Article Text

Abstract
Introduction Depression is a highly prevalent condition with typical onset in early adulthood. Internet-delivered cognitive behavioural therapy (iCBT) is a promising cost-effective and more widely available alternative to face-to-face CBT. However, it is not known whether it can reduce sickness absence in employees showing depressive symptoms. The randomised controlled trial component of the DAQI (Depression and sickness absence in young adults: a quasi-experimental trial and web-based treatment intervention) project aims to investigate if iCBT is effective in reducing sickness absence compared with care as usual (CAU) among young employees with depressive symptoms in primary care provided in an occupational health setting.
Methods and analysis This study will use a randomised controlled single-centre service-based trial of an existing iCBT programme (Mental Hub iCBT for Depression) to evaluate whether or not this treatment can reduce the number of sickness absence days in public sector employees aged 18–34 years who present at the occupational health service with mild depressive symptoms (score ≥9 on the Beck Depression Inventory-IA). Control participants will be offered CAU, with no constraints regarding the range of treatments. The active condition will consist of seven weekly modules of iCBT, with support from a web therapist. Primary outcome will be participants’ all-cause sickness absence as indicated in employer’s and national administrative records up to 6 months from study entry. Secondary outcomes relating to long-term sickness absence (over 11 calendar days) for mental and musculoskeletal disorders and psychotropic medication use will be obtained from the Finnish Social Insurance Institution’s administrative records; and short sickness absence spells (up to 11 calendar days) will be extracted from employer’s records. Analyses will be conducted on an intention-to-treat basis.
Ethics and dissemination The Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa has approved the study (HUS/974/2019). The results will be published in peer-reviewed scientific journals and in publications for lay audience.
Trial registration number ISRCTN10877837
- depression
- depressive symptoms
- online interventions
- web-based intervention
- RCT
- iCBT
- internet-delivered
- young workers
- sickness absence
- work disability
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- depression
- depressive symptoms
- online interventions
- web-based intervention
- RCT
- iCBT
- internet-delivered
- young workers
- sickness absence
- work disability
Strengths and limitations of this study
A study strength is the rigorous methodology, including the use of randomisation, an assessment by nurse and iCBT administered with a support from a web psychotherapist.
We will use employer’s and national registers to obtain information about primary and secondary outcomes; we will therefore not rely on self-reports on sickness absence or medication use.
This is a pragmatic randomised controlled trial and the control group is care-as-usual controls; therefore, the comparator treatment will comprise the form of usual care that control participants receive.
Due to our inclusion and exclusion criteria, there is likely to be a need to conduct a further trial of the intervention with respect to more severe cases of depression.
Introduction
Depression is the single largest contributor to non-fatal health loss worldwide,1 and it causes a vast burden on the quality of life, society, healthcare systems and the economy.2 Three quarters of all mental health problems are established by the age of 24, and for mood disorders the median age of onset is 30 years.3 Work disability is one of the key adverse outcomes of depression in young adults. Over the past few decades, the proportion of young adults receiving disability benefits has considerably increased across Western Europe4 with mental disorders being the leading cause.5–7 Across the 28 European Union countries, the total cost of mental ill health is more than €600 billion, equivalent to 4.1% of gross domestic product (GDP).8 In Finland, between 2005 and 2015, the number of newly awarded work disability pensions due to mental disorders among people under 35 years increased by 30%.9 These facts strongly indicate that interventions aimed at prevention or early treatment need to focus primarily on younger people.3 However, mental health conditions such as depression are widely untreated or the treatment is postponed or discontinued due to lack of resources, shortage of trained professionals, cost of services and stigma.10 11 This unmanaged situation calls for new modes of treatment, which are easily implemented, safe, scalable, easily accessible, convenient, affordable and avoid stigma. Internet-delivered treatments may be suitable especially for young adults, as these types of treatments are in line with their preference for self-reliance.12 In addition, as the uptake of psychological treatments in working populations is low,13 one way to address it could be the delivery of internet-based mental health interventions in occupational settings.14 Early treatment of depressive symptoms is important, as depression can significantly impair young adult’s quality of life, social functioning and attachment to the labour market.9
