Article Text

Abstract
Objective We aimed to evaluate the association of the severity of left ventricular (LV) diastolic dysfunction with long-term outcomes in patients with normal ejection fraction.
Design Retrospective study.
Setting A single centre in Japan.
Participants We included 3576 patients who underwent both scheduled transthoracic echocardiography and ECG between 1 January and 31 December 2013, in a hospital-based population after excluding valvular diseases or low ejection fraction (<50%) or atrial fibrillation and categorised them into three groups: septal tissue Doppler early diastolic mitral annular velocity (e′)≥7 (without relaxation disorder, n=1593), e′<7 and early mitral inflow velocity (E)/e′≤14 (with relaxation disorder and normal LV end-diastolic pressure, n=1337) and e′<7 and E/e′>14 (with relaxation disorder and high LV end-diastolic pressure, n=646).
Primary and secondary outcome measures The primary outcome measure was a composite of all-cause death and major adverse cardiac events (MACE). The secondary outcome measure were all-cause death and MACE, separately.
Results The cumulative 3-year incidences of the primary outcome measures were significantly higher in the e′<7 and E/e′≤14 (19.0%) and e′<7 and E/e′>14 group (23.4%) than those for the e′≥7 group (13.0%; p<0.001). After adjusting for confounders, the excess 3-year risk of primary outcome for the groups with e′<7 and E/e′≤14 related to e′≥7 (HR: 1.24; 95% CI 1.02 to 1.52) and e′<7 and E/e′>14 related to e′<7 (HR: 1.57; 95% CI 1.28 to 1.94) were significant. The severity of diastolic dysfunction was associated with incrementally higher risk for primary outcomes (p<0.001).
Conclusion The severity of LV diastolic dysfunction using e′<7 and E/e′>14 was associated with the long-term prognosis in patients with normal ejection fraction in an incremental fashion.
- diastolic dysfunction
- preserved ejection fraction
- retrospective
- echocardiography
- cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The present study assessed the association of the e′<7 and high E/e′>14 with long-term outcomes in patients with normal ejection fraction in a hospital-based population.
We categorised them into three groups: e′≥7, e′<7 and E/e′≤14, and e′<7 and E/e′>14 based on echocardiographic findings.
Severity of left ventricular diastolic dysfunction using e′<7 and E/e′>14 was associated with the long-term prognosis in patients with normal ejection fraction in an incremental fashion.
The study was limited to subjects in a single centre in Japan.
Introduction
Diastolic dysfunction is common in heart disease and is recognised as an important major cause of heart failure.1 2 Cardiac echocardiography is the most practical routine non-invasive clinical assessment for evaluating left ventricular (LV) systolic and diastolic function with clinical and experimental evidence. Tissue Doppler imaging is the method of choice for assessing cardiac diastolic function. Mitral annulus velocity analysing using tissue Doppler imaging is used as a reliable index of diastolic function, relatively unaffected by preload effects.3–6 Previous reports have shown that abnormal tissue Doppler imaging parameters are powerful predictors of adverse outcomes in patients with hypertension,7 8 ischaemic heart disease,9 10 heart failure11 12 and atrial fibrillation.13
However, the difference in the prognostic impact of the severity of LV diastolic dysfunction has not been fully elucidated. The tissue Doppler early diastolic mitral annular velocity (e′) reflects LV relaxation.14 15 The ratio of transmitral Doppler early filling velocity (E) to e′ (E/e′) is suggested as a useful index in the estimation of left atrial pressure15 16 and surrogate measurement for LV end-diastolic pressure.17
In the present study, we categorised the grade of diastolic dysfunction according to tissue Doppler imaging parameters: e′≥7 (without relaxation disorder), e′<7 and E/e′≤14 (with relaxation disorder and normal LV end-diastolic pressure) and e′<7 and E/e′>14 (with relaxation disorder and high LV end-diastolic pressure). We evaluated the association of the grade of LV diastolic dysfunction with lont-term outcomes in a Japanese hospital-based population with normal ejection fraction.
