Article Text

Abstract
Introduction and aim Uncontrolled asthma is a global health challenge with substantial impact on quality of life (QoL) and overall healthcare costs. Unrecognised and/or unmanaged comorbidities often contribute to presence of uncontrolled asthma. Abnormalities in breathing pattern are termed dysfunctional breathing and are not only common in asthma but also lead to asthma-like symptoms and reduced QoL, and, in keeping with this, improvement with breathing normalisation. Evidence-based guidelines recommend breathing retraining interventions as an adjuvant treatment in uncontrolled asthma. Physiotherapy-based breathing pattern modification interventions incorporating relaxation have been shown to improve asthma-related QoL in primary care patients with impaired asthma control. Despite anecdotal reports, effectiveness of breathing retraining in patients referred to secondary care with incomplete asthma control has not been formally assessed in a randomised controlled trial (RCT). We aim to investigate the effect of breathing exercises on asthma-related QoL in patients with incomplete asthma control despite specialist care.
Methods and analysis This two-armed assessor-blinded multicentre RCT will investigate the effect of physiotherapist-delivered breathing retraining on asthma QoL questionnaire (MiniAQLQ) in addition to usual specialist care, recruiting from seven outpatient departments and one specialised clinic representing all regions of Denmark during 2017–2019. We will include 190 consenting adults with incomplete asthma control, defined as Asthma Control Questionnaire 6-item score ≥0.8. Participants will randomly be allocated to either breathing exercise programme in addition to usual care (BrEX +UC) or UC alone. BrEX compiles three physiotherapy sessions and encouragement to perform home exercise daily. Both groups continue usual secondary care management. Primary outcome is between-group difference in MiniAQLQ at 6 months. Secondary outcomes include patient-reported outcome measures, spirometry and accelerometer.
Ethics and dissemination Ethics Committee, Region Zealand (SJ-552) and Danish Data Protection Agency (REG-55–2016) approved the trial. Results will be reported in peer-reviewed scientific journals.
Trial registration number NCT03127059; Pre-results.
- asthma
- asthma control
- breathing exercises
- physiotherapist-delivered breathing retraining
- dysfunctional breathing
- asthma quality of life questionnaire
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- asthma
- asthma control
- breathing exercises
- physiotherapist-delivered breathing retraining
- dysfunctional breathing
- asthma quality of life questionnaire
Strengths and limitation of this study
This trial investigates the effects of physiotherapist-delivered breathing pattern modification and relaxation on asthma-related quality of life in patients with incomplete asthma control despite attending specialist care, a resource demanding group where evidence for management strategies are lacking.
The multicentre design including participants at secondary care centres in all regions of Denmark comparing a clinically relevant and low-cost intervention with usual care supports external validity.
Participants and treatment providers cannot be blinded due to the nature of the intervention.
Background
Asthma is a chronic, common, heterogeneous disease characterised by variable airflow obstruction due to airway inflammation and bronchial hyperreactivity.1 Globally, asthma affects around 300 million people. Dyspnoea is a very important symptom, which significantly restricts physical activity and quality of life (QoL).1 2
Asthma-related QoL describes the subjective impairment conferred by asthma on a person’s life, and is a key patient-reported outcome.3 It is impaired in most patients with asthma, and may be assessed by the validated MiniAsthma Quality of Life Questionnaire (MiniAQLQ).4 Several factors affect asthma-related QoL: (a) asthma-specific such as severity and type of asthma symptoms, (b) asthma-related such as triggers and comorbidities and (c) ‘patient-related’ factors, such as emotional stability, overall stamina, education and income.5–7
Asthma-related QoL is only moderately associated with asthma control, and asthma control remains the key metric for assessing the impact of living with asthma.6 Asthma control is currently defined as absence of key symptoms and signs of asthma (dyspnoea or coughing during night-time or exercise, exacerbations, and emergency healthcare usage), and no asthma-related impairment of activity or QoL.2 A tool widely used to measure asthma control is the Asthma Control Questionnaire (ACQ), which is available in 5-item, 6-item or 7-item versions, where item 7 is lung function expressed as percentage of expected forced expiratory volume in first second (FEV1 % expected).8 9
More than 10% of the asthma population has difficult-to-treat asthma with poor asthma control despite substantial pharmacological treatment (ie, Global Initiative for Asthma, GINA, steps 4–5).2 10 11 This subgroup uses high levels of asthma-related healthcare resources due to increased symptom burden, medication usage, prevalence of comorbidities, smoking, sick leave, higher exacerbation rates and emergency department visits compared with patients with asthma control.2 12 Likewise, individual costs to medication, unemployment, poorer education, sick leave, and early retirement are substantial too. True severe asthma is seldom the cause of difficult-to-treat asthma. Common causes are inadequate treatment (eg, adherence, inhaler technique), triggers (eg, smoking, allergens), erroneous asthma diagnoses or comorbidities (both: eg, non-asthma respiratory disease, obesity, rhinitis, cardiovascular diseases, dysfunctional breathing (DB), neuromuscular disease or poor cardiorespiratory fitness).2 13–17
