Article Text

Abstract
Objectives To estimate the impact of a smallpox attack in Mumbai, India, examine the impact of case isolation and ring vaccination for epidemic containment and test the health system capacity under different scenarios with available interventions.
Setting The research is based on Mumbai, India population.
Interventions We tested 50%, 70%, 90% of case isolation and contacts traced and vaccinated (ring vaccination) in the susceptible, exposed, infected, recovered model and varied the start of intervention between 20, 30 and 40 days after the initial attack.
Primary and secondary outcome measures We estimated and incorporated in the model the effect of past vaccination protection, age-specific immunosuppression and contact rates and Mumbai population age structure in modelling disease morbidity and transmission.
Results The estimated duration of an outbreak ranged from 127 days to 8 years under different scenarios, and the number of vaccine doses needed for ring vaccination ranged from 16 813 to 8 722 400 in the best-case and worst-case scenarios, respectively. In the worst-case scenario, the available hospital beds in Mumbai would be exceeded. The impact of a smallpox epidemic may be severe in Mumbai, especially compared with high-income settings, but can be reduced with early diagnosis and rapid response, high rates of case finding and isolation and ring vaccination.
Conclusions This study tells us that if smallpox re-emergence occurs, it may have significant health and economic impact, the extent of which will depend on the availability and delivery of interventions such as a vaccine or antiviral agent, and the capacity of case isolation and treatment. Further research on health systems requirements and capacity across the diverse states and territories of India could improve the preparedness and management strategies in the event of re-emergent smallpox or other serious emerging infections.
- public health
- infection control
- virology
- smallpox
- variola
- vaccines
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The model takes into account heterogeneity of age, disease transmission and immunological levels.
Age-specific rates of immunosuppressive conditions were estimated for Mumbai and included in the model.
This study does not include different route of transmission than airborne.
Other aspects that could influence transmission include seasonality, or vaccination effectiveness such as vaccine refusal were not included in the model.
Introduction
India is the second-most populous country in the world, with several megacities, such as Mumbai, Delhi and Chennai, where people live in close proximity with high population density. Infectious disease epidemics are common in India, such as H1N1pdm09 which has been causing recurrent, severe epidemics since 2009.1 2 A study of the phylogeography of influenza H1N1pdm09 in India showed that most transmission around the country was from Maharashtra.3 Any respiratory transmissible infectious disease can spread rapidly especially in an urban population. A biological attack caused by a respiratory-transmissible agent such as smallpox could have a serious impact in India, due to high contact rates and population density.4 The last natural case of smallpox occurred in 1977, but India was at that time the epicentre of smallpox globally.5
Smallpox was declared eradicated globally in 1980, but recent developments in synthetic biology of orthopoxviruses have increased the risk of re-emergence of the variola virus (VARV).6–9 Stocks of live VARV are currently held in two WHO collaborating centres in the USA and the Russian Federation, but the virus could be created synthetically.7 10
Before smallpox eradication, nearly 60% of unvaccinated close contacts or secondary household contacts of smallpox were infected, and airborne transmission was also observed.11 India was one of the most challenging settings for the global eradication campaign, which began in 1967 using mass vaccination as a strategy.12 India had its first lymph smallpox vaccine in the 19th century,10 13–16 and at the beginning of 20th century (1900–1947), many research institutes in India started manufacturing smallpox vaccine as lymph.17 In the previous century, the ‘Government of India Act of 1919’ introduced a system of dual government for the British India provinces with the principle of division of executive branch of each provincial government into popularly responsible section and authoritarian section.18 19 This resulted in fragmentation of authority, due to transfer of various areas of administration from federal ministers to local-government, including education, agriculture, public works and public health.18 19 Local governments were responsible for providing public health programmes, such as smallpox vaccination.17 However, insufficient financial support from local authorities to finance vaccination led to low uptake of smallpox vaccination.17 Patchy vaccination efforts continued till the start of World War II (1939) and became worse during the war.17 World War II led to a further resurgence of smallpox in the period 1944–1945 in India.17 However, an increased focus on smallpox vaccination after the war resulted in a decrease in cases.17 Due to the inability to achieve high coverage with mass vaccination in India, the WHO made the decision to change from mass vaccination to ‘surveillance contaminant searching’ and ring vaccination first in Africa, followed by India; this thereafter became the mainstay of the global eradication strategy.17 20 Ring vaccination strategy limits the spread of disease by vaccinating close or direct contacts of diagnosed cases, who are most likely to be infected.21
Smallpox is a highly infectious disease, which can be caused by two different variants, variola minor and variola major. The first presents with much milder symptoms and a case fatality rate (CFR) of about 1%, while variola major had a CFR greater than 30%22–24 and the risk of death higher among infants,25 26 older people27 and the immunosuppressed. The impact of smallpox reemergence is affected by residual vaccine immunity and immunosuppression.28 Smallpox vaccine immunity wanes over time, possibly as rapidly as within 5 years.29 30 People with multiple primary vaccinations may have greater protection, up to 10–20 years or longer.31 32 However, it is unclear how long protection lasts after multiple vaccinations. Nearly 40 years since mass vaccination programmes ceased, residual vaccine immunity is likely to be minimal.31 32 Routine smallpox vaccination has not occurred in India since eradication was declared in 1980.29 Population immunity in India is therefore likely to be low. There has been limited research on population-level smallpox immunologic status and residual vaccine immunity in India. Furthermore, health capacity in India in the event of resurgent smallpox will be a challenge in remote, rural and urban settings, as well as in coordinating public health response across a largely privatised health sector.33
Aims
The aim of this study is to estimate the impact of smallpox re-emergence in Mumbai, India under different scenarios with available interventions.