Methods
Study population
We retrospectively analysed 4444 patients who had undergone simultaneous scheduled transthoracic echocardiography and ECG at Kitano Hospital during 1 January and 31 December in 201318–21 ordered at the discretion of the physician. A flowchart of the study population is shown in figure 1. A total of 730 patients who demonstrated severe or moderate valvular disease (aortic stenosis, n=133; aortic regurgitation, n=133; mitral stenosis, n=9; and mitral regurgitation, n=169), low LV ejection fraction (<50%, n=407), AF (n=496) were excluded due to the effects of the diseases on LV end-diastolic pressure or the transmitral Doppler early filling velocity. We also excluded the patients with no data regarding e′ and E/e′ (n=79). The study population in the present study was 3576 patients, who were categorised into three groups: 1593 with e′≥7 (without relaxation disorder) (44.6%), 1337 with e′<7 and E/e′≤14 (with relaxation disorder and normal LV end-diastolic pressure) (37.4%) and 646 with e′<7 and E/e′>14 (with relaxation disorder and high LV end-diastolic pressure) (18.0%). The cut-off of e′ and E/e′ were defined as <7 and >14, respectively.3 In addition, we also analysed the data using the age-adjusted and sex-adjusted e′ classification. The following equations were used to define the reference values of e′ for men: y = − 0.16 ∗ years+19.2, and for women: y = − 0.15 ∗ years+18.6 in the online supplementary figure 1.22
Supplemental material

Flowchart of the study population. AR,aortic regurgitation; AS, aortic stenosis; E, the transmitral Doppler earlyfilling velocity; e, transmitral Doppler early filling velocity; E′, the tissue Doppler early diastolic mitralannular velocity; LVEF, left ventricular ejection fraction; MR, mitralregurgitation; MS, mitral stenosis; TTE, transthoracic echocardiography.
The research protocol was approved by the Institutional Review Board of Kitano Hospital (approval number: P16-02-005). Informed consent was waived because this was a retrospective study. We disclosed the details of the present study to the public as an opt-out method and the notice clearly informed patients of their right to refuse enrollment. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a priori approval by the institution’s human research committee. Patients’ records and information were anonymised and deidentified before analysis.
Data collection
Using the transthoracic echocardiography database, we extracted data regarding wall thickness, LV diastolic dimensions, LV systolic dimensions, diameter of left atrium, left atrium volume index, LV ejection fraction and body mass index. From the ECG database, we extracted the cardiac rhythm data and recorded them as they were documented. Therefore, we could not determine whether atrial fibrillation was paroxysmal or persistent. The LV mass index and relative wall thickness were calculated using the formula recommended by the American Society of Echocardiography.23
We defined high relative wall thickness as a ratio >0.42. High LV mass index was defined as LV mass index >115 g/m2 for male patients and >95 g/m2 for female patients.23 The septal e′ was measured on the apical four-chamber view and the E/e′ ratio was calculated at the interventricular septum. The cut-off of e′ and E/e′ were defined as <7 and >14, respectively, according to American Society of Echocardiography guideline.3 Data from the two-dimensional transthoracic echocardiography were analysed at baseline. LV ejection fraction was measured using the Teichholz method or the modified Simpson’s rule methods. All transthoracic echocardiography measurements were determined using the average of at least three cardiac cycles.
We extracted patient information from their electronic medical records at our institution, including age, sex and type of disease (ie, ischaemic heart disease, International Statistical Classification of Diseases and Related Health Problems, Tenth Edition (ICD-10) codes I20, I21, I22, I23, I24 and I25; hypertension, ICD-10 codes I10, I11, I12, I13, I14 and I15; dyslipidemia, ICD-10 code E78; diabetes mellitus, ICD-10 codes E10, E11, E12, E13 and E14; and chronic kidney disease, ICD-10 code N18).18–20 The follow-up data from serial clinic visits were also collected retrospectively from the electronic medical records during June 2017.18–21
Outcome measures
The primary outcome measure was a composite of all-cause death and major adverse cardiac events (MACE) defined as acute heart failure, acute myocardial infarction, unstable angina pectoris, cerebral infarction, cerebral haemorrhage, and aorta and peripheral vascular disease requiring an emergent treatment. The secondary outcome measure was each component of primary outcome: all-cause death and MACE, separately.