Abnormalities in breathing pattern are usually referred to as DB. The extreme disordered breathing patterns range from fast and shallow to slow and deep. The first, for example, rate 20–40, thoracic breathing also known as hyperventilation, and the latter, for example, rate 5–8, diaphragmatic and whole thorax breathing, large tidal volume close to total lung capacity resulting in high ventilation volume.18 19 However, both patterns result in increased minute volume. A patient with disordered breathing pattern may sigh often to compensate for over-inflated lung and elevated tidal volume (eg, end of tidal volume over functional residual capacity, FRC) to achieve FRC (relaxation pressure of lung plus chest wall equals the atmospheric pressure).19 20 DB is well-recognised but ill-defined disorder that often coexists with asthma but may be an isolated problem and cause persistent or intermittent dyspnoea, coughing, loss of voice, chest tightness, anxiety and fatigue.2 13 15 21 22 There is no consensus on diagnostic criteria.21 The Nijmegen Questionnaire (NQ) is the commonly used screening tool,22–24 and estimates a prevalence of DB of 25% in Danish patients with severe asthma.25 However, the use of the NQ as a screening tool for DB in asthma has been questioned,26 and the NQ does not predict a response to intervention in controlled trials of breathing retraining.27 28
In asthma, pharmacological treatment targets airway inflammation, bronchoconstriction and possible comorbidities. Non-pharmacological treatment focuses on reduction of airway inflammation by avoidance of triggers, diet and physical fitness, and (in obese) weight reduction, to improve asthma control.2 29 Physiotherapy has gained increasing attention as part of asthma care as many patients with asthma explicit signs of DB pattern.15 30
Trained physiotherapists provide breathing exercises (BrEX) including re-education or modification of the breathing pattern. This involves instructions that encourage nasal route of breathing, mainly diaphragmatic respiratory movement, and normalising respiratory rate and tidal volume.31–33
In controlled trials in people with mild and moderate asthma (GINA steps 1–3), BrEX are safe, reduce symptoms, improve QoL and asthma control, but does not change lung function parameters or airways inflammation.28 34–37 Interestingly, the clinical effect of BrEX is unrelated to baseline NQ scores.26
Recent systematic reviews of BrEX in moderate to severe asthma conclude that the methodological quality and poor methods descriptions leave insufficient evidence for a firm recommendation.1 32 38 39
A previous, well-performed pragmatic-designed trial investigated a similar intervention (delivered by a DVD or face-to-face by a single physiotherapist) in patients in primary care in UK.28 The Danish healthcare system shares many similarities with the British NHS: Free health service for all citizens, all patients have a general practitioner (GP) who is the gate-keeper to secondary care. Asthma GINA steps 1–4 is the responsibility of the GPs, who can refer to the local hospital’s Respiratory Service in case of diagnostic uncertainty or lack of control. There are few multidisciplinary clinics for ‘difficult-to-control asthma’ in Denmark (total population 5.6 million inhabitants).
However, patients with more difficult to control asthma attending secondary, outpatient respiratory clinic have not to date been studied. Therefore, we decided to perform an adequately powered, randomised controlled clinical trial of well-defined BrEX in a well-characterised cohort of patients referred from GP due to lack of control and still having suboptimal control (ACQ6 score ≥0.8) of pulmonologist-diagnosed asthma after ≥2 consultations with a pulmonologist.
Thus, the present pragmatic multicentre trial will contribute to the existing (sparse) evidence on physiotherapy in asthma concerning target group (secondary care) and intervention (multicentre), the latter improving external validity of our findings.
The aim of our randomised controlled trial (RCT) is to compare changes in the key patient-reported outcome asthma-related QoL (MiniAQLQ scores) in patients undergoing a BrEX programme (three sessions and encouragement to do daily home exercise during 12 weeks) in addition to usual specialist care (US) with patients receiving specialist care management. Secondarily, we will investigate the effects of the intervention on important patient-reported outcomes, including lung function, gait distance and physical activity level.
Methods and analyses
Trial design
The trial is designed as a randomised, controlled, assessor-blinded multicentre superiority trial with two parallel groups with a primary endpoint of change in asthma-related quality of life (MiniAQLQ) at 6 months from initiating the intervention, that is, 12 weeks after intervention period.
The benefits achieved at 6 months are hypothesised to be maintained at 12 months.
Main trial information is presented in online supplementary file table S1.
Supplemental material
The trial protocol conforms to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT),40 and the Template for Intervention Description and Replication (TIDieR) will be used.41 The schedule of enrolment, interventions and assessments is shown in figure 1.
