Article Text

Abstract
Introduction Major depression is a highly prevalent pathology that is currently the second most common cause of disease-induced disability in our society. The onset and continuation of depression may be related to a wide variety of biological and psychosocial factors, many of which are linked to different lifestyle aspects. Therefore, health systems must design and implement health promotion and lifestyle modification programmes (LMPs), taking into account personal factors and facilitators. The main objective of this protocol is to analyse the clinical effectiveness, cost-effectiveness and cost utility of an LMP and an LMP with information and communication technologies (ICTs) as adjunctive treatment for depression in primary care patients. The secondary objectives are to analyse the clinical effectiveness in the subgroup that presents comorbidity and to analyse the correlation between personal factors on health behaviour and lifestyle patterns.
Methods and analysis A randomised, multicenter pragmatic clinical trial with three parallel groups consisting of primary healthcare patients suffering from subclinical, mild or moderate depression. The following interventions will be used: (1) Usual antidepressant treatment with psychological advice and/or psychotropic drugs prescribed by the general practitioner (treatment as usual (TAU)). (2) TAU+LMP. A programme to be imparted in six weekly 90-minute group sessions, intended to improve the following aspects: behavioural activation+daily physical activity+adherence to the Mediterranean diet pattern+sleep hygiene+careful exposure to sunlight. (3) TAU+LMP+ICTs: healthy lifestyle recommendations (TAU+LMP)+monitoring using ICTs (a wearable smartwatch). The primary outcome will be the depressive symptomatology and the secondary outcomes will be the quality of life, the use of health and social resources, personal factors on health behaviour, social support, lifestyle patterns and chronic comorbid pathology. Data will be collected before and after the intervention, with 6-month and 12-month follow-ups.
Ethics and dissemination This study has been approved by the Clinical Research Ethics Committee of Aragón (approval number: C.P.-C.I. PI18/286) and the Research Ethics Committee of the Balearic Islands (IB3950/19 PI). Data distribution will be anonymous. Results will be disseminated via conferences and papers published in peer-reviewed, open-access journals.
Trial registration number ClinicalTrials.gov Registry (NCT03951350).
- depression & mood disorders
- clinical trials
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The intervention has the potential to be highly scalable and sustainable for the Spanish National Health Service.
Increased motivation, on introducing self-registers for everyone and a group that will be monitored using wearable smartwatches.
Most healthcare professionals can implement the intervention groups.
Some individuals may refuse to participate in group intervention or may withdraw from the study during the 12-month trial period.
Difficulty of entire group’s attendance to a session held on one specific date and time.
Introduction
Depression is considered to be the principle cause of disability worldwide, and it contributes to the overall global burden of morbidity and mortality. By 2030, it is expected to be the main contributor to the burden of morbidity.1–3 Approximately 25%–35% of all primary care patients suffer from psychiatric disorders, and over 80% of these patients suffer from depression or anxiety disorders.4 5 In Spanish primary healthcare centres (PHCs), the prevalence of depression ranges from 9.6% to 20.2%.6 7 Furthermore, depression generates great disability and high economic and social costs.8
The prevalence of depression in Spain is 13% over one’s lifetime and 4% per year.9 Indeed, comorbidity with other chronic conditions is high (64.9%–71.0%) (diabetes, hypertension, cardiovascular diseases and cancer, among others)10–12 as well as comorbidity with other psychiatric diseases such as anxiety disorders is also high (40%–66%).13
Despite the negative impact of depression on people’s lives and the existence of numerous treatment interventions,14 these interventions are often not appropriately used in PHC services,6 mainly due to physician time or resource limitations.7 Thus, pharmacological15 treatment is usually recommended, even though research has shown that in subclinical, mild or moderate depression, non-pharmacological interventions are recommended.15 16
Since options and outcomes for the care of individuals suffering from depression and their access to treatment remains limited,17 it is important to promote cost-effective treatment options. The onset and continuation of depression has been linked to numerous biological and psychosocial factors, many of which are related to distinct lifestyle aspects.18–21 Therefore, many of the strategies promoting a healthier lifestyle could have antidepressant utility.20 22–24 In addition to multimodal studies, others have focused on one of the following aspects of lifestyle modification: daily physical activity,25 adherence to the Mediterranean diet,26 27 sleep hygiene practices28 29 and careful exposure to sunlight.30 31
The present study will be framed around the theory of salutogenesis,32 which establishes that an individual’s ability to modify our lifestyle is influenced by psychosocial generalised resistance resources, which consist of personal, interpersonal or contextual resources (money, knowledge, experience, self-esteem, healthy habits, commitment, social support, cultural capital, intelligence, traditions and vision of life) and the sense of coherence (way of making sense of the world, which is a major factor in determining how well an individual manages stress and stays healthy).