Cognitive behavioural therapy (CBT) is one of the most effective treatments for various mental health problems, and evidence-based clinical practice guidelines such as the National Institute for Health and Care Excellence guidelines recommend it as the first-line treatment for depression.15 Internet-delivered CBT (iCBT) includes the same components as face-to-face CBT, that is, psychoeducation, de-arousal, exposure and cognitive restructuring, but is administered via the internet.16 Content typically consists of series of lessons, assignments and supplementary material .17 Meta-analyses suggest that iCBT is equally effective as face-to-face CBT.18 19 Internet-delivered interventions have generally been shown to be effective in improving depression,12 17 20–23 both for those with severe depressive symptoms24 and for those with mild and moderate depression,25 26 as well as in increasing employees’ psychological well-being,14 but there is also some conflicting evidence showing lack of efficacy, particularly in primary care27 and in workplace settings.28
However, less is known about the extent to which this type of treatment can reduce work disability, for example, by reducing sickness absence. A possible pathway between reduction in depressive symptoms and decreased sickness absence is that timely access to adequate treatment can cut waiting times spent on sick leave.29 Even though sickness absence is also determined by many other factors other than symptom severity, such as poor general health and work stressors,30 in previous studies within-subject changes in the severity of depressive symptoms have been associated with within-subject improvement in sickness absenteeism.31
Moreover, the evidence for treatments targeted to employees with depressive symptoms is scarce.32 A reanalysis of data from five Australian randomised controlled trials (RCTs) showed that iCBT was associated with reduced self-reported sickness absence days among adults with depression or generalised anxiety disorder.33 In contrast, three recent studies indicated that there were no significant differences in sickness absence between those adults with depressive symptoms who were treated with iCBT and those receiving care as usual (CAU) in a primary care26 34 or in an occupational setting.35 However, in previous studies sickness absence was self-reported. More generally, in most RCTs, participants have been recruited through self-referral (advertisements) or via specialised iCBT clinics while fewer studies have been conducted in ordinary primary care settings.36 Together these issues limit the generalisability of the results and point to the need for rigorously conducted pragmatic RCTs. A pragmatic trial is a trial that is designed to evaluate the effectiveness of an intervention in real-life routine practice conditions; in other words, to test if the intervention works in real life. The aim of a pragmatic trial is to maximise the applicability and generalisability of the results.37 Previous studies have recommended the development and conduct of a pragmatic type of RCT as a robust test of the effectiveness of iCBT within routine clinical care20 38–40 and in non-specialised clinical settings.41 Furthermore, large-scale studies are warranted before wide-scale dissemination of iCBT programmes can be recommended.42 In order to address this knowledge gap, the RCT component of our DAQI (Depression and sickness absence in young adults: a quasi-experimental trial and web-based treatment intervention) study will test the effectiveness of an iCBT programme ‘Mental Hub for Depression’ compared with CAU in terms of reducing sickness absence among young (18–34 years old)43 employees showing depressive symptoms, using a large sample in a routine occupational health setting.
We hypothesise that the Mental Hub for Depression iCBT plus CAU compared with CAU will decrease sickness absence in young employees with depressive symptoms.
Method and analysis
Setting and participants
This is a single-centre, two-arm randomised controlled, CONSORT-EHEALTH guidelines44 compliant service-based pragmatic trial. The study will be conducted within Occupational Health Helsinki through an existing Mental Hub iCBT programme (https://www.mielenterveystalo.fi/en/Pages/default.aspx#) developed and offered by the HUS Helsinki University Hospital, the largest hospital district in Finland. The City of Helsinki is the largest employer in Finland, and its occupational healthcare provider Occupational Health Helsinki provides primary care services for all of the municipality’s circa 38 000 employees. In the Finnish healthcare system, the majority of employees seek medical help from their occupational health service (OHS) for any illness, including non-work-related. OHS is funded partly by employers and partly through tax-natured payments levied from all taxpayers. The use of services is free of charge for the employees at the point of delivery. Even if the study is conducted within the Occupational Health Helsinki, the study is separate from the healthcare provider–patient relationship; that is, the Principal Investigator and her research team are not responsible for the medical care of the participants.
