Article Text

Abstract
Objective To undertake a case review of deaths in a 6-week period during the COVID-19 pandemic commencing with the first death in the hospital from COVID-19 on 12th of March 2020 and contrast this with the same period in 2019.
Setting A large London teaching hospital.
Participants Three groups were compared: group 1—COVID-19-associated deaths in the 6-week period (n=243), group 2—non-COVID deaths in the same period (n=136) and group 3—all deaths in a comparison period of the same 6 weeks in 2019 (n=194).
Primary and secondary outcome measures This was a descriptive analysis of death case series review and as such no primary or secondary outcomes were pre-stipulated.
Results Deaths in patients from the Black, Asian and minority ethnic (BAME) communities in the pandemic period significantly increased both in the COVID-19 group (OR=2.43, 95% CI=1.60–3.68, p<0.001) and the non-COVID group (OR=1.76, 95% CI=1.09–2.83, p=0.02) during this time period and the increase was independent of differences in comorbidities, sex, age or deprivation. While the absolute number of deaths increased in 2020 compared with 2019, across all three groups the distribution of deaths by age was very similar. Our analyses confirm major risk factors for COVID-19 mortality including male sex, diabetes, having multiple comorbidities and background from the BAME communities.
Conclusions There was no evidence of COVID-19 deaths occurring disproportionately in the elderly compared with non-COVID deaths in this period in 2020 and 2019. Deaths in the BAME communities were over-represented in both COVID-19 and non-COVID groups, highlighting the need for detailed research in order to fully understand the influence of ethnicity on susceptibility to illness, mortality and health-seeking behaviour during the pandemic.
- coronavirus
- COVID-19
- ethnicity co-morbidity deprivation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Large timely analysis from detailed case note review by independent medical examiners capturing data from all deaths (intensive care and ward-based care) in the hospital.
All swab-positive deaths associated with COVID-19 were included and compared with non-COVID deaths and historical data from the previous year.
We identified important ethnic differences with increased mortality in the Black, Asian and minority ethnic communities in both COVID-19 and non-COVID deaths in the early weeks of the pandemic.
The principle limitation was that this was a single-centre study and focused on hospital mortality data alone and not out of hospital deaths and therefore the full picture of regional mortality could not be ascertained.
All such studies are limited by the quality of the clinical records and in particular detailed data about the demographics of the whole admission population.
Introduction
COVID-19 emerged in Wuhan, China, at the end of 2019, before spreading around the world with devastating effects. In the city of Nembro, Northern Italy, the all-monthly all-cause mortality rose from 10 per 1000 person-years to a peak of 154.4 per 1000 person-years.1 In New York, over an 8-week period, a total of 32 107 deaths were reported, of which 24 172 were found to be in excess of the seasonal expected baseline.2 The first case was recorded in the UK on 31st of January 2020 and in London on the 12th of February 2020. The first UK fatality was reported on the 28th of February 2020. As the pandemic spread across the world, a number of at-risk groups have been identified: Black, Asian and minority ethnic (BAME) groups,3 men, the elderly and those with pre-existing comorbidities, particularly diabetes mellitus, hypertension and ischaemic heart disease.4 5
The BAME communities make up 14% of the population of England and Wales in the 2011 England and Wales census, but represent 17% of deaths as of the 28th of April 2020 in England6 and 35% of those who have been admitted to intensive care units as of the 1st of May 2020.7 The UK government has committed to Public Health England undertaking a review investigating why BAME communities are disproportionately affected. The BAME communities are known to have a higher prevalence of specific cardiometabolic risk factors, including diabetes, hypertension, ischaemic heart disease and stroke.8 The BAME communities also experience higher rates of poverty. In London, the poorest boroughs (Newham, Brent and Hackney) have had the highest COVID-19 mortality per 100 000 population. Conversely, the BAME communities are, on average, younger than the white population in the UK. In the 2011 England and Wales census, the median age by ethnic group was: white, 41 years; Asian, 29 years and Black, 30 years.9 Given the mortality from COVID-19 increases significantly with age, the over-representation of the BAME communities when age adjusted, is likely to be even more pronounced.
COVID-19 mortality is significantly higher in men, whose life expectancy is also shorter than women (79.3 years vs 82.9 years).10 The reason for the excess mortality in men is also uncertain and it has been postulated that it is related to the increased prevalence of comorbidities in men than women, and to the higher smoking rates (16.5% vs 13.0%).11
St George’s University Hospital NHS Foundation Trust is one of the largest hospitals in the UK and is based in South West London. It serves a local catchment population of 560 000 and specialist services to 3.4 million people in South West London. A national system of medical examiners is being rolled out in England and Wales to provide much-needed scrutiny of deaths, support for bereaved families, to improve patient safety, and to improve death certification and data accuracy. This service reviews case notes and agrees cause of death with the clinical teams. The service is in a unique position to collect timely prospective and consistent mortality data. The first death from COVID-19 occurred on the 12th of March 2020. In this paper the medical examiner team reviewed the 6 weeks of mortality data at St George’s Hospital from this date, comparing it with deaths taking place in the same 6 weeks of 2019 as a comparison group.