Moreover, previous studies show that the use of facilitators is quite important (simplicity of guidelines, tailoring through motivational interviewing, prolonged and intense monitoring throughout the different stages of the disorder and the provision of adequate feedback and social support)23 to facilitate adherence to lifestyle modification programmes (LMPs). For example, enhanced motivation can be achieved through the use of information and communication technologies (ICTs) and with the social support resulting from intervention group participation.33 Personal factors and facilitators must be taken into account in lifestyle modification interventions, since they may determine the success of health promotion programmes.
The main objective of this protocol is to analyse the clinical effectiveness, cost-effectiveness and cost utility of an LMP and an LMP with ICTs as adjunctive treatment for depression in primary care patients. The secondary objectives are to analyse the clinical effectiveness in the subgroup that presents comorbidity and to analyse the correlation between personal factors on health behaviour and lifestyle patterns.
Methods and analysis
Study design
Multicenter pragmatic randomised controlled trial in three parallel groups.
Setting and study sample
We will recruit patients having subclinical, mild or moderate depression (scoring ≥10 and ≤30 points on the Beck II Self-Applied Depression Inventory (BDI-II))34 from PHCs of two Spanish areas (Zaragoza and Mallorca). Inclusion criteria: individuals over the age of 18, both sexes, having a duration of depression symptoms of at least 2 months, who understand written and spoken Spanish and who have provided their informed consent (online supplemental file 1). Exclusion criteria will be: suffering from another disease that affects the brain (organic brain pathology or having suffered a traumatic brain injury of any severity, dementia); having another psychiatric diagnosis or serious psychiatric illness (substance dependence or abuse, a history of schizophrenia or other psychotic disorders, eating disorders) with the exception of anxious pathology or personality disorders (collected through a medical history and from the Mini-International Neuropsychiatric Interview (MINI))35; presence of a serious or uncontrolled medical, infectious or degenerative illness that may interfere with the affective symptoms; the presence of delirium or hallucinations, risk of suicide, pregnancy or lactation; patients who have participated in another clinical trial over the past 6 months, who are currently in psychotherapy or those who have been practicing mindfulness, yoga, meditation or similar practices over the past 6 months, engaging in formal practice at least once a week and the presence of any medical, psychological or social problem that could seriously interfere with the patient’s participation in the study.
Supplemental material
Sample size
Scientific evidence suggests that a 17% reduction in the BDI-II34 is considered clinically relevant.36 In a previous study conducted by our team with psychiatric outpatients, we found that the average BDI score at the beginning of the study was 24.5 points (SD 9.8),22 so we consider that a reduction of at least 4.8 points would have clinical significance and would benefit the patient. Accepting an α risk of 0.05 and a β risk of 0.20 in a bilateral contrast, 44 subjects will be required for each group. With an estimated withdrawal rate of 20%, the sample size will require approximately 53 patients in each group. The total sample required is 159 subjects. A formula based on the Snedecor’s F distribution37 has been used (see online supplemental file 2). It is estimated that approximately 50% of these patients will present some physical or mental comorbidity.12
Supplemental material
Recruitment
General practitioners (GPs) from the PHCs of Zaragoza and Mallorca will be invited to refer patients who are suspected of suffering from depression. Most representative PHCs in the area will be invited, based on size, urban or rural area, and PHCs with a different sociodemographic profile will be selected. GPs will explain the characteristics of the study to their patients and if they agree to participate, they will be asked to provide a phone number to be contacted by a trained research assistant (RA) during the next week. The RA will call patients and establish an appointment in their PHC, in which he will explain them the study, provide them the patient information sheet and get the informed consent signed. To ensure that they fulfil the inclusion criteria, the RA will administrate the BDI-II34 and the MINI.35 If participants meet the criteria, the RA will administer the baseline questionnaires at the same appointment. Recruitment and baseline assessments will be carried out until the final sample size has been achieved.
