Article Text

Abstract
Introduction Every year, up to 1 billion children are victims of violence worldwide. Most child abuse takes place in the context of punishment. The Families First Programme, an adaptation of the Positive Discipline in Everyday Parenting Programme to the West Java context, is a parenting support programme anchored on children’s rights that gives parents guidance on child development, parenting and positive discipline practices. This trial will evaluate the effectiveness of the Families First Programme compared with a waitlist control group.
Methods and analysis This is a pragmatic, parallel-group, stratified, cluster-randomised controlled trial. Twenty rural and urban villages in the Cianjur District, Indonesia, involving 720 caregivers of children up to 7 years of age, will be randomised. Villages will receive either a parenting programme consisting of 10 group sessions and four home visits over 3 months and standard community health and social services or just the latter. After completion of the trial period, the programme will be offered to those in the delayed group. Outcome data will be collected before randomisation (baseline), immediately postintervention (3 months postrandomisation) and 6 months later (9 months postrandomisation). The primary outcome will be frequency of physical and emotional punishment as measured by a weighted sum from three self-report items. Primary outcome analysis will use Poisson regression with generalised estimating equations and assess the interaction between intervention and time over baseline and 3 and 9 months postrandomisation assessments. Concurrent process evaluation will be conducted to assess programme satisfaction and facilitators and barriers to the implementation of the programme generalisable to other settings.
Ethics and dissemination Ethics approval was obtained from McGill University and Universitas Katolik Indonesia Atma Jaya. Results will be published in peer-reviewed journals and presented at scientific conferences and events for decision-makers, including in the participating communities.
Trial registration number NCT03374761.
- child protection
- epidemiology
- public health
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This study will be conducted as an independent, large cluster randomised controlled trial concerning child discipline in a real-world setting; this is the most rigorous design to address the primary research question.
The number of clusters to be included in this protocol is limited to 20; all of the clusters will be located in one district in West Java, Indonesia. The degree to which our findings may be extrapolated to other settings remains to be explored.
Outcomes will be self-reported by primary caregiver and not interviewer assessed which can potentially bias responses as a result of social desirability.
Due to the nature of the intervention neither participants nor research staff will be masked to allocation. Interviewers will go through a profound assessment training programme.
Structured observation of intervention will not be performed; implementers’ self-reported information will be used to assess implementation fidelity.
Introduction
Child physical and emotional abuse is a major global public health, human rights and social problem.1 Worldwide, a quarter of adults report having been physically abused as children2 and every year up to 1 billion children are victims of violence, with the highest rates in low/middle-income countries (LMIC).3 A national survey of violence against children in Indonesia revealed that 39% of boys and 21% of girls under 18 years of age had experienced some type of violence in the 12 months prior to the survey, with physical (29% boys, 12% girls) and emotional (13% boys, 9% girls) violence being most common.4
Dominant social norms that support harsh punishment of children5 6 and women7 8 and the lack of family support services are among the factors that contribute to violence against children.9 Child physical and emotional abuse mostly takes place in the context of punishment10; the intergenerational continuity of maltreatment11 12 and parenting practices has also been documented in the context of physical punishment (eg, ref 13). Despite wide variation by country, physical punishment is common in LMICs,14 including Indonesia.15 16
Violence against children can have long-term consequences on a child’s physical, social, emotional17 and neural development18 19 and is a social and economic burden for families and societies at large.20 Recent systematic reviews and meta-analyses to estimate the prevalence of child maltreatment in East Asia and Pacific (EAP) countries concluded that the economic burden of child maltreatment is substantial in the region.21 A systematic review on the consequences of child maltreatment in the EAP region showed that children who have been maltreated are four times more likely to think of and attempt suicide and two times more likely to experience intimate partner violence as an adult.22 Similarly, there is ample evidence that physical punishment has negative consequences for child development and health as well as psychiatric disorders in adulthood.23–26
Evidence-based parent education, early childhood home visiting and multicomponent interventions have emerged as promising child violence prevention strategies.27–30 A recent systematic review of parenting programmes aimed at reducing rates of physical abuse recidivism documented statistically significant, although modest, reductions in child physical abuse and called for further methodologically rigorous research in this area.29 Similarly, systematic reviews of home visiting programmes, including those delivered by paraprofessionals to disadvantaged families, have found them effective in preventing child abuse and increasing positive parenting.28 31 However, hybrid interventions that combine parenting group-based programmes with home visits are few32 and have not aimed at violence prevention in LMICs. Overall, systematic reviews and meta-analyses have highlighted the need for more research on the effectiveness of child violence prevention interventions in LMICs.33 It is important that programmes are culturally appropriate for participants in order to ensure acceptability and effectiveness.34 There are examples where transporting parenting programmes across countries to address child behaviour problems has shown promising results,35 but researchers have raised concern about the applicability of current evidence outside of English-speaking, high-income countries.27 Contemporary parenting research and validated parenting measures in Indonesia are scarce. A review of parenting education programmes in Indonesia concluded that more attention is needed to teach non-violent discipline techniques to parents of young children as well as to conduct research and evaluation on parenting education.36 The only evaluation of an evidence-based parenting programme for parents in Indonesia, a randomised controlled trial (RCT) to test the efficacy and acceptability of the Triple P-Positive Parenting Programme seminar, showed sustained intervention effects in child behaviour, parental stress and parenting practices and confidence compared with parents in the waitlist control group.37 Participants in this study were parents of children aged 2–12 years and had ‘relatively good financial status’ and education.
