Article Text

Abstract
Objectives To carry out meta-analysis and systematic review on the association between soft drinks consumption and asthma prevalence among adults and children.
Design Systematic review and meta-analysis of observational research.
Data sources Medline, Scopus, ISI Web of Science and the Cochrane Library were searched up to December 2018.
Eligibility criteria We included observational studies investigating the association between soft drinks consumption (including maternal consumption during pregnancy) and asthma or wheeze.
Data extraction and synthesis Data were extracted by one author and reviewed independently by two other authors. The most adjusted estimate from each original study was used in the meta-analysis. Meta-analysis was conducted using random-effects model. The quality of studies was assessed using the Newcastle–Ottawa scale and heterogeneity was evaluated using I2 statistic.
Results Of 725 publications originally identified, 19 were included in this systematic review, including 3 cohort studies and 16 cross-sectional studies. Ten articles reported on children up to 18 years, 5 articles on adults (>18 years) and 2 articles on prenatal exposure. In total, 468 836 participants were included, with more than 50 000 asthma cases. Soft drinks consumption was associated with significantly increased odds of asthma in both adults (OR=1.37; 95% CI, 1.23 to 1.52) and children (OR=1.14; 95% CI, 1.06 to 1.21). Prenatal exposure had marginally statistically significant association (OR=1.11; 95% CI, 1.00 to 1.23) with asthma in children. In subgroup analysis for childhood exposure, the association persists for sugar-sweetened soft drinks but not for carbonated drinks.
Conclusion Our findings show a positive association between soft drinks consumption and asthma prevalence, mostly from cross-sectional studies. Therefore, more longitudinal research is required to establish causality.
- carbonated beverages
- asthma
- epidemiology
- nutrition & dietetics
- public health
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The current systematic review provides a summary of the best available evidence on the association between soft drinks consumption and asthma, combining results of previous studies in a meta-analysis and including more than 47 000 cases.
The review was based on comprehensive literature search with no language restrictions. The overall quality of the studies included in our review was satisfactory.
The majority of the included studies were cross-sectional studies, compared with three prospective cohort studies.
There was variation between the included studies in defining the study population, exposure categories, adjusted confounders and the outcome of interest.
Introduction
Asthma is a chronic disease characterised by airway hyper-reactivity and reversible obstruction. The prevalence is rising in many countries making it one of the most important global health issues.1 Asthma has a high burden of disability, particularly among children and older adults. It is ranked as the 14th most important disease worldwide in terms of years lived with disability2 and has been identified as the most common cause of hospitalisation in children.3
The causes of asthma are complex but generally considered to involve interaction between host factors, mainly genetics, and environmental factors.2 For example, exposure to second hand smoke was confirmed as a risk factor for asthma2 but also other factors like obesity, sedentary behaviour, preterm birth, low birth weight and viral infections in infancy have been associated with increased odds of developing asthma.4 Also, several dietary risk factors (eg, fast food, salt and trans fatty acids5) and protective factors (eg, fruit and vegetables, vitamins A, D and E, selenium, magnesium and Mediterranean diet4) showed consistent evidence of association with asthma.
Soft drinks or carbonated beverages are a popular component of the current dietary lifestyle both in developed and developing countries. The consumption of soft drinks has been associated with many health outcomes, including obesity,6 type 2 diabetes mellitus,7 osteopaenia8 and pancreatic cancer.9 Of particular interest in relation to asthma is the suggested positive association of the consumption of soft drinks with other respiratory diseases such as allergic rhinitis10 and chronic bronchitis.11 Previous studies already showed that soft drinks consumption is linked to asthma development,12 13 but findings are inconclusive.14 15 Although not confirmed, there were several theories proposed which suggest the importance of soft drink consumption in the development of asthma. For example, sugar (or specifically fructose) activates an inflammatory pathway16; additive substances trigger symptoms12 or soft drinks leading to overweight would serve as a mediator.14 Identification of preventable risk factors is of paramount importance to guide public health prevention measures to reduce the burden of asthma.2 4 Therefore, the aim of the current study is to perform a meta-analysis on the association between soft drinks consumption and prevalence of asthma in both children and adults to clarify the potential association. In our knowledge, no such quantitative summary assessment has been performed previously.