Methods
The scenario is a deliberate, large scale attack, with 1000 cases of smallpox occurring simultaneously in Mumbai. A large scale attack was used to test the worst case scenario. We assumed that the virus used in the biological attack is variola major, therefore the circulation of variola minor is not considered in this analysis.
We used a susceptible, exposed, infected, recovered model for smallpox transmission28 34 35 to simulate a smallpox outbreak in Mumbai. The model assumes an overall rate of transmission from person to person based on observed epidemiology as described below, but does not differentiate modes of transmission (such as airborne, fomite or contact).
In the model, the population was categorised into vaccinated and unvaccinated compartments and these compartments were further split into severely immunosuppressed, mildly immunosuppressed and immunocompetent groups. The model contains ordinary differential equations to shift the population into different epidemiological transmissible states such as susceptible, infected, infectious, recovered and dead.27 Susceptible and latent compartments in the model are a matrix of 6 rows and 18 columns, where the rows represent the different immunity levels or disease severity and the columns are the age groups, while the infectious compartment is a matrix of 4 rows and 18 columns, representing smallpox disease types and age groups, respectively.27
Mumbai was selected because transmission studies of influenza (also transmitted by the respiratory route, such as smallpox) show it to be the epicentre of respiratory transmission.3 We then simulated outbreak response in order to explore the duration of the epidemic, vaccination doses needed and required health capacity system in Mumbai. Vaccine efficacy pre-exposure was estimated and reported from WHO as between 91% and 97% for first-generation vaccines, used in the pre-eradication era, while the second-generation vaccines, stockpiled now in most countries, has an estimated efficacy between 96% and 99%.36 In this study, we assumed a vaccine efficacy of 95% and 98% for people never vaccinated and previously vaccinated, respectively. In the case of vaccine as post-exposure prophylaxis for contacts, we halved the efficacy to 50% and 53%, respectively.
We estimated the total vaccine doses required and the number of hospital beds required for both best and worst-case scenarios. The number of doses were compared with the available WHO stockpile of smallpox vaccine37 in order to determine whether the stockpile is sufficient to control the epidemic in Mumbai. We also determined the duration of the epidemic under different scenarios. The number of hospital beds were compared with the available beds in Mumbai33 to identify in which scenario the beds would be insufficient.
The model accounts for different infectivity and susceptibility for immunocompromised and healthcare workers (HCWs).28 34 The population data and contacts rates for Mumbai, to inform the model, were estimated as follows. Model diagram, differential equations and all parameters used (see online supplemental table 1) are listed in the online supplemental material 1.