The present study will be conducted in the Helsinki Health Study (https://www.helsinki.fi/en/researchgroups/helsinki-health-study) setting using the City of Helsinki personnel register data. These register data include sociodemographic and occupational factors, and short-term all-cause sickness absence data (1–11 calendar days). These data have been linked to long-term (over 11 calendar days) diagnosis-specific, ICD-10 sickness allowances (Social Insurance Institution (SII)), disability retirement, ICD-10 (Finnish Centre for Pensions), prescribed and reimbursed psychotropic medication (Anatomical Therapeutic Chemical Classification (ATC) obtained from SII) and all-cause mortality for censoring purposes (obtained from Statistics Finland). These linkages will be updated annually.
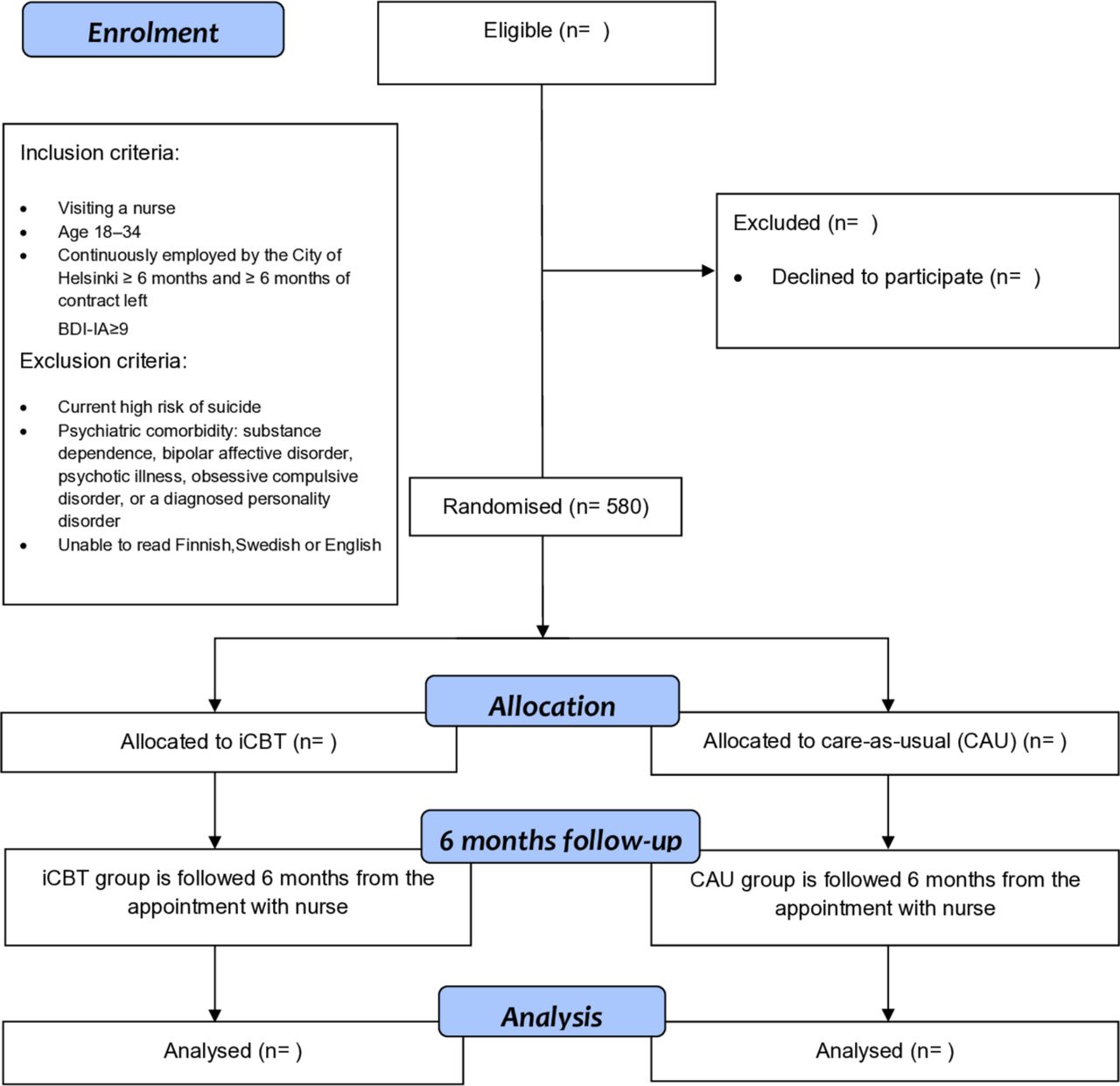
Figure 1 shows the participant flow through the trial following the CONSORT statement. The overview of the study procedures follow the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)45 (online supplementary file 1) and the intervention description follows the TIDierR guidelines.46
Supplemental material
{kind=link}
Study flowchart.
