Article Text

Abstract
Objectives Children from South Asian ethnic backgrounds are at increased risk of obesity and its associated future health risks; however, evidence is lacking as to whether parental concern about their child’s future overweight risk varies by ethnic background. We hypothesised that parents of 5-year-old children from South Asian backgrounds would be more likely to express such concerns.
Design Cross-sectional.
Setting UK.
Participants 15 039 singleton 5-year-old Millennium Cohort Study participants (48.9% girls; 86.7% White).
Primary outcome measure Parent-reported concern (some/none) about future overweight risk.
Methods We estimated the adjusted ORs (aORs) of some parental concern (ranging from a little to very concerned) by child’s ethnic background (reference group: White), adjusted for parent and child weight status, and child sex.
Results Parents of girls from Pakistani (aOR 0.4; 95% CI 0.2 to 0.5), Bangladeshi (0.3; 0.2 to 0.5), Black African (0.5; 0.3 to 0.7) and Mixed (0.7; 0.5 to 0.99) ethnic backgrounds and of boys from Pakistani ethnic backgrounds (0.6; 0.4 to 0.9) were less likely to report concern about their child’s future overweight risk than parents of White girls and boys, respectively. Overweight (2.5; 2.2 to 2.8) and obesity (6.7; 5.7 to 7.9) in children, and overweight (1.4; 1.2 to 1.5) and obesity (1.9; 1.7 to 2.2) in parents, were associated with increased likelihood of concern.
Conclusions Parents of children from South Asian ethnic backgrounds express less concern about their child’s future overweight risk. Qualitative studies are needed to understand the concerns of parents from different ethnic backgrounds to inform weight-management interventions in ethnically diverse populations.
- Pediatric obesity
- parents
- concern
- ethnic groups
- overweight
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We used robust statistical methods to analyse a large, nationally representative cohort of children from diverse ethnic backgrounds, allowing examination of parental concern across 10 ethnic groups.
We adjusted for factors known to be associated with increased parental concern, including child weight status, using clinical definitions of overweight and obesity, and applied ethnic-specific body mass index (BMI) adjustments for more accurate assessment of body fatness in children from South Asian and Black backgrounds.
We were unable to apply adjustments to the BMI of children from Mixed and Other ethnic backgrounds because validated algorithms to adjust BMI among children from these groups are not available.
Responses to the parental concern question are unlikely to be influenced by the study child weight measurement as weight was recorded after this question was answered and no interpretation or categorisation of BMI was provided to parents. As our study was cross-sectional, we are unable to determine the temporal association between concern and weight status.
Some children may have been weighed prior to interview at home, or in clinic, schools or other settings, and this might have influenced parental concern; however, this information was not available.
Introduction
In England, more than a quarter of children currently leave primary school with a body mass index (BMI) indicating they are overweight or obese, at a level needing clinical weight management support.1 These proportions vary by ethnic background and, after adjustment to account for ethnic variation in body fat mass, are significantly higher among children from South Asian backgrounds, especially boys.2 This has important implications for their future health, as children from South Asian backgrounds are known to be biologically more susceptible to the harms of overweight, and are at higher risk of developing type 2 diabetes and cardiovascular disease in adulthood.3–5
It has been suggested that parental concern about their child’s current weight status6 and about their child becoming overweight in the future7 may be meaningful predictors of willingness to engage in behaviour change.
Among parents of children whose BMI is in the overweight or obese range, there is evidence of increased parental concern about both their child’s present weight status8–11 and about their child becoming overweight in the future12 relative to those whose children have a healthy weight BMI. Furthermore, it has been shown that parents express higher levels of this concern about current13 14 and future15 16 weight status for daughters with overweight or obesity than for sons,13–16 as well as if they themselves have a BMI categorised as overweight or obese.12 16 There is only very limited evidence regarding ethnic variation in parental concern, with lower levels of concern for current childhood overweight reported in one study of parents from Black Somali backgrounds living in Liverpool,8 and greater concern about future child overweight from another study of parents from Black Afro-Caribbean backgrounds living in London,17 with others reporting no ethnic differences.12
However, these findings are based on regional studies with low response rates and consequently small sample sizes. Moreover, none adjusted BMI for ethnicity and few specifically examine parental concern about future child overweight (as opposed to current child weight status), warranting further investigation.
