REC reference 17/LO/1447).
Provenance and peer review Not commissioned; externally peer reviewed.