Article Text

Abstract
Objective This study aimed to compare the effects of intravenous, topical and combined routes of tranexamic acid (TXA) administration on blood loss and transfusion requirements in patients undergoing total knee arthroplasty (TKA) and total hip arthroplasty (THA).
Design This was a meta-analysis of randomised controlled trials (RCT) wherein the weighted mean difference (WMD) and relative risk (RR) were used for data synthesis applied in the random effects model. Stratified analyses based on the surgery type, region, intravenous and topical TXA dose and transfusion protocol were also conducted. The main outcomes included intraoperative and total blood loss volume, transfusion rate, low postoperative haemoglobin (Hb) level and postoperative Hb decline. However, the secondary outcomes included length of hospital stay (LOS) and/or occurrence of venous thromboembolism (VTE).
Setting We searched the PubMed, Embase and Cochrane CENTRAL databases for RCTs that compared different routes of TXA administration.
Participants Patients undergoing TKA or THA.
Interventions Intravenous, topical or combined intravenous and topical TXA.
Results Twenty-six RCTs were selected, and the intravenous route did not differ substantially from the topical route with respect to the total blood loss volume (WMD=30.92, p=0.31), drain blood loss (WMD=−34.53, p=0.50), postoperative Hb levels (WMD=−0.01, p=0.96), Hb decline (WMD=−0.39, p=0.08), LOS (WMD=0.15, p=0.38), transfusion rate (RR=1.08, p=0.75) and VTE occurrence (RR=1.89, p=0.15). Compared with the combined-delivery group, the single-route group had significantly increased total blood loss volume (WMD=198.07, p<0.05), greater Hb decline (WMD=0.56, p<0.05) and higher transfusion rates (RR=2.51, p<0.05). However, no significant difference was noted in the drain blood loss, postoperative Hb levels and VTE events between the two groups. The intravenous and topical routes had comparable efficacy and safety profiles.
Conclusions The combination of intravenous and topical TXA was relatively more effective in controlling bleeding without increased risk of VTE.
- tranexamic acid
- total knee arthroplasty
- total hip arthroplasty
- IV
- topical
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
All included studies used the randomised controlled design to avoid uncontrolled biases.
The combination of topical and systemic tranexamic acid administration was also studied.
The heterogeneity was assessed using sensitivity, subgroup and meta-regression analyses.
The number of participants in most of the included studies was small, and the prevalence of venous thromboembolism following joint replacement was low.
Only a small number of trials evaluated the combined-delivery group, which precluded sufficient exploration of heterogeneity through subgroup or meta-regression analysis.
Introduction
Tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine, which inhibits fibrinolysis by blocking the lysine-binding site of plasminogen.1 Currently, it is one of the most commonly used haemostatic drugs and is capable of reducing blood loss volume in surgical patients by approximately 34%.2 3 Moreover, this drug has effectively reduced the blood loss volume and transfusion rate in various surgical settings, including in traumatic haemorrhage,4 caesarean section,5 endoscopic sinus6 and cardiac7 surgeries and arthroplasty.8
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are reliable surgical procedures for patients suffering from moderate to severe degenerative joint diseases. Total joint arthroplasty (TJA) is effective in relieving pain, restoring physical function and improving health-related quality of life.9 By 2030, the demand for primary THA is estimated to increase to 572 000 and that for primary TKA is estimated to reach 3.48 million procedures.10 Despite substantial advances in surgical and anaesthetic techniques, TKA and THA are still associated with a large amount of perioperative blood loss.11 The intraoperative blood loss volume in either procedure is generally between 500 and 1500 mL. Additionally, patients may experience a postoperative drop in haemoglobin (Hb) level between 1 and 3 g/dL.12 Up to 50% of the patients undergoing TJA inevitably experience postoperative anaemia.11
The role of TXA during arthroplasty has been an issue of concern for the past two decades. Several previous trials or meta-analyses have mainly focused on comparing TXA and non-TXA, proving that oral, intravenous and topical TXA were associated with significantly reduced perioperative blood loss volume and blood transfusion requirements.13–19 Furthermore, two important meta-analyses showed comparable haemostatic effects between oral and intravenous TXA.20 21 Moreover, another two studies showed that patients who received combined intravenous and topical TXA experienced more benefits than those with single-route TXA administration.22 23 However, few studies have directly compared the different TXA administration routes, and they were limited due to combination of various study design types and relatively small number of included studies.24 In addition, the potential for thromboembolic events (deep vein thromboembolism (DVT) or pulmonary embolism (PE)) after TXA use represents TXA’s Achilles’ heel.1 Topical TXA application during arthroplasty may be a safer route than the systemic method, which may reduce postoperative haemorrhage without causing hypercoagulation. Notably, the topical route has been shown to be a cost-effective and convenient route for TXA administration during dental, cardiac and spinal surgeries.25 Several relevant trials have been published recently. Thus, we compiled this systematic review and meta-analysis to compare the efficacy and safety of topical and intravenous TXA use in patients undergoing TKA and TXA. In addition, the combination of topical and systemic administration of TXA was evaluated.
Methods
Patient and public involvement
No patients were involved in the study design or conduct of the study.
Search strategy
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement issued in 2009.26 Ethical approval was not necessary for this study, as only deidentified pooled data from individual studies were analysed. We searched the PubMed, Embase and Cochrane CENTRAL databases for relevant studies from the time of these databases’ inception to April 2018. The following groups of keywords and medical terms were used for the literature search: ‘tranexamic acid’ and ‘total knee arthroplasty’, ‘total knee replacement’, ‘total hip arthroplasty’, ‘total hip replacement’ or ‘arthroplasty’ and random*, prospective* or trial*. The details of the search strategy in PubMed are shown in online supplementary file 1. This study was restricted to the English language. Furthermore, an additional search was conducted by screening the references of eligible studies.