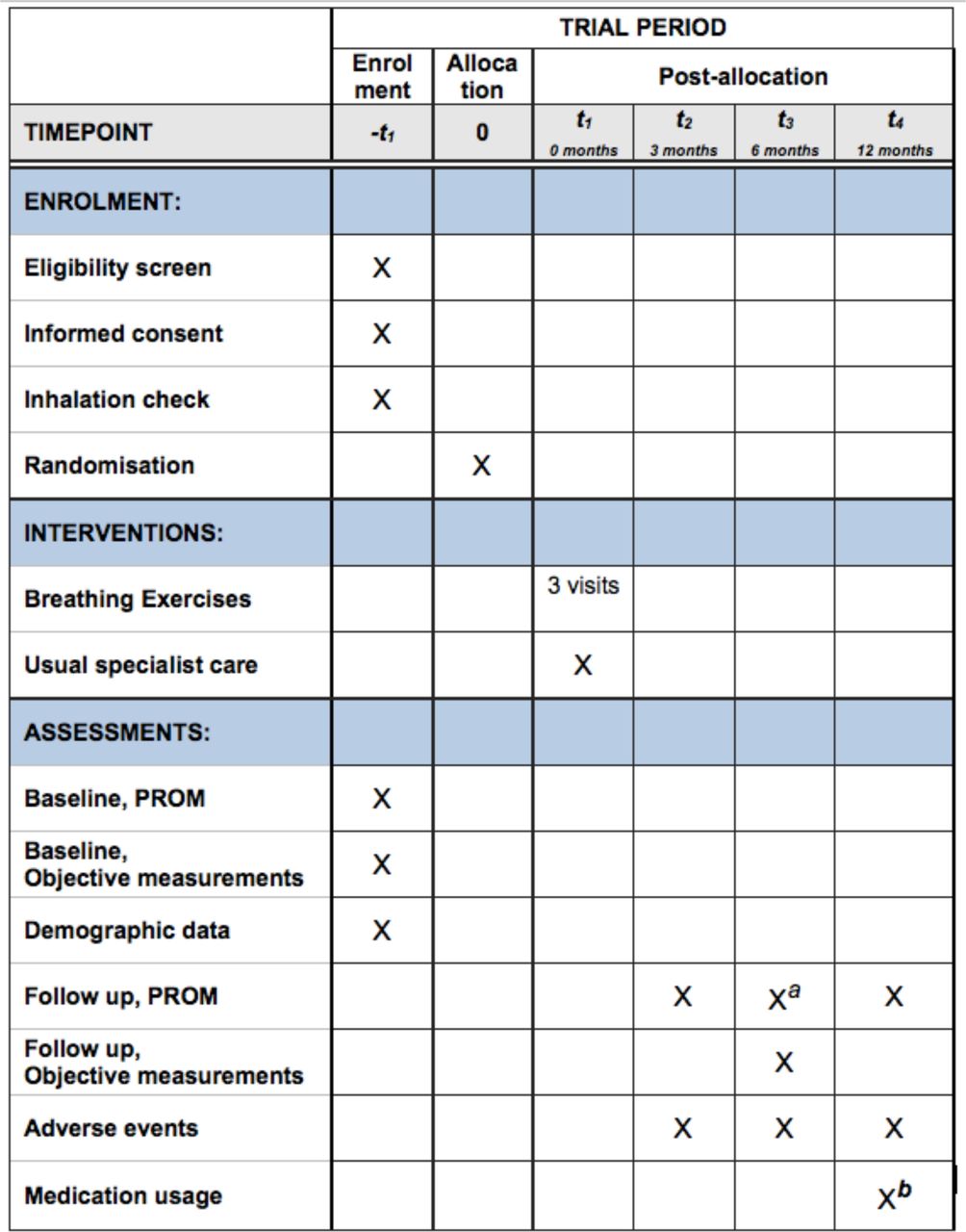
The figure details the schedule of enrolment, interventions and assessments of BEAT DB trial in accordance with the Standard Protocol Items: Recommendations for Interventional Trials template.40 BEAT DB trial: this acronym is used in ClinicalTrial.gov registration. a Primary endpoint is at 6 months follow-up. b Data collection of medication usage from baseline before allocation throughout until 12 months after allocation will be done at 12-months follow-up. BEAT DB, Breathing Exercises in Asthma Targeting Dysfunctional Breathing; PROM, patient-reported outcome measures.
The trial is registered on 26 April 2017. Enrolment started at the first centre on 26 April 2017 and at the last centre in January 2019. A much lower recruitment rate than expected were observed in the first months of the trial and the following actions were taken: inclusion criteria were modified (Protocol Version 2.4, see Participants), additional recruiting centres were initiated in March 2018, October 2018, and January 2019 (Protocol Versions 2.4–2.6, March 2018–January 2019), and based also on high retention rate, the sample size was revised based on updated power calculation in May 2019. We expect to end recruitment in October 2019.