Across the UK, children’s heights and weights are measured on or shortly after entry to primary school at age 5 years. Following measurement, parents receive a feedback letter informing them of their child’s weight status. Given the longitudinal evidence that obesity at the beginning of primary school strongly predicts obesity on leaving primary school,18 19 age 5 may be viewed as an appropriate time to intervene to prevent and tackle obesity. It is therefore important to understand how parental concern about future childhood overweight might relate to weight status at this point in the life course.
We used cross-sectional data from a large ethnically diverse UK-wide cohort study to examine whether parental concern about their child’s future risk of overweight, reported when the child was aged 5 years, varied by ethnic background. Given the high rates of overweight and obesity observed among children from South Asian backgrounds after adjustments for body fat,2 and having taken parent weight status and child sex into account, we hypothesised that parents of overweight and obese children from South Asian backgrounds would be more concerned about their child becoming overweight in the future relative to parents of overweight and obese children from White backgrounds.
Materials and methods
Study design
We used data from the Millennium Cohort Study (MCS), a prospective nationally representative cohort of children born between September 2000 and January 2002 in the UK, which used a stratified clustered sampling design to over-represent children born in disadvantaged areas, from ethnic minority groups or from Northern Ireland, Scotland and Wales. When the cohort child was aged 9 months, 18 552 (68%) of 27 257 families contacted were interviewed at home when demographic, social and health information was obtained. An additional 692 families were recruited at age 3. Further interviews were conducted when children were aged 3, 5, 7, 11 and 14 years, when height and weight were measured. At age 5, 15 246 (85.8%) of 17 770 families eligible for interview were interviewed, providing data for 15 459 children (online supplementary figure S1).
Supplemental material
Inclusion and exclusion criteria
We included 15 039 of 15 459 singleton children whose parent (natural mother (97.0%), else child’s main care-giver, all referred to hereafter as the parent) was interviewed when their child was aged 5 years, having excluded 418 twins and triplets, as well as two children with extreme height and/or weight measures at age 5 or missing ethnicity (online supplementary figure S1). We extracted information available for these children from their two earlier and two subsequent MCS interviews. Characteristics of those who did and did not participate in the age 5 interview are given in online supplementary table S1; participating children were more likely to be from families in the highest income quintiles and to have more highly educated mothers compared with non-participating children. We weighted all analyses to take account of survey design and to allow for potential ethnic and socioeconomic biases in cohort attrition by age 5 years.
Main outcome measure
The main outcome measure was parental concern about their child’s future risk of becoming overweight. This was assessed at the age 5 interview from responses to a question administered by a trained interviewer who asked the parent “How concerned are you about [child’s name] becoming overweight in the future?” We followed the methods applied by others12 14–16 and derived a binary variable from the five possible responses as follows: parents reporting they were unconcerned (n=10 964), were categorised as ‘no parental concern’, with all other responses (a little concerned (n=2645), concerned (n=540), fairly concerned (n=390), very concerned (n=418)) categorised as ‘parental concern’. Response to this question was missing for 82 parents.
Main exposure variable
Ethnic background of the child was obtained from parental report at the first MCS interview and categorised using UK 2011 Census categories. Analyses were based on 10 individual Census categories, with the exception of some analyses where individual ethnic groups were too small to create 95% CIs when categories were grouped as follows: White (Irish, Traveller, Other), South Asian (Indian, Pakistani, Bangladeshi), Black (Black Caribbean, Black African, other Black), Mixed and Other (Other Asian, Chinese, Mixed, Other).20
Covariates
We examined two covariates: child weight status and parental weight status. At age 5 years, trained interviewers in the home measured the child’s height and weight: height was recorded to the nearest millimetre using a Leicester Height Measure Stadiometer (Seca, Birmingham, UK) with the head positioned in the Frankfort plane. Children were weighed barefoot and without outdoor clothing on Tanita HD-305 scales (Tanita, Middlesex, UK) and weight recorded in kilograms to one decimal place.21
To enable comparison with the current English child measurement programme, we used published guidance from Public Health England22 to assess the quality and range of height and weight measurements. We excluded one child with extreme short stature, and in addition assigned measurements in two children with extreme weight values as missing, as these were assumed erroneous when compared with their earlier or subsequent MCS weight measurements.