Methods
Participants
The mortality data for deaths occurring at St George’s Hospital for the 6 weeks commencing 12th of March 2020 were collated. Deaths in this period were divided into two groups. Group 1 were the COVID-19-associated deaths where COVID-19 had been identified by a positive swab, and in all cases COVID-19 was declared on the death certificate. Group 2 were non-COVID deaths in the same period with no patients in this group having swabbed positive for COVID-19. The comparison groups were patients who had died at St George’s during the same 6 weeks from 12th of March in 2019.
Data available included sex, age, postcode of residence at time of death, declared ethnicity and cause of death. The electronic medical record was reviewed to identity the presence of specific comorbidities: diabetes mellitus, ischaemic heart disease and hypertension. Ethnicity was categorised as White, Black, Asian, Other (including mixed) and not specified or known.
The postcode was used to identify the Index of Multiple Deprivation (IMD) decile using the 2019 IMD data. England is divided into 32 844 Lower-layer Super Output Areas (LSOAs) and the relative level of deprivation in each LSOA has been determined using a multi-faceted metric.12 The LSOAs are ranked from first (most deprived) to last, and then turned into deciles of deprivation, with decile 1 being the most deprived and decile 10 the least.
Patient and public involvement
This was a retrospective analysis of mortality in a large London centre in the first phases of the COVID-19 pandemic. This was a description of the data and analysis of routinely collected data. Patients and the public will be involved in dissemination of these data in order to inform local management and policy.
Statistical analyses
Data were anonymised prior to analysis. There were no missing data for age or sex. The IMD was unknown in two cases and ethnicity either not known or not stated for 103 of the 573 cases analysed. Cross tabulations of the risk factors for COVID-19 mortality were undertaken by group. Statistical comparisons were made using Χ2 tests for categorical variables and t-tests (normally distributed) or Wilcoxon rank-sum tests (non-normally distributed such as age) for continuous variables as appropriate. An adjusted logistic analysis was undertaken to establish the independent effects of ethnicity, sex, comorbidities and deprivation on COVID-19 mortality, adjusting for age. Analyses were undertaken using Stata V.15 (Stata Corp, Texas, USA).
Results
In the 6-week period from 12th of March 2020 there were 243 deaths among patients with confirmed COVID-19 (group 1) and 136 deaths from non-COVID causes (group 2) at St George’s Hospital (table 1). The total number of deaths in this period in 2020, 379, significantly exceeded the 194 deaths in the same 6 weeks in 2019 (group 3) (comparison of average weekly death rates, p<0.001). The COVID-19 weekly death rate alone exceeded the 2019 weekly death rate. In contrast, there was a marked reduction in the non-COVID weekly death rate in 2020 and it was significantly lower than the 2019 weekly death rate (p=0.03).
Demographics and risk factor distribution by group
That the lower weekly death rate from non-COVID causes in 2020 was not an anomaly is demonstrated in figure 1, where the average weekly death rate in the 6 weeks preceding 12th of March 2020, 29 deaths/week, was similar to the 2019 weekly average death rate of 32 deaths/week (p=0.26). Furthermore, while the COVID-19 weekly deaths peaked in the week commencing 2nd of April 2020, the weekly death rate from non-COVID causes continued to diminish across the 6-week period, reaching less than half (14 deaths) of the normal weekly rate by the final week of the period.

Weekly death rate in the 6 weeks up to the first COVID-19 death followed by the first 6 weeks' mortality during the pandemic at St George’s Hospital.
Sex
While there was no significant difference in the sex ratio for non-COVID deaths in 2020 (group 2) or 2019 (group 3), men were significantly more likely to have died of COVID-19 (67% (162/243), p<0.0001) (table 1). The excess of men among those dying of COVID-19 was present in every ethnic group (data not shown).