Method
Literature search
A systematic search of the literature was conducted up to December 2018 using four electronic databases: Medline (PubMed interface), Scopus, ISI Web of Science and the Cochrane Library. The literature search aimed to identify observational studies on the association between soft drinks consumption and development of asthma. There was no language or publication date restriction. In case we identified non-English articles, professional translators would be employed to translate the full text of the articles. The following search query was used: (sweetened OR carbonated OR soft beverages OR drinks OR Soda OR Juices OR Fruit and Vegetable Juices) AND (Asthma OR wheezing OR bronchoconstriction OR bronchospasm OR bronchial OR respiratory OR airway OR hypersensitivity OR hyperreactivity OR allergy OR spasm). The full search strategy can be found in the online supplementary table S1. Additional citations were obtained manually by searching the reference lists of articles selected for review to complement the database literature search. The search was conducted by INE, AK, AGA, AH, NMA, MA and supervised by AHA-Z. Articles were downloaded into Endnote software (V.15) and duplicates were removed.
Supplemental material
Study selection
The first selection was done based on title and abstract of articles identified through a literature search. Second selection was based on full text of articles identified in the previous step, using the following eligibility criteria: reported on the association between soft drinks consumption (including maternal consumption during pregnancy) and asthma or wheeze; presented original data from observational studies and reported effect measure of relative risk or OR with 95% CI or data to enable their calculation. The outcome of interest was asthma and wheeze. The exposure of interest was soft drinks consumption including both sugar-sweetened and artificially sweetened. The selection was carried out by one researcher (INE, AK) and double-checked independently by two others (AGA, AH, NMA, MA, AHA-Z). Disagreements between researchers were resolved by discussion until consensus was reached.
If a study provided more than one estimate, we selected estimates in the following order: documented doctor-diagnosed asthma; self/parental-reported asthma based on a combination of symptoms, medication and doctor diagnosis; self/parental-reported doctor-diagnosed asthma; self/parental-reported asthma based on symptoms or medication. Risk estimates from cross-sectional, case–control and cohort studies were accepted.
Data extraction
The following data were extracted: author, publication year, country where the study was carried out, study design, study period, participants’ age and sex, sample size, number of cases, methods of data collection, exposure, outcome, risk estimates with 95% CI, p value and covariates that had been adjusted for. If a study provided more than one estimate, for example, various adjustment or consumption levels, we selected (1) the most adjusted estimate and (2) the estimate of the highest consumption level category. Data extraction was conducted by one author and reviewed independently by two other authors, with disagreements resolved by discussion until consensus was reached.
Quality assessment
The quality of cohort studies was assessed using the Newcastle–Ottawa scale,17 while the quality of cross-sectional studies was assessed by Newcastle–Ottawa scale adapted for cross-sectional studies.18 Points, or ‘stars’, were awarded for high-quality elements. The stars were then added up and used to compare study quality in a quantitative way. The highest methodological quality receives a maximum score of 9 stars for cohort studies and 10 stars for cross-sectional studies.
Data synthesis and statistical analysis
Meta-analysis was conducted using random-effects model to calculate summary OR estimates and 95% CI for asthma as well as wheeze comparing the highest versus lowest level of consumption of soft drinks. We decided that it is inappropriate to combine risk ratios (RR), hazard ratios (HR) and OR into one estimate. This decision was because asthma is a common disease which means that OR, RR and HR cannot be assumed to be similar and thus are not recommended to be combined in meta-analyses.19 We conducted a meta-analysis for adults and children separately due to the potential variation in asthma between children and adults,20 as risk factors may affect lung functions differently in children and adults as have been shown in studies of other risk factors.21 Heterogeneity among studies was evaluated using I2 statistic.22 Publication bias was evaluated using Egger’s test. All statistical analyses were carried out with Stata V.13. A two-tailed p value of <0.05 was considered to be statistically significant. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses and meta-analysis of observational studies in epidemiology (MOOSE) reporting guidelines were followed in writing this publication.23
Patient and public involvement
Patients were not directly involved in the development of the research question and outcome measures, design and conduct of the study or interpretation of the results.