Supplemental material
Selection of studies
Studies were pooled for meta-analysis if they met the following criteria: (1) study design: randomised controlled trials (RCT); (2) patients: those with TKA or THA; (3) intervention and control: comparing intravenous TXA with topical TXA or considering their combination with single TXA regimen; and (4) outcomes: the main outcomes included intraoperative and total blood loss, transfusion rate, low postoperative Hb level and postoperative Hb decline. However, the secondary outcomes included length of hospital stay (LOS) and/or the occurrence of venous thromboembolism (VTE) which may present as PE or DVT.
Data collection and quality assessment
Two reviewers independently evaluated the eligibility of the collected studies and extracted their data. Any discrepancy was resolved via a consensus meeting. The full text of the eligible studies was reviewed, and information was entered into an electronic database, including author, year of publication, region, sample size, patient characteristics (eg, age, gender, surgery type), intravenous and topical regimen, transfusion threshold, tourniquet use, thromboembolism prophylaxis and outcomes. The Jadad scale was used for the quality assessment of RCTs,27 which assigned a score of 0–5 according to the items of randomisation, blinding and withdrawals reported during the study period.
Statistical analysis
All meta-analyses were conducted using Stata V.12.0 (StataCorp, College Station, TX, USA). The relative risk (RR) and 95% CI were used as estimates to analyse dichotomous outcomes. The weighted mean differences (WMD) were used for continuous data and 95% CI was used for estimates. We converted the median to mean following Hozo’s method.28 The random effects model was used for data processing. In addition, statistical heterogeneity among the studies was assessed by using the Cochran’s Q statistic and was quantified according to the I2 statistics. We considered the low, moderate and high heterogeneity as I2 values of ≤25%, 25%–75% and ≥75%, respectively.29 Sensitivity analysis was performed by removing one trial at a time to determine its influence on the overall result. Subgroup analysis was further performed according to the following variables: surgery (THA or TKA), region (Asia, North America or Europe), intravenous dose (≥2 g or <2 g), topical dose (≥2 g or <2 g) and transfusion protocol (strict or loose). The TXA dose of 30 mg/kg was categorised into the subgroup ≥2 g. A strict transfusion protocol was implemented for the threshold of Hb <0.8 g/L. When more than 10 studies were available for certain outcomes, meta-regression analysis was performed to examine the impact of the sample size. A funnel plot was constructed to visually evaluate the publication bias. The Egger’s and Begg’s tests were used for quantitative assessment of publication bias.30 31 A p value <0.05 was considered statistically significant.
Results
Figure 1 shows the flow diagram of the study selection process. After step-by-step exclusion, 26 RCTs were finally included. One trial had three comparison arms of intravenous and topical TXA and their combination.32 Tables 1 and 2 show the main features of the trials. We identified 20 RCTs comparing intravenous TXA with topical TXA, with a total of 1912 participants (table 1).32–51 About 15 trials used TXA in TKA procedures and five trials used TXA in THA procedures. Only one TKA study did not use a tourniquet during surgery.49 Ten trials were conducted in Asia, seven in Europe and three in the USA. The patients’ mean age ranged from 44 to 73 years. Seventeen trials presented a thromboprophylaxis protocol, with low-molecular-weight heparin used most frequently. Seven RCTs compared single-route administration (intravenous or intra-articular) with a combination of intravenous and topical routes32 52–57 (table 2), with a total of 877 patients. Most of the studies (5/7) were conducted in the Chinese population. Four studies were conducted on patients who underwent TKA, whereas three studies were performed among those with THA. For the arm of single route, five trials used the intravenous route, one used the topical route and one used both. All studies implemented a thromboprophylaxis protocol. With regard to the TKA studies, only Nielsen et al did not use an intraoperative tourniquet.55 The quality assessment of the selected trials using the Jadad scale is shown in online supplementary table 1, and the total score of the included trials is presented in tables 1 and 2. The total score ranged from 1 to 5, with a mean score of 3.7. The items related to blinding were least satisfied.