Age distribution
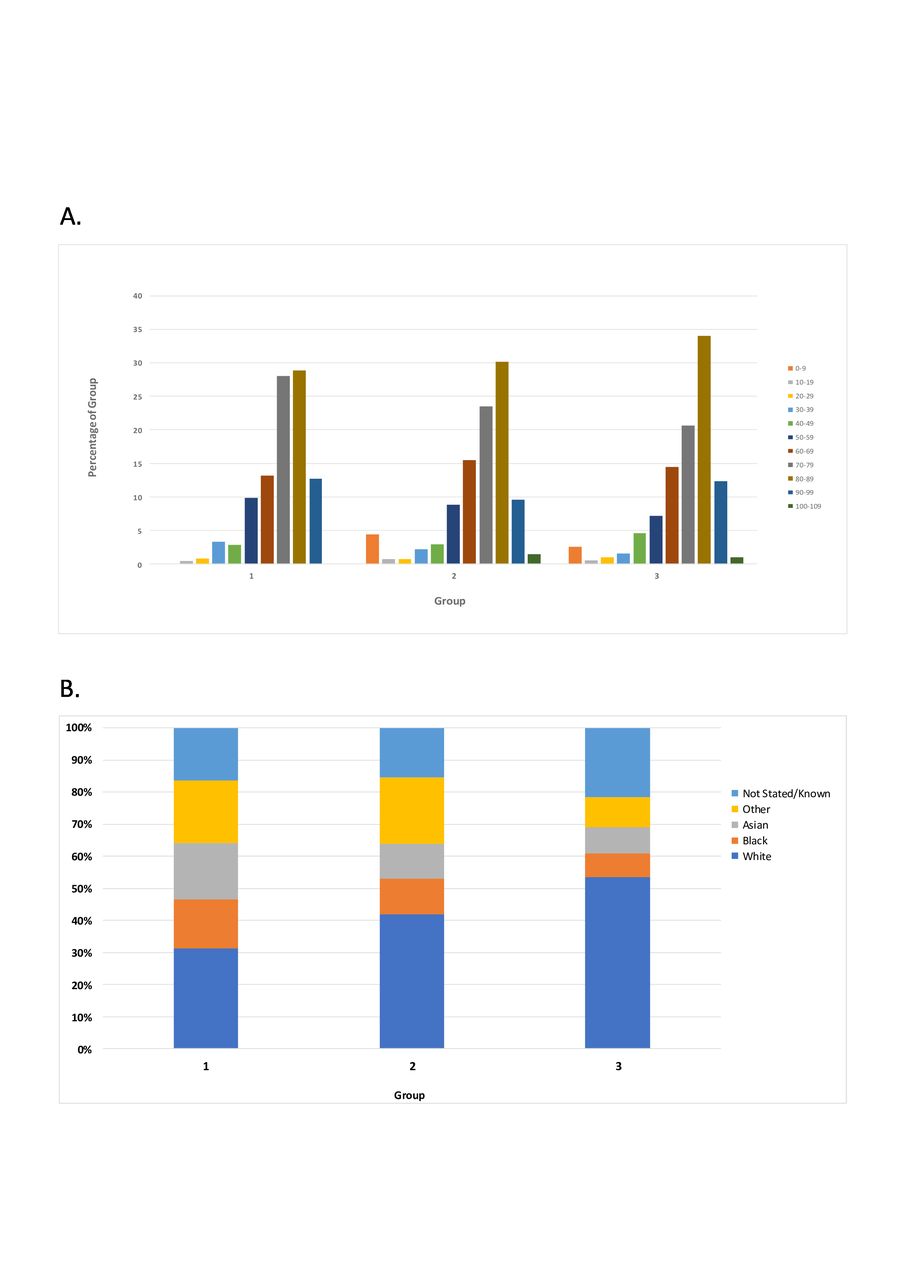
There was no significant difference in the median age of death between the three groups (table 1). Looking at the distribution of ages within each group, the distribution was notably similar in all three groups (figure 2A). Hence, there was no suggestion that the elderly were disproportionately represented in the hospital COVID-19 deaths compared with deaths from other causes in either 2020 or 2019.
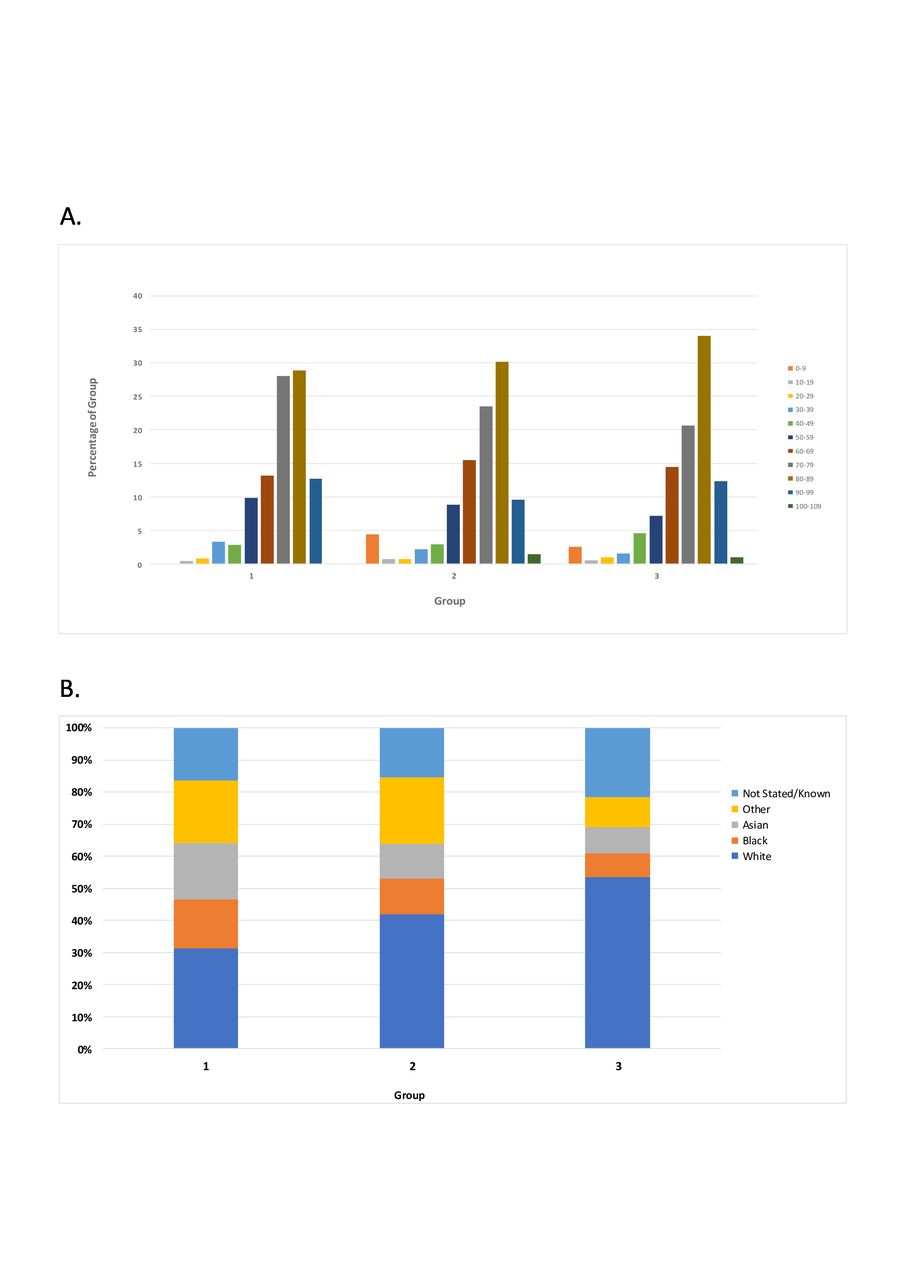
Relative age distribution (A) and ethnic distribution (B) in each of the three groups. Group 1: COVID-19 deaths (2020); group 2: non-COVID deaths (2020); group 3: all deaths (2019).
The median age of death in the three groups combined, varied with ethnicity. The median age of death among the 573 cases was: white, 80 years; Asian, 71 years (p<0.001 vs white); Black, 77 years (p=0.05 vs white); Other, 76 years and Not known/not stated, 74 years. In contrast, there was no significant difference within ethnic groups in median age of death comparing those dying of COVID-19 or non-COVID causes in 2020, with the median age of death in 2019 (table 1).
Declared ethnicity
Compared with deaths in 2019 (46% (90/194) non-white), non-white ethnic groups were significantly over-represented among non-COVID deaths in 2020 (58% (79/136), p=0.04), but particularly among COVID-19 deaths (69% (167/243), p<0.001). This over-representation was most marked among the Asian and Black ethnic groups (figure 2B).
Deprivation
