Article Text

Abstract
Objective Given the South Asian phenotype of higher body fat at similar body mass index (BMI) relative to Caucasians, we sought to explore the association between prominent adiposity indicators with blood pressure (BP) and hypertension, to compare the accuracy of these indicators in estimating hypertension, and to provide cut-off values associated with adverse hypertension risk in South Asian children.
Design Cross-sectional study.
Setting Community-based recruitment in two Canadian cities (Hamilton and Surrey).
Participants South Asian children (n=762) were recruited from two Canadian cities. Waist circumference, waist to height ratio and BMI were determined. Body fat percentage was assessed by bioelectrical impedance analysis and BP was assessed using an automated device. All variables (except body fat percentage) were transformed to z-scores using published standards.
Outcome measures Linear and Poisson regression was used to explore associations between the adiposity indicators with BP z-score and hypertension. Receiver operating curve (ROC) analysis was used to explore the strength of the adiposity indicators in estimating hypertension risk and sex-stratified optimal adiposity cut-off values associated with hypertension risk.
Results Significant associations were detected in adjusted and unadjusted models between the adiposity indicators with BP z-score and hypertension (p<0.01 for all). The area under the curve (AUC) values for the adiposity indicators for boys and girls ranged from 0.74 to 0.80, suggesting that the adiposity indicators are fair measures of estimating hypertension risk. Sex-stratified cut-off associated with adverse risk of hypertension for girls and boys, respectively, were at the 92nd and 82nd percentile for BMI z-scores, 65th and 80th percentile for WC z-score, 63rd and 67th percentile for WHtR z-score and at 29.8% and 23.5% for body fat.
Conclusion Our results show associations between adiposity indicators with BP and hypertension and suggests that South Asian children might be at adverse risk of hypertension at levels of adiposity considered normal.
- adiposity
- hypertension
- South Asian
- children
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study is cross-sectional by design and as such limits to the attributions of causality apply.
Our restriction of sampling to only two Canadian cities might also limit the generalisability of this study.
The strength of this study is in its large sample size of South Asian children.
Introduction
The prevalence of childhood obesity has been increasing globally.1 Between 1980 and 2013, childhood overweight and obesity in developed countries increased from 17% to 24% in boys and 16% to 23% in girls. In low/middle-income countries, meanwhile, it rose from 8% to 13% in both boys and girls within the same period.1 Childhood obesity has adverse influence on metabolic health and blood pressure (BP), with a similar pattern to that seen in adults.2 Compared with children with normal weight, being overweight is associated with three times the risk for hypertension (BP ≥95th percentile).3 In children (ie, ≤18 years) with obesity, the risk for hypertension is even greater at about four to ten times the risk.4 This is a concern as children with hypertension are likely to continue to have hypertension as adults, and to be at greater risk for a variety of cardiometabolic diseases including cardiovascular diseases (CVD), stroke and renal failure.5
South Asian ethnicity is associated with a greater risk of conventional CVD risk factors such as dyslipidaemia, type 2 diabetes and abdominal obesity.6–8 In children, a few studies have demonstrated increased prevalence of obesity and, concomitantly, hypertension in South Asians.9 Specifically, South Asian children have been shown to have a unique phenotype that lends itself to higher fat at similar body mass index (BMI) compared with Caucasians10 11 placing them at greater risk for a number of diseases. This finding has important health implications as South Asians represent about 25% of the global population.12 In Western countries such as the UK, the USA and Canada, South Asians represent a significant portion of the visible ethnic minority group of the population.13–15 To reduce the potential economic impact on healthcare systems as well as the impact on individuals, it is crucial to address the increased prevalence of obesity with appropriate measures that are related to health risks in South Asian children.