Patient and public involvement
Participants in a pilot study on breathing retraining in asthma gave formal feedback on the intervention including information, patient instruction and follow-up (KH Andreasson, ST Skou, M Thomas, U Bodtger, 2017, ‘Breathing Exercise pilot study’, unpublished).
Participants
The target population is patients with physician diagnosed and specialist confirmed asthma, including patients with fixed airway obstruction, cough-variant asthma or other forms without current evidence of variable airflow obstruction,42 and incomplete asthma control despite specialist-provided asthma care and regular use of moderate-dose to high-dose inhaled steroids with or without a second controller (GINA steps 3–5). The diagnosis of asthma is not simple, and variable airflow limitation can be difficult to demonstrate in patients currently on treatment.14 43 Restricting the trial to those able to display physiological reversibility on treatment at recruitment into the trial would have resulted in a biassed and unrepresentative sample.
Danish respiratory outpatient clinics at Naestved, Roskilde, Bispebjerg, Aalborg, Hvidovre, Silkeborg and Odense hospitals, and the private Allergy & Lung Clinic, Elsinore (Allergi og Lungeklinikken Helsingør) will recruit consecutively during a 30-month inclusion period. Recruitment is expected to be finalised 31 October 2019.
The recruitment target is 190 participants with incomplete asthma control, randomly allocated 1:1 to intervention or control groups. At recruitment, ACQ6 ≥1.5 is used to identify participants with uncontrolled asthma. Modification was done 1 January 2018 to improve inclusion rates: participants will need to have an ACQ6 score ≥0.8 and to be in a stable phase of their asthma defined as no treatment changes in the month preceding randomisation to be randomised, while still having incomplete asthma control.
Inclusion criteria
Referred from GP to a secondary, outpatient respiratory clinic for lack of asthma control.
Asthma diagnosed by a pulmonologist.
≥2 doctor visits at a specialised, pulmonologist-lead asthma clinic.
Age≥18 years.
ACQ6 score ≥0.8.
Willing and able to give written informed consent.
Speaks, reads and understands Danish.
Exclusion criteria
Trained in breathing exercises by physiotherapist last 6 months.
Pregnancy.
Any severe disease as judged by the responsible physician.
Participating in another respiratory interventional research project.
Recruitment procedure and consent
The trial flow is outlined in figure 2. Written advertisements in the clinics pre-inform patients on the possibility of trial participation to motivate participation. The respiratory nurse or the pulmonologist will enrol eligible participants during the scheduled visit (which routinely includes ACQ6 scoring). The nurse will provide the initial oral and written trial information, and the pulmonologist will screen for eligibility. The participant will receive thorough verbal and written trial information and will have to return for a separate visit where a nurse or a physiotherapist will provide detailed information on the trial and respond to participant queries before written informed consent is obtained. Consent paper form, online supplementary file S2. If the enrolment rate is inadequate to meet the recruitment target, more centres will be invited to participate.
Supplemental material

{kind=link}
{kind=link}
Patient flow through the RCT BEAT DB trial. Consolidated Standards of Reporting Trials (CONSORT) flow diagram 2010. BEAT DB, Breathing Exercises in Asthma Targeting Dysfunctional Breathing; ACQ6, asthma control questionnaire; BrEX, breathing exercises; MiniAQLQ, miniasthma quality of life questionnaire; RCT, randomised controlled trial; UC, usual specialist care.
Randomisation procedure and concealment of allocation
After completion of baseline assessment, participants will randomly be allocated to UC with or without BrEX in a 1:1 allocation ratio by computer-generated randomisation using EasyTrial (EasyTrial APS, Aalborg, Denmark) in fixed blocks of four stratified by centre to assure equal size of groups at the seven centres. The chief investigator and all project workers will be blinded to the generation sequence. The nurse will activate the EasyTrial randomisation function to reveal the allocated group for each individual participant. This information will be forwarded to the participants by e-mail sent from EasyTrial. After allocation, the chief investigator will be informed and will ask the local physiotherapists to invite participants in the BrEX +UC group to initiate the intervention.
Blinding
The nature of the trial precludes blinding of participants or the physiotherapists delivering BrEX. Outcome assessors are blinded to the randomisation result, and participants will be reminded not to disclose their treatment allocation to the outcome assessor. Nurses who will perform extraction of clinical data from medical reports, and the statistician who will perform the analyses will also blinded to the allocation.
Blinded results (presented as group A compared with group B) will be presented to the research group, who will interpret the blinded results and prepare two alternative conclusions, prior to unblinding of the trial results.44
Interventions
At baseline, all participants will receive individual instruction in optimal inhalation technique by a respiratory nurse, who will also encourage the participant to use online video instructions.45
As the design is a pragmatic ‘real-world setting’ trial without standardisation of asthma therapy, the pharmacological treatment will be the choice of the responsible respiratory specialist, including changes, discontinuation or add-on of any treatment/combination. Treatment with positive expiratory pressure devices is not prohibited. The patient will be randomised to either usual care with Breathing Exercises (BrEX +UC) or usual care alone (UC).