There was a difference in IMD distribution between the three groups (table 1). While non-COVID deaths in 2019 and 2020 had broadly the same IMD distribution, COVID-19 deaths in 2020 were more likely to have occurred in those living in the top five deciles of deprivation (44% (108/243) of COVID-19 deaths in 2020 compared with 33% (64/194) of deaths in 2019, p=0.02).
Causes of death
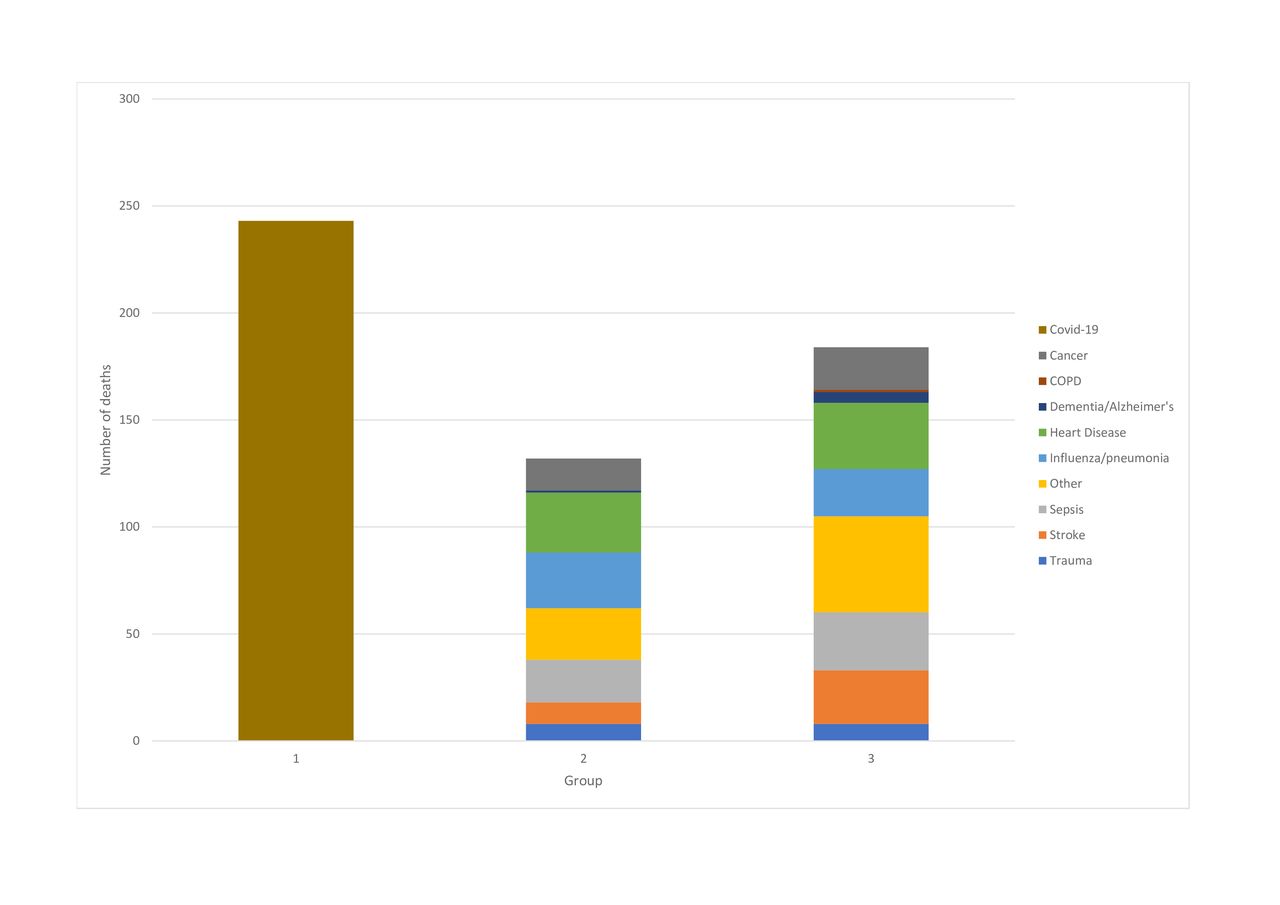
Given that there had been a significant reduction in the number of deaths, excluding COVID-19, between 2019 and 2020, we explored what the underlying cause of death had been in groups 2 and 3 (figure 3). St George’s is a regional stroke and interventional cardiology centre and one of London’s four trauma centres. Hence, it was particularly notable to see a large reduction in the number of deaths from stroke (60% reduction), but not from heart disease (10%) or trauma (0%).

Causes of death in each of the three groups. Group 1: COVID-19 deaths (2020); group 2: non-COVID deaths (2020); group 3: all deaths (2019). COPD, chronic obstructive pulmonary disease.
Comorbidities
Diabetes mellitus was significantly more common among patients who died with COVID-19 in 2020 (33% (79/243), p<0.001), compared with deaths in 2019 (16% (32/194)). Hypertension was more prevalent in both the COVID-19 mortality group (53% (129/243), p=0.02) and the non-COVID deaths in 2020 (55% (75/136), p=0.02), compared with deaths in 2019 (42% (81/194)). Pre-existing ischaemic heart disease was significantly more prevalent among the non-COVID 2020 deaths compared with the deaths in 2019 (32% (44/136) vs 13% (26/194), p<0.001) (table 1). Multiple comorbidities were significantly more likely in those dying from COVID-19 or non-COVID causes in 2020, compared with deaths in 2019 (table 1).