Supplemental material
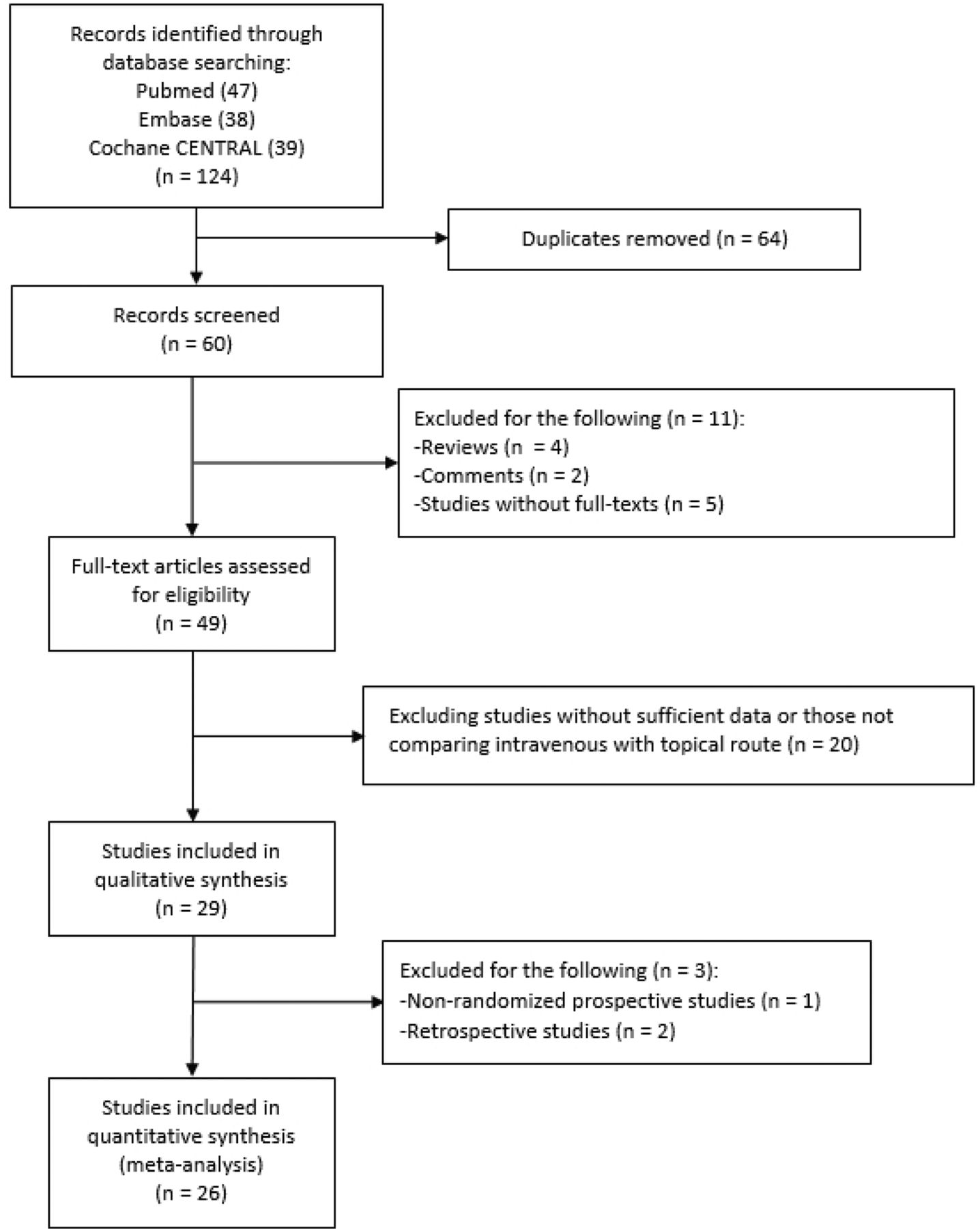
The flow diagram showing the study selection process.
Characteristics of prospective studies comparing topical with intravenous tranexamic acid in patients receiving total knee or hip arthroplasty
Characteristics of prospective studies comparing combination of topical and intravenous tranexamic acid with single tranexamic acid in patients receiving total knee or hip arthroplasty
Intravenous versus topical route
Blood loss
About 14 studies reported on blood loss. No significant difference was observed in the total blood loss volume (WMD=30.92, 95% CI −28.40 to 90.25, p=0.31; I2=87.0%, p<0.05) between intravenous TXA administration and topical administration. This effect was not substantially different for either TKA (WMD=52.69, 95% CI −18.58 to 123.97, p=0.15) or THA (WMD=−31.03, 95% CI −156.16 to 94.10, p=0.63) (figure 2).
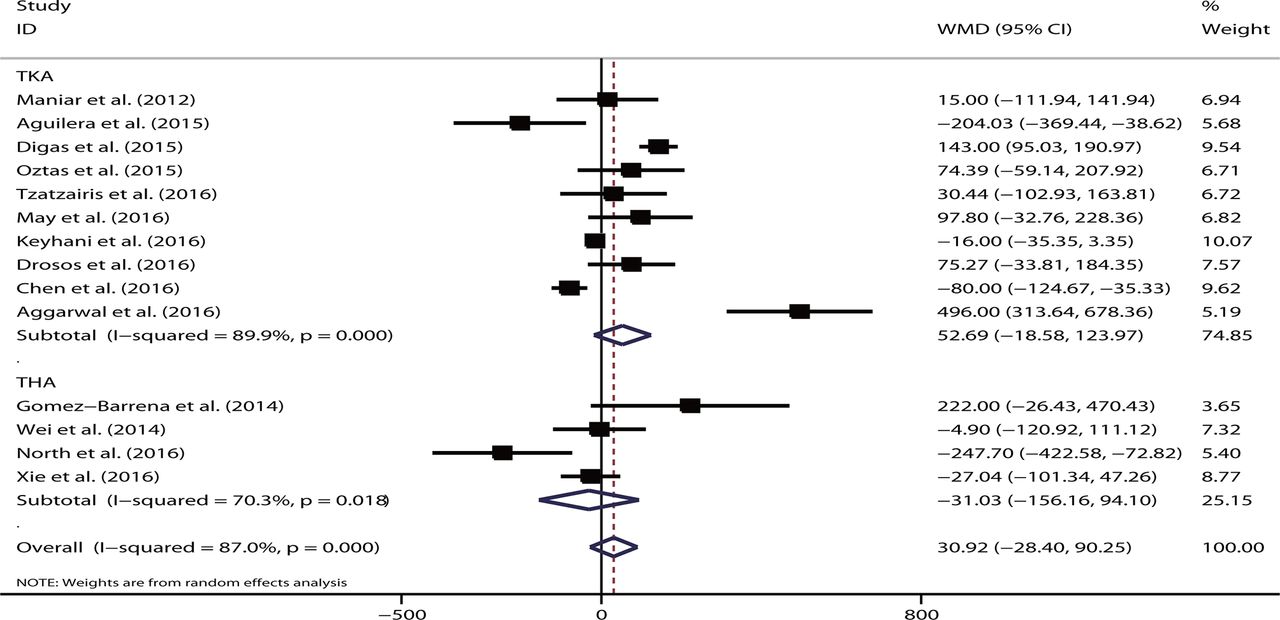
Forest plot comparing the efficacy of intravenous versus topical tranexamic acid (TXA) on total blood loss. THA, total hip arthroplasty; TKA, total knee arthroplasty; WMD, weighted mean difference.