BMI at age 5 was calculated and adjusted for ethnicity using methods described by Hudda et al who used similar ethnic categories to those employed in this study.23 The authors pooled data from four UK studies which used the deuterium dilution method to measure body fat in approximately 2000 children from White European, South Asian and Black African backgrounds. They derived a height-standardised fat mass index (FMI) to represent body fat and fitted linear regression models to quantify ethnic differences in BMI–FMI relationships to provide ethnic-specific BMI adjustments. This adjustment entails adding approximately 1.1 kg/m2 to the BMI of children from South Asian backgrounds, and subtracting between −0.12 kg/m2 and −5.52 kg/m2 dependent on sex, age group and unadjusted BMI to the BMI of children from Black backgrounds to more accurately reflect adiposity in these groups, since it has been shown that BMI overestimates and underestimates body fat in children from Black and South Asian backgrounds, respectively. No adjustment is available to apply to children from Mixed or Other ethnic backgrounds.
We categorised the adjusted BMI, according to the UK90 clinical reference standard,24 into four mutually exclusive groups: ‘underweight’ (BMI <2nd centile), ‘healthy weight’ (≥2nd to <91st centile), ‘overweight’ (≥91st to <98th centile) or ‘obese’ (≥98th centile) based on alignment with sex-specific and age-specific BMI centiles from the LMS growth tool Excel add-in.25 26 We defined those with BMI ≥98th centile or ≥91st to <98th centile as clinically obese and clinically overweight, respectively. The UK90 clinical reference standard uses higher thresholds to define overweight and obesity compared with the UK90 population reference standard, indicating the need for clinical support for weight management. These thresholds are used by a variety of health professionals to assess individual children, as opposed to the UK90 population thresholds which are used to monitor population prevalence of overweight and obesity.24
Parental BMI was calculated using the parent’s self-reported weight (at the age 5 sweep) and their most recent self-reported height (usually recorded at the first contact sweep). Trained interviewers measured parental heights and weights objectively if they did not know their measurements for self-report. Parental BMI was categorised into four mutually exclusive groups: ‘underweight’ (BMI <18.5 kg/m2), ‘healthy weight’ (≥18.5 to <25 kg/m2), ‘overweight’ (≥25 to <30 kg/m2) or ‘obese’ (≥30 kg/m2). Due to the higher risk of type 2 diabetes and cardiovascular disease among adults from Asian backgrounds at a BMI lower than 25 kg/m2, lower thresholds for classifying overweight and obesity in South Asian adults were employed, where ‘overweight’ is considered ≥23 to <27.5 kg/m2 and ‘obese’ as ≥27.5 kg/m2, based on National Institute for Healthcare Excellence guidelines.27
Statistical methods
Response to the parental concern question was missing for 82 children. All children for whom consent was obtained from a parent or guardian and who could stand unaided had their height and weight measured.21 Height was missing for 235 and weight was missing for 234 5-year-olds (both height and weight were missing for 218 5-year-olds). BMI was missing for 2456 parents. We used multiple imputation to estimate missing data on parental concern, child height and weight at age 5, and parental BMI, and built 20 imputed datasets using the weighted iterative chain algorithm,28 including all variables involved in the analysis steps under the assumption that missingness is at random (online supplementary table S2). All analyses were carried out on imputed datasets and sensitivity analyses on complete cases.
We used descriptive statistics (proportions and 95% CIs) to assess the prevalence of parental concern overall, and by sex, ethnic background, child weight status and parental weight status. Similarly, we examined associations of child’s weight status with parental concern by sex and ethnic background. We used logistic regression to estimate the unadjusted odds of a parent being concerned about their child being overweight in the future by child’s ethnic group, sex, weight status and parental weight status (reported as ORs). We then mutually adjusted for child’s ethnic background, sex, and child and parent weight status. We tested for interactions between the child’s ethnic background and sex, and between child’s ethnic background and weight status, and used Wald test statistics for these interaction terms to inform the final logistic regression model. We derived sex-specific and ethnic-specific ORs by multiplying the interaction term coefficient by the ethnicity coefficient and plotted these in a forest plot.
All analyses and percentages cited were performed in Stata and weighted to take account of survey design and to allow for potential biases in attrition by age 5 years, using the svyset command (Stata/SE V.15; StataCorp, College Station, Texas, USA).