Supplemental material
Supplemental material
Population, healthcare workers and hospital beds
We used an estimated total population for Mumbai, India in 2019,38 with age distributed following the age-specific percentages of Mumbai population.39 The model uses 18 age groups, 5-year wide up to 84 years old with an additional age group, 85+ years. We estimated the number of HCWs in India, consisting of physicians, nurses and midwives, who accounted for 0.29% of the total Indian population in 2015 and used this estimate for Mumbai population.40 To distribute the HCWs across age groups, we used the age distribution of nurses in Mumbai,41 as they represent the biggest part of the HCW population. We estimated the number of hospital beds in Mumbai, and the proportion of beds in private hospitals using available data sources.42 43
Contact matrix
We used an estimated age-specific contact matrix for India.4 The matrix is represented in 5-year age group starting from 0 to 4 years old to 70–74 years old and the rest of the contacts are presented in one upper age group (75+ years).4 Since our model uses a 15 age-group contact matrix and the India matrix is available in 16 age groups, we took the mean of the last two age groups and fitted 15 age group contact rates in the model (see online supplemental table 2).4 27
Supplemental material
Previously vaccinated population
We assumed that about 70% of the population in 40–69 years age group in India (born before 1977) were previously vaccinated (see online supplemental table 3),17 considering the fact that smallpox was epidemic in India in 197444 and a higher proportion of Indian populations born before 1977 are vaccinated.20 We considered vaccination had stopped in India after 1977 since the last case of smallpox in India was seen in May 197520 and India was declared free from smallpox in 1977.17 The immunity against smallpox wanes 1.41% per year after vaccination.27 30 Using this rate of waning, we calculated the age-specific residual protection by multiplying 1.41% with the number of years from vaccination and then subtracted from 100% effectiveness, for vaccinated people 40–69 years.27 We considered that vaccine immunity wanes over time and people vaccinated prior to 1980 and now aged >69 years have zero residual immunity against smallpox.27
Supplemental material
Immunosuppressed population
A minimum estimate of immunosuppression in India was made using HIV infection, cancer chemotherapy, steroid treatment for asthma and chronic obstructive airways disease, organ transplantation and autoimmune diseases, using a previously published method for estimating immunosuppression.27 The total patients with HIV in India was estimated to be 2.14 million in 2017, which is 0.1597% of the total population.45 We used an estimated age-specific distribution from 2009.46 However, this study divides the HIV prevalence in only three age-groups, which we further divided equally for our 18 age groups. We estimated the cancer prevalence to be 0.08391% in India in 2015.47 We distributed this across age groups in the model using age-specific cancer prevalence data from 2014.47 Around 7715 solid organ transplants were made in India in 201548 representing 0.00058938% of the total population. We have used age-specific transplants distribution estimated for the US population, as Indian data were not available.49 Asthma and chronic obstructive pulmonary disease (COPD) were estimated to be 5.47% and 1.30% of the total Indian population in 2015.50 51 However, most patients in India would not receive oral or inhaled corticosteroids compared with a high-income country, therefore we assumed one-third of asthma and patients with COPD that is, 1.82% and 0.43%, respectively would be treated with corticosteroids. We estimated the number of people with asthma and COPD for the given age groups and divided equally for 5-year age groups, respectively, and then estimated the prevalence percentage with respect to the population in that age group. Persons living with autoimmune diseases in India are estimated to be 7.96% of the total population.52–59 As most people in India with the autoimmune disease would not have access to immunosuppressive drugs, we assumed one-third of the total, that is, 2.65% of people would be treated with immunosuppressive drugs. We distributed this prevalence using the average age-specific distribution estimated from Spain and the US rheumatoid arthritis incidence.60 61 They divide the incidence into seven age groups over the entire population, which we adapted to 18 age groups. Accordingly, the model was fitted with the immunosuppressed proportion estimated for India adjusted to the Mumbai population.
Smallpox disease types
Once infected we assumed four different types of disease for smallpox: vaccine-modified, ordinary, flat and haemorrhagic smallpox. We assumed that each disease type has a different infectivity (R0), a different CFR and a different age distribution rate depending on the immunological status of the infected person, as outlined in our previous study and in online supplemental table 6.34 Infection with haemorrhagic and flat smallpox have the highest infectivity with R0=1062; however, we used an R0=5 to account for the isolation of severely ill patients. For ordinary smallpox, we assumed R0=7.96, estimated from a detailed study of an outbreak in Nigeria in an unvaccinated community,63 and for modified smallpox, we assumed R0=5.3 (2/3 of the R0 estimated for the ordinary type). Because of milder symptoms, we accounted for isolation and halved R0 from the third and fourth day for ordinary and modified smallpox, respectively.
Supplemental material
Data from historical outbreaks31 64 shows that persons infected with haemorrhagic, flat and vaccine-modified smallpox have a CFR of 100%–95%, 90% and 0%, respectively, while for ordinary smallpox, infection is age-specific.31 In our study, to take into account better access to healthcare, we assumed the same CFR for ordinary and vaccine-modified smallpox, but a slightly lower CFR for haemorrhagic and flat cases, being 90% and 75%, respectively. All CFRs are shown in the online supplemental material 1.