Adjusted analysis: COVID-19 deaths 2020 compared with 2019
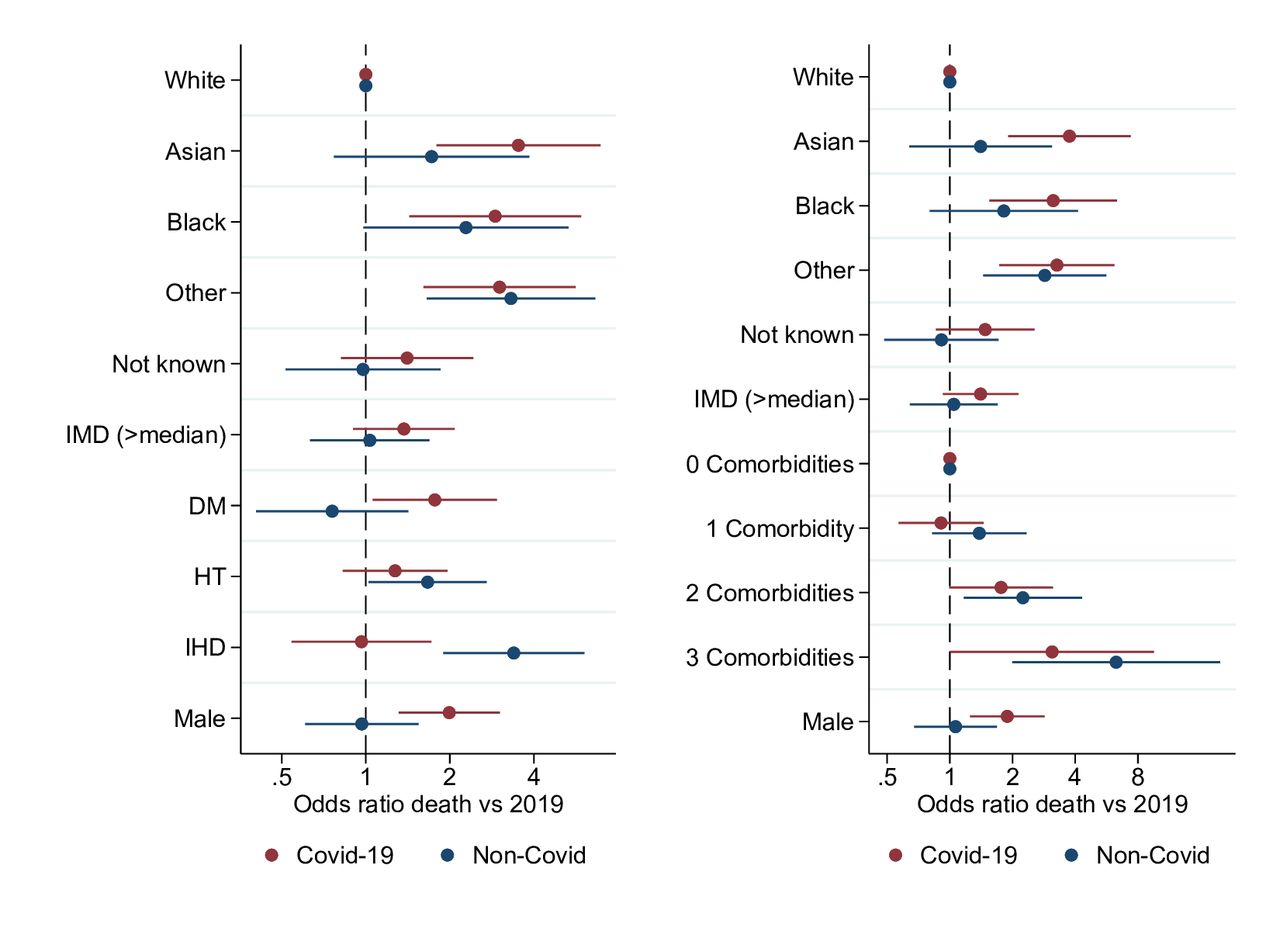
The logistic model included ethnic group, deprivation (being in the top five deciles of deprivation), sex, and comorbidities and adjusted for age. In the left panel of figure 4, the comorbidities were included individually. Compared with 2019, COVID-19 deaths were increased across the ethnic groups: Asian (ORadj=3.62, 95% CI=1.84–7.11, p<0.001); Black (ORadj=2.91, 95% CI= 1.43–5.91, p=0.003) and Other ethnicity (ORadj=3.01, 95% CI=1.61–5.64, p<0.001). Deprivation (IMD>median) was associated with a non-significant increase in likelihood of COVID-19 death, compared with 2019.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Independent effects of risk factors on likelihood of death in 2020 from COVID-19 or non-COVID-19 causes, compared with the same period in 2019. IMD>median—IMD 1–5 versus IMD 6–10. DM, diabetes mellitus; HT, hypertension; IHD, ischaemic heart disease; IMD, Index of Multiple Deprivation.
Among the individual risk factors, diabetes mellitus significantly increased the risk of COVID-19 death compared with 2019 (ORadj=1.76, 95% CI=1.05–2.94, p=0.03). There was no significant association with either hypertension or ischaemic heart disease. Male sex remained significantly associated with COVID-19 death (ORadj=2.00, 95% CI=1.32–3.03, p=0.001).
Replacing the ethnic subgroups with ethnicity dichotomised to white/non-white resulted in non-white ethnicity being significantly associated with COVID-19 mortality (ORadj=2.43, 95% CI=1.60–3.68, p<0.001).