Results
A total of 725 records were identified through our initial databases search (PubMed: 152, Scopus: 400, Web of Science: 172, Cochrane: 1). Four articles were identified from the reference lists of relevant studies. After removing duplicates, a total of 487 records were screened based on title and abstract. Of these, 455 records were excluded (not relevant, eg, narrative reviews, expert opinion, physiological studies or other topics) leaving 32 articles to be screened based on the full text. Of these, 13 studies were excluded because soft drinks were investigated as a part of dietary patterns but not analysed separately or no risk estimate was reported. Finally, 19 papers were included in the present systematic review (3 cohort and 16 cross-sectional studies), of which 18 studies were suitable to be combined in meta-analyses (1 study reported HR and thus was inappropriate to combine with other studies reporting OR). The flow chart of the selection process is shown in figure 1.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram describing selection process.
Study characteristics
Table 1 shows the main characteristics of all 19 studies included in our review. Twelve studies reported on childhood exposure to soft drinks,5 11 12 14 24–31 six studies on adulthood exposure to soft drinks13 15 16 32–34 and two studies on maternal consumption of soft drinks and asthma in the offspring.31 35 Three studies were cohort studies16 31 35 and 16 were cross-sectional studies.5 12–15 24 26–30 32–34 36 37 Six studies were conducted in Europe,5 14 26 29 32 35 six in the USA,12 16 24 31 33 36 four in Asia,15 25 27 34 one in Brazil,30 one in New Zealand28 and one in Australia.13 The studies were published between 2002 and 2019. One study was in Italian29 and has been translated into English by a professional translator. None of the included studies reported on documented doctor-diagnosed asthma. The selected studies included 468 836 participants. Of these, 236 932 were children, 170 385 were adults and 61 519 were pregnant women, and together involved more than 50 000 asthma cases. The quality scores ranged from 6 to 8 stars (online supplementary tables S2 and S3).
Study characteristics of published cross-sectional and cohort studies on soft drinks and asthma
Adulthood exposure and asthma
Adulthood exposure was studied in six studies: one cohort study16 reporting HRs, and five cross-sectional studies13 15 32–34 reporting ORs. The meta-analysis of soft drinks consumption and asthma in adults was based on the five cross-sectional studies only, therefore providing only estimates of the prevalence of asthma. This prevalence was significantly higher among adults with the highest levels of soft drink consumption compared with the lowest levels of consumption (OR=1.37; 95% CI, 1.23 to 1.52; figure 2). There was a moderate level of heterogeneity among studies (p=0.029, I2=60.0%) and no evidence of publication bias (Egger p=0.649). The cohort study reported an increased hazard among adults who consumed soft drinks 5–7 times/week (HR=1.48; 95% CI, 1.09 to 2.01) but not in those consuming more than once per day (HR=0.94; 95% CI, 0.68 to 1.31), compared with no soft drink consumption. They also separately reported on the association between asthma and artificially sweetened soft drinks consumption but found no association at either level of consumption (table 1).