Distribution rates of each disease type for healthy unvaccinated people are derived from available data from Rao study31 by linear interpolation of the available age groups. While for severe immunosuppressed we assumed them to have only haemorrhagic smallpox, for mild immunosuppressed people we doubled the rates of haemorrhagic and flat estimated for healthy unvaccinated people. For the previously vaccinated subgroup we estimated 25.3% of vaccinated persons get vaccine modified smallpox31 and we applied a waning immunity rate of 1.41% per year following vaccination.65 Age-specific rates of each disease by immunity level are shown in the online supplemental material 1.
Sensitivity analysis
A sensitivity analysis conducted on the number of initial infected, percentage of case isolation and of contacts vaccinated and time to starting the response (see online supplemental table 4). We varied the initial attack size between 50 and 100 000 to determine the effect of the epidemic without intervention in Mumbai. The total recovered, infected and death rates were estimated for Mumbai for several scenarios. We tested 50%, 70%, 90% of case isolation and contacts traced and vaccinated (ring vaccination). We varied the start of intervention between 20, 30 and 40 days after the initial attack. We defined ‘epidemic control’ as being able to reduce the daily number of new infected per infectious person, so in this study, an epidemic is defined under control when the infectious incidence is decreasing and we estimated the critical threshold proportion of case and contacts to be isolated and traced, respectively, to be able to reduce transmissions.9 The threshold value was also estimated at which epidemic control is lost9 through simulation of the model at values between 50% and 60% of case isolation and contact vaccination.
Supplemental material
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Results
The population of Mumbai is over 20 million. Mumbai has a very young population compared with developed countries, with 83% of the total population aged between 0 and 49 years,38 39 which is the age group with the highest transmission rates.8 We estimated 58 537 HCWs in Mumbai. We estimated there are 40 000+ hospital beds in Mumbai, with 50% of those beds in private hospitals.
Immunosuppressed population
We estimated a rate of 5.14% immunosuppression in India, with a higher percentage of immunosuppressed people in the 50+ age group (see online supplemental table 5) and the highest immunosuppression observed in persons 85+ years old.
Supplemental material
Impact of response time and interventions
For a fixed number of 1000 initial infected by the attack, with the best case scenario of 90% of contacts vaccinated and isolation of 90% of infectious cases (figure 1), at time to starting interventions of day 40 after the attack, the infectious incidence peaks at 1456 people and it takes over 176 days, respectively, to contain the epidemic. On day 40 of intervention, a total of 22 040 people will be infected, with a corresponding increase in required vaccine doses (table 1). A total of 2319 deaths by day 50, 7646 deaths by day 100 and 9472 deaths by day 150 will be observed when the intervention starts on day 40.

Epidemic response for 1000 initial attack at a fixed time of intervention T=40, with 90%, 70% and 50% of cases isolated and contacts traced and vaccinated.
Vaccine doses required for epidemic control with varying % of case isolated and % contacts traced and vaccinated
Figure 1 shows that as rates of case isolation and contact vaccination fall, the epidemic becomes more severe, with a large difference between 70% and 50% rates. If ring vaccination and isolation decreases to 50% of the contacts and cases, respectively (figure 1), the epidemic is more severe resulting in a very high infected and death rates with a very long period of the epidemic and a total of 761 900 people infected. The large difference between the two scenarios such as case isolation and degree of vaccination at 70% and 50% rates compared with 90% and 70% suggests that epidemic control is lost somewhere between 70% and 50%.
The epidemic impact was also examined at varying proportions each of case isolation and ring vaccination. With a decrease in the percentage of case isolation and vaccination, the infection and deaths incidence increase and the epidemic takes longer to control.
Duration of epidemic
Figure 2 illustrates the time to control the epidemic in Mumbai by varying rates of case isolation and ring vaccination, with initial attack size of 1000 infected people. The epidemic will end in less than half a year at 90% case isolation and ring vaccination rate, and, within 1 year at 70% of each rate. However, if the rates are 50% each, the epidemic will continue for more than 6 years, as shown in figure 2.

Epidemic duration with varying contact vaccination and case isolation rates.
Vaccine doses
A total of 16 813, 37 092 and 82 486 vaccine doses will be needed with 90% of each case isolation and ring vaccination, at time of intervention on day 20, 30 and 40, respectively. However, at 50% of each rate, a maximum of 2 228 600, 2 336 600 and 2 548 800 vaccines are needed at time of intervention on day 20, 30 and 40, respectively (table 1). Vaccine requirements for epidemic control more than double with every 10 days of delay in intervention at higher case isolation and vaccination (70% or 90%).