In the present study, the focus is on young employees. The occurrence of mental ill health and the patterns of sickness absence are different in different age groups. The transitions to independence are increasingly protracted especially in terms of permanent employment, which typically requires postsecondary educational qualifications. The European Commission’s Eurostat defines young employees as those aged 15–34.43
Inclusion criteria
(1) Visiting a nurse at the Occupational Health Helsinki with a mental health concern; (2) being 18–34 years old at the time of recruitment; (3) continuously employed by the City of Helsinki for at least 6 months before recruitment and permanent contract or a minimum of 6 months of fixed-term contract left; (4) score ≥9 on the Beck Depression Inventory-IA (BDI-IA).47 The BDI cutoff score was set relatively low in order to ensure sensitivity to work-related stress and burnout that have been shown to precede more severe depressive states in employee populations.48 Moreover, in comparison studies, BDI-IA has shown lower total scores than the BDI-II.49
Exclusion criteria
(1) Current high risk for suicide; (2) psychiatric comorbidity: substance dependence, bipolar affective disorder, psychotic illness, obsessive compulsive disorder, personality disorder; (3) not able to read Finnish, Swedish or English well (the intervention is only available in these languages). The first two will be assessed by the nurse using patient records and all available information. The third will be based on participants’ self-assessment. This is a pragmatic trial, a real-world evaluation of an existing iCBT programme. Therefore, we will impose no constraints on CAU participants’ use of the intervention and there is a possibility of potential crossover.27
Recruitment
At Occupational Health Helsinki, nurse is the usual first point of call for employees who experience any mental health difficulties. During the first appointment, BDI-IA will be routinely completed. If a patient in the target age group (18–34 years) scores≥9, has been employed by the City of Helsinki at least for 6 months, has at least 6 months of contract left and does not meet any of the exclusion criteria, he or she will be deemed to be eligible for participation in the trial. Next, the nurse will inform the patient about the study by providing them with general information about the study including a participant information sheet and consent form. Patients will be informed that participation in the intervention is voluntary, informed consent will be sought, their data will be pseudonymised and they cannot be identified from any study publications. Participants will be invited to sign the informed consent form to indicate that they have read and understood the study information including being free to withdraw at any time and without experiencing any negative feedback from the study team or related personnel. The form also states that regardless of their participation, they will continue to receive the treatment considered most appropriate for their condition by their nurse or physician. In Occupational Health Helsinki, the procedure is that patients experiencing depressive symptoms will routinely be offered a second appointment. If he or she wishes, the potential participant can thus take the participant information sheet home and decide on participation during the second visit. The fact that all patients, those patients who choose not to participate, as well as control group participants, will meet with OHS staff and receive their CAU significantly reduces any potential ethical risk. All nurses who participate in recruitment have been trained for their role in recruitment from one of the research team members who is pedagogically qualified and a trained OH nurse by prior profession with several years of work experience at the Occupational Health Helsinki. Recruitment will begin in October 2019 and will continue for 18 months or until the planned sample size is reached.
Patient and public involvement
Neither the patients nor the public was involved in the development of the research questions, selection of outcome measures, study design or study conduct.