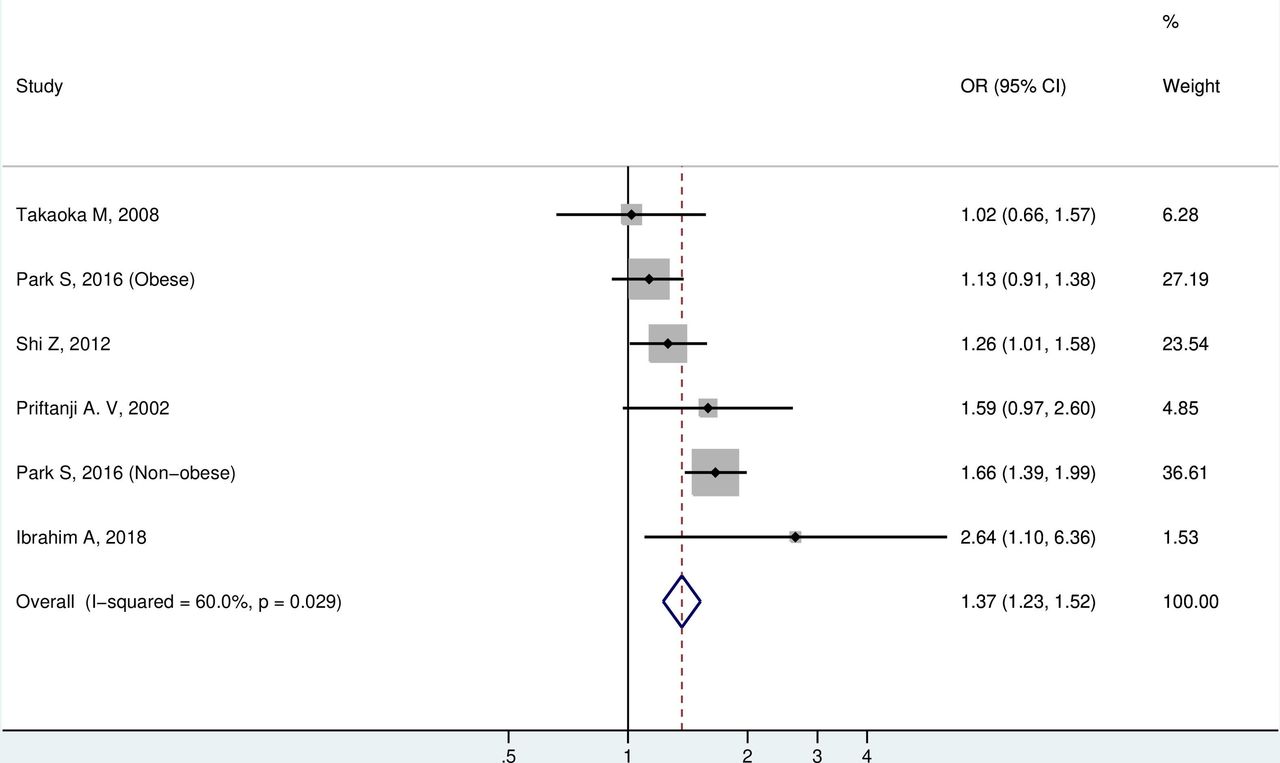
Meta-analysis of asthma among adults comparing highest versus lowest levels of soft drinks consumption.
Childhood exposure and asthma
The meta-analysis of soft drinks consumption and asthma in children was based on 1 cohort31 and 11 cross-sectional studies.5 12 14 24–30 36 The overall OR of highest versus lowest levels of soft drinks consumption was 1.14 (95% CI, 1.06 to 1.21; figure 3), suggesting that soft drinks consumption is associated with increased odds of asthma. There was a low level of heterogeneity among studies (p=0.111, I2=39.4%) and no evidence of publication bias (Egger p=0.279).

Meta-analysis of asthma among children comparing highest versus lowest levels of soft drinks consumption.
We were also able to do meta-analyses for studies reporting separate estimates for consumption of sugar-sweetened soft drinks as well as carbonated drinks (figure 4 and table 2). We found increased odds of asthma with high versus low intakes of sugar-sweetened soft drinks (OR=1.26; 95% CI, 1.07 to 1.48) but not with high versus low intakes of carbonated drinks (OR=1.05; 95% CI, 0.94 to 1.16).