Statistical analyses
Categorical variables are presented as numbers and percentages. They were compared using the χ2 test or Fisher’s exact test. The trend across the three groups were assessed by the Cochran-Armitage trend test. Continuous variables are expressed as mean (±SD) or median (IQR). Based on their distributions, the continuous variables were compared using the one-way analysis of variance (ANOVA) or Kruskal-Wallis test.
We compared the 3-year clinical outcomes among the three groups with (1) e′≥7, (2) e′<7 and E/e′≤14 and (3) e′<7 and E/e′>14. The cumulative incidences of clinical events were estimated using the Kaplan-Meier method, and the intergroup differences were assessed using the log-rank test. Multivariable Cox proportional hazards models were used to estimate the risk of primary and secondary outcomes associated with the three groups. The results were expressed as HRs and 95% CIs. We selected the clinically relevant risk-adjusted variables (the model 1: age >70 years, male, diabetes, hypertension, dyslipidemia, ischaemic heart disease, chronic kidney disease, high LV mass index, and the model 2: age as a continuous variable and other factors except for age >70 years) for the primary and secondary outcomes for use in the main analysis. Next, we used the multivariable logistic regression model including the grades of diastolic dysfunction as continuous variables to estimate the incremental impact on the primary outcome measure. Then, we performed the post hoc subgroup analysis stratified by subgrouping factors; age >70 years, male, diabetes, hypertension, dyslipidemia, ischaemic heart disease and chronic kidney disease. In addition, we also perform the analysis based on modified criteria using the formula mentioned above. Finally, we compared the net reclassification improvement level and integrated discrimination improvement degree among the original staging classification and the modified one regarding the improvement of prognosis prediction accuracy.
All statistical analyses were performed by physicians (YS, TK and YM) using JMP V.14 and R V.3.4.1, and the R package of survIDINRI V.1.1.1. All reported p values were two-tailed, and p<0.05 was considered statistically significant.
Patient and public involvement
No patient involved.
Results
Baseline clinical and echocardiographic characteristics
A total of 1593 patients had e′≥7, 1337 patients had e′<7 and E/e′≤14, whereas 646 patients had e′<7 and E/e′>14 (figure 1). The baseline characteristics of the study population are presented in table 1. There were significant differences in age, sex, history of atrial fibrillation, diabetes, hypertension, dyslipidemia, ischaemic heart disease, chronic kidney disease and echocardiographic parameters among the three groups (table 1 and online supplementary table 1). The values of left atrial volume index were 21.4 mL/m2 in the e′≥7 group, 21.2 mL/m2 in the e′<7 and E/e′≤14 group, and 28.0 mL/m2 in the e′<7 and E/e′>14 group.