Breathing Exercises (BrEX)
BrEX consists of three physiotherapist-sessions with duration of 60 min (initial session=week 1) and 30 min (at weeks 4 and 9, ± 7 days).
BrEX session one is t1 in the group of usual specialist care with BrEX (BrEX +UC) figure 1.
The participant will be encouraged to do 10 min of home exercise twice daily.32 The entire intervention combines elements of the Papworth method46 and the Buteyko technique.47
Key points in the intervention are
Modification/normalisation of respiratory rate and/or depth of breath by rhythmic, nasal inspiration, and diaphragmatic breathing, by long expiration, and by breath holding at FRC.32 46 47 Uncontrolled, non-phlegm coughing and frequent sighing are often seen in patients with disordered breathing pattern. The participant will be trained to reduce sighing and/or coughing by a suppression-technique.48
Relaxation,32 46 especially of the neck, jaw, tongue and shoulders. We will emphasise the lowering of muscle tone in these areas and boost the feeling of gravity. The participant will be asked to ‘let go’ to get full support from the surroundings (pillow, plint, chair and ground) to increase feeling of being carried.
Use of the breathing modification during walk and other physical activities.32 46
Daily home exercise of BrEX.
The participant will receive a booklet covering all exercises in text and illustrations, theoretical information about breathing patterns and modification, and a page designated for an individualised home programme specified by the treating physiotherapist.
See TIDieR table (table 1) and Supplementary note for details on the BrEX intervention (online supplementary S3), and 12-item interview list (online supplementary S4). Danish version of the participant booklet and an English translation will be available on request, when the trial data collection has finished.
Supplemental material
Supplemental material
Overview of the BrEX intervention
Usual specialist care
Participants in both groups will receive UC, which will be provided at the discretion of the responsible pulmonologist based on the individual needs of the participant’s severity of disease and current level of asthma control. The UC is not a uniform intervention neither in contents nor in time spent (range 15–30 min), number of visits, nor visit intervals. The choice of pharmacotherapy is supported by step-up and step-down guidelines.2
The UC without BrEX group will be the control group in the trial and baseline date equals t1 in this group figure 1.
Data collection procedure and retention
Data will be collected at baseline (t1) and at 3, 6 and 12 months (t2−t4). Overview of outcome collection is showed in table 2. Before RCT initiation, all assessors will be introduced to, trained in, and supervised in the assessment procedure by the chief investigator. All assessors will be provided trial-specific assessment manuals, which have been tested in a pilot study (KH Andreasson, ST Skou, M Thomas, U Bodtger, 2017, ‘Breathing Exercise pilot study’, unpublished).
Overview of data collection in BEAT DB
Patients-reported outcome measures (PROM) will be collected using online questionnaires in EasyTrial. Participants will receive invitation and links by e-mail, and—if necessary—an SMS reminder 2 weeks later (t1-t4 plus 2 weeks).
SenseWear (SW) data (accelerometry) will be extracted and entered by a research assistant not involved in any clinical parts of the trial.
Objective assessments will be done at the hospitals at baseline and at 6-month follow-up (±4 weeks) following a standardised procedure. The assessor will manually complete a datasheet, which will be entered as an electronic CaseReportForm in EasyTrial later.
The 6-month follow-up visit (t3) will be planned by phone with the participant by a coordinating research assistant. Two days before the scheduled follow visit, the participant will receive standard reminders by e-mail and SMS. If the visit is not completed, no matter the cause, the coordinating research assistant will contact the participant by phone to reschedule the visit within the pre-specified time frame of maximally +4 weeks.
Participants will be prompted to complete 3-month and 12-month follow-ups every second week until completion, reminders sent as SMS and e-mails after 2 weeks, and a phone call after 4 weeks.
If a participant discontinues the assigned allocation without withdrawing the consent, we will prompt him/her to remain in the trial that is, to complete the remaining follow-up visits/online questionnaires.
Reasons for non-adherence (eg, lack of interest, comorbidity reasons, exacerbation, emigration) and for non-retention (consent withdrawal, lost to follow-up) will be recorded.
Outcomes
Demographic data will be collected at baseline: gender, age, body mass index, smoking status and socioeconomic status (educational level, work status, and income).