BMI, waist circumference (WC), waist to height ratio (WHtR) and bioelectrical impedance analysis (BIA) estimation of body fat percentage are some of the predominant measures used in research and clinical practice to assess adiposity in children as they are relatively easy and non-invasive. Several studies have assessed these adiposity measures to determine whether they are reliable indicators of obesity in the broader paediatric population.16–18 A few studies have also explored their diagnostic accuracy in estimating metabolic risk factors such as hypertension in children.19 However, most of these studies have been carried out in predominantly Caucasian populations. Given that differences have been observed with respect to the distribution of body fat when comparing South Asians with other ethnic groups, validating these indicators in South Asian children is important. Furthermore, it is also unclear what adiposity cut-offs might correspond to increased cardiometabolic risk specifically in South Asian children.
This study therefore explores the association between adiposity indicators with BP and hypertension in South Asian children, and compares the accuracy of these indicators in estimating the risk of hypertension. As a secondary aim, we explore what adiposity cut-off values might be associated with risk for hypertension in this population.
Methods
Study design
Participants in this study were recruited as part of the Research in International Cardiovascular Health—Lifestyles, Environments and Genetic Attributes in Children and Youth (RICH-LEGACY) study, a cross-sectional study designed to investigate CVD risk factors among South Asian children living in Canada. Parents of participants provided written informed consent, while participants assented to take part in the study.
Recruitment
Elementary school children and high school children (n=762) were recruited using community-based recruitment methods in two Canadian cities (Brampton, Ontario and Surrey, British Columbia) by convenience sampling between 2012 and 2016. Elementary schools with high South Asian enrolments were first identified by contacting the school boards. Once schools were identified, packages containing an invitation letter, a RICH-LEGACY study description and consent forms were sent to parent/guardians of children enrolled in the identified schools. Additionally, the study was advertised through venues used by South Asian groups including newspapers, local television stations, community centres, worship centres and festivals. Inclusion criteria included: children (in elementary or high school) having at least three grandparents of South Asian origin; being able to communicate in English; and being able to provide consent (parents) and assent (children). Research assistants fluent in Hindi and Punjabi were responsible for recruitment and data collection. The research assistants who were involved in the measurements all undertook training together through simulator sessions and were retrained if variations in measurement protocol were observed by the research coordinator. This process was repeated for a few days to ensure accuracy and consistency among the research assistants in the assessment of the measurements collected in this study. In addition, written materials (including consent forms) were provided in English, Punjabi, Hindi and Urdu as needed.
Participant assessment and anthropometric characteristics
Children self-reported demographic characteristics including age and sex, while parents provided information on their educational level. Assessment took place within the community (ie, community or worship centres) depending on which the child and parent were comfortable with. Anthropometric characteristics including height and weight (used to calculate BMI), and WC were measured by trained researchers. WHtR was calculated using WC and height. Height was measured to the nearest 0.1 cm using a right angle triangle and a calibrated wall-mounted scale. Weight was measured to the nearest 0.1 kg using the Tanita Ironman Innerscan BC-554 scale with participants dressed in light clothing. WC was recorded in centimetres as the average of two measures taken using a non-stretching tape, against the skin after a normal expiration, halfway between the lower rib margin and the iliac crest.20 Body fat percentage estimated by BIA was also measured using the Tanita Ironman Innerscan BC-554 fat scale. Participants were asked to stand on the Tanita Ironman Innerscan BC-554 with bare feet wearing light clothing to measure weight and estimate body fat percentage. Assessments were done at times of day convenient for participants and parents irrespective of food or fluid intake. The Tanita scale has been found to yield acceptable levels of agreement when compared with dual-energy x-ray absorptiometry in validation studies.21 22 Following anthropometric assessment, BMI was transformed to z-scores using WHO growth references for young people aged 5–19 years23. Using WHO weight categories, normal weight was defined as BMI z-score <1, overweight as BMI z-score of 1–2 and obesity as BMI z-score >2. WC and WHtR were both transformed to z-scores using recently published values for age and sex using the Third US National Health and Nutrition Examination Survey (NHANES III).24 The transformation to z-scores allows for standardised comparisons across children with similar or different ages and sex.