Subgroup analysis showed that region (Asia, Europe or USA), intravenous dose (≥2 g or <2 g) or topical dose (≥2 g or <2 g) did not markedly affected the overall effect of the analysis (all p>0.05). None of the studies that significantly changed the overall effect in the sensitivity analysis were identified. Meta-regression demonstrated that the sample size did not account for the heterogeneity of the study (p=0.20). The funnel plot appeared to be symmetrical. No publication bias was revealed based on the Egger’s test (p=0.37) or Begg’s test (p=0.27).
Eight studies presented the outcome of drain blood loss. No significant difference was demonstrated in the intravenous route (WMD=−34.53, 95% CI −135.39 to 66.34, p=0.50; I2=97.2%, p<0.05) and overall effect on TKA (WMD=−38.28, 95% CI −146.29 to 69.73, p=0.49) or THA (WMD=−7.50, 95% CI −95.00 to 80.00, p=0.87).
Postoperative Hb
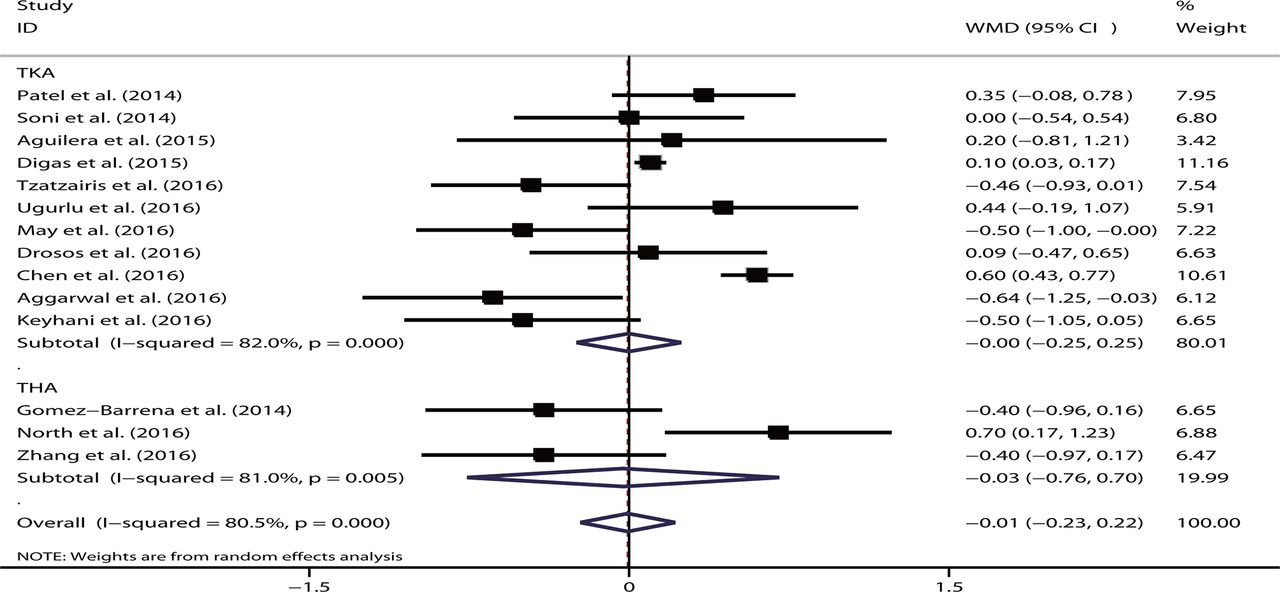
By pooling data from 14 relevant studies, no significant difference was found between the intravenous and topical routes of TXA administration with respect to the postoperative Hb level (WMD=−0.01, 95% CI −0.23 to 0.22, p=0.96; I2=80.5%, p<0.05). The result remained insignificant for TKA (WMD=−0.00, 95% CI −0.25 to 0.25, p=0.99) and THA (WMD=−0.03, 95% CI −0.76 to 0.70, p=0.94) (figure 3). When stratified according to the region and intravenous and topical dose, no significant data were noted in any subgroup (all p>0.05). Sensitivity analysis was performed by excluding studies one at a time; however, no significant difference was noted. The significant role of the sample size in explaining the heterogeneity (p=0.27) was not revealed in the meta-regression analysis. The funnel plot was symmetrical, and no bias was shown based on the Egger’s test (p=0.38) or Begg’s test (p=0.91).

Forest plot comparing the efficacy of intravenous versus topical tranexamic acid (TXA) on postoperative haemoglobin levels. THA, total hip arthroplasty; TKA, total knee arthroplasty; WMD, weighted mean difference.
Seven studies reported a decline in Hb levels after arthroplasty. The pooled data revealed no significant difference in the intravenous route compared with the topical route (WMD=−0.39, 95% CI −0.82 to 0.04, p=0.08; I2=89.4%, p<0.05). In the subgroup analysis, two studies on THA showed that the intravenous route had a significantly lesser amount of Hb decline than the topical route (WMD=−0.49, 95% CI −0.70 to 0.28, p<0.05). However, no statistical significance was noted on the TKA procedure (WMD=−0.35, 95% CI −1.02 to 0.32, p=0.31). When excluding the studies by Soni et al 38 or Tzatzairis et al,49 the overall effect was significant (p<0.05).