Sample size calculation
The planned sample size is 580—calculated on the primary outcome of sickness absence days in 6 months follow-up. A power calculation with expected 8 days of sickness absence for each control group member during the follow-up, an incidence rate ratio (IRR) of 1.45 (control vs treatment) and dispersion parameter of 0.41 in negative binomial regression, a significance level of 5% and a power of 0.80 indicated that 290 participants per group are required. IRR of 1.45 for controls means that those in the intervention group will have 0.69 (1/1.45) times the sickness absence days compared with those in the control group. Thus, the sample size calculation was based on expected eight sickness absence days per a control group participant and 5.52 sickness absence days per a treatment group participant.
Randomisation
Participants will be randomly assigned to parallel groups in 1:1 ratio. Randomisation will be handled by a computerised random number generator administered by an independent statistician who is not involved in the study. The numbers corresponding to the treatment group (I=iCBT) and the control group (C=CAU), respectively, will be placed in sequentially numbered opaque sealed envelopes by a research assistant. The randomisation envelopes will be then manually assigned to all Occupational Health Helsinki nurses, who will in turn assign them to participants after the eligibility has been determined, trial discussed and written informed consent obtained. All researchers and nurses will be blind during the randomisation scheme; however, blinding for treatment allocation will not be possible as it will be clear to the referring nurse as well as the participant whether the participant has been allocated to iCBT treatment or the control arm. The allocation list will be stored in a password-protected file on the University of Helsinki server.
Outcomes
The primary outcome is the cumulative length of sickness absence, measured as sickness absence days in current and new spells during study period. The measurement includes sickness absence days between the study entry and the end of the 6 months follow-up from the study entry. Even if at the first stage of the study the follow-up is only 6 months, the data allow for a longer follow-up to be conducted at a later stage, as register data will be updated annually. In the participant information sheet, it has been stated that register data will be collected from 2019 to 2024, so the participants have consented to a possibility of a longer follow-up. The measurement will be based on the intention-to-treat (ITT) principle including sickness absence days for all study participants.
We will focus primarily on all-cause sickness absence but will additionally examine sickness absence separately for mental and musculoskeletal disorders as they commonly co-occur, and their co-morbidity is associated with a higher risk of work disability.50 51 By focusing on all-cause sickness absence, we can demonstrate the overall change in sickness absence. If sickness absence days decrease due to mental disorders, it is also important to confirm the change in the total absence days. Moreover, all-cause sickness absence was selected as primary outcome because we have no diagnostic data on short sickness absence spells. Short sickness absence spells constitute a large bulk of total sickness absence; by excluding these, we would have excluded a large number of absence days. An earlier study in the present study setting showed that the risk for long sickness absence for mental disorders increased with an increasing number of short sickness absence spells and days.52
The secondary outcomes are: (1) the cumulative length of long-term sickness absence both for depressive and anxiety disorders (F30-F48 diagnoses) from the SII’s register (over 11 calendar days); (2) the cumulative length of long-term sickness absence for any musculoskeletal disorder (M00–M99) from the SII’s register (over 11 calendar days); (3) the cumulative length of short sickness absence from employer’s records (up to 11 days) and (4) defined daily doses (DDDs) of prescribed anxiolytics, hypnotics and sedatives and antidepressant medication purchases (ATC classification codes: N05B, N05C, N06A with DDDs) from the SII register. Prescription data will be obtained from the Finnish National Prescription Register, which is a national pharmacy claims database kept by the SII. The measurements include sickness absence days and prescriptions between the study entry and the end of the 6 months follow-up. Overview of the outcome measurements is presented in table 1.
Outcome measurements
Treatment
The intervention (iCBT) will use an established mental health portal, structured web-based intervention model, the Mental Hub. The portal brings patients and professionals together through iCBT, which is available for a number of mental disorders. Referred patients can access therapy independently anytime and from anywhere except during working hours, and their personal web therapist who is a clinical psychologist monitors their development and supports them. Compared with the internet-based self-help interventions, therapist guidance or support during iCBT has been shown to improve treatment effect and reduce dropout rates53 54 and to be important for longer-term maintenance of symptom improvement.17 Adherence is monitored through full completion or by session or page completed. For example, patients who do not complete all seven sessions can still make substantial improvement by completing some of the sessions. Outside this study setting, a physician referral is required to access this therapy.