In the right-hand panel of figure 4, the comorbidities score was included. Compared with deaths in 2019, there was a dose–response relationship between likelihood of death from COVID-19 and increasing number of comorbidities: baseline, no comorbidities (OR=1.0), one comorbidity (ORadj=0.90, 95% CI=0.56–1.44, p=0.67), two comorbidities (ORadj=1.75, 95% CI=0.99–3.10, p=0.06) and three comorbidities (ORadj=3.08, 95% CI=1.00–9.51, p=0.05).
Adjusted analysis: non-COVID deaths 2020 compared with 2019
For non-COVID deaths in 2020, all the BAME groups were at increased risk, although with broader CIs given the smaller number of non-COVID deaths: Asian (ORadj=1.59, 95% CI=0.73–3.60, p=0.26), Black (ORadj=2.27, 95% CI=0.98–5.30, p=0.06) and Other ethnicity (ORadj=3.32, 95% CI=1.66–6.65, p=0.001). Among the individual comorbidities, hypertension (ORadj=1.68, 95% CI=1.03–2.74, p=0.04), and particularly ischaemic heart disease (ORadj=3.41, 95% CI=1.91–6.11, p<0.001), were significantly more likely to be associated with a non-COVID death in 2020 compared with death in 2019. There was no association with sex or deprivation. With ethnicity incorporated as a binary variable, non-white ethnicity was significantly associated with non-COVID death in 2020 (ORadj=1.76, 95% CI=1.09–2.83, p=0.02).
As with COVID-19 deaths, there was a dose-dependent association with increasing numbers of comorbidities leading to a higher likelihood of death from a non-COVID cause in 2020, compared with deaths in 2019: baseline no comorbidities (OR=1.0), one comorbidity (ORadj=1.41, 95% CI=0.84–2.39, p=0.20), two comorbidities (ORadj=2.30, 95% CI=1.19–4.42, p=0.01) and three comorbidities (ORadj=6.46, 95% CI=2.04–20.4, p=0.001).