Randomisation, allocation and masking of study groups
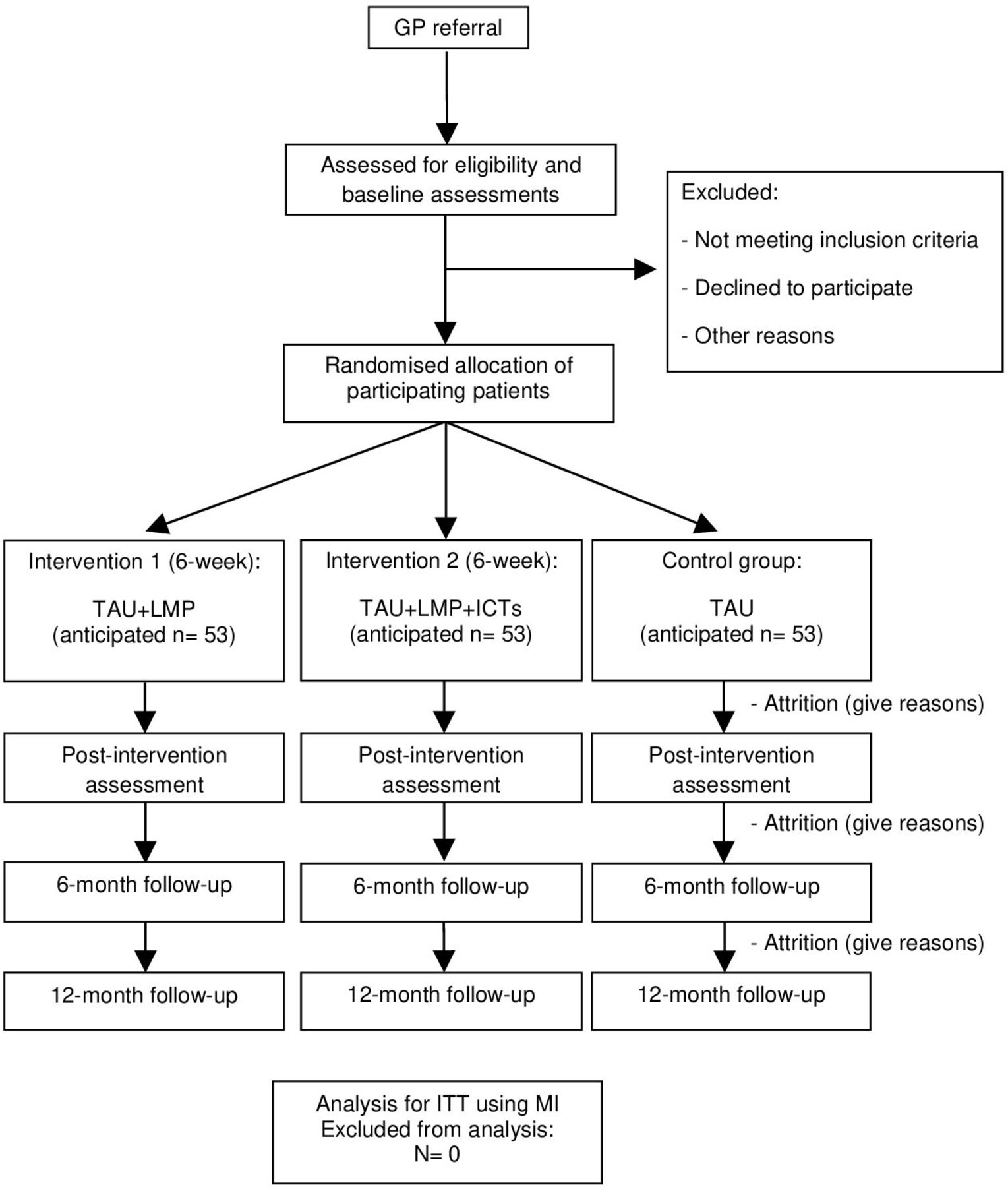
Once baseline data are collected, the participants will be randomised. An independent statistician will perform the individual randomisation using a computer-generated random number sequence. The randomisation will be carried out using a list of patients from Zaragoza and Mallorca (figure 1). Given the nature of the interventions, participants will not be blinded to their allocation. An RA will call them to explain their assigned intervention and where they should go and when. The RA will request that participants not to inform other researchers of their allocation.

