Article Text

Abstract
Introduction Cardiac rehabilitation (CR) is recommended for secondary prevention of cardiovascular disease and reducing the risk of repeat cardiac events. Physical activity is a core component of CR; however, studies show that participants remain largely sedentary. Sedentary behaviour is an independent risk factor for all-cause mortality. Strategies to encourage sedentary behaviour change are needed. This study will explore the effectiveness and costs of a smartphone application (Vire) and an individualised online behaviour change program (ToDo-CR) in reducing sedentary behaviour, all-cause hospital admissions and emergency department visits over 12 months after commencing CR.
Methods and analysis A multicentre, assessor-blind parallel randomised controlled trial will be conducted with 144 participants (18+ years). Participants will be recruited from three phase-II CR centres. They will be assessed on admission to CR and randomly assigned (1:1) to one of two groups: CR plus the ToDo-CR 6-month programme or usual care CR. Both groups will be re-assessed at 6 months and 12 months for the primary outcome of all-cause hospital admissions and presentations to the emergency department. Accelerometer-measured changes in sedentary behaviour and physical activity will also be assessed. Logistic regression models will be used for the primary outcome of hospital admissions and emergency department visits. Methods for repeated measures analysis will be used for all other outcomes. A cost-effectiveness analysis will be conducted to evaluate the effects of the intervention on the rates of hospital admissions and emergency department visits within the 12 months post commencing CR.
Ethics and dissemination This study received ethical approval from the Australian Capital Territory Health (2019.ETH.00162), Calvary Public Hospital Bruce (20–2019) and the University of Canberra (HREC-2325) Human Research Ethics Committees (HREC). Results will be disseminated through peer-reviewed academic journals. Results will be made available to participants on request.
Trial registration number ACTRN12619001223123.
- health informatics
- coronary heart disease
- myocardial infarction
- complementary medicine
- preventive medicine
- rehabilitation medicine
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- health informatics
- coronary heart disease
- myocardial infarction
- complementary medicine
- preventive medicine
- rehabilitation medicine
Strengths and limitations of this study
To our knowledge, this is the first multicentre, assessor-blind parallel randomised controlled trial assessing the effect of a smartphone application (app) targeting sedentary behaviour change in cardiac rehabilitation (CR) and the effect on hospital admissions and emergency department visits.
The novelty of this study lies in the use of an individualised smartphone app, informed by statistical analysis of personal data, for sedentary behaviour change in CR participants.
The ToDo-CR program uses multiple behaviour change techniques.
We will be completing an economic analysis to assess cost-effectiveness of the intervention for real-world application and potential dissemination into healthcare systems.
A limitation to this study is the requirement of participants to have a compatible smartphone to download the app which may slow recruitment and distort the study population.
Introduction
Cardiovascular disease (CVD) is ranked as the highest burden of disease in Australia and globally.1 2 One in three people who have a cardiac event, a form of CVD, will have another episode and repeat cardiac events increase the risk of premature mortality.3 Secondary prevention programmes, such as cardiac rehabilitation (CR), are important in reducing repeat cardiac events, hospitalisations, economic burden and the progression of CVD.4 5
CR targets positive lifestyle behaviour change (eg, diet, stress self-management, smoking cessation, medication adherence, sleep hygiene) and participants are encouraged to meet physical activity guidelines.4 Despite this, participants continue to not meet the Australian Physical Activity and Sedentary Behaviour Guidelines.6 Increasing physical activity and cardiorespiratory fitness are the main focus of CR.7 8 This does not appear to be effective at changing sedentary behaviour in this group.9–11 An Australian study found that CR participants were engaged in sedentary behaviours for on average 11 waking hours per day.6 Additionally, there was no change in their sedentary behaviour over a 12-month follow-up period.9 Similarly high levels of device-measured sedentary behaviour have been found in other CR and CVD studies in Canada,10 the USA12 and the Netherlands.11 The factors influencing sedentary behaviour in CR participants are unknown.
Sedentary behaviour and physical activity are independent risk factors for all-cause mortality.13–15 A study examining the relationship between television watching (a marker of sedentary behaviour) and 13-year all-cause mortality among people with CVD (n=609), found a 52% increased risk of mortality in those who watched >4 hours per day compared with those who watched <2 hours per day.16 Future research to reduce sitting time and improve health outcomes may need to acknowledge the abundant opportunities and habitual nature of sedentariness if it is to produce sustained benefits.17 A habit is ‘a process by which a stimulus automatically generates an impulse towards action, based on learnt stimulus-response associations’;18 for example, regular prolonged television watching. The apparent habitual sedentary behaviour exhibited by CR participants indicates a potential pathway of change to reduce hospitalisations and all-cause mortality in this population group.