Meta-analysis of asthma among children with soft drinks consumption: sugar-sweetened and carbonated beverages.
Summary of effect estimates for various exposures
Childhood exposure and wheeze
Seven studies investigated the association between soft drinks consumption and wheeze in children.5 14 26–30 The overall OR of highest versus lowest soft drinks consumption and wheeze among children was 1.09 (95% CI, 1.05 to 1.13; figure 5 and table 2), suggesting that soft drinks consumption is associated with increased odds of wheeze in children. There was low heterogeneity among studies (p=0.161, I2=33.5%) and no evidence of publication bias (Egger p=0.932).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Meta-analysis of wheeze among children for highest versus lowest levels of soft drinks consumption.
Prenatal exposure and childhood asthma
Two cohort studies31 35 reported on the association between maternal soft drinks consumption during pregnancy and asthma prevalence in children. Maslova et al 35 did not find a statistically significant association with asthma for either artificially sweetened soft drinks (carbonated: OR=1.18; 95% CI, 0.87 to 1.59; non-carbonated: OR=1.0; 95% CI, 0.82 to 1.22) or sugar-sweetened soft drinks (carbonated: OR=1.20, 95% CI: 0.93 to 1.56; non-carbonated: OR=1.07; 95% CI, 0.90 to 1.28). Wright et al 31 reported an increased risk of asthma in children with highest maternal consumption of sugar-sweetened soft drinks during pregnancy (OR=1.68; 95% CI, 1.07 to 2.65) compared with the lowest levels of exposure. We combined all estimates from the two studies in a meta-analysis and found marginally statistically significant association (OR=1.11; 95% CI, 1.00 to 1.23; table 2). We also combined the estimates for sugar-sweetened soft drinks from the two studies in a meta-analysis, and found similar results (OR=1.15; 95% CI, 1.00 to 1.32).
Table 2 summarises effect estimates for various exposures based on the results of our meta-analyses when possible. When meta-analysis was not possible due to lack of data, we included results from single studies to provide the best evidence for that association.
Discussion
The results of the current meta-analyses show a positive association between consumption of soft drinks and asthma in adults, consumption of soft drinks and asthma and wheeze in children, as well as prenatal maternal consumption of soft drinks and asthma in their children. Subgroup analyses for childhood exposure also showed increased odds for sugar-sweetened soft drinks but not for carbonated drinks. Further subgroup analysis could not be performed because not enough studies were available.
Unfortunately, based on our results, it is not possible to determine the mechanism of action by which soft drinks play a role in the development of asthma. However, several theories have been proposed. A common hypothesis to explain the association between soft drinks consumption and asthma revolves around its sugar content, which was hypothesised to activate an inflammatory pathway that may lead to the development of asthma. A diet that is high in sugar-sweetened drinks was found to be related to increased inflammatory markers.38 39 In a randomised controlled trial, sugar-sweetened beverages resulted in increased level of high-sensitivity C-reactive protein.40 Furthermore, the link between sugar and asthma was supported by an ecological study showing a parallel trend between severe asthma and per-capita sugar consumption.41
However, two studies included in the current review investigated the effect of sugar-sweetened versus artificially sweetened soft drinks and their results do not support this sugar hypothesis.14 35 In the study by Berentzen et al,14 a significant association was found for fruit juice but not for sweetened milk drinks, energy drinks or sports drinks although they contain the same amount of sugar. Moreover, the registry-based analysis of the study by Maslova et al 35 even showed the opposite, finding an association with asthma for artificially sweetened drinks but not for sugar-sweetened drinks.