Blood pressure
BP was assessed following 10 min of seated rest in the left arm using the Omron HEM-711DLX automated blood pressure monitor with appropriately sized cuffs. Three BP measures were taken over a 10 min period, and the average of the three measures was recorded. Subsequently, BP was transformed to SD scores and percentiles for age, sex and height according to the fourth recommendation of the US National High Blood Pressure Education Program (NHBPEP) working group report for children.5 Systolic and diastolic hypertension were diagnosed using the NHBPEP recommendations as average systolic blood pressure or diastolic blood pressure that is greater than or equal to the 95th percentile for sex, age and height.5
Statistical analysis
All continuous variables were examined using P-P plots and found to be normally distributed. For descriptive analysis, continuous variables were presented as means and SD while categorical variables were reported as counts and percentages. Independent t-test analysis was used to assess sex differences in continuous variables, while χ2 tests were used to assess sex differences in categorical variables.
Pearson’s correlation was used to examine associations between the various adiposity indicators with systolic and diastolic BP z-scores. These associations were then further adjusted for child age, sex and fathers’ education in linear regression. To explore the association between adiposity indicators and systolic and diastolic hypertension, unadjusted Poisson regression was used. These models were subsequently adjusted for age, sex and fathers’ education. Estimates of relative risk (RR) of systolic and diastolic hypertension were reported as incidence rate ratios (IRR) with 95% CI.
Following regression analyses, we used the area under the receiver operating characteristics (ROC) curve to compare the accuracy of the different adiposity indicators in estimating hypertension risk for both sexes. ROC analysis is a method widely known for assessing the accuracy of a diagnostic test in determining a particular health outcome. ROC analysis is a plot of sensitivity (true positive rate) against one minus specificity (true negative rate) for different cut-offs for the outcome. Using the highest Youden’s index (J) (a summary measure of the ROC curve) calculated as J=Sensitivity- (1-specificity), we determined cut-off values for the adiposity indices that optimise both the sensitivity and specificity of the adiposity indicators for identifying hypertension. Likewise, the area under the curve (AUC) was used to examine the overall strength of the adiposity indicators in estimating hypertension risk (ie, AUC <0.7=poor; 0.7–0.8=fair; >0.8=good). Because the prevalence of hypertension in this sample was determined based on systolic hypertension, ROC analysis to determine the strength and cut-offs for the different adiposity indicators was limited to just systolic hypertension. Statistical analysis was done using SPSS V.24.0. P values <0.05 were considered statistically significant. This study was written in line with the Strengthening the Reporting of Observational studies in Epidemiology guidelines.25
Patient and public involvement
The research questions and outcome measures in this study were chosen by a team of researchers and clinicians with extensive experience working with the South Asian population to better understand the potential health risks faced by South Asian children. No patients were involved in in the development of the research question or study design. There are currently no plans to disseminate the results of this research study to study participants or to the relevant patient population.
Results
This study included 360 boys and 402 girls (n=762) between the ages of 5.8 and 17 years (mean age of 9.5±3.0 years). Mean non-transformed systolic BP was 109±11 mm Hg while mean diastolic BP was 65±8 mm Hg. Significant differences were observed between South Asian boys and girls for body fat percentage (p<0.001), WC z-score (p<0.001), WHtR z-score (p=0.02), non-transformed systolic BP (p<0.001), systolic BP z-score (p=0.001) and the prevalence of systolic hypertension (p=0.01). No significant differences were observed for age, BMI z-score, diastolic BP z-score and the prevalence of diastolic hypertension. Twelve per cent of this sample was found to have systolic hypertension (table 1).
Sociodemographic characteristics, adiposity measures and BP values stratified by sex
Consistent but weak to moderate associations were observed between adiposity measures (BMI z-score, WC z-score, WHtR z-score and body fat percentage) with systolic and diastolic BP z-scores using Pearson correlation. The strongest Pearson’s coefficient for systolic BP z-score was observed for BMI z-score (r=0.430 p<0.001), while the strongest coefficient for diastolic BP z-score was observed for body fat percentage (r=0.322 p<0.001) (table 2). After adjustment for covariates in linear regression analyses, the significant association between all the adiposity measures with systolic and diastolic BP z-scores remained consistent (p<0.001 for all) (table 3).