Cues and prompts from mobile technologies such as smartphone applications (apps) and wearables may offer new approaches for changing health behaviours such as sedentary time for CR participants.19 The delivery of app-based interventions for both healthy and chronic disease population groups has shown modest improvements in: daily step counts;20–22 exercise capacity;23 24 self-report25–28 and accelerometer-measured29 physical activity. These findings show the viability of the use of apps in physical activity promotion, yet few studies have reported on, or have targeted, sedentary behaviour change. The few that have investigated apps and sedentary behaviour in healthy and overweight/obese populations have provided mixed results. Some studies found improvements in self-reported television watching time28 and device-measured sitting time,30 31 while others have found no change in sedentary behaviour.26
The translation of evidence into practice for eHealth and mHealth research projects is an issue. Most research and commercially available apps: (1) Are not rooted in evidence-based practice and do not use behaviour change techniques (BCTs);32 33 (2) Are short in duration34 and (3) Use a ‘one size fits all’ approach.35 Statistical analysis of personalised data to create and deliver ‘tailored’ interventions may be more effective. Smartphone apps can be used in this way to review the user’s data, interpret it in relation to the intervention’s aim (eg, reducing sedentary behaviour) and then to initiate the preferred action in an automated fashion. To our knowledge there are no randomised controlled trials (RCTs) assessing the effect of individualised smartphone apps that target sedentary behaviour change in CR.
The aim of this study is to test if a highly personalised behavioural smartphone app for sedentary behaviour change is effective at reducing all-cause hospital admissions and emergency department visits. The research questions are:
Is the behavioural smartphone app (Vire) and 6-month online behaviour change program (ToDo-CR) effective in reducing the risk of all-cause hospital admissions and emergency department visits during the 12 months following commencement of a traditional CR programme compared with usual care CR?
Is the ToDo-CR program effective in decreasing device-measured sedentary time in CR participants at the end of the intervention (6 months) and at follow-up (12 months) compared with usual care CR?
Is the ToDo-CR program cost-effective in delivering the desired outcome?
Methods and analysis
Study design
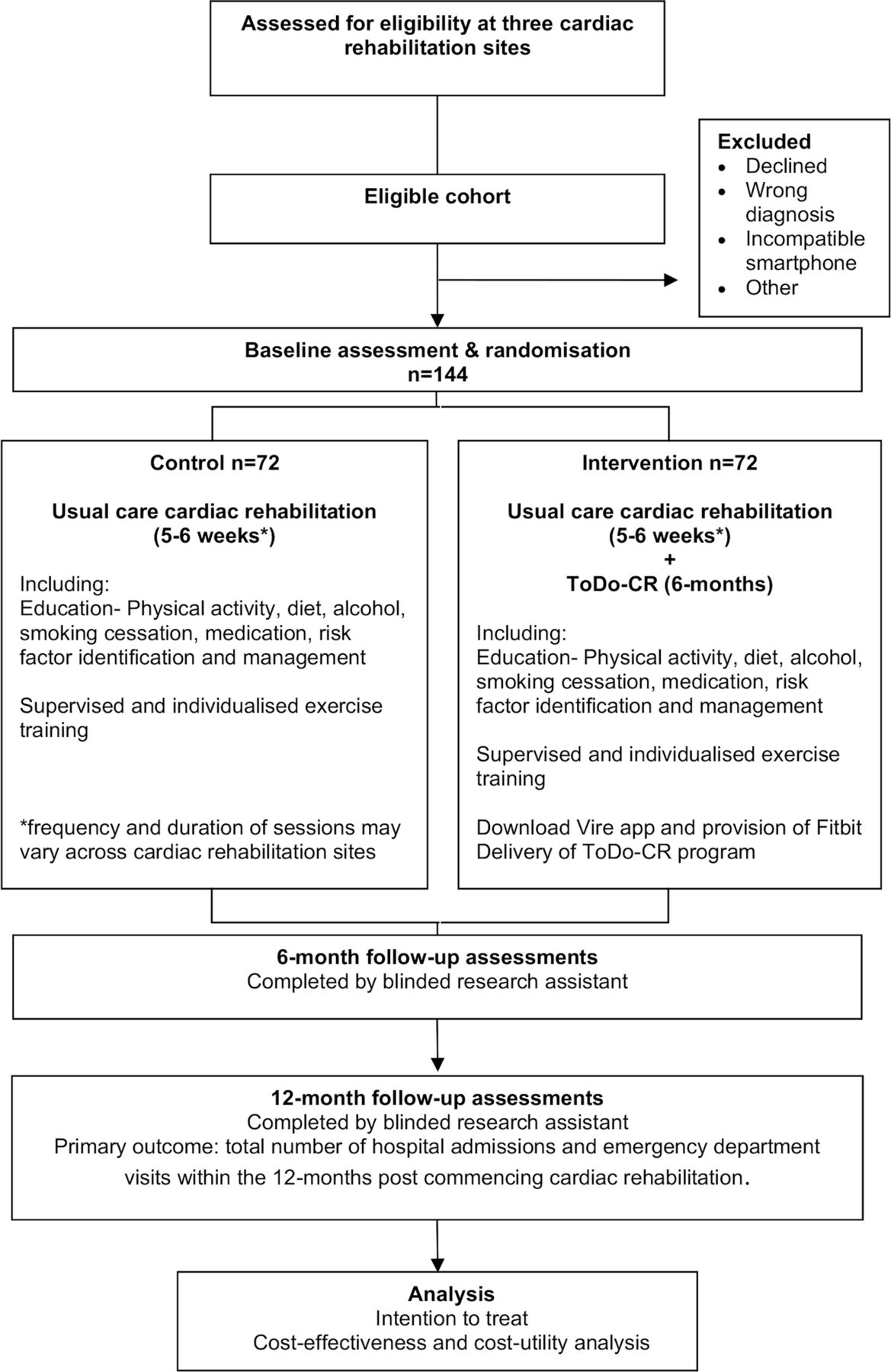