These contradictory findings should however not fully disregard the ‘sugar hypothesis’, as another explanation may be found in the sugar composition rather than content, accusing fructose to be the culprit behind inflammation induction. Fructose is metabolised differently in the liver and leads to increased lipogenesis, dyslipidaemia and insulin resistance.42 Fructose also increased uric acid level which in turn leads to insulin resistance and low-grade inflammation.43 High-fructose corn syrup (HFCS) is a commonly used sugar-based sweetener of soft drinks. Although HFCS supposedly contains 55% fructose, which is almost similar to the fructose content of sucrose (50%),44 some studies reported a fructose content of up to 65% in popular sugar-sweetened beverages.45 DeChristopher et al 16 36 investigated the role of fructose and analysed data separately for drinks containing high and low levels of fructose, specifically excess free fructose (EFF). They found higher odds of asthma associated with drinks containing high levels of EFF, supporting this theory.
Another hypothesis to explain the association between soft drinks and asthma is the presence of additives in soft drinks, for example, sodium benzoate and sulfites. Sodium benzoate and sulfites have been demonstrated to evoke symptoms in asthma and allergic rhinitis patients in addition to inducing urticaria and contact dermatitis.46 However, it was not confirmed that these substances play a role in the development of asthma rather than triggering asthma symptoms.12
Finally, in addition to the above-mentioned hypotheses, Berentzen et al 14 proposed that overweight may explain the association between soft drinks and asthma. Soft drinks consumption can lead to overweight which has been associated with decreased lung functions and asthma probably through mechanical and immunological effects including insulin resistance.21 47 48 Weight loss has been found to improve asthma control.47 However, Berentzen et al’s14 data analysis did not support this hypothesis. Moreover, consumption of one type of food or drink is frequently linked to a dietary pattern. Thus, it is possible that soft drink consumption is associated with other unhealthy dietary habits and consequently displacing healthy diet, for example, fruit and vegetables.
The observed association could be confounded by various factors. First, primary studies included in the current review have adjusted for various potential confounders, but the exact factors varied between studies and residual confounding cannot be excluded. Second, measurement of soft drink consumption as well as other confounding factors was based on self-report by participants which can lead to misclassification and less precise risk estimates. Third, the definition of soft drinks is broad and different additives and different amount of constituents may affect precision of effect size estimation.
The current systematic review summarises the results of available research, including more than 47 000 cases, to elucidate the question of the association between soft drink consumption and asthma. The review was based on comprehensive literature search with no dates or language restrictions. The overall quality of the studies included in our review was satisfactory. The majority of the included studies were cross-sectional studies, compared with three prospective cohort studies. Although it is unlikely that asthma leads to increased intake of soft drinks, the issue of reverse causality cannot be excluded in the cross-sectional design. However, the fact that the three cohort studies showed a positive association in line with the current meta-analysis findings is reassuring. In addition, the longitudinal studies presented ORs, which may overestimate the true association when the prevalence is greater than 10%, as was the case in the cohort studies included. Another limitation of this systematic review is the variation between the included studies in defining the study population, exposure categories, adjusted confounders and the outcome of interest. Moreover, subgroup analyses, such as carbonated versus non-carbonated or sugar-sweetened versus artificially sweetened, were not possible for each outcome and exposure window. Such analyses would allow for elucidation on the exact mechanisms by which soft drinks increase the risk of asthma and/or wheeze.
Conclusion
The current systematic review provides a summary of the best available evidence on the topic. The identified scarcity in longitudinal research highlights the need for further studies to shed light on the relationship between soft drinks and asthma and mechanisms of action. Taking into consideration the other health effect of soft drinks consumption like obesity49 and dental caries,50 it would be wise to continue to initiate and support measures to reduce the consumption of soft drinks.
References
Footnotes
Twitter @alzalabani
Contributors Study conceptualised and designed by all authors. Literature search, study selection and data extraction by INE, AK, AGA, AH, NMA, MA, AHA-Z. Data analysis by AZ. Data interpretation and writing by AHA-Z, AW, KFJS. All the authors critically reviewed the manuscript for scientific content and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by Research Ethics Committee of College of Medicine, Taibah University.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.