Pearson’s correlation between adiposity measures with systolic and diastolic BP z-scores
Adjusted linear regression between adiposity measures with systolic and diastolic BP z-scores
All adiposity measures had strong associations with systolic and diastolic hypertension (p<0.01 for all). The model with WC z-score had an IRR of 2.26 (95% CI 1.82 to 2.82) for systolic hypertension and an IRR of 1.83 (95% CI 1.30 to 2.60) for diastolic hypertension. WHtR z-score had an IRR of 2.12 (95% CI 1.73 to 2.60) for systolic hypertension and an IRR of 1.72 (95% CI 1.24 to 2.37) for diastolic hypertension. BMI z-score had an IRR of 1.82 (95% CI 1.59 to 2.09) for systolic hypertension and an IRR of 1.62 (95% CI 1.28 to 2.05) for diastolic hypertension. Lastly, the model with body fat percentage had an IRR of 1.10, (95% CI 1.07 to 1.13) for systolic hypertension, and an IRR of 1.09, (95% CI 1.04 to 1.13) for diastolic hypertension. On adjustment for covariates, the association between the adiposity indicators with both systolic hypertension and diastolic hypertension remained (p<0.001 for all) (see table 4). When compared with those with normal weight, children who were overweight or obese had an IRR of 6.19 (95% CI 3.73 to 10.26, p<0.001) for developing systolic hypertension and an IRR of 4.05 (95% CI 1.86 to 8.79, p<0.001) for developing diastolic hypertension. Similarly, when compared with children with WC <90th percentile, South Asian children with WC above the 90th percentile had an IRR of 4.41 (95% CI 2.91 to 6.68, p<0.001) for developing systolic hypertension and an IRR of 3.48 (95% CI 1.69 to 7.17, p=0.001) for developing diastolic hypertension.
Incidence rate ratios for systolic and diastolic hypertension per increment in adiposity measures
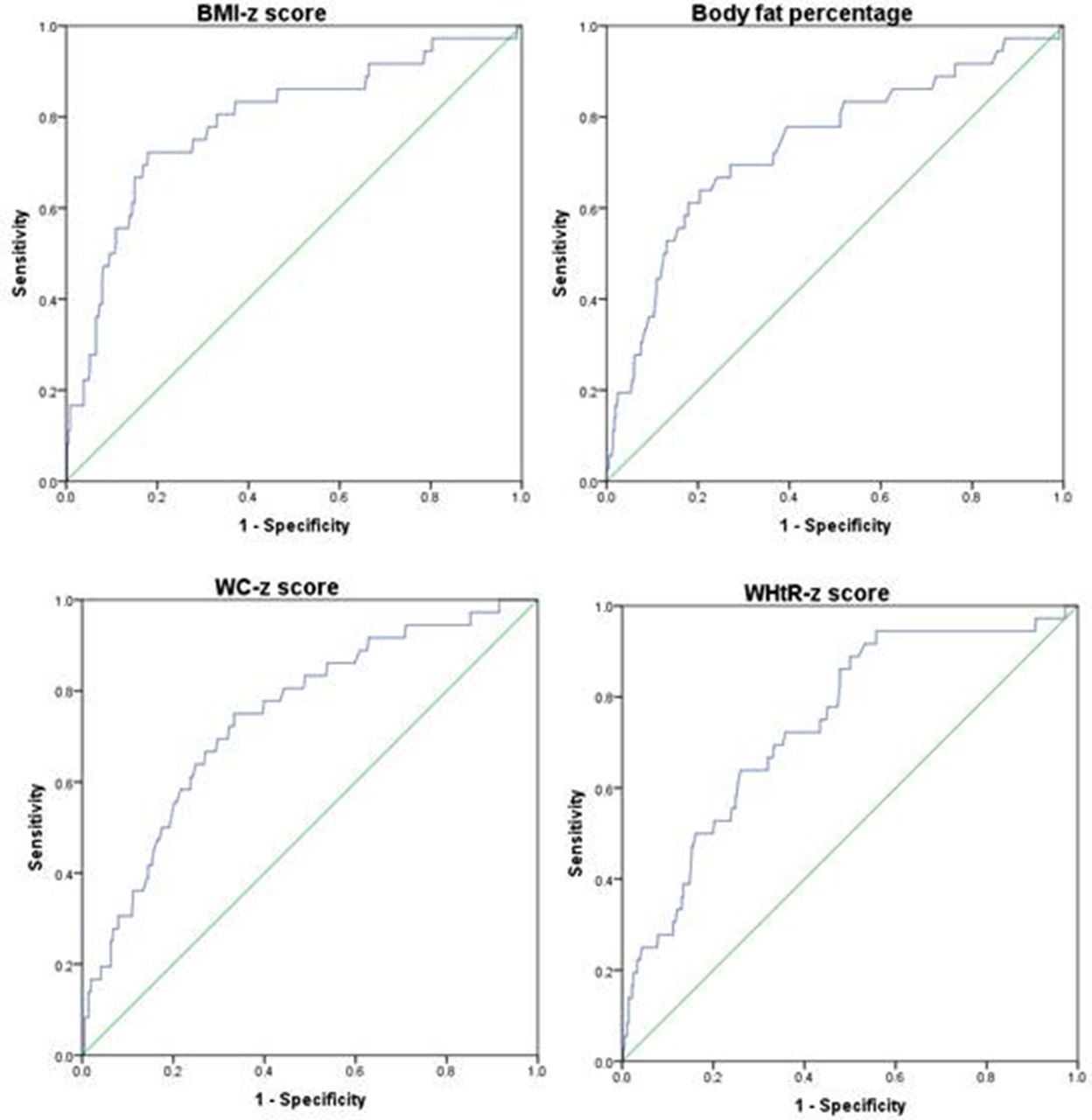
Figures 1 and 2 shows the sex-stratified AUC plots and their values estimating the accuracy of the adiposity indicators in identifying risks for systolic hypertension. All the adiposity indicators were found to be within the range considered to be fair in their ability to estimate hypertension risk for both sexes. In boys, body fat was observed to rank high in its ability to estimate the risk of systolic hypertension (AUC=0.80, 95% CI 0.74 to 0.86). The other adiposity measures were also found to be within close range of the AUC value for body fat, with BMI z-score coming next at (AUC=0.79, 95% CI 0.72 to 0.85), WC z-score at (AUC=0.78, 95% CI 0.71 to 0.85), and WHtR z-score at (AUC=0.77, 95% CI 0.70 to 0.84) (figure 1). In girls, the strongest measure was found to be BMI z-score (AUC=0.79, 95% CI 0.70 to 0.88), while body fat (AUC=0.74, 95% CI 0.65 to 0.83), WC z-score (AUC=0.74, 95% CI 0.66 to 0.83) and WHtR (AUC=0.74 95% CI 0.66 to 0.82) all had similar AUC values (figure 2)
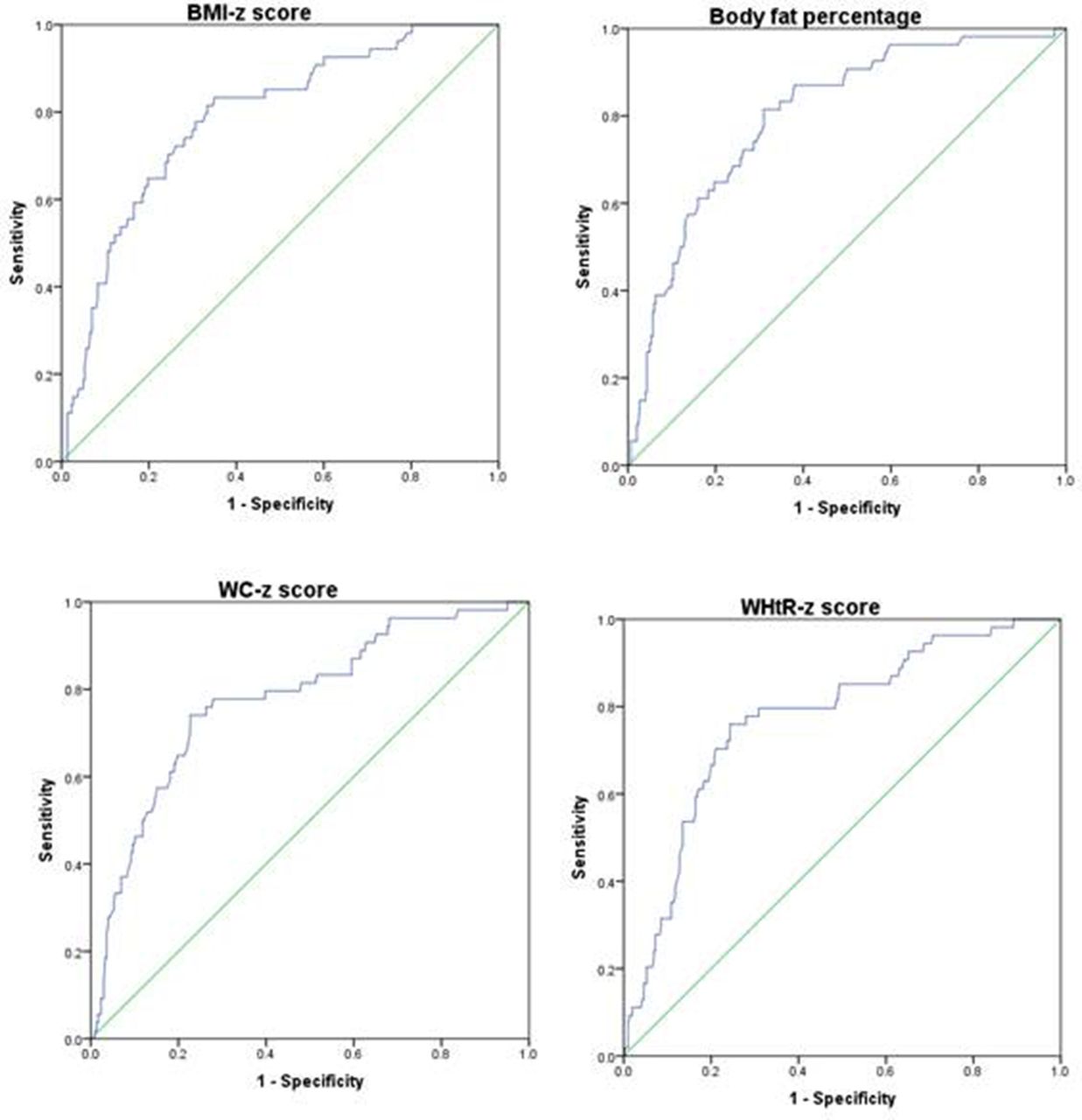
Receiver operating characteristics assessing the predictive power of adiposity measures and systolic hypertension in boys. Body mass index (BMI) z-score (area under the curve (AUC)=0.79 (0.72–0.85)); body fat percentage (AUC=0.80 (0.74–0.86)); waist circumference (WC) z-score (AUC=0.78 (0.71–0.85)); waist to height ratio (WHtR) (AUC=0.77 (0.70–0.84). P<0.001 for all.

{kind=link}
{kind=link}
Receiver operating characteristics assessing the predictive power of adiposity measures and systolic hypertension in girls. Body mass index (BMI) z-score (area under the curve (AUC)=0.79 (0.70–0.88); body fat % (AUC=0.74 (0.65–0.83)); waist circumference (WC) z-score (AUC=0.74 (0.66–0.83)); waist to height ratio (WHtR) (AUC=0.74 (0.66–0.82)). P<0.001 for all.