{kind=link}
Flowchart of the study: randomisation, sampling and monitoring of patients. GP, general practitioner; ICTs, information and communication technologies; ITT, intention to treat; LMP, lifestyle modification programme; MI, multiple imputation; TAU, treatment as usual.
Data collection and monitoring
One RA will collect the data and another will perform entry and coding of the identified data. All RA managing the data will be blinded to participant allocation, as well as the RA conducting the outcome assessments and data analysis. All information collected will be treated in accordance with the provisions of current legislation on personal data protection.
The study will not have a formal data monitoring committee since adverse intervention events have not been reported. Any serious unexpected adverse events or outcomes will be discussed by the trial management committee (identical to the authors of this protocol). There are no plans to discontinue or modify interventions, or to improve adherence or promote participant retention. The trial management committee will monitor recruitment, treatment and attrition rates and any concerns related to the study. Reasons for dropping out will be also registered. Concomitant care is permitted and registered as long as it is not one of the exclusion criteria. Group-specific processes will be taken into account and will be evaluated and informed, in accordance with recommendations of the ‘mechanisms of action in group-based interventions’ (MAGI) framework.38
Intervention development and evaluation
Patients allocated in the first arm (control group) will follow the usual treatment provided by their GP (treatment as usual (TAU)).
Patients allocated in the second arm (first intervention group) will follow the TAU and the LMP. This programme will consist of six weekly group sessions (lasting 90 min each) led by an experienced psychologist and complemented by PowerPoint presentations.
Patients allocated in the third arm (second intervention group) will follow TAU and LMP and will be monitored using a wearable smart wristwatch that will track their daily sleep patterns and physical activity (LMP+ICTs).
The group sessions will consist of the following content:
Presentation of the project and psychoeducation on depression: presentation of the project and a review of the study objectives. Definition, symptoms, causes, consequences of depression and, also, how lifestyles and social environment changes influence the symptomatology of depression.
Behaviour activation: a psychologist will provide information on the importance of establishing, maintaining and monitoring activities. For the LMP+ICTs group, they will also learn how to use the smart wristwatch, ensuring all participants are able to use it.
Sleep hygiene habits and careful exposure to sunlight: recommendations on healthy sleep habits, factors influencing sleep quality and possible solutions. The benefits of careful exposure to sunlight and recommendations of when to do so and for how long. Responding to questions regarding the previous session.
Physical activity: the benefits of engaging in regular physical activity. Personalised recommendations about what physical exercise may be practiced, how and when to do so. Responding to questions regarding the previous session.
Adherence to the Mediterranean diet: explanations about the Mediterranean diet, food groups and their characteristics, as well as the most beneficial foods for physical and mental health, how to cook it and food-related habits. Responding to questions regarding the previous session.
Summary of previous sessions with practical final suggestions: personalised experiences and doubts of the participants throughout the course. Recommendations for daily healthy lifestyle practices for the future and farewell.
At the end of each session, the participants will receive a paper with self-registration tables (online supplemental file 3). They will complete the tables with the information on their daily routines regarding the modification of lifestyles on which they have been instructed. They will be asked about when they wake up and when they go to bed, the duration of their sleep, the time spent exposed to sunlight, the diet pattern, the physical activity and sports practiced, the social support and the subjective perception of satisfaction after these activities. A qualitative study associated with this study will be included to analyse the participants' difficulties in following the intervention.