Baseline characteristics of the study subjects and transthoracic echocardiography results of the patients
Clinical outcomes of the diastolic dysfunction
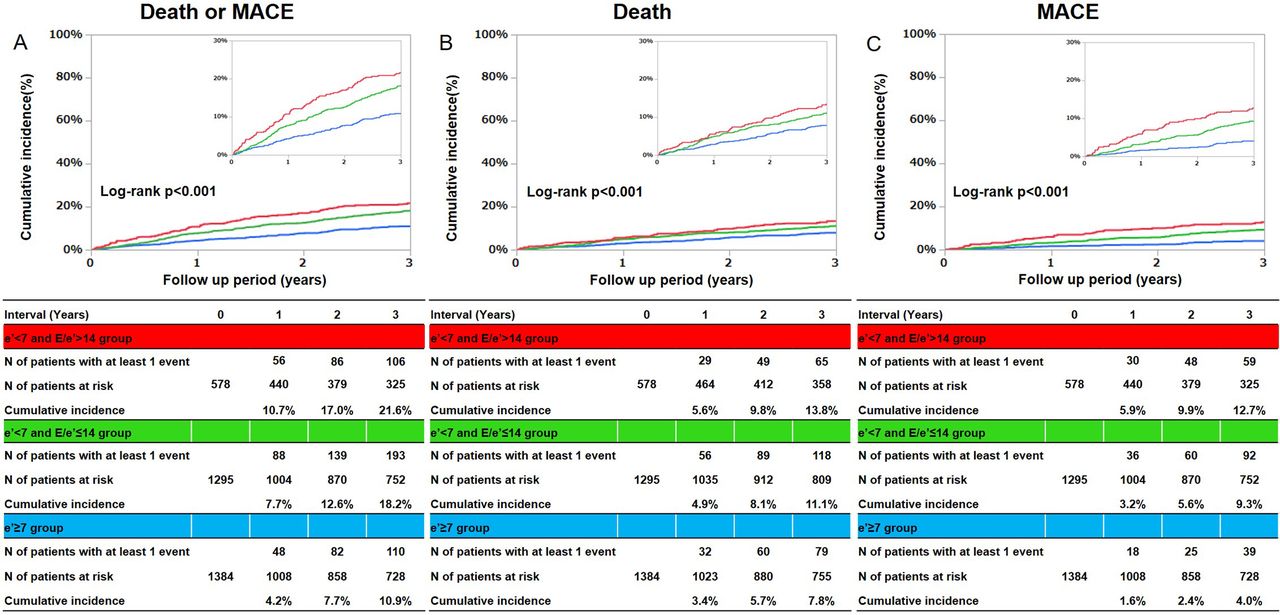
The median follow-up duration after index echocardiography was 1280 days (IQR, 440–1469), with a follow-up rate of 81.8% and 74.4% at 1 and 2 years, respectively. The cumulative 3-year incidences of the primary and secondary outcome measures were significantly higher in the e′<7 and E/e′≤14 group, and the e′<7 and E/e′>14 group than those for the e′≥7 group (figure 2A; composite of all-cause death and MACE, figure 2B; all-cause death, figure 2C; MACE). After adjustment for confounders, the excess risk of primary outcome measures in the e′<7 and E/e′≤14 group (HR: 1.24; 95% CI 1.02 to 1.52; p=0.032) and the e′<7 and E/e′>14 group (HR: 1.57; 95% CI 1.28 to 1.94; p<0.001) relative to that in the e′≥7 group remained significant (table 2). The excess risk of all cause death in the e′<7 and E/e′>14 group relative to that in the e′≥7 group remained significant (HR: 1.42; 95% CI 1.11 to 1.82; p=0.0049), whereas the excess risk of all cause death in the e′<7 and E/e′≤14 relative to that in the e′≥7 group was not significant (table 2). The excess risk of MACE in the e′<7 and E/e′≤14 group (HR: 1.54; 95% CI 1.13 to 2.16; p<0.001) and the e′<7 and E/e′>14 group (HR: 2.14; 95% CI 1.55 to 3.02; p<0.001) group relative to that in the e′≥7 group remained significant (table 2). When analysed by each component of MACE, the excess risk of heart failure in the e′<7 and E/e′>14 (HR: 2.82; 95% CI 1.51 to 5.88; p<0.001) group relative to that in the e′≥7 group remained significant (online supplementary table 2).