Primary outcome
Primary outcome is the between-group mean change in MiniAsthma Quality of Life Questionnaire (MiniAQLQ) from baseline to 6-month follow-up.4 MiniAQLQ is a validated, 15-item disease-specific PROM on experiences in symptoms, activity limitation, emotions and environment during the previous 2 weeks. A 7-point Likert scale (1=maximum impairment; 7=no impairment) is used, and MiniAQLQ-score is the mean of all items. In moderate to severe asthma cohorts, MiniAQLQ has good reliability (ICC 0.83–0.86) and strong validity (criteria validity to AQLQ, r≥0.80; construct validity against ACQ, r=0.69).4 49 The Danish version of MiniAQLQ is validated linguistically, although cultural adaptation is missing.50 51
Secondary outcome measures
Secondary (continuous) outcome measures are the between-group mean change for each. All secondary outcomes will be considered supportive of the primary outcome, that is, conclusions will only be guided by the primary outcome.52 53
Patient-reported outcomes
ACQ6 is the 6-item questionnaire version on asthma control addressing five symptoms using a 7-point Likert scale (0=fully controlled; 6=severely uncontrolled), and reliever medication use (0=No use; 6=More than 16 puffs most days) during the previous 7 days. Test–retest reliability of ACQ is excellent (ICC 0.83–0.90).8 9 ACQ6 is valid in moderate to severe asthma; Cronbach’s α is 0.86 (KH Andreasson, U Bodtger, ST Skou, M Thomas, J Comins, 2019, ‘Rasch validation of the Asthma Control Questionnaire’, unpublished results). ACQ score <0.75 corresponds to well-controlled asthma, ACQ score ≥1.5 denotes uncontrolled asthma, whereas ACQ from 0.75 to 1.5 correspond to incomplete asthma control or partly controlled asthma.2 8 54
NQ is a reliable 16-item screening questionnaire designed to assess subjective sensations compatible with hyperventilation during previous 7 days.23
Hospital Anxiety and Depression Scale (HADS) contains seven items concerning anxiety, and seven concerning depression and uses 4-point Likert scales; a low score indicates least mental health problems.55 Asthma and disordered breathing pattern are known as associated with anxiety and depression.56 57
Global perceived effect (GPE) rate will be used as a retrospective evaluation of effect of asthma-related QoL as well as asthma control on a 7-point Likert scale.58 59 This global transition rating enables investigation of the validity and the interpretability of the primary outcome.59 60 This will be followed by the dichotomous Patient Acceptable Symptom State (PASS) that evaluates treatment success from the participant’s perspective related to level of asthma-related QoL and to asthma control.61 If the participant considers the symptom state to be ‘non-acceptable’, the participant will be asked whether he/she considers the state so unsatisfactory that Treatment Failure (TF) has occurred, answered by ‘yes’ or ‘no’. GPE, PASS and TF will be used at all follow-ups.
EuroQol-5Dimension is a generic QoL tool consisting of a 5-dimension descriptive index (ranging from −0.59 to 1.00) and a Visual Analogue Scale (ranging from 0 to 100) describing self-perceived health status.62 63
Foster Score will be used to define the numbers of days (0–7) per week that the participant reports having taken his/her medication as prescribed.64
Objective performance outcomes
Physical activity level (PAL), metabolic equivalents, numbers of steps, and total energy expenditure (TEE) will be measured by a two axial accelerometer (SenceWear, SW) (BodyMedia SenseWear, Pittsburgh, PA, USA) monitoring activity during 6 days.65 This is measured in all participants included May 2017–May 2018, hereafter only in participants from Naestved and Hvidovre Hospitals.
Functional capacity will be measured by 6 min Walk Test (6MWT). The 6MWT is a validated measure of response to physical activity intervention in respiratory research.66
Dyspnoea level will be measured before and after 6MWT. To rate perceived dyspnoea the validated Borg CR10 will be used,67 as well as the Count Scale (CS).68 CS implies that the participant loudly counts starting from one to as high as possible at a constant speed of 2 counts per second, guided by a metronome, during one exhalation from maximum inspiratory level.
Breathing pattern observation during 60 s, following a non-validated 10-item observational list assesses the respiratory pattern at rest. See table 3.
Breath Holding Time (BHT)69 will be measured in seconds from respiratory resting position (eg, FRC) until first involuntary respiratory muscle motion.
Spirometry (MedikroPro, M915, OY Finland) will be used to measure FEV1, forced vital capacity (FVC), FEV1/FVC ratio and peak expiratory flow rate.70 Predicted values will be calculated using GLI2012.71
Inspiratory muscle strength (Maximal Inspiratory Pressure, MIP) will be measured by KH2 (POWER Breathe, Southam, Warwickshire, UK).72
Breathing pattern, 10-item observational list
Register data from medical records
We will extract medication prescriptions and comorbidity at baseline, and medication prescriptions, comorbidity, adverse events (AEs; eg, emergency room visits), and number of consultations at specialist care respiratory nurses and/or pulmonologists from baseline until 12-month follow-up from electronic medical records.
Adherence
Participants in BrEX +UC group will be asked to complete a BrEX home training diary during the 12 weeks of intervention. Number of exercising days and minutes used will be described. At sessions 2 and 3, the physiotherapist will evaluate the adherence to the home exercise programme in a numeric rang scale 1–5 (1=no adherence, 5=excellent adherence). The physiotherapist will re-schedule any missed appointments. Good adherence with BrEX is defined as completion of three treatment sessions.