Supplemental material
Outcomes and measures
We will collect patient data using the questionnaires administered in baseline, immediately after the intervention (in a period of 2–7 days after the last intervention session) and at 6-month and 12-month follow-up after the last intervention session (with a margin of ±2 weeks) (see table 1). A blinded RA will call each patient of the three arms and set up an appointment in their PHC for questionnaire administration. Study outcomes and measures are summarised in table 1.
Study variables
Sociodemographic data
We will collect information on gender, age, marital status, education, occupation and economical level. These data will be collected through an ad hoc questionnaire.
Primary outcome
Severity of depression
The primary outcome will be measured using the BDI-II.34 This is a self-report inventory for measuring the severity of depression, consisting of 21 multiple-choice questions with each answer being scored on a scale ranging from 0 to 3. It was translated and validated into Spanish with a reliability of 0.89.39 The standardised cutoffs are: 0–13: minimal depression; 14–19: mild depression; 20–28: moderate depression and 29–63: severe depression.
Secondary outcomes
Health-related quality of life
Health-related quality of life will be measured using the European Quality of Life-5 Dimensions Questionnaire (EQ-5D).40 41 EQ-5D scores will be used to calculate the quality-adjusted life year (QALY) during the monitoring period by adjusting the length of time affected by the health result by the utility value. It contains five health dimensions (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) and each of these has three levels (no problems, slight problems or moderate and severe problems). The EQ records the patient’s self-rated health on a vertical Visual Analogue Scale (VAS) of 20 cm, where the endpoints are labelled ‘The best health you can imagine’ and ‘The worst health you can imagine’. The VAS can be used as a quantitative measure of health outcome that reflect the patient’s own judgement. Patients mark the point on the vertical line that best reflects their assessment of their current global health status.42 Cronbach’s alpha coefficient has been calculated in research with disease-specific populations. We highlight the study of Seoane et al43 in which the overall alpha value was 0.788. Being the only study with a general population, it provides an overall mean estimate of the minimum important difference for the EQ-5D, which is 0.074.44
Comorbidity with chronic diseases
Comorbidity with chronic diseases will be determined according to the International Classification of Diseases, Tenth Revision45: diabetes (glucose concentration (mg/dL), glycated haemoglobin (%), creatinine, arterial hypertension and diseases of lipid metabolism. In patients with chronic heart disease, coagulation variables will be added. They will be collected from the last blood test or control measurements of the clinical history, taken by their GP or nurse (assuming they were taken over the past 3 months). Otherwise, their GP will be asked for a blood control test. It is estimated that approximately 50% of these patients will present some comorbidity.12 Anthropometric measures will also be collected (weight, size and perimeter of the waist).
Social support
It will be measured by the Medical Outcomes Study Social Support Survey (MOS-SS).46 It is a self-report instrument consisting of four subscales (emotional/informational, tangible, affectionate and positive social interaction) and an overall functional social support index. It has a good reliability (Cronbach’s alpha ≥0.91) and is quite stable over time. It has 19 items, a 5-point Likert Scale. Higher scores indicate more support. We will use the Spanish validated version.47
Use of health and social services
It will be measured using the Client Service Receipt Inventory.48 These data may be used for a wide range of applications, including estimates of the costs of service receipt. To collect information on the entire range of services and supports used by study participants. It retrospectively collects data on the use of services over the past 6 months (eg, rates of use of individual services, mean intensity of service use, rates of accommodation use over time). We will use the validated Spanish version.49
Assessment of lifestyle
Physical activity
Physical activity will be measured using the International Physical Activity Questionnaire-Short Form (IPAQ-SF).50 It assesses the levels of habitual physical activity over the last 7 days. It has seven items and records the activity of four intensity levels: vigorous-intensity activity and moderate-intensity activity (walking and sitting). We will use the validated Spanish version.51 IPAQ-SF has acceptable validity for the measurement of total and vigorous physical activity and poor validity for moderate activity and good reliability.52
Adherence to the Mediterranean diet