The assessor-blind, multicentre parallel RCT will be conducted in phase II (outpatient) CR programmes in Canberra, Australia, commencing in early 2020. Recruitment will be staggered across a 12-month period and the total study duration for each participant will be 12 months from commencing CR. Participants will be assessed on admission to CR by CR clinical staff. They will then be randomly assigned to either usual care CR or the intervention: CR plus the 6-month behavioural smartphone app (Vire) and ToDo-CR program (see figure 1). CR staff will provide their usual programme with no additional encouragement for participants to increase their physical activity or reduce sedentary behaviour beyond usual care. At 6 months and 12 months postadmission to their CR programme, repeat assessments will be conducted at the University of Canberra by a blinded research assistant for all participants.

Flow of participants through the trial.
Randomisation
Block randomisation will be computerised by an external biostatistician, with participants allocated in a 1:1 ratio to CR plus the ToDo-CR program or usual care CR.36 Randomised group status will be revealed to the baseline assessor and participant following completion of all baseline measures via a phone call from a research member.
Study population
Participants
Participants will be recruited from traditional phase-II (outpatient), hospital-based CR programmes from three sites: Canberra Hospital, Calvary Public Hospital Bruce and National Capital Private Hospital. These hospitals follow the Australian guidelines for CR.7 They are multidisciplinary, group-based and time limited. The Canberra Hospital and Calvary Public Hospital deliver 1 hour of exercise and 1 hour of education, two times per week for 6 weeks. National Capital Private hospital delivers 1 hour of exercise and 1 hour of education, once per week for 5 weeks.
Inclusion and exclusion criteria
Participants will be eligible if they are aged 18+ years old, currently enrolled in CR at the above sites, have a smartphone compatible with downloading the Vire app, willing to wear a Fitbit for 6 months, and have adequate English language and cognitive skills. Participants must have stable coronary heart disease and be receiving optimal medical treatment±revascularisation (eg, coronary artery bypass graft surgery, percutaneous coronary intervention), or have had a myocardial infarction. Optimal medical treatment includes best practice pharmacological therapies and surgical interventions in order to aid in stabilising the participant’s cardiac condition and any other comorbidities (eg, diabetes, hypertension).37
Participants will be excluded if they have a primary diagnosis of atrial fibrillation, spontaneous coronary artery dissection, or aortic or mitral valve replacement. Participants will also be excluded if they have New York Heart Association class II–IV symptoms of heart failure (or documented signs and symptoms of chronic heart failure with ejection fraction <45%), uncontrolled arrhythmias, severe chronic obstructive pulmonary disease, uncontrolled hypertension or diabetes, symptomatic peripheral artery disease, unstable angina, inability to perform a submaximal walking test or unable to wear an accelerometer due to disability (eg, confined to a wheelchair). Written informed consent will be provided by all participants on entry (see online supplemental file 1): model consent form and participant information sheet).