Discussion
In this analysis of a 6-week period of mortality data, commencing with the first COVID-19 death in in a large teaching hospital in London on 12th of March 2020, two phenomena were observed. First, the COVID-19 deaths rapidly escalated such that the total number of COVID-19 deaths significantly exceeded the number of all-cause deaths that occurred in the same 6-week period in 2019. Second, the number of non-COVID deaths diminished significantly throughout the period, dropping to less than half of the usual weekly number of deaths. The latter is consistent with the significant reduction in patients attending emergency departments with attendances having dropped by 30% in March 2020 at the start of the COVID-19 pandemic, compared with March 2019.13 Notable among the reduced number of non-COVID deaths has been the reduction of deaths for specific causes, with the number of stroke deaths having dropped by 60%. Assuming the rate of fatal strokes has remained constant, this suggests that more patients are dying of strokes in the community or at hospitals that may refer patients to our stroke unit. It is not possible from our data to analyse differences in referral patterns for regional specialty services, or indeed stroke deaths outside the hospital from the data evaluated. Conversely, it could be that the change in environmental circumstances during the lockdown has resulted in fewer strokes occurring.
The concern that the drop in non-COVID deaths in the hospital setting may be concealing a rise in such deaths in the community was confirmed in an independent analysis of the Office of National Statistic (ONS) data which demonstrated an absolute and relative increase in non-COVID deaths during the pandemic.14Subsequent analysis of mortality data in England and Wales by the ONS themselves has confirmed that non-COVID-19 deaths in hospitals fell to significantly below the 5-year average during this period, whereas an excess of non-COVID-19 deaths has occurred in care homes and private homes.15 The ONS hypothesised that if patients have been discharged from hospital sooner than they may have been typically, because of pressure on the National Health Service’s (NHS) resources, this could have resulted in some deaths occurring in care homes or private homes that would have otherwise occurred in hospital.15 The hospital never reached a point at which patients could not be admitted or could not have access to intensive care if this was required.
Although COVID-19 deaths occurred more frequently in the elderly, the age distribution of deaths was very similar in the three groups. Hence, in our analysis there was no evidence that the elderly were disproportionately represented in the COVID-19 deaths, compared with non-COVID-19 deaths during the same period and also compared with deaths occurring in the same period in the previous year. A possible explanation for why we did not see a difference in the age distribution of deaths between groups within the hospital is that our data only relate to deaths in the hospital and not those in the community and a significant proportion of COVID-19 deaths in the UK is occurring in nursing homes or at home.
COVID-19 deaths occurred significantly more frequently in those of non-white ethnicity. While concern has been expressed that the data on ethnicity in patients with COVID-19 are limited,16 our observation has been replicated by others.17 The degree of increase observed in our analyses is remarkably consistent with a recent analysis of NHS England mortality data for the whole of England.18 This combined data on COVID-19 fatalities with deaths by ethnicity and then undertook indirect standardisation of these data (using the whole population of England as the reference) to produce ethnic-specific standardised mortality ratios adjusted for age and geographical region. Death from COVID-19 was significantly more likely in BAME groups: Black African (3.24; 95% CIs=2.90–3.62), Black Caribbean (2.21; 95% CIs=2.02–2.41), Pakistani (3.29; 95% CIs=2.96–3.64), Bangladeshi (2.41; 95% CIs=1.98–2.91) and Indian (1.70; 95% CIs=1.56–1.85) minority ethnic groups.
Public Health England has undertaken a rapid review of the published literature, which included four studies describing the COVID-19 epidemic individual NHS trusts, to identify if inequalities exist in how BAME groups are affected by COVID-19 infection when compared with the White British population. This observed that the all-cause mortality was almost four times higher than expected among Black men, almost three times higher in Asian men and almost two times higher in White men.19 The review found that the highest age standardised diagnosis rates of COVID-19 per 100 000 population were in people of Black ethnic groups (486 in women and 649 in men) and the lowest were in people of White ethnic groups (220 in women and 224 in men).19
The increased mortality in the BAME communities has also been confirmed in an analysis combining general practitioner records of over 17 million adults with COVID-19 mortality data.20 Death from COVID-19 was strongly associated with: being man (HR=1.99, 95% CI=1.88–2.10); older age and deprivation (both with a strong gradient); uncontrolled diabetes (HR=2.36 95% CI=2.18–2.56) and severe asthma (HR=1.25 CI=1.08–1.44). Compared with people with ethnicity recorded as white, black people were at higher risk of death, with only partial attenuation in HRs from the fully adjusted model (age-sex adjusted HR=2.17, 95% CI=1.84–2.57; fully adjusted HR=1.71, 95% CI=1.44–2.02); with similar findings for Asian people (age-sex adjusted HR=1.95, 95% CI=1.73–2.18; fully adjusted HR=1.62, 95% CI=1.43–1.82).