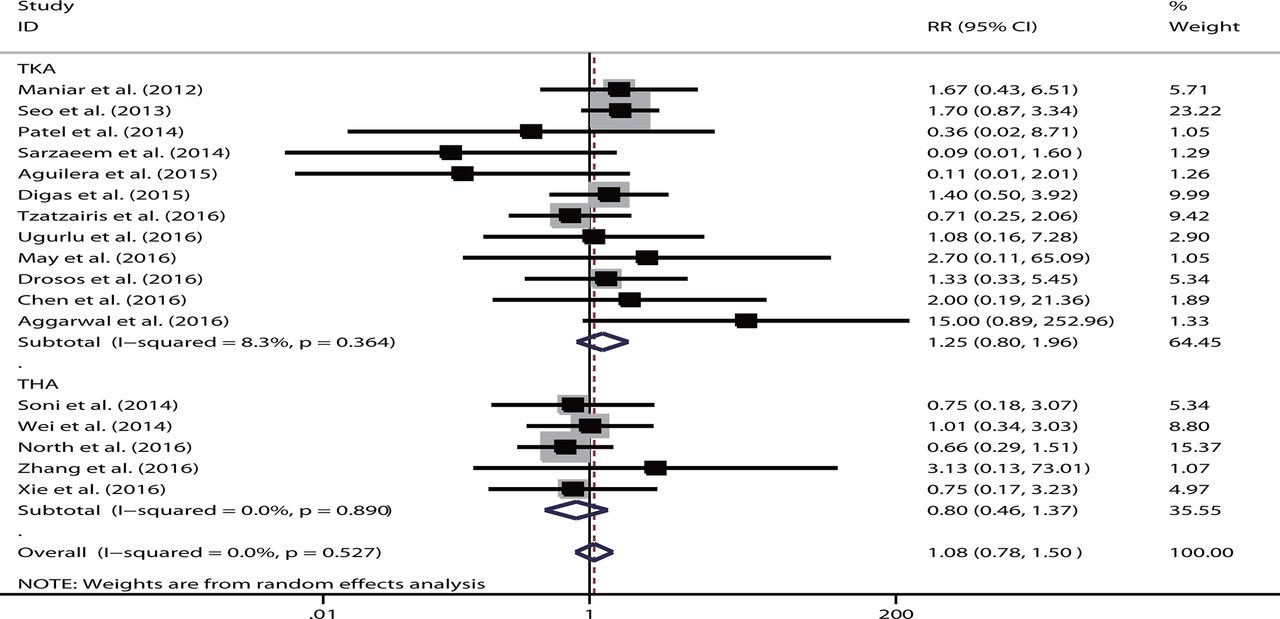
Transfusion rate
Information on the transfusion rate was reported in 17 studies. The pooled results demonstrated that no significant difference was observed in the transfusion rate of the intravenous route (RR=1.08, 95% CI 0.78 to 1.50, p=0.75). No heterogeneity was detected (I2=0%, p=0.63). In a separate analysis completed according to different arthroplasty procedures, the result was not substantially altered (TKA: RR=1.25, 95% CI 0.80 to 1.96, p=0.32; THA: RR=0.80, 95% CI 0.46 to 1.37, p=0.41) (figure 4). When stratified according to the transfusion threshold (ie, loose or strict), no significant result was shown in any subgroup (loose: RR=1.13, p=0.65; strict: RR=1.00, p=1.00). Similarly, no substantially significant results were noted in the subgroups based on the region and intravenous or topical dose (all p>0.05). The sensitivity analysis did not show that the inclusion of any individual study significantly changed the overall effect. The sample size was not the source of heterogeneity in meta-regression analysis (p=0.36). The funnel plot was symmetrical. No publication bias was shown based on the Egger’s test (p=0.69) or Begg’s test (p=1.00).
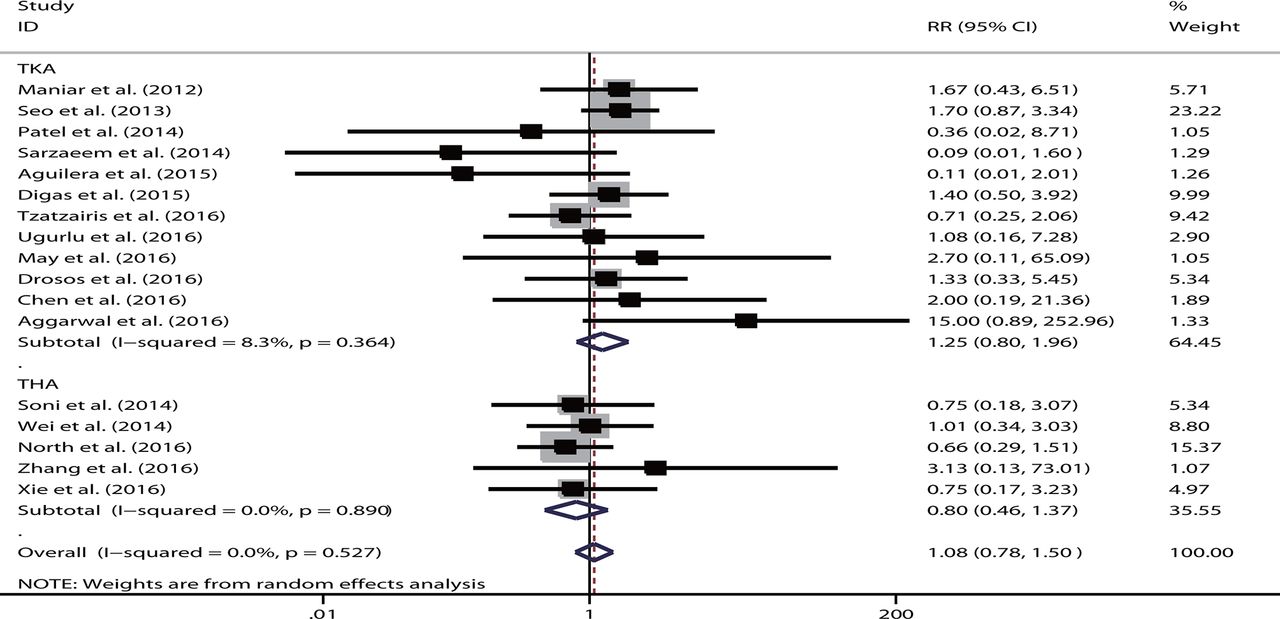
Forest plot comparing the efficacy of intravenous versus topical tranexamic acid (TXA) on postoperative transfusion rate. RR, relative risk; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Length of hospital stay
The LOS was reported in seven studies. One study was excluded due to 0 SD.49 The pooled results showed that patients with the intravenous and topical routes had similar LOS (WMD=0.15, 95% CI −0.18 to 0.47, p=0.38; I2=90.1%, p<0.05). No marked change was revealed for TKA (WMD=0.27, 95% CI −0.01 to 0.54, p=0.06) or THA (WMD=−0.05, 95% CI −0.42 to 0.32, p=0.80).