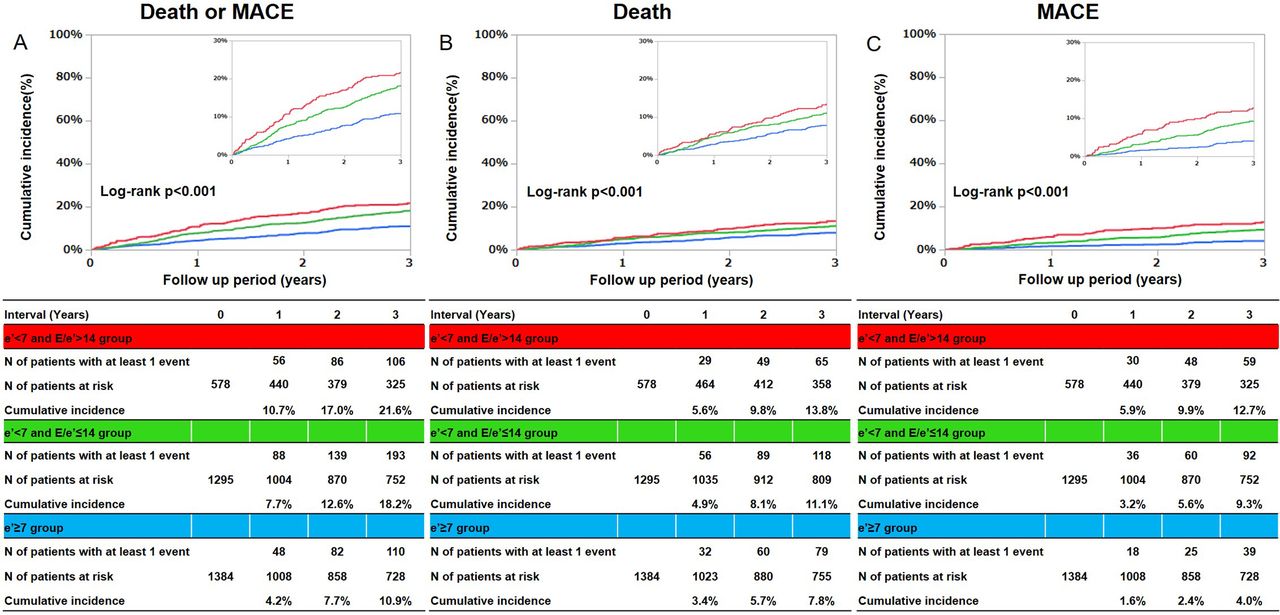
Cumulative incidence of the primary outcome measure (a composite of all-cause death and MACE) and secondary outcomes measure (all cause death, MACE). (A) A composite of all cause death and MACE, (B) all cause death, (C) MACE. MACE defined as acute heart failure, acute myocardial infarction, unstable angina pectoris, cerebral infarction, cerebral haemorrhage, aortic dissection and treatment of aortic aneurysm. MACE, major adverse cardiac event.
Clinical outcomes of patients in each grade of LV diastolic dysfunction
To further evaluate the association of the severity grade with long-term outcomes, we constructed the multivariable model using the severity grade as the continuous variables. The severity of grades was incrementally associated with higher risk for primary outcome measure (HR per 1 grade increase: 1.26; 95% CI 1.14 to 1.39; p<0.001), all cause death (HR per 1 grade increase: 1.22; 95% CI 1.08 to 1.38; p=0.02) and MACE (HR per 1 grade increase: 1.43; 95% CI, 1.24 to 1.65; p<0.001).
In the model 2 where we included age as a continuous variable, the e′<7 and E/e′>14 group (HR: 1.24; 95% CI 1.01 to 1.53; p=0.041) relative to that in the e′≥7 group remained significant, whereas the excess risk of primary outcome measures in the e′<7 and E/e′≤14 group relative to that in the e′≥7 group was not significant (HR: 1.04; 95% CI 0.86 to 1.27; p=0.69). The severity of grades was incrementally associated with higher risk for primary outcome measure (HR per 1 grade increase: 1.13; 95% CI 1.03 to 1.25; p=0.012).