Ethics approval
Approval for MCS was granted by the London Research Ethics Committees29 and no further approval was required for this secondary analysis.
Patient and public involvement
This research was done without patient or public involvement. Neither were invited to comment on the study design and were not consulted to develop relevant outcomes or interpret results.
Results
Sample characteristics
Of 15 039 children, 48.9% were girls, and 86.7% were from White and 6.1% from South Asian backgrounds (table 1). Parental concern about their child becoming overweight in the future was reported by 27.3% of parents (18.6% ‘a little concerned’, 3.5% ‘concerned’, 2.6% ‘fairly concerned’, 2.6% ‘very concerned’), and this was more common among parents of girls than of boys (table 1).
Sample characteristics and proportion of parents reporting parental concern
Parental concern
Parental concern was strongly associated with child’s BMI status and was more common among parents of children with overweight or obesity (42.3% and 66.2%, respectively) than among parents of children with a healthy weight (22.3%; table 1). Similarly, parental concern was more likely to be reported by parents with overweight or obesity: 29.9% and 39.7%, respectively, compared with parents with a healthy weight (22.7%; table 1).
Parental concern was reported significantly less among parents of children from Pakistani (20.9%) and Black African (20.1%) backgrounds, compared with parents of children from White ethnic backgrounds (27.8%; table 1).
Overweight and obesity prevalence by ethnic background and sex
At age 5, the prevalence of overweight and obesity was 11.0% and 6.6%, respectively, with obesity more prevalent among boys (7.5%) than girls (5.7%) (table 2; parent weight status was positively associated with child weight status, see online supplementary table S3).
Overweight and obesity* prevalence by ethnic background† and sex
Within each ethnic group, most 5-year-old children were of healthy weight; however, children from South Asian backgrounds were more likely to have a BMI in the obese range than children from White backgrounds (table 2). There were some minor differences by sex, with boys from South Asian backgrounds and girls from Pakistani and Bangladeshi backgrounds more likely to have a BMI in the obese range than those from White backgrounds (table 2).
Parental concern by ethnic background and sex
Fewer parents of girls from Pakistani, Bangladeshi or Black African backgrounds reported parental concern relative to parents of girls from White backgrounds. These differences were not seen in boys (table 3).
Parental concern about future overweight risk at age 5 years by ethnic background* and sex
Parental concern by weight status, ethnic background and sex
Parental concern was reported for 73.4% of girls with obesity compared with 61.0% of boys with obesity (table 4).
Parental concern about future overweight risk at age 5 years, by child weight status* at age 5
Parental concern was reported by fewer parents of healthy weight, overweight and obese girls from South Asian backgrounds compared with parents of girls from White backgrounds (table 4). No differences in parental concern by weight status were observed between boys from different ethnic backgrounds (table 4).
Logistic regression analyses
After mutual adjustment for ethnic background, sex and child and parent weight status, parental concern was significantly less likely among children from Pakistani, Bangladeshi and Black African ethnic backgrounds. Parental concern was more likely among parents of overweight and obese children, or of girls, and among parents who themselves were overweight or obese (table 5 ‘Adjusted’ model).
Unadjusted, adjusted and sex-specific and ethnic-specific adjusted odds of parental concern about future overweight risk at age 5 years
As the Wald test statistic for an interaction between sex and ethnic background was significant (online supplementary table S4), the final adjusted model included this interaction term (other interactions were not significant and were excluded from the final model; see online supplementary table S4). The sex-specific and ethnic-specific odds accounting for this interaction are shown in table 5 and figure 1, using White ethnic background as the reference category.