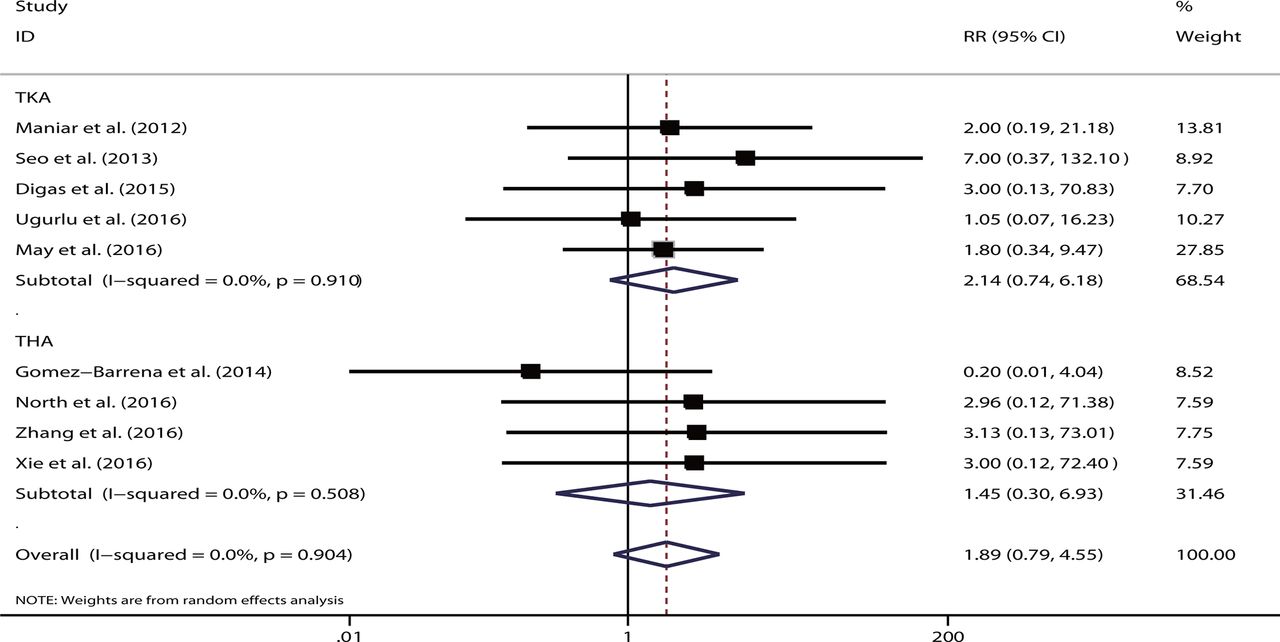
VTE events
A total of 20 studies reported VTE events. However, 11 trials showed no VTE occurrence in any study group,36–40 42–46 49 and thus were excluded from meta-analysis. For the remaining nine trials, except for one study,34 low-molecular-weight heparin was unanimously used for thromboprophylaxis. The aggregated data showed no significant difference for the intravenous versus topical route (RR=1.89, 95% CI 0.79 to 4.55, p=0.15). No heterogeneity was detected (I2=0%, p=0.90). The pooled results remained non-significant for TKA (RR=2.14, 95% CI 0.74 to 6.18, p=0.16) and THA (RR=1.45, 95% CI 0.30 to 6.93, p=0.64) (figure 5). No single study played a substantial role in sensitivity analysis. Sample size was not the source of heterogeneity in meta-regression analysis (p=0.74).