Significantly in our analysis we also find an increased mortality in the BAME communities from non-COVID causes during the early phases of the pandemic at St George’s Hospital. Both the COVID-19 and non-COVID increases in mortality were independent of comorbidities, sex, age and deprivation. That these other factors do not explain the increase leaves the outstanding question as to what is responsible for the increase in mortality during the pandemic within the BAME communities.
The comorbidity analyses demonstrate that those dying in 2020 at St George’s Hospital were more likely to have multiple morbidities. We focused on the three most common comorbidities and subsequent research has confirmed the importance of these. The principal comorbidity we had limited data on was obesity, largely because of poor recording of weight in the medical records. Furthermore, it would have been useful to have information about other comorbidities such as respiratory disease. This suggests that potentially the patients being admitted to the hospital were more likely to be complex and chronically ill. It maybe that there has been an ethnic variation in who has attended and subsequently been admitted to hospital during the pandemic. A history of hypertension was associated with both COVID-19 and non-COVID deaths in 2020, with diabetes mellitus a major risk factor in COVID-19 deaths, and a history of ischaemic heart disease in non-COVID deaths. Our case notes review ascertained pre-existing comorbidities rather than comorbidities acquired during the hospital admission. It is recognised that COVID-19 acutely affects the kidneys21 and heart22 in a significant proportion of critically ill patients.
While we can compare the IMD distribution between the three groups, we have to infer how this relates to the IMD distribution of the St George’s catchment area. The IMD distribution of Merton is broadly consistent with the IMD distribution for the deaths in 2019 (group 3).23 Compared with the 2019 deaths, those living in more deprived areas were over-represented among the COVID-19 deaths, consistent with national data associating poverty with increased likelihood of death from COVID-19 disease. The association was statistically significant in univariate analysis but not in the adjusted analysis. All-cause mortality increases with increasing deprivation. A recent ONS analysis has shown that over and above this stepwise association with increasing poverty, COVID-19 deaths are over-represented in the top three deciles of deprivation.24 Hence, the absence of detecting a stronger signal between deprivation and COVID-19 mortality in the St George’s data, is likely to reflect the paucity of the most deprived areas in our catchment area.
In a recent analysis of 16 749 patients with COVID-19 admitted to 166 UK hospitals between 6th of February and 18th of April, the most common comorbidities were chronic cardiac disease (29%), uncomplicated diabetes (19%), non-asthmatic chronic pulmonary disease (19%) and asthma (14%), with 47% having no documented comorbidity.25 The median age of admissions was 72 years and of deaths was 80 years, and 60% were men. The excess of male deaths was confirmed, as was the association of diabetes and chronic cardiac disease with increased risk of mortality from COVID-19. The analysis did not refer to ethnicity.25
This paper describes a comprehensive analysis of the early phases of the COVID-19 pandemic in a major London teaching hospital. The strengths of our study are that the data were acquired prospectively through medical examiner case review and all patients who had a positive COVID-19 swab were captured in the COVID-19 group. COVID-19-associated deaths may have been very slightly underestimated in the context of possible false negative swabs, or in patients who died prior to a swab being taken. It is unlikely that the in-hospital non-COVID deaths are underestimated, although some patients in the COVID-19 group may have died with, rather than of, COVID-19. Importantly, St George’s Hospital serves a population of rich diversity and declared ethnicity data were derived from patient and family reporting.
This study was limited by the relatively small numbers in a single centre, and the methodology focusing on in-hospital deaths alone. The study was not designed to evaluate the characteristics of survivors of COVID-19. We were not able to determine whether there were differences in sociocultural determinants of attendance behaviour between ethnic groups, or indeed differences in those who survived COVID-19 and clinical records do not consistently record this information. The recommendations of the Public Health England report include improving the comprehensiveness and quality of ethnicity data collection and recording, as well as improving access, experiences and outcomes of NHS services by BAME communities.19
Medical examiners have the ability to contribute to future research through their timely review of clinical records, consistency of data recording and their role enabling them to gain further insights from bereaved families. Individual case review, such as what took place in this analysis, may help facilitate distinguishing between death being directly caused by COVID-19 as opposed to it being a contributor.
Conclusions
Analysis of COVID-19 deaths at St George’s demonstrated a similar age distribution to deaths normally observed in the hospital. In contrast, BAME communities are disproportionately affected by COVID-19 and non-COVID deaths, and the excess in mortality in the BAME groups remains after adjustment and is not fully explained by available hospital information on comorbidities, age, sex or poverty.
Footnotes
Contributors MRP made substantial contribution to the analysis and interpretation of data, drafting the manuscript and review of literature. SLH, ACG, WA, SH, ZA, RH, JB and KH all made substantial contributions to design, case note review and data acquisition through their exceptional medical examiner work during the COVID-19 pandemic, and to drafting and critical reviewing the manuscript. NK led the group and had the concept, contributed to daily data acquisition, data analysis and drafting of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval We undertook a surveillance analysis of the early stages of the Covid-19 pandemic at a large London teaching hospital to identify and understand risks associated with death from Covid-19 using anonymised mortality data routinely gathered by the Medical Examiners’ Office. The proposed analyses were discussed with our local Research office who agreed this was disease surveillance and therefore did not require formal NHS Research Ethics Committee approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included. No further data available.