Subgroup analysis
We performed the post hoc subgroup analysis stratified by subgrouping factors; the age >70 years old, sex and the comorbid disease (diabetes, hypertension, dyslipidemia, ischaemic heart disease and chronic kidney disease) (figure 3). There were no interactions between the presence or absence of diabetes, dyslipidemia and chronic kidney disease and the risk for the primary outcome measures. There were significant interactions between the age >70 years old, sex, and the presence of hypertension and ischaemic heart disease and the risk for the primary outcome measures in the e′<7 and E/e′≤14 group and the e′<7 and E/e′>14 group relative to the e′≥7 group.

{kind=link}
{kind=link}
{kind=link}
Subgroup analyses. DM, diabetes mellitus; HT=hypertension; IHD, ischemic heart disease; CKD, chronic kidney disease.
Additional analysis using age-adjusted and sex-adjusted value of e′
The baseline characteristics of the three groups based on the age-adjusted and sex-adjusted value of e′ are presented in online supplementary table 3. The cumulative 3-year incidence of the primary outcome measures were significantly lower in the low e′ and E/e′≤14 group (online supplementary file 2). According to integrated discrimination improvement and net reclassification improvement analysis, staging using conventional e′ and E/e′ showed a better prognosis prediction accuracy than the staging using age-adjusted and sex-adjusted value of e′ (online supplementary table 4).
Discussion
The main finding of this study is that the severity of the grade using e′ and E/e′ was stepwise related to adverse outcomes in patients with normal ejection fraction in a hospital-based population.
The e′ and E/e′ ratio can be applied for the estimation of LV diastolic dysfunction3–6 19 and is reported to be useful in the prediction of poor prognosis in patients with comorbid heart diseases.7–13 The combination of e′ and E/e′ ratio allows the evaluation of the relaxation property of LV and levels of LV end-diastolic pressure simultaneously; however, previous reports about this combinative evaluation of e′ and E/e′ ratio are very limited in dialysis patients.24 In the present study, we graded the patients according to the abnormal values of e′ and E/e′ as follows: (1) e′≥7 (without relaxation disorder), (2) e′<7 and E/e′≤14 (with relaxation disorder and normal LV end-diastolic pressure) and (3) e′<7 and E/e′>14 (with relaxation disorder and high LV end-diastolic pressure). The severity grade showed the incremental association with adverse events in patients who underwent scheduled transthoracic echocardiography after excluding patients with valvular disease, atrial fibrillation or LV ejection fraction <50%. Using the large clinical database, to the best of our knowledge, this is the first report showing the association of the severity grade of LV diastolic dysfunction with 3-year outcomes
in patients with normal ejection fraction in a hospital-based population.
Our data provide insights into the mechanisms why relaxation disorder leads to adverse outcomes through elevated LV end-diastolic pressure.1–3 It is currently not determined in the present study that patients in the e′<7 and E/e′≤14 group developed high E/e′ before the adverse events; however, the longitudinal examination will clarify the relationship between the disease trajectory and adverse events. The abnormality of e′ and E/e′ was linked to the increased risk of MACE defined as acute heart failure, acute myocardial infarction, unstable angina pectoris, cerebral infarction, cerebral haemorrhage, and aorta and peripheral vascular disease requiring an emergent treatment. As presented in the supplementary tables, not only heart failure but also vascular events were high in the e′<7 and E/e′≤14 and the e′<7 and E/e′>14 groups. Diastolic dysfunction may be related to the increased elasticity of artery caused by atherosclerotic change. In fact, we did not evaluate the atherosclerotic burden; however, Kim et al reported the association between arterial stiffness and LV filling pressure.25 Therefore, the assessment of e′ and E/e′ in routine echocardiographic practice is very helpful for risk stratification in patients with normal ejection fraction in a hospital-based population.