Sex-based cut-off values for the various adiposity indicators that were associated with adverse systolic hypertension risk, as identified using the Youden’s index, and their corresponding sensitivity and specificity values are outlined in table 5. The optimal cut-offs varied by sex with BMI z-score and body fat being higher in girls, and WC z-score and WHtR z-score higher in boys. The optimal cut-off for BMI z-score was 1.41 for girls and 0.92 for boys—corresponding to the 92nd and 82nd percentile, respectively, using WHO 2007 reference values. For body fat, the cut-offs were 29.8% and 23.5% for girls and boys, respectively. For WC z-score, the cut-offs were 0.39 for girls and 0.85 for boys, which corresponds to the 65th and 80th percentiles using the NHANES-III reference values. Lastly, the cut-off value for WHtR z-score for girls was 0.32, while that for boys was 0.43, corresponding to the 63rd and 67th percentiles using NHANES-III reference values.
Sex-specific cut points in adiposity measures for identifying individuals with systolic hypertension
Discussion
In this population of South Asian children, we found a high prevalence of hypertension at 12%. In addition, consistent positive associations were found between adiposity indicators with systolic and diastolic BP and systolic and diastolic hypertension. These associations remained on adjusting for sociodemographic measures. Moreover, being overweight or obese was associated with increased risk of systolic and diastolic hypertension. When sex-specific ROC curve analysis was used to validate the strength of all four adiposity measures in identifying risk of hypertension, we found them to be fair measures both in boys and girls as identified by their AUC scores. Likewise, we also estimated sex-stratified optimal cut-off values for the adiposity measures that were associated with hypertension. Combined, the broad consistency observed for the adiposity measures in their association with the BP z-scores, systolic and diastolic hypertension and their AUC values highlights their validity as fairly good measures for identifying risk of hypertension in South Asian children. The results also suggest that the adiposity measures included were similar in their ability to detect risk for hypertension.
In children, the global prevalence of childhood hypertension is not clearly known due to the lack of routine collection of BP data in children and variations in standards for defining hypertension. Evidence from US studies shows rates that vary from 1% to 5% and markedly higher rates in countries like China.26 In Canada, prevalence of hypertension in children ages 6 to 19 years was estimated at 4%.27 In terms of ethnic comparisons, our results are consistent with results from Jafar et al who found a 12% hypertension prevalence in South Asian children living in Pakistan.9 This estimate was in contrast to the 5% prevalence value predicted for Caucasian children in the USA.9 It is not clear if the rates observed in our study are representative of all South Asian children in Canada given that our sampling was restricted to volunteers in only two Canadian cities. However, the high rates obtained in this study compared with the Canadian average might be indicative of a disproportionately higher burden for hypertension in the South Asian paediatric population.
Our results showing associations between adiposity and BP and hypertension are consistent with many studies which have also explored similar relationships.28–32 Moreover, the consistency of the relationship between adiposity and hypertension in this study lends support to existing theories that attribute the increase in prevalence of hypertension in children partly to the concomitant increase in obesity.33 These observed associations have important clinical implications. BP has been shown to track into adulthood,34 suggesting that problems with hypertension in childhood—if sustained and left untreated—may progress into adulthood. This in turn might result in a cascade that affects the cardiovascular and renal systems due to known links between hypertension and damage to kidney function, vascular structure and function.35 36 Consequently, interventions aimed at preventing and treating obesity and hypertension should be prioritised in primary care, especially for South Asian children.
To our knowledge, this is the first study conducted with South Asian children that includes the range of adiposity measures we used. A few studies carried out in other children populations have shown findings comparable to our study results. For example, in validation analysis of adiposity indicators, WHtR appeared to be a strong indicator of hypertension in both sexes, while BMI seemed to be stronger in boys, but also observed to be a good measure in estimating hypertension risk in both sexes.19 Likewise, in children and adolescents who were overweight and obese, BIA-derived body fat was comparable to BMI in estimating hypertension risk.37 Given the South Asian obesity phenotype which lends itself to accumulation of fat in the abdominal region, and is a greater indicator of risk in adults than BMI, it was surprising to observe slightly higher AUC values for BMI in boys and girls when compared with measures such as WC and WHtR. Longitudinal studies conducted in South Asian children are needed to confirm how fat distribution might change in South Asian children as they age.