{kind=link}
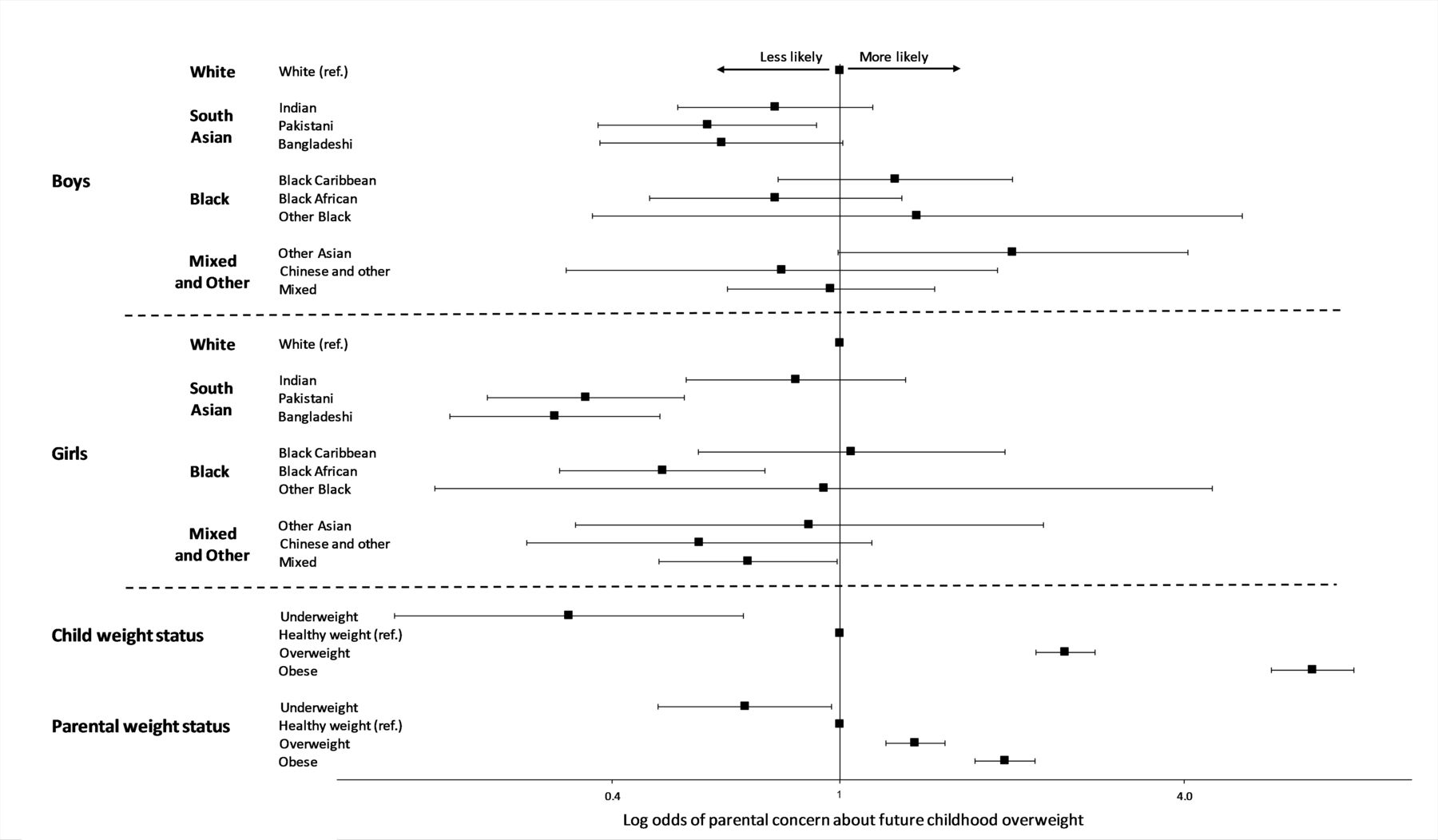
Adjusted odds of parental concern about future childhood overweight (mutually adjusted for ethnic background, sex, child weight status, parent weight status, and an interaction between sex and ethnic background).
Parents of boys from Pakistani backgrounds were less likely to be concerned about their child’s future risk of being overweight (figure 1), as were parents of girls from Pakistani, Bangladeshi, Black African, Mixed or Other ethnic backgrounds.
In the final model, parental concern about future childhood overweight was more likely among parents of children with overweight and obesity, and less likely among parents of children considered underweight, compared with parents of children with a healthy weight (figure 1). Parents who themselves had a BMI in the overweight or obese range were more likely, and those with a BMI considered underweight less likely, to report concern than those with a healthy weight (figure 1).
Adjusted ORs were similar for complete case analyses (with the exception of the interaction between female sex and Bangladeshi ethnic background; online supplementary table S5) and for BMI without ethnic adjustment (data not shown).