Forest plot comparing the safety of intravenous versus topical tranexamic acid (TXA) on postoperative venous thromboembolism. RR, relative risk; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Combined routes versus single route
Blood loss
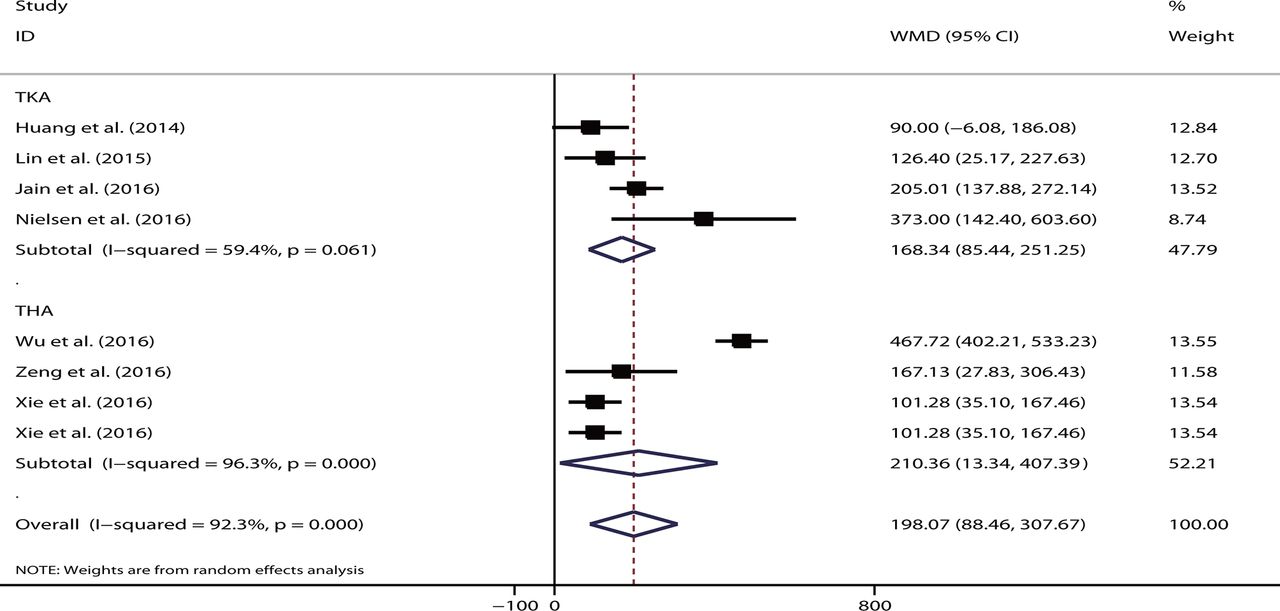
The pooled data showed that the single route had significant increased total blood loss volume (WMD=198.07, 95% CI 88.46 to 307.67, p<0.05; I2=92.3%) compared with the combined regimen. When stratified according to different procedures, the results remained significant for TKA (WMD=168.34, 95% CI 85.44 to 251.25, p<0.05; I2=59.4%) and THA (WMD=210.36, 95% CI 13.34 to 407.39, p<0.05; I2=96.3%) (figure 6). Either the intravenous (WMD=228.93, p<0.05) or topical route (WMD=108.80, p<0.05) showed significantly increased total blood loss volume. Only two studies reported data on drain blood loss,52 56 and their pooled results showed no significant difference between single route and combined regimen (WMD=109.51, 95% CI −34.73 to 253.74, p=0.14; I2=98.1%, p<0.05).

Forest plot comparing the efficacy of single versus combined routes of tranexamic acid (TXA) on total blood loss. THA, total hip arthroplasty; TKA, total knee arthroplasty; WMD, weighted mean difference.
Hb level
Three studies presented the postoperative Hb levels, including two on TKA53 55 and one on THA.57 No significant difference was noted on the single route compared with the combined routes (WMD=−0.28, 95% CI −1.30 to 0.74, p=0.59; I2=89.6%, p<0.05). Six studies presented the outcome of Hb decline following surgery. The single route had a significantly greater magnitude of Hb decline than the combined method (WMD=0.56, 95% CI 0.30 to 0.81, p<0.05; I2=85.2%, p<0.05). The result remained significant for studies on both TKA (WMD=0.44, p<0.05) and THA (WMD=0.67, p<0.05).
Transfusion rate
Seven studies were eligible, including four studies on TKA52–55 and three studies on THA.32 56 57 Xie et al reported the use of both intravenous and topical TXA administration.32 The single route had a significantly higher transfusion rate than the combined group (RR=2.51, 95% CI 1.48 to 4.25, p<0.05). No heterogeneity was shown (I2=0%). This trend remained significant for studies on TKA (RR=0.09, p<0.05) and THA (RR=2.66, p<0.05) (figure 7). The intravenous route still showed a markedly higher transfusion rate than the combination group (RR=2.39, 95% CI 1.38 to 4.11, p<0.05). However, a significantly higher transfusion rate (RR=5.45, 95% CI 0.64 to 46.42, p=0.12) was not observed in two studies that used the topical route.

Forest plot comparing the efficacy of single versus combined routes of tranexamic acid (TXA) on blood transfusion rate. RR, relative risk; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Length of hospital stay
Four studies were relevant in terms of evaluating the LOS,32 52 55 56 and Xie et al presented on both intravenous and topical routes.32 The LOS did not differ significantly between the single route and combination regimen (WMD=0.09, 95% CI −0.10 to 0.28, p=0.36; I2=45.8%, p=0.12). No significant difference was noted in the LOS of patients who underwent TKA or THA (both p>0.05). The result remained non-significant (WMD=0.14, p=0.22) as reported in four studies conducting intravenous TXA administration.
VTE events
Six studies were eligible for consideration of VTE events.32 52–54 56 57 One study showed zero events for both arms,53 and one study presented both intravenous and topical routes.32 The pooled data suggested that the risk of VTE events did not differ substantially between the single and combination routes (RR=0.80, 95% CI 0.27 to 2.35, p=0.68; I2=0%). No statistical significance was shown between the different types of arthroplasty (TKA: RR=2.98, p=0.34; and THA: RR=0.54, p=0.32) (figure 8) or different single-delivery routes (intravenous: RR=0.98, p=0.97; topical: RR=0.20, p=0.30).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot comparing the safety of single versus combined routes of postoperative venous thromboembolism. RR, relative risk; THA, total hip arthroplasty; TKA, total knee arthroplasty.