Data management and data monitoring
Data storage follows requirements in GDPR and will be kept confident and safe in EasyTrial during and after the trial. The Danish Data Protection Agency (REG-55–2016) has approved the trial. Only the chief investigator will have access to the full dataset. Security is enforced by personal password and SMS passcode accompanied with limited assignation at different levels of EasyTrial to the individual worker. All paper forms are designated pseudonyms and transported in code-locked bag to locked file cabinet at Naestved Hospital.
All paper-based data will be verified by an independent duplicate data entry.
No stopping guidelines are scheduled and no Data Monitoring Committee is involved, as the interventions and assessments are deemed safe in former trials.
Sample size
As argued by Norman et al, 73 no universal minimal important difference (MID) exists, as MID depends on the clinical setting, population and the intervention. However, it can often be estimated as half a standard deviation (SD).73 Thomas et al. (breathing exercises vs education by a nurse in mild to moderate asthma) found a 0.38 change in MiniAQLQ score.27
We will use the effect size found in Thomas et al 27 as MID in our sample calculation (with a calculated SD of 0.76) and expect to find a similar or higher effect size, as (a) BrEX will be an add-on intervention to standard specialist care instead of a head-to-head comparison as in Thomas et al , and (b) as this secondary care asthma population is expected to have a higher disease burden due to asthma, that is, greater room for improvement.
There is an inherent risk of the trial being underpowered because the SD of MiniAQLQ after BrEX in secondary care is unknown. However, based on previous studies,27 28 we expect that our SD will be sufficient to reflect the population.
For the present trial, the sample size needed is 172 to detect a 0.38 unit difference between groups in MiniAQLQ score (SD of 0.76, power of 90%, and p value of 0.05 (two-sided)). To allow for drop-outs, we will aim to randomise 190 participants.
Statistical methods
Analysis of primary and secondary outcomes
Data will be analysed on an intention-to-treat basis, thus regardless of protocol adherence, using appropriate parametric or non-parametric tests depending on data distribution. Primary endpoint (between-group difference in change in the MiniAQLQ at 6-month follow-up) and other continuous variables will be analysed using a mixed effects model with subject being a random factor and visit (ie, baseline, 3 months and 6 months) and treatment arm (BrEX +UC or UC) being fixed factors and adjusted for baseline imbalance and treatment centre. These analyses will start in April 2020. Per protocol analyses in participant with good adherence will be done. Data at 12 months will be included in subsequent secondary analyses of long-term treatment results.
Imputations will only be done to explore results of SW, and sensitivity analyses (with and with-out imputation) will test robustness of these results. We will conduct an analysis of SW data to explore the effect of the intervention on PAL, TEE and steps per day.
Secondary analyses include a numbers-needed-to-treat (NNT) estimation and trial-specific cut-offs for clinically relevant differences in MiniAQLQ (primary outcome) to guide the clinical interpretation of the results. We will estimate NNT as formula 1/(TER−MER), TER being the event rate (proportion of responders, ie, participants improving at least corresponding to the clinically relevant difference, 0.5 units)49 in the BrEX group, and MER the event rate in the usual care group. We will calculate the trial-specific MID/responder threshold by subtracting the mean MiniAQLQ score for those reporting to have experienced a ‘small but not important change’ in GPE from those reporting ‘important change’ in GPE at 6 months.
Both adjusted and unadjusted results will be reported including 95% CIs. No interim analyses will be made. STATA 15.0 (StataCorp LP) will be used. P values<0.05 will be regarded statistically significant. Statistical analyses plan will be made publicly available before any analyses and unblinding of data.
Ethics, Dissemination and perspectives of the trial
Ethics and auditing
Region Zealand Research Ethics Committee approved this trial (SJ-552), and it will be conducted in agreement with the Helsinki declaration. Written informed consents will be obtained from all participants. At the recruitment interview, the participants will be informed that if they are allocated to usual care group they will be provided physiotherapy (BrEX) later, given the RCT will find a clinically relevant benefit.
Before informed written consent is obtained, potential participants will receive written information about the trial, after which research team members (nurse or physiotherapist, trained and supervised by chief investigator) will inform about the trial and answer any questions from the potential trial participant. The Regional Committees on Health Research Ethics are annually selecting a number of trials for auditing. The audit process is independent of research groups and sponsors.
Adverse events
We will ask participants about experienced AEs at every follow-up using open-probe questions, and record on standardises forms for reporting and analysis. Additionally, the medical records will be checked at 12 months follow-up for all AEs occurring during period of trial. We define an AE as respiratory events or other events during the trial, which may be related to aspects of trial participation leading to contact with the GP or hospital. All serious AEs, defined as life threatening or resulting in hospitalisation,74 will be recorded. If a participant sustains a trial related harm, the hospital assurance covers him/her.