Discussion
Principal findings
In this large nationally representative study, we found that parents of children from South Asian backgrounds were less likely to be concerned about their child’s future overweight risk compared with those from White backgrounds. This was particularly so for girls from Pakistani and Bangladeshi backgrounds, and was independent of child and parent weight status. Furthermore, among our total sample of more than 15 000 children, we confirmed associations between parental concern and child sex and weight status reported by others.
Increased understanding of the context in which people from different ethnic backgrounds report parental concern is important to inform the development of interventions to support parents and families to alter the weight trajectories of their children with overweight or obesity. This is especially important for children from South Asian backgrounds, given their higher absolute risk of obesity and greater metabolic sensitivity to its effects. Our findings make a significant contribution to the literature on parental concern. This is, to our knowledge, the first study to use a UK-wide nationally representative cohort to examine whether parental concern about future risk of overweight in their child varies by ethnic background.
Strengths and limitations
Strengths of our study include analyses based on a large, nationally representative cohort of children from diverse ethnic backgrounds, allowing examination of parental concern across 10 ethnic groups. Our findings are generalisable to the UK reflecting the nationally representative nature of the MCS: both the prevalence of overweight and obesity and the proportion of children from each ethnic background at age 5 in this cohort are similar to that reported in Public Health England’s National Child Measurement Programme (NCMP) for the 2006/2007 academic year, when most children included in this study were aged 5 years.30 31
We used robust statistical methods including imputation of missing data and use of survey weights to account for survey design and to allow for biases in attrition. We used a clinical definition of overweight and obesity that indicates the need for clinical weight management support, and applied ethnic-specific BMI adjustment for more accurate assessment of body fatness in children from South Asian and Black ethnic backgrounds. While this method of adjusting children’s BMI is not currently employed in the NCMP, which may make comparisons with other studies less straightforward, analyses without ethnic adjustment produced similar findings.
We were able to adjust for a number of covariates in our analysis including those shown previously to be strongly associated with parental concern, including parental and child weight status (the latter based on objective measurements). Responses to the question eliciting parental concern are unlikely to be influenced by the MCS weight measurement as this question was asked before the child was weighed, and furthermore no interpretation or categorisation of MCS BMI was provided in the feedback to parents.29
Although it is possible that some children may have been recently weighed either at home, in clinical care or in school as part of the NCMP, information on the timing of this in relation to the MCS interview, or the feedback given to parents, is unavailable. The MCS interview did not ask parents about their perception of their child’s weight status at age 5, and consequently we were unable to adjust for this in our final model. Furthermore, given the cross-sectional design of this study, we are unable to draw any conclusions about the temporal relationship between parental concern and child weight status. Since the majority of main respondents were natural mothers, our findings may not be generalisable to fathers or other parents.
As one in seven children in this study were from Black, South Asian and Other ethnic backgrounds, we were able to examine parental concern across all major ethnic groups; however, absolute numbers for some groups were small, resulting in greater uncertainty for these estimates.
We used lower thresholds for overweight and obesity to categorise BMI in adults from South Asian backgrounds to reflect the higher risk of type 2 diabetes and cardiovascular disease at lower levels of BMI experienced among these adults.27 Although parental height and weight were self-reported, this is considered a reliable measure in epidemiological studies.32 33 Furthermore, at present there are no validated algorithms for the adjustment of BMI for children from Mixed and Other ethnic backgrounds, so no adjustments were made for these children in our analyses. Although we lacked statistical power to evaluate all subcategories of parental concern, we used the approach others have taken using this instrument and dichotomised parental concern into ‘concern’ or ‘no concern’ in order to produce robust estimates when examining parental concern by sex and ethnic background.12 14–16
Other studies
There are, to our knowledge, no other published reports examining ethnic variation in parental concerns about their child’s future risk of becoming overweight using a UK-wide nationally representative cohort of children. Our finding of less parental concern among parents of girls from Black African backgrounds is similar to that reported for parents from Black Somali backgrounds in Liverpool,8 but not consistent with those from a regional study which observed greater parental concern among parents from Black Afro-Caribbean backgrounds living in London.17
The explanations for our main finding that there is variation by ethnic background in parental reported concern about their child’s future risk of becoming overweight warrant further investigation. This finding may reflect differences in awareness of children’s weight status or perceptions of childhood weight and size among parents from different ethnic backgrounds. However, it may be more useful to explore the wider context and barriers which children and their families from different ethnic backgrounds face in negotiating healthy or ‘ideal’ weight so that interventions can be considered which reflect the diverse ethnic backgrounds of children with obesity in the UK.