Hospital beds
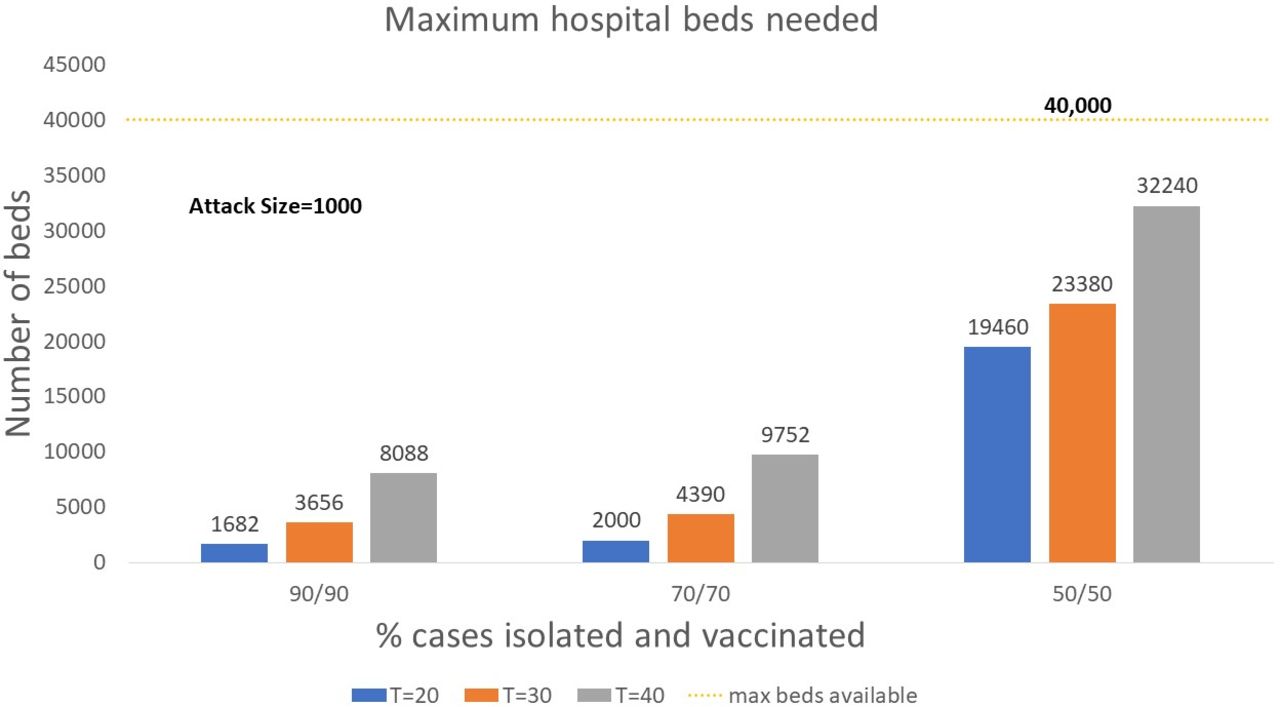
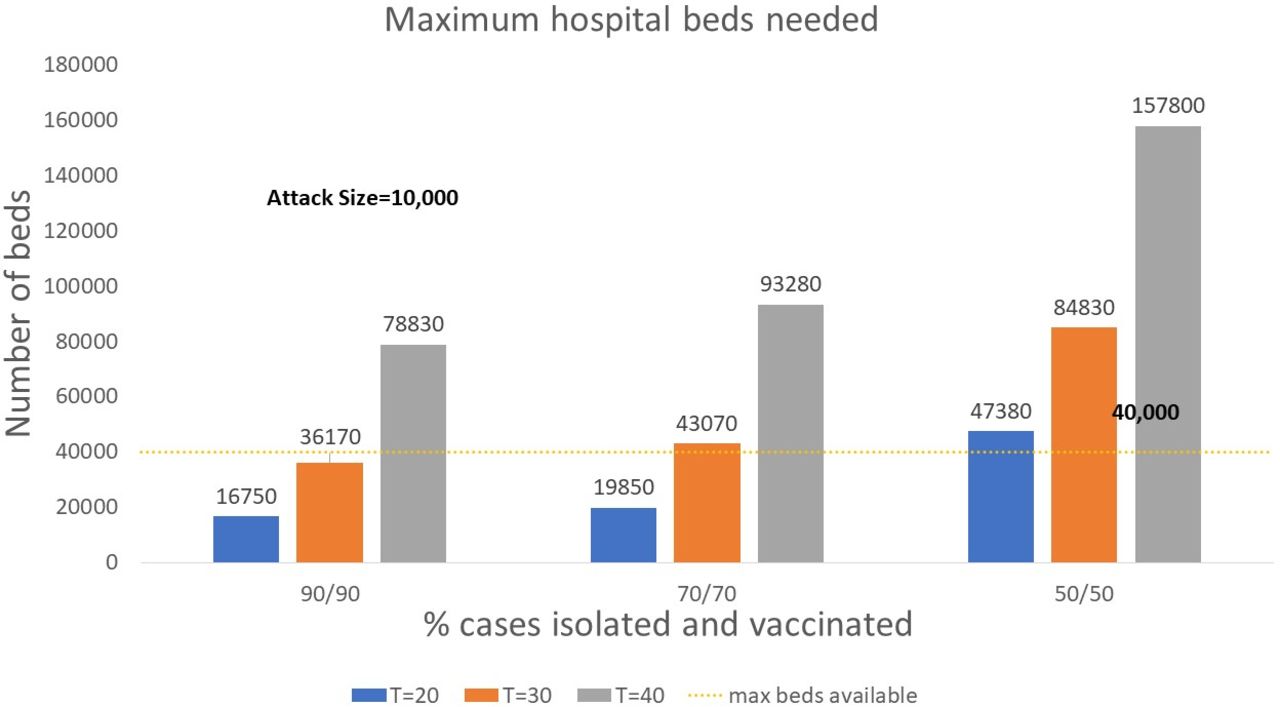
Figure 3 shows the maximum number of beds that will be needed in Mumbai by case isolation and contact vaccination rates, and time of starting interventions, for an attack size of 1000. The required hospital beds more than double with every 10 days of delay. In all the above cases, at the initial attack size of 1000, the maximum beds required do not exceed the total available hospital beds of Mumbai (40 000 beds). However, in the worst