Supplemental material
The intervention: Vire app and ToDo-CR program
The Vire app, ToDo-CR program and Fitbit are considered one intervention. The Vire app is the front-end app used to deliver the online ToDo-CR program (figure 2) and is further explained in the feasibility study prior to this RCT.38 The Vire app also uses data input from the wearable fitness tracker Fitbit. The ToDo program was created by the company Onmi, in collaboration with the Do Something Different approach to behaviour change.39 40 The Do Something Different approach encourages people to try various small tasks to break existing habits and achieve behavioural flexibility without needing sustained willpower.41 Neubeck et al42 reviewed mobile technologies for CVD, and suggested the core components and ideal features for apps to change behaviour include: simplicity of use, provision of credible information, use of behaviour change concepts, real-time biometric data tracking, rewards, app personalisation, social elements and privacy.42 The research team chose the Vire app due to it largely meeting these criteria. The ToDo program was adapted by the research team to target sedentary behaviour based on the Australian Physical Activity and Sedentary Behaviour Guidelines43 and CR guidelines7 to create the 6-month ToDo-CR program. These guidelines encourage people to minimise prolonged sitting and to break up periods of sitting frequently. The ToDo-CR program will commence within 1 week of starting CR.

{kind=link}
{kind=link}
Vire app. (A) Home screen showing the current day’s profile. (B) Fourteen-day overview of scores achieved in each domain. (C) Short behaviour change messages known as ‘Do’s’. (D) The activity score is informed by Fitbit data in the form of daily steps and time spent being active. (E) The social opportunity score is informed by GPS location data. The number of new places visited in a day is recorded, as well as the amount of time spent in each location. Spending more time in a new place creates more opportunities to meet new people and be social. (F) The variety score uses Fitbit data and GPS location. It looks at how different today is from your usual day in terms of locations visited, how uncommon those locations are to you, the routes and distances taken between locations, and the time of day you are being active. GPS, global positioning system.
The Vire app integrates and analyses data from a Fitbit and the phone global positioning system (GPS) location. This is done in real time, using specific algorithms which process and interpret the data input and generate an appropriate action. These algorithms create a comprehensive digital profile and inform the delivery of the personalised ToDo-CR program to target the participant’s current behaviour. Vire addresses three domains that influence the habitual constructs that may trap a person in prolonged periods of sedentary behaviour: activity, social opportunity and variety. These are presented as scores that update throughout the day and provide the participant with insight into these behaviours through clickable displays in the app (figure 2A and B).
At the beginning of the programme, participants complete a brief initial questionnaire in the app. This collects information regarding personality traits and habitual behaviours relating to sedentary behaviour (eg, how often do you spend evenings watching TV or in front of a screen?).
For a duration of 1 week, baseline data are collected in Vire to establish the participant’s ‘typical’ week. Minimum and maximum values are recorded during this week for each domain (ie, activity, variety and social opportunity) and then linearly rescaled (0–10 range). These baseline data are used to determine the scoring in terms of absolute and relative behaviour (ie, actual number of steps and relative increases and decreases). A score of ‘0’ is given when daily values are equal to or below the baseline minimum. A ‘10’ is awarded when the daily value equals or exceeds the baseline maximum. The baseline minimum and maximum values for each domain will be updated based on a sliding 30-day window to allow for changes in behaviour throughout the 6-month programme. The minimum and maximum values are then used to calibrate the ToDo-CR program and trigger the key behaviour change component: ‘Do’s’.
Do’s are short behaviour change messages sent by the Vire app as push notifications (figure 2C). They suggest small positive actions designed to disrupt usual habits; encouraging the participant to step outside of their comfort zone (ie, habitual behaviours).44 Participants will receive up to three Do’s per week. The frequency of messages will peak and taper throughout the 6 months. This will manage participants’ commitment and engagement over time which has been raised as a potential issue for longer-term app-based studies.45 Each participant will receive 52 Do’s during the ToDo-CR program. There are 23 Do’s that all participants will receive involving an introduction to the app and generic advice relating to sedentary behaviour, physical activity, and monitoring adverse signs and symptoms while being active. These Do’s are known as ‘static Do’s’. The Do’s either directly or indirectly target sedentary behaviour change by suggesting microbehavioural alternatives to their usual habits that may influence sedentary time in such a way that they don’t feel the burden of making a significant lifestyle change. A third of the static Do’s relate directly towards sedentary behaviour and physical activity. We acknowledge that sedentary behaviour and physical activity are influenced by different factors (ie, environmental, social and individual determinants),17 46 however both sedentary behaviour and physical activity are on the energy expenditure continuum.47 Though the targeted behaviour in this intervention is sedentary behaviour, when sedentary behaviour is reduced, the behaviour is substituted by physical activity, although often light intensity physical activity.17 Further, incorporating a combination of sedentary behaviour and physical activity focused elements has been identified as a feature of promising sedentary behaviour interventions in those with pre-existing disease.48 This justifies the relevance of some Do’s promoting physical activity.