Many parents are unable to identify overweight or obesity in their children,15 34 35 with the majority of parents of children with a BMI in the overweight or obese range underestimating their child’s weight status,12 36 a finding replicated in numerous high-income countries across the world.35 37 38 While there is some evidence that recognition of overweight or obesity is difficult among adults from South Asian backgrounds,39 the reasons for this remain unclear and similar studies in children are lacking.
While parental recognition of child overweight or obesity can be helped by presenting them with child age-specific and sex-specific body images,40 these have not been tested among parents from different ethnic backgrounds. Furthermore, we did not find any evidence to suggest that parental concern about child future overweight risk among children from different ethnic backgrounds varied by objectively measured child weight status.
Qualitative research provides important contextual information about South Asian parents and their extended families. Pallan et al have highlighted the importance of intergenerational influences on child diet and perception of their weight status, suggesting that fatness may signal health and that provision of abundant food may symbolise parental/carer affection for the child.41 This may be important for families relying on grandparents for informal childcare, and multigenerational households where meals are communally prepared and eaten.41 42 For example, studies of women from Pakistan living in North West England and an ethnically diverse sample of families in London have both reported that in these groups, familial expectations to maintain traditional home-cooking procedures are obstacles to changing food preparation and eating practices.42 Similarly, qualitative research involving women from Somalia living in Liverpool found that many women felt restricted in their efforts to live healthier lifestyles by older relatives’ perspectives which promote increased weight, although this study did not focus on the influence of the home environment on their child’s weight status,43 highlighting differences between people from different ethnic backgrounds.
While there is evidence that acculturation can alter maternal health behaviours with the adoption of potentially less healthy behaviours by migrants over time,44 we did not set out to examine structural barriers or acculturation among migrants in this study and further research to explore intergenerational variation in parental concern about future childhood overweight is required.
Our finding that a greater proportion of parents of girls compared with parents of boys from White backgrounds were concerned about their child becoming overweight in the future is consistent with findings from other UK studies of predominantly White populations13–15 and with one from Australia.16 This may reflect societal expectations of ‘ideal’ body shapes for boys and girls14 whereby girls are expected to be slight or petite, and boys to be bigger, stronger or more muscular.45 Findings from a qualitative study interviewing parents of preschool-aged children in America suggest that childhood overweight is normalised through the use of euphemistic terms like ‘cute baby fat’ or ‘podge’,46 and discussions of body size relate to how ‘big’, ‘strong’ or ‘muscular’ the child is.47 Other studies have suggested that parents do not worry about their child’s weight status because they believe their child participates in an appropriate level of physical activity and/or eats a balanced or healthy diet.47 48
Given these accounts, parents from different ethnic backgrounds may experience social contexts where monitoring child weight is not a priority, particularly in environments where higher weight is a signal of wellness, health and affection for the child. Similarly, given that people from ethnic minority backgrounds, particularly from Pakistan and Bangladesh, are more likely than White British people to live in the most deprived areas in England,49 it is possible parents prioritise providing for their family over parental concern about future childhood overweight, a less immediate concern. This view is supported by literature which suggests that the future may be perceived differently depending on personal circumstances, such that concepts of ‘public health futures’ are not applicable to all individuals.50
Our finding that concern was reported more often for children with overweight and obesity is consistent with previously published reports.9 12–15 Our findings are similar to those of Carnell et al who used the same question and response scale but did not examine the influence of ethnicity on this association.12 Parents may be better able to identify their child’s weight status at the extreme end of obesity14 15 indicating that, to some extent, parents are aware of overweight in their children. Inability to assess correctly their child’s weight may be a barrier to prevention of childhood obesity13 14 51 since lifestyle changes are not initiated36 52; however, Carnell et al have argued that parental concern is a more sensitive indicator of parental awareness of than parental identification of a child’s weight status.