case, almost all beds will be used just for smallpox cases. Figure 4 shows that if the attack size is 10 000, available beds will be exceeded in almost all scenarios.

Maximum hospital beds needed under scenarios of different case isolation and contact vaccination rates, by time to response, for an attack size of 1000.
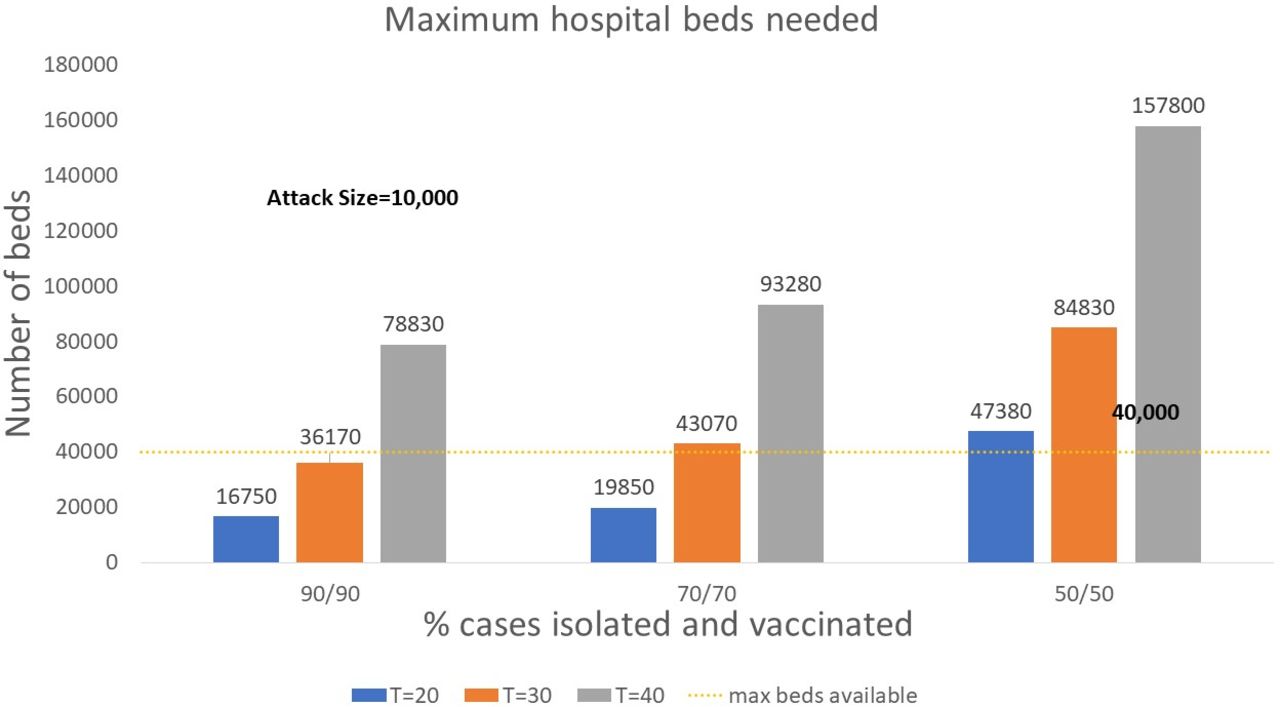
Maximum hospital beds needed under scenarios of different case isolation and contact vaccination rates, by time to response, for an attack size of 10 000 mixed scenario.