The subgroup analysis implies that the association of e′<7 and E/e′>14 with outcomes was directionally weak in patients over 70 years, the presence of hypertension and ischaemic heart disease, and women. The higher prevalence of non-cardiovascular events in aged people or ischaemic heart disease26 may hamper the association between diastolic dysfunction and outcomes. In addition, age dependence of e′ has been quantified recently.22 27 28 Age (in years) determines at least 80% of the velocity e′ in healthy and normal individuals. This dependence physiologically decreases e′ by 1% per year of age.22 The observation that the association of e′<7 and E/e′>14 with outcomes was directionally week in patients over 70 years supports the above problem. In addition, when we included age as a continuous variable into the adjusting model (the model 2), the trend of the risk was consistent, but it was hampered by the model construction including age as a continuous variable. However, we could not find the superiority of the classification using the age-adjusted and sex-adjusted criteria of e′ compared with that using the conventional criteria of e′ in the risk prediction. Our study population is a hospital-based population who underwent scheduled echocardiography. The results may differ from those found in the general population, but no studies have actually examined the long-term prognosis of the abnormality of the e′ value in the general population. In addition, there might be a difference between the age-adjusted and sex-adjusted normal values and the age-adjusted and sex-adjusted cut-off values to predict prognosis. Regarding E/e′, Yoshida et al reported an increase in E/e′ with age, in which mean E/e′ is from 6.5 in 20 s to 10.0 in 70 s and 80 s in healthy participants.29 Although the cut-off value of e′<7 and E/e′>143 had a prognostic impact in clinical settings in a hospital-based population, further study is needed to confirm the link between the age-adjusted and sex-adjusted criteria of e′ or E/e′ and the long-term prognosis in general population.
In patients with hypertension and ischaemic heart disease, the reference group (ie, the e′≥7 group) showed the high incidence of primary endpoints. Patients with hypertension and ischaemic heart disease are strongly associated with cardiovascular events30–34; LV hypertrophy and elevated blood pressure in patients with hypertension or interventional or pharmacological therapy in patients with ischaemic heart disease26 may be related to the prognosis of those patients. Thus, an additive value of e′<7 and E/e′>14 on the risk stratification may be limited in patients in the present study. A low prevalence of cardiovascular events in women, coupled with a gender difference in ventricular response to cardiac overload,34 may account for a significant interaction with the association of e′<7 and E/e′>14 with outcome. Although mild aortic stenosis can affect the loading condition, we could not perform subgroup analyses because of the very limited number of patients with mild aortic stenosis, as presented in online supplementary table 1.
This study had several limitations. First, ECG and transthoracic echocardiography were ordered at the discretion of the treating physician, with no standardised indications. Second, patient data were extracted from their electronic medical records. In addition, information regarding the symptoms was not included. Thus, we had no data regarding the proportion of heart failure patients with preserved ejection fraction18–21 nor the respiratory comorbidities, such as chronic obstructive lung diseases, obstructive sleep apnea and smoking status. Third, we use only septal e′ and E/e′ because only septal information was available for most patients. Fourth, this was a single-centre study performed in Japan; thus, possible selection bias could not be excluded despite the large sample size. Fifth, although we constructed multivariable Cox hazard models and used adjusting clinical variables in generally consistent with our previous studies,19 20 the numbers of event when stratified by subgrouping factors or each component of MACE were very small for the multivariable adjustment. Finally, there remain unmeasured confounders affecting the long-term prognosis. Nevertheless, we performed extensive statistical adjustments for the measured confounders. Further research is warranted to generalise this result in other populations or ethnicities.
Conclusion
The severity of LV diastolic dysfunction stratified by e′≥7, e′<7 and E/e′≤14, and e′<7 and E/e′>14 was associated with the long-term prognosis in patients with normal ejection fraction in an incremental fashion. The result indicated the importance of assessment of e′ and E/e′ in routine echocardiographic practice.
References
Footnotes
Contributors YS and TK: conceived the design, performed statistical analysis and wrote manuscript. MS, YM, YY, YH, EN, HH, TH and MI: collected the data and made critical revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.