The Mental Hub can be used on a laptop, PC, tablet or smartphone and can be accessed in Finnish, Swedish and English. Mental Hub for Depression is a seven-module (therapy session) online CBT-based intervention using media-rich interactive content. The patient will access the platform using online banking details or a mobile ID (these are the typical means of accessing most public as well as many private online services in Finland). The sessions represent best practice principles used in CBT programmes for depression including behavioural activation, cognitive restructuring, problem solving, setting goals and challenging inner beliefs. The programme consists of similar treatment structures and methods as conventional standardised CBT programmes, which are commonly divided into steps or therapy sessions. Each module follows a structured format that can incorporate introductory quizzes, videos, informational textual content, interactive activities, as well as exercises in written and behavioural format, such as thought and behaviour recording, and summaries. Participants are expected to do their homework tasks prior to completing the next session. In addition, accounts from three fictional peer support persons, who are using iCBT and gaining mastery over their symptoms, are incorporated into the presentation of the material. Automatic messages of positive affirmation are sent to participants when they complete sessions and to remind them to complete further tasks as well as to inform them about new resources. The web therapist will give written feedback about progress and exercises during the treatment, and is available to answer patients’ questions. Patients can contact their web therapist via the portal any time and the therapist will answer within seven working days. Strict confidentiality rules apply; the therapist has a duty to notify the patient’s healthcare provider only if their patient displays suicidal ideation or tendencies. The tasks and instruments that are completed during treatment will be saved in the portal and patients can also make notes and save them within the system.
The typical length of the treatment is 7 weeks, with one session completed per week. The expected time to complete each session is 60 min. After 3 months of completion, there is a follow-up booster session. The effectiveness of any of the Mental Hub iCBT programmes has not been evaluated before.
Care as usual
CAU is defined as the routine care that employees receive when they are presenting with depressive symptoms at the OHS. All participants in the intervention arm and in the control group will have access to usual care. In practice, CAU may vary between patients and it is likely to include pharmacological treatment, psychotherapy, sickness certification, visits to OH physician, OH nurse, OH psychologist, referral to psychiatric nurse, ‘depression school’ (a Finnish self-help manual and associated group prevention and treatment programme that uses materials adapted from ‘Control your Depression’),55 peer support group, iCBT (physician referral required) or a combination of these. We will not interfere with CAU, which may cause some crossover. In an earlier pragmatic trial of a different programme, 19% of the CAU (control) group had used iCBT.27
Engagement and usage measures
The online system will collect descriptive data relating to engagement and use of the platform by service users. Every patient login, completed page and filled assignment or measurement is time-logged, as all are on-platform messages between the patient and the therapist. Engagement can be described, for example, as the completion time, sessions per week, number of messages sent to therapist and total actions performed during the course of the treatment.
Statistical analyses
Statistical analyses for the cumulative length of recorded all-cause sickness absence (the primary outcome) will be performed with statistical models suitable for count data, including, for example, Poisson, negative binomial, zero-inflated, hurdle or difference in differences models. The model selection will be based on the actual frequency distributions found in the data. Secondary outcomes with count data, namely recorded sickness absence days for mental (F30–F49) and musculoskeletal disorders (M00–M99), short-term sickness absence and psychotropic prescriptions, will be similarly assessed. The key measurement unit for psychotropic medication purchases is DDD. Stratified analyses can additionally be run separately for those with and without sickness absence spells during the intervention.
In subsidiary analyses, outcomes with a dichotomous measure, that is, measurements of incidence or recurrence of sickness absence or psychotropic medication purchases, can additionally be assessed with the most applicable advanced statistical methods such as Cox regression models, where the survival time is defined as the distance between the study entry date and the date of outcome occurrence or the end of the follow-up.
Data on register-based measurements will also be collected 6 months prior to recruitment.