After the first week, ‘personalised Do’s’ commence. These Do’s are driven by the initial questionnaire and the Fitbit and phone GPS data (see examples in table 1). The Vire app integrates these data through machine learning models (ie, dynamic warping).49 In the ToDo-CR program, there are a possible 105 personalised Do’s in the message bank. Forty-five per cent of personalised Do’s are directed specifically at sedentary behaviour and physical activity, with the remaining personalised Do’s relating to other health and lifestyle-based messages that influence activity levels (ie, sleep, stress, mental health, socialisation and healthy eating). However, the exact percentage of sedentary behaviour and physical activity-based Do’s that each participant receives is dependent on the individualised app data.
Example of personalised Do’s informed by collected Fitbit and global positioning system (GPS) data
The personalised Do’s are sent when the system identifies a need for improvement in a certain domain (figure 2D, E and F). This is initiated when the participant scores low (between 0 and 3.3 in any of the domains) on three consecutive days. As a result, an appropriate individualised and context-specific Do is sent to target that behaviour on the third day. In instances where a person may be scoring high in one domain, such as social, and low in another, such as activity, a Do which plays to the individual’s strength, yet encourages an increase in their low-performing domain is triggered. This is demonstrated in table 1 example 1d. In addition, the ToDo-CR program is localised with links and references to local landmarks and community pages to help increase the relevance of the programme to the participants (example table 1b).
The BCTs and theoretical framework
The ToDo-CR program content and features use 16 different BCTs (as analysed using Michie’s BCT taxonomy v1)50 targeted at decreasing prolonged periods of sedentary behaviour. These are explained in detail in table 2. A summary of the functional requirements of the Vire app is provided by the app developers; see online supplemental file 2. Furthermore, ToDo-CR can be linked with elements of social cognitive theory,51 cognitive flexibility theory52 53 and theories relating to habit,54 to promote an accumulation of microbehavioural changes targeted at reducing long-term, sustained sedentary behaviour.
Supplemental material
The BCTs* used in the Vire application (app) and ToDo-CR programme
Social cognitive theory can be linked with this study because it acknowledges that learning occurs in a social context.51 This theory considers the unique way that people develop and maintain behaviour with consideration to the social environment in which they perform the behaviour in. Sedentary behaviour may be a function of the social calendar.17 By encouraging an increase in social activity, sedentary behaviour patterns may change. Out of the six main constructs of social cognitive theory, the ToDo-CR program is compatible with three: reciprocal determinism, behavioural capability and self-efficacy. Reciprocal determinism is incorporated in the way the ToDo-CR program uses the domains of activity, social opportunity and variety to draw on the strengths an individual may have in one area to improve in another. Behavioural capability is demonstrated by how the program builds the participant’s essential knowledge and skills and teaches them how to become less sedentary. The ToDo-CR program aims to develop self-efficacy by suggesting small and easily achievable actions that slowly build confidence, remove perceived barriers and increase facilitators of behaviour change.
Cognitive flexibility may be the key mechanism in reducing unwanted habits and may reflect individual differences in the ability to break habitual behaviours.55 Cognitive flexibility is the ability to restructure and transfer knowledge and skills as an adaptive response to changing situations, beyond the initial learnt situation.56 The ToDo-CR program is compatible with the four main principles of cognitive flexibility theory: (1) Learning activities are provided in multiple representations; (2) Materials are not oversimplified and support context-dependent knowledge; (3) Instruction is individualised with an emphasis on knowledge construction; (4) Knowledge is highly interconnected rather than compartmentalised.52 53 By prompting microbehaviour changes, the ToDo-CR program may help the individual to become more cognitively or behaviourally flexible and, as such, provide the individual with more choice over how they respond in different situations.44
In theories of habit, there is the notion of habit as habitus:54 the structure that organises the many dispositions that make up someone’s character and overarchingly regulates and prioritises their choice of action in any given situation.57 58 Habitus may undermine traditional rehabilitation for creating behaviour change.54 The ToDo-CR program intends to elicit sedentary behaviour habit transformation to support usual care CR.
Delivery of intervention
The participants randomised to the ToDo-CR program will be given a Fitbit Inspire and will download the Vire app (with a study-specific login code) onto their smartphone. They will be provided with written instructions on how to download the Vire and Fitbit apps (available in both Android and iOS). Participants will receive a phone call from a researcher to ensure they have been able to download the app. These participants will be required to wear their Fitbit throughout the 6-month intervention duration during waking hours. If a participant stops wearing their Fitbit, it will not impact the delivery of the intervention as the Vire app can also use the native smartphone step-tracking software. The ToDo-CR program will be delivered for 6 months and then access to the Vire app will be ceased.