Discussion
In recent history, TXA is one of the most commonly used haemostatic drugs for reducing blood loss during total joint replacement and ensuring fast postoperative recovery. To our knowledge, this is the most comprehensive meta-analysis of updated randomised trials investigating the efficacy and safety of intravenous versus topical TXA in patients undergoing TKA and THA. We found that the intravenous and topical routes did not differ substantially for the outcomes of total blood loss, drain blood loss, postoperative Hb level, postoperative Hb decline, transfusion rate and/or LOS. The incidence of VTE was low for both studied arms. The two routes appeared to be of comparable safety profiles for patients undergoing arthroplasty. Except for two THA studies showing that the intravenous route resulted in a lesser magnitude of Hb decline, the overall effect remained insignificant for the majority of subgroups stratified based on THA or TKA. When comparing the combination regimen with the single route, our meta-analysis demonstrated that the combination of intravenous and topical routes could significantly decrease the total blood loss volume and reduce transfusion requirements. A relatively lesser degree of Hb decline was revealed in the combined-delivery regimen. LOS was similar for both arms. Overall, VTE events occurred rarely for both routes, and no marked difference was revealed when comparing the combination and single-route groups.
Following intravenous administration, TXA is spread in the extracellular and intracellular compartments. It rapidly diffuses into the synovial fluid until its concentration reaches to that of the serum. The biological half-life is 3 hours in the joint fluid, and 90% of TXA is eliminated within 24 hours after administration.58 For the intra-articular route, TXA administration could provide a maximum local dose at the site where needed. Local administration of TXA inhibits fibrin dissolution and induces partial microvascular haemostasis.59 Particularly, the release of the tourniquet always causes increased fibrinolysis, which can be attenuated by topical TXA.60 Compared with the intravenous route, the systemic absorption for local use is at a substantially lower level.61 Additionally, topical TXA could be safer than intravenous TXA in patients with renal impairment.41 Moreover, the antifibrinolytic effect of topical TXA is limited to postoperative bleeding. Preoperatively, intravenous TXA was associated with lower blood loss volume during arthroplasty, which explains the greater benefit of combined regimen of using intravenous along with topical routes.62
Several meta-analyses have been published on TXA use during arthroplasty. Both intravenous and intra-articular administration of TXA have been demonstrated to reduce the blood loss volume without increased risk of thromboembolic complications, and the use of intravenous TXA is considerably more common.13 14 16 21–24 63–68 However, most of these meta-analyses compared TXA with a placebo. We only identified two meta-analyses that performed a head-to-head comparison between the topical and intravenous routes, including one on TKA24 and the other on THA.61 Both analyses included only a very small number of studies. In addition, a methodological flaw was observed because they included non-randomised or retrospective studies.
Our meta-analysis has several apparent strengths. First, all included studies were RCTs. The number of included trials was also larger in our meta-analysis than that in other meta-analyses, which increased the statistical power. All relevant trials published during the past 2 years were analysed. In addition, we investigated the efficacy of the combination of topical and intravenous routes. Given the similar mechanism of TXA administration in both TKA and THA, both procedures were considered for this meta-analysis.
Several clinical variables may influence the efficacy of TXA. The optimal dose of TXA remained controversial. When topically applied, there was no difference in the efficacy of 1.5 g vs 3 g of TXA wash in reducing perioperative blood loss.69 However, a meta-analysis of seven trials suggested that a higher dose of TXA (>2 g), but not a low dose, was correlated with significantly reduced transfusion requirements.15 In our subgroups stratified based on the high (≥2 g) and low doses (<2 g), no significant difference was observed between the doses and most outcomes. In fact, the effect on blood loss reduction between low-dose and high-dose TXA may be explained by the ‘tissue contact time’—the time when TXA is applied on the joint bed.70 At least 5 min of contact time was allowed before TXA was suctioned from the wound to allow for the repair of the retinaculum.44 Sa-Ngasoongsong et al suggested that prolonging the contact time could enhance the effects of low-dose TXA.70
We were aware of several limitations with respect to this meta-analysis. The number of participants in most of the included studies was small. As the prevalence of VTE was low following joint replacement, trials with a larger sample size were further needed to increase the statistical power. Only a small number of trials evaluated the combined-delivery group, which precluded sufficient exploration of heterogeneity through subgroup or meta-regression analysis. Additionally, many included trials had methodological deficits, such as the description of the randomisation process, blinded assessment and/or explanation of withdrawal and dropouts. Several studied outcomes have been criticised for their inaccuracy. For example, drains may not be suitable for the measurement of blood loss volume, as the haematocrit in the drain output declined over time and drains may increase the blood loss. The existing literature provided variable and heterogeneous information with respect to the clinical features. For instance, the estimated blood loss, timing of Hb measurement and indications for blood transfusion were not standardised among various trials. Several studies used tourniquet to facilitate the arthroplasty procedure, which may adversely impact the efficacy of intraoperative intravenous TXA.44 A meta-analysis showed that the use of a tourniquet was associated with increased risk for vein thrombosis.71 Intraoperative hypotension or hypertension may affect the blood loss volume, whereas related information was unclear in most included trials. Additionally, LOS may be further affected by the patients’ age, surgical experience and/or infection complications. We speculated that these confounding factors were balanced between different comparison groups due to the randomised design. Not searching grey literature and articles in other languages might have also skewed the results. Finally, high heterogeneity was observed in places that might limit the ability to make strong inferences.
Conclusions
Our meta-analysis showed that intravenous and topical TXA had comparable efficacy and safety profiles. The combined-delivery method using intravenous and topical TXA may be the most effective strategy that can be used while maintaining patient safety.
References
Footnotes
Patient consent for publication Not required.
QS and JL contributed equally.
Contributors QS and JL contributed to the conception and design of the study. QS, JL, JC, CZ, CL and YJ contributed to data acquisition or analysis and interpretation. QS and JL were involved in drafting the manuscript or revising it critically for important intellectual content. All authors have given final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All of the data were based on published studies and no additional data are available.