We will use two-sided p values with alpha≤0.05 level of significance for all tests.
The analyses will be conducted as ITT analyses involving all randomised participants, all retained in the group to which they were allocated, regardless of adherence.
All statistical analyses will be conducted with R, SAS 9.4, Stata 16 or other advanced statistical software. Results will be reported following the CONSORT and TIDierR guidelines.44 56
Data management and data protection
The EU General Data Protection Regulation, Finnish data protection laws and the data protection guidelines of the University of Helsinki are followed strictly while storing and processing the data.
Each permanent resident in Finland has a personal identification (ID) number common to all registers.57 These IDs will be used to link the data sets on a University of Helsinki computer, but the ID numbers will be replaced by study IDs when the data are given to researchers. Data on accessing iCBT will be collected via Mental Hub software and stored on the Mental Hub server. Information collected via Mental Hub will be coded with a participant ID number to allow matching with sickness absence and psychotropic medication records. In the final data, participants are distinguished only by an ID number created for this study. All linked data will be collected and stored via the University of Helsinki server. Any identifiable information collected remains confidential. During data analysis, only non-identifiable data will be used. At study completion, non-identifiable data will be written to a password-protected database. Participants will be informed during the consent process at application that the research team plans to disseminate the trial results in peer-reviewed scientific publications and scientific and lay publications and presentations.
In this research, personal data is collected for scientific research purpose only, and it is not further processed in a manner that is incompatible with this purpose. The data are stored until 2030 and will be destroyed at the end of that year. All data files will be password-protected and can be accessed only by authorised members of the research team who will need to sign relevant confidentiality agreements.
The consent form is accompanied by a participant information sheet describing the purpose of the study, explaining that participation is voluntary, and the data processing and storing procedures.
The authors are aware of the right of the respondents to know what data related to him or her the researchers have, and to receive a copy of all personal data related to him or her. As advised by the University of Helsinki guidelines, the authors will contact the Data Protection Group if they receive such requests to ensure the correct course of action.
The risks related to processing the data are related to the possible annulment of anonymisation, which could lead to social harm for the respondents in the form of uncontrolled and unwanted access to their personal information, including health issues, which are categorised as sensitive information by the EU General Data Protection Regulation (GDPR). However, according to the GDPR, the use of this information for scientific purposes is permitted. Risk for the annulment is low because of secure data management. The risk of social harm produced by a possible data breach is also assessed as low by the authors.
Ethics and dissemination
The study will be conducted and reported following the CONSORT statement,58 the CONSORT extension for web-based interventions (CONSORT-EHEALTH)44 and the SPIRIT guidelines.45 The results will be published in peer-reviewed journals, lay publications and in conference and seminar presentations. We aim to publish our peer-reviewed papers in Open Access journals.
Discussion
This large-scale pragmatic RCT will evaluate the effectiveness of iCBT as a treatment for depressive symptoms for reducing sickness absence among young Finnish employees in an OHS setting. Although the effectiveness of iCBT for treating depression is well established,18 20 23 important knowledge gaps remain. To the best of our knowledge, this study will be the first iCBT RCT using register-based sickness absence as the primary outcome and one of the first large-scale pragmatic RCTs conducted in a health service setting in (younger) employees. The present study will make an important contribution to the evidence base about online treatments for depressive symptoms. The primary outcome measure is the cumulative length of sickness absence. The secondary outcomes are self-certified short-term sickness absence, long-term sickness absence for mental and musculoskeletal disorders and psychotropic medication use.
If successful, the study will have significant implications for the effects and feasibility of integrating iCBT into existing healthcare infrastructure and to increase the scalability of the healthcare system, improving the capacity to deliver evidence-based mental healthcare to more patients and reducing their sickness absence.