Regular app updates are required to improve app functioning due to the fast-evolving nature of technology. Participants will be requested to switch their smartphones to automatic updates. All updates will be recorded and reported.
Usual care control group
Those randomised to the control group will participate in usual care CR and will not have access to the Vire app and Fitbit during their 12-month participation in the study. A Fitbit Inspire will be gifted to the usual care group on completion of the study.
Outcome measures
Assessor blinding to group allocation will be used throughout the study. The CR clinical staff and research assistant will complete calibration training and follow a standardised protocol using the same research grade equipment in order to reduce between-assessor inconsistencies. All outcome measures will be completed at baseline (on entry to CR), at 6 months and 12 months (figure 1).
Hospital admissions and emergency department visits
The primary outcome measure is total number of hospital admissions and emergency department visits within the 12 months post commencing CR. All-cause hospital admissions will be defined as any non-elective admission to an acute care hospital. We will also be considering the timeframe from CR to hospitalisation and/or emergency department visits. Participants will be surveyed at 6 months and 12 months to report if they have had any unplanned hospital admissions or presentations to the emergency department in the last 6 months. This information will then be verified by hospital patient admission records to ascertain the Australian Refined Diagnosis Related Group (AR-DRG) and Urgent Related Group (URG) classification code assigned to the admission.
Secondary outcomes
Sedentary and physical activity levels will be objectively measured using a triaxial commercial accelerometer (Actigraph wGT3X-BT, Fort Walton Beach, Florida, USA) worn by participants on the right hip for seven consecutive days during waking hours. ActiLife software (ActiLife V.6. 13.4) will be used to sample and download all raw data (30 Hz), convert it to 15 s epochs and then to counts per minute (cpm).10 11 Data will be screened and excluded if there are less than 10 hours per day wear time (non-wear time defined as >60 consecutive minutes of zero activity data) or if there are less than 4 days of valid data.10 11 59 To determine time spent in light and moderate-to-vigorous intensity physical activity, the Sasaki vector magnitude cut-points will be used (150–2689 cpm and ≥2690 cpm).10 11 59 60 For sedentary behaviour, the vector magnitude cut point will be <150 cpm.10 11 59 61 To estimate the daily time spent in sedentary behaviour and physical activity, the total time (minutes) spent in each threshold will be divided by the number of valid days. Sedentary behaviour will also be expressed as a percentage of total daily wear time. A minimum length of 10 min will be used to detect a sedentary bout and each bout will be recorded to determine the number and average length of sedentary bouts per day.10
Anthropometric characteristics and blood pressure will be recorded. A calibrated set of scales and stadiometer will be used to measure height (m) and weight (kg) and body mass index (kg/m2) will be calculated. Waist and hip measures (cm) will be completed using a stretch-resistant tape measure. The waist circumference will be recorded as the midpoint between the lower margin of the lowest palpable rib and the top of the iliac crest. The hip circumference will be recorded as the widest portion of the buttocks when viewing from the side and keeping the tape measure parallel to the floor. Each measure will be repeated twice; if the measurements are within 1 cm of each other, the average will be calculated. If the difference exceeds 1 cm, the two measures will be repeated. A sphygmomanometer (Welch-Allyn DS66) will be used to measure blood pressure on the right arm of seated participants.
Functional exercise capacity will be measured with the 6 min walk test, frequently used in CR as a submaximal test of exercise capacity and shown to have moderate-to-high reliability and validity.62 Participants will be encouraged to walk as fast as possible on a 20–25 m walking track for 6 min and the distance achieved will be recorded. A change in distance of 25 m is considered a clinically meaningful change in coronary heart disease participants in CR.63
Health-related quality of life (HRQOL) will be assessed using the Assessment of Quality of Life (AQoL-6D). The AQoL-6D was developed in Australia and uses Australian importance weights.64 The AQoL-6D is self-administered and consists of 20 items covering: independent living, mental health, coping, relationships, pain and sense. A multiattribute utility score is then obtained; where a score of 100 reflects best health.65 The AQoL-6D is reliable and valid in community settings.66 67
The Hospital Anxiety and Depression Scale (HADS) will be used to assess anxiety and depression.68 It is a valid measure for cardiac populations.69 70 The HADS involves 14 questions (4-point Likert Scale) covering the occurrence of symptoms of anxiety and depression in the last 2 weeks. A score of 0 represents the best outcome and a score of 21 is an indicator of anxiety or depression.68 The minimal clinically important difference for patients with CVD is 1.7.71
The stage of behaviour change will be assessed using the University of Rhode Island Change Assessment Scale (URICA-E2) for exercise behaviour. The URICA-E2 Questionnaire is based on the Transtheoretical Model of Behaviour Change.72 It describes the phases through which a person passes when changing a health behaviour based on their readiness to make the change. The five stages include: precontemplation, contemplation, preparation, action and maintenance. The URICA-E2 is a 24-item (5-point Likert Scale) measurement scale leading to a continuous total score. For this study, we have adapted the wording and definitions from ‘exercise’ to physical activity to align with the secondary aims of reducing sedentary behaviour and, hence increasing physical activity. We do not anticipate that this will interfere with the questionnaire psychometrics.