Adherence to the Mediterranean diet will be measured using the 14-item Mediterranean Diet Adherence Screener (MEDAS), developed within the prevention with Mediterrean diet (PREDIMED) study group.53 It includes items on food consumption and intake habits: the use of olive oil as the main source of cooking fat, preference for white meat over red meat, servings of vegetables, portions of fruit, red meat or sausages, servings of animal fat, sugar-sweetened beverages, red wine, legumes, fish, commercial pastries and dressing food with a traditional sauce made of tomatoes, garlic, onion or leeks sautéed in olive oil. The total score ranges from 0 to 14, with a higher score indicating a better accordance with the Mediterranean diet.54
Quality and patterns of sleep
Quality and patterns of sleep will be measured using the Pittsburgh Sleep Quality Index (PSQI).55 It differentiates between ‘poor’ and ‘good’ sleep by measuring seven domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication and daytime dysfunction over the past month. It consists of 19 self-applied questions and five questions that request the evaluation of the patient’s bedmate or roommate (these are not scored). Answers range from 0 (no difficulty) to 3 (severe difficulty). The overall score ranges from 0 to 21 points. In its Spanish version, the Cronbach’s alpha coefficient is 0.81, sensitivity is 88.63% and specificity is 74.99%. We will use the validated Spanish version.56
Personal factors on health behavior
We will assess: (1) self-efficacy57; (2) activation58; (3) sense of coherence59; (4) health literacy60 and (5) procrastination.61
Self-efficacy
Self-efficacy will be measured using the Self-Efficacy Scale.57 To measure General Self-Efficacy Subscale (17 items including individuals' beliefs in their ability to perform well in a variety of situations) and Social Self-Efficacy Subscale (six items). It contains 23 items that are rated on a 14-point scale (ranging from strongly agree to strongly disagree). Higher scores indicate higher levels of self-efficacy. It has a Cronbach coefficient alpha of 0.86 for General Self-Efficacy Subscale and 0.71 for the Social Self-Efficacy Subscale. The unpublished Spanish version was translated by Godoy in 1990.62
Patient activation in their own health
Patient activation in their own health will be measured using the Patient Activation Measure (PAM) Questionnaire with regard to the management of their health.58 It evaluates the patient’s perceived knowledge, skills and confidence to engage in self-management activities. It has 13 items with a Likert Scale from 1 (strongly disagree) to 4 (strongly agree). The resulting score (between 0 and 100) places the individual at one of four levels of activation, each of which reveals insight into a range of health-related characteristics, including behaviours and outcomes. Higher scores indicate higher levels of activation.58 This scale is only validated in Spanish for chronic patients. It had an item separation index for the parameters of 6.64 and a reliability of 0.98.63
Sense of coherence
Sense of coherence will be measured using the Sense of Coherence (SOC-13) Questionnaire by Antonovsky.59 It values the personal disposition towards the assessment of vital experiences. It measures the sense of coherence, comprehensibility, manageability and meaningfulness. It has 13 items scoring between 13 and 91 points. It has consistency rates between 0.84 and 0.93. Higher scores (after reversal of the inverted items) indicate a higher sense of coherence. We will use the validated Spanish version.64
Health literacy
Health literacy will be measured using the Health Literacy Europe Questionnaire (HLS-EUQ16).60 It can indicate that the probability of functional literacy in limited health is high, a possibility of functional literacy in limited health, and functional health literacy in adequate health. It contains 16 items. Higher scores indicate better health literacy. It presents a high consistency (Cronbach’s alpha of 0.982) in the Spanish validation.65
Procrastination
Procrastination will be measured using the Irrational Procrastination Scale (IPS).66 To measure general procrastination (dysfunctional delay). It has nine items, rated on a 5-point Likert Scale, with higher scores (after reversal of the three procrastination-inconsistent items) indicating a higher level of procrastination. Its Cronbach’s alpha value is 0.90. We will use the validated Spanish version.61
Data analysis plan
Analysis of the outcomes at baseline
First, descriptive analyses of all the variables (proportions for qualitative variables, means and SD for quantitative variables) will be performed. Then, correlation analysis will be carried out between the questionnaires that evaluate personal factors on health behaviour (Self-Efficacy Scale, PAM, SOC-13, HLS-EUQ16 and IPS), social support (MOS-SS) and depression (BDI-II). We will also analyse the correlation between personal factors on health behaviour and the questionnaires assessing lifestyle patterns (IPAQ-SF, MEDAS and PSQI). Finally, we will analyse the relation of lifestyle patterns and social support with depression. Inferential statistical analysis will be carried out using the χ2 test for qualitative variables, and Student’s t-test or one-wayanalysis of variance (ANOVA) test to assess the potential relationship between qualitative and quantitative variables.