The temporality of this relationship, however, remains unclear as our study was cross-sectional. While it seems plausible that parents are more likely to report concern because their children are already overweight, a range of studies, predominantly from Australia53–55 and the USA56–60 as well as from the UK61 and Sweden,62 have proposed that parents reporting concern about their child becoming overweight might be more likely to engage in behaviours such as restrictive feeding, where children’s food is controlled and limited.
Longitudinal research has suggested that restrictive feeding practices can result in child weight gain. A prospective study of Australian children aged 2 years suggests restrictive feeding practices lead to obesogenic behaviours such as overeating,63 while in the USA a study of children 5 to 7 years old showed a positive association between restrictive feeding and additional weight gain among children at risk of obesity.64 Two further longitudinal studies in the USA showed restrictive feeding practices were associated with increased eating in the absence of hunger among girls aged 5 to 9 years.65 66
With this in mind and given the cross-sectional nature of our study, our findings require careful interpretation: while it is possible that parental concern is a response to child overweight, it remains that child overweight could be in part driven by parental concern and associated feeding practices.
Whether parental feeding practices vary by ethnic background is largely unknown,67 but remains an important research question particularly as it has been suggested that there may be benefits to restrictive feeding for older, more overweight children but less so for younger, healthy weight children who are yet to develop their eating behaviours.67 One cross-sectional study comparing feeding practices in Germany and Britain found that parents from Black Afro-Caribbean backgrounds living in Britain were more likely to use restrictive feeding practices than parents from White backgrounds living in either Britain or Germany, and this was associated with higher child BMI.68 Further research is needed to understand how social context and ethnic backgrounds might influence parents’ feeding practices.
Implications for policy and practice
Our study has implications for practice and research. Our cross-sectional analyses confirmed a strong positive association between the child’s current weight status and parental concern, suggesting parents of children with a BMI in the overweight and obese range are more likely than other parents to be concerned about their child’s future overweight risk. This is important, given the suggestion that appropriate parental concern is vital for effective parental engagement with obesity intervention programmes7 and positive behaviour change.6 Further research is needed to determine whether parental concern is associated with healthier weight trajectories, as well as to understand how feedback given to parents about their child’s weight status from the NCMP can be appropriately and accurately conveyed to parents from different ethnic backgrounds.
Our study also has implications in particular for targeted interventions aimed at childhood obesity prevention and management. Parents from particular ethnic backgrounds at higher risk of obesity are less likely to express concern about future childhood overweight, particularly so for girls. This needs to be taken into account in developing ethnically sensitive interventions for weight management of children with obesity in multiethnic populations. As with all complex interventions, these need to be informed by qualitative studies to elucidate the factors underlying these novel observed differences in rates of parental concern among participants from different ethnic backgrounds, and to aid their interpretation.
Conclusion
In summary, we have found that, in contrast to our original hypothesis and after taking into account child and parental weight status, parents of children from South Asian ethnic backgrounds who are at higher risk of childhood obesity and its adverse consequences are less likely to report concern for their child’s future overweight risk, particularly for their daughters. These novel insights are of importance to the UK population, where the highest risk of obesity is observed in individuals and communities from these backgrounds.
Acknowledgments
The co-operation of the Millennium Cohort Study participating families is gratefully acknowledged. The authors are grateful to Mohammed Hudda, Professor Peter Whincup and colleagues at St. George’s University of London, Population Health Research Institute, for sharing their algorithms for ethnic-specific BMI adjustment.
References
Footnotes
Contributors NF and CD conceptualised and designed the analysis. NF carried out the literature search, conducted and interpreted the analyses, generated tables and figures, and drafted the initial manuscript. CD contributed to the interpretation of analyses, and reviewed and revised the manuscript. All authors were involved in writing the paper and had final approval of the submitted and published versions.
Funding This research was funded by a grant from Barts Charity ref: MGU0419. The authors are grateful to the Centre for Longitudinal Studies, UCL Institute of Education and the UK Data Service.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Approval for MCS1 was granted by South West MREC MREC/01/6/19. Approval for MCS2 was granted by London MREC MREC/03/2/022. Approval for MCS3 was granted by London MREC Committee. 05/MRE02/46. Approval for MCS4 was granted by Yorkshire MREC 07/MRE03/32. Approval for MCS5 was granted by Yorkshire and The Humber—Leeds East 11/YH/0203.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open-access repository.