Strengths and limitations
The study has several strengths. First, we will employ a rigorous protocol including the BDI assessment by a nurse and iCBT administered with support from a web psychotherapist. Second, employer’s and national registers are used to obtain information about primary and secondary outcomes; we will not rely on self-reports on sickness absence or medication use and in terms of the data obtained from SII (long-term sickness absence and prescribed medication), and there is practically no loss of outcome data to follow-up. The use of an employee cohort and routinely collected sickness absence and medication data enables a sufficiently large and representative sample, and a better real-world generalisability. Third, the study population represents widely different occupational groups and both white-collar and blue-collar occupations. Fourth, our sickness absence follow-up is long, 6 months, and we will have an option for even extending the follow-up. We will therefore be able to pick up longer-term effects. Finally, we will test if iCBT is effective in routine clinical non-specialised setting.
However, the study has also some limitations. First, this is a pragmatic RCT and the control group is CAU controls; it is therefore not possible to control for the effects of usual care the control participants receive. Future studies should investigate the effectiveness of iCBT for reducing sickness absence in comparison with face-to-face CBT and active control groups. Second, participants in both the intervention and control group may take up other forms of treatment, but we will not be able to collect data on such treatments. Third, in iCBT trials there is often a risk for high dropout and attrition rates. However, earlier research indicates that even 50% attrition does not necessarily distort the results.59 Fourth, there may be variation between nurses in terms of the adherence to the randomisation procedure and picking up the cases with depressive symptoms. Fifth, the effectiveness of the Mental Hub iCBT in reducing depressive symptoms has not been evaluated.
Sixth, simultaneously addressing work environment factors would be important when aiming to reduce sickness absence. Unfortunately, in the present study we cannot implement workplace interventions such as work modifications. However, for all participants, that is, for both those in the intervention group and those receiving CAU, addressing the work environment such as recommending and implementing work modifications can be done, should the employers and OHS so decide. We can expect that due to randomisation these interventions do not differ between the intervention and the control groups. In the present study, we are able to test what is the contribution of iCBT to reduction of sickness absence.
Finally, if the employee terminates his/her contract with the City of Helsinki some point during the follow-up, we will not be able to follow them up for total and short-term sickness absence but only for long-term sickness absence and psychotropic medication use. However, in the City of Helsinki, the turnover is typically low, on average about 10% a year.
Despite these limitations, our study will provide novel evidence about the effects of iCBT to reduce sickness absence in young employees with depressive symptoms.
Trial status
The trial was launched in October 2019.
References
Footnotes
Twitter @AKouvonen, @JaakkoHarkko, @SamiPirkola
Contributors AK led the study design and funding application and, as chief investigator, has oversight for the trial. AK, MM, HS, JL, SP, OR and TL conceived the original idea of the study, and AK wrote the initial draft of the study protocol. HK, MD, BS, JB and EM-R helped to refine the trial design. JH, JL, OP and E-LK are responsible for day-to-day management of the study. JH and OP planned the statistical analyses. J-HS and SP have been involved in the development of the Mental Hub for Depression program. HS trained the nurses involved in participant recruitment. ET helped to adapt the trial into the study setting. ET, SP, BS and J-HS provided clinical expertise, and JB and EM-R provided assistance with the outcome measures. All authors have in different ways been involved in different degrees in the development of study design. AK, MM, JH, HS, HK, JL, OP, JB, ET, E-LK, J-HS, MD, BS, EM-R, SP, OR and TL have contributed to the protocol development and have read, critically revised and approved the final protocol.
Funding This work was supported by the Academy of Finland (grant 315343) and the City of Helsinki. The funding sources had no role in the design of this study and will not have any role during its execution, analyses, interpretation of the data or decision to submit results. The City of Helsinki representative attends some project meetings.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study will be conducted in line with the Declaration of Helsinki and the trial has been registered in a clinical trial register (ISRCTN10877837). The study protocol, information on the study, informed consent form, participant information sheet and other requested trial-related documents have been approved by the Coordinating Ethics Committee of Hospital District of Helsinki and Uusimaa, Finland (HUS/974/2019).
Provenance and peer review Not commissioned; externally peer reviewed.
Author note 2019.03.05 study protocol (original): 2019.05.10 study protocol (amendment 01): 2019.08.26 study protocol (amendment 02): 2019.09.23 (amendment 03). We will periodically update to the trial registration site for important protocol modifications and other changes after the publication of this paper.