Sex differences in the optimal cut-offs for the adiposity measures associated with hypertension were found, suggesting that the adiposity cut-offs associated with hypertension might be sex specific. Moreover, when compared with reference standards from WHO for BMI, our results suggest that important considerations need to be placed in terms of differences in risk across ethnic lines. For example, WHO 2007 definition of obesity corresponds to the 97.7th percentile, while overweight corresponds to the 84th percentile.38 39 Based on this, the 82nd percentile observed in this study as the adiposity threshold for hypertension risk in boys would be considered normal weight using WHO reference. It is important to note that the WHO sample included a portion of children from a South Asian country. However, it is possible that the heterogeneity in the sampling might dilute risk detection, especially in those with heightened risk predisposition such as South Asians. Similarly, NHANES proposed the 90th percentile as the cut-off for WC in identifying risk from metabolic syndrome.40 Our findings of WC at the 65th percentile in girls and the 80th percentile in boys again underscore the fact that South Asians may be predisposed to CVD risk at lower fat levels. Our findings are comparable to a similar study conducted in Indian children which found that WC cut-off at the 70th percentile predicted risk of having two or more metabolic syndrome risk factors.41 For WHtR in the paediatric population, studies have estimated that the ≥0.5 threshold of concern used in adults remains applicable in children.42 43 This threshold corresponds to WHtR at the 65th percentile in girls and at the 77th percentile in boys.24 Similar to BMI and WC, our findings show that the threshold of concern appears to be much lower in South Asians (at the 63rd percentile for girls and at the 67th for boys).
Strengths and limitations
This study has two limitations. First, although we aimed to recruit a representative sample of urban South Asian children, it was not a random sample, and restricting sampling to only two Canadian cities might limit generalisability of the findings. However, given the focus of the study, a self-selection bias is unlikely. Second, this study is cross-sectional by design and as such limits to inferences about causality apply. The strength of the study lies in its large sample size of South Asian children.
Conclusion
We found BMI, BIA, WC and WHtR to be positively associated with BP and hypertension in an urban cohort of South Asian children in Canada. Additionally, the thresholds reported for the various adiposity indicators in identifying hypertension suggest that South Asian children are at risk of hypertension at levels of excess adiposity that are less extreme than those reported in the literature for predominantly Caucasian populations. Further research is needed to replicate our findings, and to confirm findings prospectively. However, the cut-offs provided for the four adiposity measures provide cut-off values that would be clinically useful in estimating and addressing risk for hypertension in South Asian children. Given the ease of use and practicality of the four adiposity measures, implementing them in primary care centres provides feasible and cost-effective methods for addressing the burden of hypertension in South Asian children. This would ensure that at-risk children are easily identifiable in primary care centres and afforded with the appropriate clinical interventions.
Acknowledgments
SAL is the Pfizer/Heart and Stroke Foundation Chair in Cardiovascular Prevention Research at St. Paul’s Hospital. CW is the Canada Research Chair in Children’s Health Policy. Research coordinators Pam Mackie, Michelle Tsigoulis, Veronica de Jong, Vaven Ghaat, Erica Corber and Amanpreet Thind were instrumental in completing the data collection for this project.
References
Footnotes
Patient consent for publication Not required.
Contributors SAL, ZP, KMM, MG, KT and SR conceptualised the study, contributed to study design and reviewed the manuscript. AOF conceptualised the study, drafted the initial manuscript, carried out statistical analysis and revised the manuscript. CW and MR contributed to the design of the study and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This study was funded by the Canadian Institutes of Health Research (FRN: 109206).
Competing interests None declared.
Ethics approval Simon Fraser University Research Ethics Board (REB), Providence Health Care REB, and the Hamilton Integrated REB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Raw data are held by the lead author of the study in accordance with ethics guidelines.