Demographic and other relevant clinical information will be collected using a questionnaire. This includes questions on sociodemographic variables (eg, gender, age, education level) as well as clinical predictor variables (eg, cardiac-related medication, other medical conditions, smoking status), and whether they use an activity tracker such as a smartphone app or watch. The CR clinicians will also record participant admission diagnosis and date of event or intervention details.
The usability of the Vire app and ToDo-CR program will be assessed through the Unified Theory of Acceptance and Use of Technology (UTAUT2) Questionnaire.73 The UTAUT2 is a 23-item questionnaire (7-point Likert Scale) assessing performance expectancy, effort expectancy, social influence, facilitating conditions, hedonic motivation, habit, behavioural intention and use. This questionnaire was developed to provide an understanding of consumer acceptance towards a new technology or system. Adherence to using the Vire app will be assessed through viewing app logs showing completion of Do’s.
If an adverse event occurs while the participant is taking part in the study, they will be managed immediately in line with university and CR centre policies and procedures. This has been outlined in the model consent form and participant information sheet (see online supplemental file 1). If there is an adverse event that is related to the intervention, the study coordinator will be made aware of group allocation and will discuss continuation of the participant’s involvement with the research team. Any adverse events will be reported to the relevant ethics committees and advisory group. A database will be kept and reported accordingly.
Economic evaluation
Information relating to the costs of implementing and delivering the intervention will be collected including payment for the use of the Vire app and ToDo-CR program, time and phone call support from a researcher for issues relating to the app download and general function, and Fitbit Inspire purchases. We will evaluate the effect of the intervention on the rates of unplanned cardiac-related and/or all-cause hospital admissions and emergency department visits within the 12 months post commencing CR using a cost-effectiveness analysis. Hospital cost information will be obtained from Independent Hospital Pricing Authority, Australia and/or Australian Institute of Health and Welfare. Information on secondary measures such as health behaviour change (sedentary behaviour and moderate-to-vigorous physical activity), body mass index, waist circumference, quality of life (AQoL-6D), clinical and demographic information and the costs associated with the use and delivery of the Vire app and ToDo-CR program will be used. A cost-utility analysis will also be undertaken with societal perspective using gained quality-adjusted life years (QALYs) as the measure of health effects. The impact on HRQOL can be measured using the AQoL-6D and the incremental cost-effectiveness ratios per QALYs will be calculated.74 Information on the participants’ medication and health service utilisation costs, based on the AR-DRG and URG classification codes will also be used. From these analyses, the additional cost per unit of health benefit gained over the lifetime (by using the ToDo-CR program with CR compared with usual care CR alone) can be determined.
Sample size calculation
The sample size is based on a similar study23 finding a 28% difference in rehospitalisation and emergency department visits between the usual care CR group (a standard rate of 44%) and the CR plus digital health intervention group (a standard rate of 16%) at 3 months following CR. With a two-sided significance of p<0.05 and power of 88% (calculated using G*Power 3.1.9.4), 108 participants are needed (54 in each group). Based on a previous observational study in the same population group, we will allow for a 30% dropout.9 This does not account for missing data. The total sample will be 144 participants, with 72 in each group.
Data analysis
All participants who complete the baseline assessment and attend at least one CR session will be included in the analysis. Data will be analysed according to group assignment using both intention-to-treat and on-protocol analyses to determine if the two methods yield the same results. This justifies the allowance of a 30% dropout.
The primary analysis will be the comparison of rates of hospital admissions and emergency department visits (intervention vs control) within the 12 months post commencing CR. This will be done using logistic regression models, adjusting for sociodemographic and other covariates. To analyse sedentary behaviour and all other secondary outcomes, methods for repeated measures analysis will be used. Linear (for continuous outcome data) and generalised linear (for binary and count outcome data) mixed-effects models for repeated measures will be used for between-within group comparisons and time-interactions analyses adjusting for demographic characteristics and other potential covariates. The significance level will be set at 5% α level. All estimated effects will be reported along with their associated 95% CIs. All data will be analysed using SPSS (Statistics V.26).
Data management
Participant paper and electronic files will be maintained in secure storage and on a password protected computer for a period of 7 years after completion of the study as required by the ethics committees. Non-numerical data will be coded as per predefined coding definitions. Data entry screening will be conducted at the time of data entry to ensure no inconsistencies between paper-based and electronic data.