Data collection and statistical analysis will be performed using Excel software, SPSS software (V.25.0)67 and the R statistical software environment (V.3.6.2).68
Clinical effectiveness analysis
The report of the results will follow a prespecified plan, based on the Consolidated Standards of Reporting Trials guidelines69 in order to compare the three groups using an intention-to-treat analysis and multiple imputation (MI) technique for handling missing data. Initially, a descriptive comparison (proportions, means or medians) will be carried out between groups for prognostic variables in order to establish their baseline comparability after randomisation. To analyse the clinical effectiveness, a repeated-measure linear regression will be conducted, including all evaluations over time. For this purpose, the main variable, BDI-II score, will be used as a continuous variable. The models will include adjustments for the baseline value of the BDI-II and for any other variable that would have shown differences in the baseline measurement. Possible group per time interactions will be examined using linear regression. Similar analyses will be carried out using the secondary outcomes (personal factors on health behaviour and assessment of lifestyle). To counteract the problem of multiple comparisons, we will use Bonferroni correction.
Comparisons will also be made between the LMP and LMP+ICTs groups regarding adherence to lifestyle modification requirements. Adherence will be considered as a good or beneficial score on the questionnaires assessing lifestyle patterns (IPAQ-SF, MEDAS and PSQI). In addition, we will compare the LMP and combined LMP+ICTs groups, assuming that they are comparable to each other and the two groups have significant results.
A binary variable regarding comorbidity will be created (comorbidity yes/no). We will determine if the effectiveness of the intervention differs in the subgroup presenting comorbidity and if the pathology improves. Statistical analyses will be selected based on subsample size (parametric or non-parametric tests).
As for the timepoint in which we administrate the follow-up questionnaires, we will consider the first follow-up assessment (in a period of 2–7 days after the last session of the intervention) as more relevant. We expect to find an immediate effect in the LMP and LMP+ICTs groups after attending group intervention, due to the potential social support received. In the 6-month and 12-month follow-up, we expect a beneficial change in the questionnaires assessing lifestyle, reflecting a long-lasting effect.
Cost-effectiveness and cost-utility analysis
The effectiveness of the interventions will be estimated using the difference between the BDI-II baseline score and the score at the 6-month and 12-month follow-ups, and utility will be estimated using QALYs at the 6-month and 12-month follow-ups. QALYs will be calculated based on these scores using the Spanish EQ-5D tariffs.70 Along with the EQ-5D utility scores, scores recorded on the EQ VAS will also be used as an outcome for the analysis.
Cost-effectiveness will be explored through the calculation of incremental cost-effectiveness ratios (ICERs) for the active intervention groups (LMP and LMP+ICTs) using the TAU group as the control. ICER is defined as the ratio between incremental costs and incremental effectiveness. In this way, cost utility will be explored by calculating incremental cost-utility ratios, which are defined as the ratio between incremental costs and incremental utilities measured on QALYs. QALYs gained in each evaluation are approximated using the area under the curve technique.71
Total costs will be calculated by adding direct and indirect costs. Direct costs will be calculated by adding the costs derived from the medication and the use of health services and clinical tests. The medication costs will be calculated by determining the price per milligram during the study period according to the vade-mecum of the last year of study, including value-added tax. The total cost of drug treatment will be calculated by multiplying the price per milligram by the daily dose in milligrams and the number of days the treatment is received. Costs derived from the use of health services will be calculated considering the data from the Oblikue database.72 Indirect costs will be calculated based on the sick leave days and multiplying them by the Spanish minimum daily wage during the study period, 2019–2020.