Dissemination of results and protocol amendments
All results will be published, regardless positive, negative or inconclusive, in peer-reviewed journals in due time after trial completion and to follow the Consolidated Standards of Reporting Trials (CONSORT) statement.52
Exclusion criteria were modified on first of March 2018 when (a) other known cause of dyspnoea (eg, cardiovascular disease, other respiratory disease) and (b) neurological disease (cannot follow an instruction or close lips) were deleted.
Any important protocol modification will be reported to the Ethics Committee for approval, and they will be registered at ClinicalTrials.gov.
Perspective and additional knowledge for clinical practice
The present trial will provide evidence of the effectiveness of the BrEX programme in patients with incomplete asthma control despite attending specialist care and adhering to moderate to high doses inhaled corticosteroids (ICS) with/without a second controller (GINA steps 3–5).2 Asthma control is not obtained in the majority of patients,14 75 76 and new measures to improve patients’ daily life with asthma are needed. The trial results will add pivotal information to future evidence-based guidelines and clinical practice. Although primarily an effectiveness trial, we will also gain potential insights into the characteristics of responders and into the mechanisms of effectiveness. In particular, we will explore the predictive value of reduced BHT, comorbid anxiety and depression (HADS), socioeconomic status, smoking status, and PAL at baseline.
Acknowledgments
We thank all involved departments of respiratory medicine and departments of physiotherapy and occupational therapy mentioned below, who made necessary resources available and contributed in recruitment, inhalation check, assessment, and treatment of participants in the trial: Department of Physiotherapy and Occupational Therapy, Naestved-Slagelse-Ringsted Hospitals, Department of Respiratory Medicine, Naestved Hospital, Department of Physiotherapy and Occupational Therapy, Hvidovre Hospital, Respiratory Research Unit Hvidovre, Department of Respiratory Medicine, Hvidovre Hospital, Department of Physiotherapy and Occupational Therapy, Aalborg University Hospital, Department of Respiratory Medicine, Aalborg University Hospital, Department of Physiotherapy and Occupational Therapy, Bispebjerg Hospital, Respiratory Research Unit, Department of Respiratory Medicine, Bispebjerg Hospital, Department of Physiotherapy and Occupational Therapy, Zealand University Hospital, Department of Respiratory Medicine, Zealand University Hospital, Allergy & Lung Clinic, Elsinore, Department of Physiotherapy and Occupational Therapy, Silkeborg Regional Hospital, Pulmonary Disease Unit, Diagnostic Centre, Silkeborg Regional Hospital, Department of Physiotherapy and Occupational Therapy, Odense University Hospital, and Department of Respiratory Medicine, Odense University Hospital, Odense. Trial sponsor: Department of Physiotherapy and Occupational Therapy and Department of Respiratory Medicine, Naestved-Slagelse-Ringsted Hospitals, Denmark. The principal investigators at each centre, Charlotte Suppli Ulrik, Karin Dahl Assing, Kirsten Brændholt Rasmussen, Celeste Porsbjerg, Kirsten Sidenius, Charlotte Hyldgaard, and Hanne Madsen provided feedback on the trial, led procedures and set-up at the recruiting hospitals.
References
Footnotes
Twitter @KarenAndreasson, @STSkou
Contributors KHA, UB, STS and MT (Research group, ie, 'steering committee') contributed substantially to the concept and design of this trial. The chief investigator (KHA) developed manuals for recruitment, assessment, and treatment, written information, applications for grants, and approval assignments, made registry at ClinicalTrial.gov, introduced and supervised the recruitment, assessment, and treatment procedures to all involved physiotherapists and nurses, and led the data collection. UB, STS, and MT gave feedback. STS specifically contributed in description of the statistical analyses.KHA drafted the manuscript. All authors (KHA, STS, CSU, HM, KS, JSJ, KDA, KBR, CP, MT, and UB) provided intellectual feedback to the manuscript and approved the final version.
Funding The trial is funded by the following non-commercial funders: Naestved, Slagelse and Ringsted Hospitals’ Research Fund, Region Zealand Health Scientific Research Foundation, The Danish Foundation TrygFonden (ID: 117031), and the Association of Danish Physiotherapist’s Research Fund. STS is currently funded by the Independent Research Fund Denmark (DFF – 6110-00045) and the Lundbeck Foundation.
Disclaimer The funders have no part in the design of the trial and will not have any role in its execution, analyses, interpretation of results, or decision related to reports of the results. The funders did not have any role in this trial other than to provide funding.
Competing interests STS is an associate editor of the Journal of Orthopaedic & Sports Physical Therapy, has received grants from The Lundbeck Foundation, personal fees from Munksgaard, all of which are outside the submitted work. He is co-founder of GLA:D®, a not-for profit initiative hosted at University of Southern Denmark aimed at implementing clinical guidelines for osteoarthritis in clinical practice.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.