The threshold initial attack size found to be 5000 (at time of intervention T=40) above which the number of hospital beds needed exceeds available beds in Mumbai at 90% case isolation and 90% vaccination.
Mixed scenario
When the base case input parameters were used, with 1000 initial infected starting interventions after 30 days and assuming that 70% of cases presenting symptoms get isolated, reducing the contact traced percentage to 30% and 20%, the epidemic can still be controlled with 216 790 and 981 310 vaccination doses used, resulting in 55 402 and 380 584 deaths, respectively. However, in the case of only 10% of contacts traced for infected person, the epidemic is not controlled ending with 1 082 121 deaths using 1 337 100 vaccination doses. The results are shown in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Epidemic curve in the scenario with 1000 initial infected, starting intervention at T=30, assuming 70% of symptomatic people will get isolated and varying the percentage of contacts traced as 10%, 20% and 30%. Number of new infected symptomatic over time (left) and cumulative number of deaths (right).
Discussion
In the event of re-emergent smallpox in Mumbai, there are several approaches to mitigating the impact, which will be proportional to the size of the attack. Transmission of infection would be intense because Mumbai has high population density, a young population age structure, coupled with higher contact rates among younger people.4 66 Smallpox has a mean incubation period of 12 days, so that starting vaccination and case isolation at day 20 means, in reality, starting the response 8 days after the first case becomes symptomatic, which, even in the best-resourced country, would be a challenge. It is also likely that the diagnosis may be delayed, given the unfamiliarity of current clinicians with smallpox and many examples of missed or delayed diagnoses of serious infections, such as Ebola, Middle East Respiratory Syndrome (MERS) coronavirus and smallpox.67 Every 10 days of delay results in a worsening epidemic. However, diagnosing smallpox may not be that difficult given it is a typical clinical presentation including the centrifugal distribution of the rash, high fever, ocular complications.
Rapid response will depend on early diagnosis, availability of vaccine stockpiles, as well as physical and surge capacity including human resources for isolating infectious cases, tracking contacts and managing the epidemic. The influential predictors of epidemic size are initial attack size, time to start of the intervention, residual vaccine immunity and percentage of cases isolated, contacts traced and vaccinated. While the initial attack size is not within our control, factors that can be controlled include rapid response, high case isolation and high rates of contact tracing and vaccination. Achieving high case isolation and vaccination rates in Mumbai is critical, as failure to do so will increase the epidemic test the health system capacity. In scenarios with a delayed response, low case isolation and vaccination rates, the duration of the epidemic may be more than 6 years.
Due to high density and contacts number, a smallpox outbreak could infect hundreds of thousands of people in Mumbai in a very short time and, unless it is quickly controlled, it can easily spread to the rest of India and globally. This work shows the importance of rapid response, which includes vaccination, contact tracing and case isolation.
The already overstretched health infrastructure with respect to available healthcare workforce, hospital beds and health system capacity in a metropolitan area with a population over 20 million will be tested during any serious epidemic. There are over 40 000 hospital beds in Mumbai, with about 50% of these beds in private hospitals.33 42 The total available beds in Mumbai would not be exceeded in the best-case scenario, when the initial attack size is 1000 and the case isolation and vaccination is high. However, all scenarios will require surge capacity, and will affect the ability to provide care for other non-smallpox illness. With low case isolation or vaccination, or a large attack size, the maximum beds required will exceed the entire capacity very early in the epidemic. Given the large private hospital sector in India, coordination of pandemic planning with private hospitals may be important. India has a more privatised health system than many other countries, with at least 70% of care provided in the private sector.68 This is a challenge not just for epidemic control, but also for establishing representative disease surveillance across both public and private sectors.