Discussion
This study uses an individualised smartphone app, informed by statistical analysis of personal data, for sedentary behaviour change in CR participants. We will be determining the short-term and medium-term changes in sedentary behaviour and physical activity with the intention that this will have a positive effect on unplanned hospitalisations and emergency department admissions.
Methodological considerations and limitations
Many methodological considerations will be related to the technological nature of this intervention. A limitation to this study is the requirement of participants to have a compatible smartphone to download the app which may slow recruitment and distort the study population. A study using a smartphone-based home care model to deliver CR, compared with traditional CR, found that of the 835 potential participants assessed for eligibility, 106 (12%) were excluded due to not having a compatible smartphone to deliver the intervention.24 Further, the use of new and innovative smartphone technology is likely to skew the participant population to a younger cohort as seen in other CVD smartphone-based interventions, with mean age: 46–58 years.24 38 75–77 Despite this, studies have found that Australian CR participants are interested in support via the internet and mobile phones78 79 and approximately 65% of CR participants reported having a smartphone.80 This may not be an issue in the future with further proliferation of mobile technology use across generations and in healthcare.81 Another limitation is the use of multiple assessors to collect baseline data at each of the CR sites which may introduce an element of bias. We have tried to account for this by using identical calibrated equipment and by providing assessors with training on standardised outcome measurement. The use of the Actigraph triaxial accelerometers may also misclassify standing stationary time or arm-based exercise as sedentary behaviour due to the worn location on the hips. However, this means of measuring quantity and intensity of movement is still considered to be valid when using appropriate cut points for sedentary behaviour.10 61 The use of a Fitbit in combination with the Vire app may make it difficult to determine if changes in behaviour occurred due to self-monitoring using the Fitbit or from self-monitoring and prompting from the Vire app. Subgroup analysis may be completed for those identified in the control group who do use activity trackers such as smartphone apps and watches in comparison to those using the Vire app and ToDo-CR program.
Impact
The results of this research will help inform clinical practice and potentially reduce unplanned hospital admissions and emergency department visits. By combining innovative technology, evidence-based activity guidelines and BCTs, the ToDo-CR program aims to create sustained behaviour change in reducing sedentary time. The Vire app and ToDo-CR program is the only program to our knowledge targeting sedentary behaviour in CR. If successful, the use of ToDo-CR will be promoted as an adjunct modality to traditional CR and may have the potential to be extended towards other chronic disease rehabilitation programmes due to its scalability and highly personalised approach.
Ethics and dissemination
Ethics approval has been received from the Australian Capital Territory Health (2019.ETH.00162), Calvary Public Hospital Bruce (20–2019) and the University of Canberra (HREC-2325) Human Research Ethics Committees. Results will be disseminated through peer-reviewed academic journals. Results will be made available to participants on request.
Trial status
Australian New Zealand Clinical Trials Registry: ACTRN12619001223123, Date registered: 04 September 2019; anzctr.org.au/Trial/Registration/TrialReview.aspx?id=378184&isReview=true.
Acknowledgments
The authors thank The Canberra Hospital, Calvary Public Hospital Bruce and National Capital Private Hospital cardiac rehabilitation program staff for their ongoing support in recruiting participants and collecting baseline data.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KP, RD, RK, IM, TN, SvB and NF participated in the design of the study and development of the trial protocol. KP drafted the manuscript and all authors contributed to subsequent drafts. All authors read and approved the final manuscript.
Funding This work was supported by a Medical Research Future Fund grant number (1184607). The funding organisation was not involved in the writing of this manuscript. The Medical Research Future Fund conducts periodical audits of trial conduct.
Competing interests KP, RD, RK, IM, TN and NF declare they have no competing interests. Vire and ToDo-CR was created by a private company, Onmi in collaboration with Do Something Different Limited. Onmi will not provide any funding for this study. SvB is the Manager and Designer for Onmi (https://onmi.design/), the Vire app and ToDo behaviour change program developer.
Patient and public involvement statement Following completion of a feasibility trial using the Vire app and a version of the ToDo-CR programprogramme, participants, CR staff and the research team reviewed the intervention usability to inform the RCT development. The Vire app has been progressively developed by the creators, Onmi, and reviewed by the public in previous studies.
Patient consent for publication Not required.
Ethics approval Ethics approval has been received from the Australian Capital Territory Health (2019.ETH.00162), Calvary Public Hospital Bruce (20–2019) and the University of Canberra (HREC-2325) Human Research Ethics Committees. Results will be disseminated through peer-reviewed academic journals. Results will be made available to participants on request.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.