We assume that data will be missing at random. Only patients with both cost and relevant outcome data at the 6-month and 12-month follow-ups will be included in the cost-effectiveness and cost-utility analyses. Notwithstanding this, sensitivity analysis imputing missing 6-month and 12-month data will test the robustness of cost-effectiveness and cost-utility results. The imputations will be performed using the ‘mice’ package,73 freely available in the Comprehensive R Archive Network (CRAN-R).68
Discussion
Depression is a significant cause of morbidity having low detection and treatment rates in primary care.74 75 Only 9% of all depressed primary care patients receive adequate treatment, and only 6% achieve remission, making depression an important management issue in primary care.76 An effective treatment for depression that can be implemented in PHCs is brief psychotherapy (six to eight sessions programmes), which have the advantage of being performed by either mental health professionals or trained non-mental health providers.77 In this case, the promotion of healthy lifestyles will be used to address depressive symptoms, as it has shown efficacy in a number of studies.20–31 To ensure treatment adherence, facilitators should be used, such as the use of ICTs and the group format. They provide monitoring and social support, respectively.33 Organising group therapies in PHCs generates a range of organisational benefits, in relation to efficient use of facilities, high therapist-to-patient ratios and potential reductions to treatment wait times.78 Moreover, participants are just as likely to engage in group treatment as individual work and the benefits are also maintained over time.79
The strengths of this study include the design and the wide range of outcome measures. It will provide a wealth of information on the interplay between depression, personal factors on health behaviour and lifestyles. Study limitations include the possible attrition of participants due to session scheduling or participant refusal to participate in a group intervention or do the complete follow-ups.80 However, the possible reasons for attrition and other issues will be registered regarding MAGI framework.38
Therefore, the creation of a six-session group programme addressing lifestyle modifications (plus testing the monitoring with ICTs by adding a smartwatch to one of the intervention group) appears to be a good choice for depression treatment. The long-term aim of this study is to establish intervention for patients with depression, making it accessible in their PHCs, effective and cost-effective.
Execution dates
Initial recruitment of patients: April 2020.
Finalisation of patient recruitment: May 2020.
Finalisation of patient monitoring period: June 2021.
Publication of results: July 2021.
Partial patient and public involvement (PPI)
PPI representatives worked with us to refine the research question; however, it was difficult to involve patients in other areas of the study design due to data protection restrictions and the very technical methods required to do a data linkage analysis. PPI representatives will write a plain language summary and design a leaflet for dissemination to their peers and distributing to patient groups.
Ethics approval
Ethics approval was granted by the Clinical Research Ethics Committee of Aragón (PI18/286) and the Research Ethics Committee of the Balearic Islands (IB3950/19 PI). The study has been developed in accordance with the Declaration of Helsinki. All of the subjects will sign an informed consent form, their data will be anonymised and will only be used for the purposes of the study. Participants and healthcare professionals will be informed about the results. Patients of the TAU group will be invited to participate in the LMP at the end of the study. The ethics committee will be notified of any protocol modifications.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the Primary Care Prevention and Health Promotion Network (RedIAPP-Health Institute Carlos III, Spain), Primary Health Care Research Group of Aragon (GAIAP-B21-17R) of the Department of Science, University and Knowledge Society of the Aragon (Spain) government and FEDER Funds ‘Another way to make Europe’.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors BO-B, M-JS-R and MG-T designed and developed the study and had the original idea. RMB, M-JS-R, CN and BO-B coordinated the fieldwork. AA-L and CCV undertook the fieldwork. AA-L, BO-B, EG and SB wrote the first draft of the article. The rest of the signing authors have read the manuscript critically, offering contributions and approving the final version. BO-B attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding This work was supported by Carlos III Health Institute grant number PI18/01336, FEDER Funds ‘Another way to make Europe’. The funders have no role in study design, data collection and analysis, decision to publish or manuscript preparation. The funding body will conduct audit trial once a year.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.