The re-emergence of infectious diseases is a real possibility, not just due to synthetic biology and genetic engineering, but also due to laboratory accidents. In September 2019, a gas explosion occurred in one of the two sites known to house variola, The Russian State Research Centre of Virology and Biotechnology building (Vector) in the city of Koltsovo.69 Despite Russian government denials, there was a real risk of the aerosolized virus being propagated through shattered windows in the Vector building by the shock wave of the explosion69 and a need for preparedness. Koltsovo, where the explosion occurred is in the Southern part of Russia, bordering China, Mongolia and Kazakhstan and less than 2500 km from Jammu and Kashmir in India. Health system capacity for detecting unusual epidemics early and responding as rapidly as possible is critical. A rapid and well-coordinated response will require both physical space for case isolation and quarantine of contacts, as well as health workers and personnel for contact tracing and for accomplishing vaccination drives.9 While India has the potential for large the surge in personnel, this will require protection of health workers and incentivisation of community volunteers to conduct contact tracing and case finding. Enough vaccine should be reserved for the health workforce, as well as for community volunteers. During smallpox eradication, India was the most challenging setting, with the failure of mass vaccination attempts.70 When the strategy was switched to contact tracing and ring vaccination, community volunteers were paid financial incentives.17 This approach may be required in the event of smallpox re-emergence in India. The first Biosecurity Level (BSL) 4 laboratory in India, established in Pune, will enhance capacity for diagnostics and surveillance. A review of smallpox vaccine stockpiles and manufacturing capacity is also important. This study also has lessons for COVID-19 vaccination in India, as the incubation period is similar and it is also caused by a respiratory transmissible virus.
Limitations of this study include unavailability of some data, such as age-specific rates of organ transplants and autoimmune diseases for the Indian population. The age-specific distributions from other countries were adapted for India (such as incidence data of rheumatoid arthritis) to distribute organ transplants and autoimmune diseases for estimation of immunosuppression.27 However, we still used a minimum estimate of the immunosuppressed population and did not include diseases such as diabetes, malaria or the presence of malnutrition, all of which are highly prevalent in India and would worsen the impact of an epidemic. The contact matrix was derived from a study which estimated the age-specific contact rates for India.4 We estimated 70% of people over the age of 40 in India were vaccinated against smallpox before 1977.17 20 44 However, there is uncertainty around the degree of the waning of vaccine immunity.17 Finally, we looked at a large, densely populated city, Mumbai and studied the epidemic consequences. This may not be generalisable to other parts of India, as almost 70% of the population of India lives in rural areas and small towns where the transmission would be less intense because of lower population density. However, healthcare facilities, diagnostics and health workers are in short supply in rural areas.71 72 Further limitations are the lack of consideration of seasonality in the virus transmissions and vaccine refusal. We did not set a particular time of the year for the scenario tested, however, smallpox transmission varies with season and is most likely enhanced by dry weather.73 This could influence the outcomes of a smallpox outbreak in India, where there is only a dry and wet season. Regarding vaccine refusal, we did not account for this parameter in our study, although many recent outbreaks of vaccine-preventable diseases have been linked to under vaccinated communities.74 However, in India, accessibility due to long distances from healthcare facilities is the main factor linked to under-vaccination, but the level of vaccine acceptance is found to be still high,75 with only 16% of the vaccine-hesitant people refusing vaccination.76
Finally, for this study, we tested the sensitivity of results to variations in parameters involved in the public health response, such as contacts traced and cases isolated, time to start the intervention and number of doses delivered each day. This helps inform policy making for the most effective response within limited resources. However, we acknowledge that we could not vary every parameter involved and this can represent a further limitation.
Conclusion
In summary, we have shown a range of possible scenarios of re-emergent smallpox in Mumbai. Speed of response, stockpiling, vaccination, human resources for health and physical space for smallpox treatment and isolation are all influential factors. This study tells us that if smallpox reemergence occurs, it may have significant health and economic impact, the extent of which will depend on the availability and delivery of interventions such as a vaccine or antiviral agent, where these are needed the most, and the capacity of case isolation and treatment. Further research on health systems requirements and capacity across the diverse states and territories of India, across public and private health systems and inter-sectoral engagement especially the involvement of the community, could improve the preparedness and management strategies in the event of re-emergent smallpox or other serious emerging infections.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CRM designed the study and developed the research questions, supervised the research, drafted and revised the manuscript, gave final approval of the manuscript. VC participated in the literature review and study development, developed research questions, modelling analysis and drafted and revised the manuscript. BM conducted a literature review, collected the data, performed modelling analysis and drafted and revised the manuscript. AAC helped with the development of the study, participated in the literature review and manuscript drafting and revision. JN participated in the literature review, study development, drafted and revised the manuscript. AD collected the data, participated in the literature review and drafted the manuscript.
Funding Raina MacIntyre is supported by a NHMRC Principal Research Fellowship, grant number 1137582.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information. All data used in this study are publicly available online and listed in the references.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.