This cluster RCT will evaluate the effect of the Families First with Home Visitation Programme38 on the frequency of physical and emotional punishment among children aged 0–7 years in the West Java province of Indonesia. Families First is an adaptation of the Positive Discipline in Everyday Parenting (PDEP) support programme. It is based on research on children’s healthy development and effective parenting and grounded in principles of children’s rights. The programme is delivered in 10 group sessions and has four components: (1) identifying parents’ long-term childrearing goals; (2) providing warmth and structure; (3) understanding how children think and feel; and (4) problem-solving.39 40 Pre/post PDEP programme evaluations in other contexts have shown lower endorsement of physical punishment and higher parenting self-efficacy41 and satisfaction with the programme42 among participants. The adaptation of the programme to the West Java context entailed the cultural adaptation and translation of teaching materials and the addition of four home visits to the group sessions delivered by trained community facilitators. Findings from a pilot test of the programme in 2015 were used to further refine the programme before beginning the present trial. The present trial responds to a need to rigorously evaluate violence prevention interventions in LMICs and their cultural adaptation to different settings.43 Both the Ministry of Social Affairs through its Program Keluarga Harapan (PKH) or Family Hope Programme and the Ministry of Women Empowerment and Child Protection through the Pusat Pembelajaran Keluarga (PUSPAGA) or Family Learning Center Programme have committed to integrating and scaling up the programme nationally. The primary objective of this study is to estimate the extent to which the Families First programme impacts on the frequency of the use of physical and emotional punishment, as measured by a weighted summed score from three self-report items, among caregivers of children aged 0–7 years in Cianjur District, West Java, Indonesia, compared with caregivers in a waitlist control group. We hypothesise that the change in frequency of reported use of physical and emotional punishment among caregivers will be more positive in the intervention group than the change in the waitlist control group.
Methods and analysis
Trial registration
The trial is registered with ClinicalTrials.gov NCT03374761. Trial registration was initiated before participant recruitment yet it was only completed when data collection was under way due to staff changes and relocation of the trialist’s lab. Modifications to the protocol will be updated online.
Design
This is a pragmatic, delayed-entry, parallel-group, stratified, cluster RCT in a real-world setting (figure 1). Twenty rural and urban villages, involving 720 caregivers of children up to and including 7 years of age, will be randomised to two parallel arms. A waitlist control design will be adopted to promote acceptance of the research process by the communities. There will be one primary outcome, namely frequency of caregiver reported physical and emotional punishment. Only one child will be assessed per caregiver. Mixed methods will be used to assess study outcomes and to map the causal chain from programme targets to outcomes.

Trial flow chart.
Eligibility
Communities
Data will be collected in 20 villages or clusters that are representative of the general population in four subdistricts (Campaka, Ciranjang, Karangtengah and Naringgul) in Cianjur District, West Java, Indonesia. This is a priority area for the implementing agency due to high incidence of child protection concerns such as being a well-known sending area for human trafficking and migrant workers to the Middle East or Asia, and institutionalisation of children.44 Selected villages will consist of (A) rural and urban/periurban communities with similar size and average household income; (B) that have not been previously exposed to Families First; (C) that are within a 1 hour driving distance of the subdistrict capital and 1–8 hours driving distance of Cianjur Regency, the district capital; (D) that are located at ample distance from other clusters (to minimise intervention contamination); and (E) that have local political leaders who express strong support for the intervention and the evaluation.
Participants
Eligible families will: (A) have at least one biological or adopted child aged up to and including 7 years, in line with the implementing agency’s focus on early childhood education to set a good foundation for parenting and to complement existing government programmes for parents of young children; (B) have at least one risk factor associated with the placement of children into residential care16 as per Save the Children’s child protection framework in Indonesia, including living below the government poverty line or receiving social protection programme, being a single and teenage mother, and having a father or mother who has migrated or a mother who is considering migration; (C) reside in the village and not have the intention to move away in the next year; (D) have at least one female caregiver who has not been previously identified as having cognitive impairment and who is able to provide informed consent and to speak and read in Bahasa; (E) have never engaged in any another parenting programme; and (F) provide informed consent to participate.
Procedure
A database containing maps and information for all inclusion criteria for each village in the four subdistricts will be created to evaluate village eligibility. The implementing agency will approach and obtain agreement from local authorities. Final selection of 20 villages will be made by the local research team in collaboration with the implementing agency to ensure representation of all subdistricts and strong political support of village leaders while reducing the risk of contamination. The implementing agency will validate the selection with village authorities and introduce the research team for further communications regarding the evaluation. Individual families in each village will be approached by local research team members to obtain informed consent for participation in the trial.
Randomisation and allocation concealment
Stratified randomisation will be used to allocate 20 clusters among 47 eligible clusters in rural (65%) and urban (35%) settings in the four subdistricts in a 1:1 ratio for the intervention and the control arms. Clusters will be randomised to avoid resentment or contamination that might occur as a result of delivering the intervention to some families but not others in the community. Randomisation will be done in a random allocation ceremony led by the research team and attended by the chiefs from all participating villages and staff from the implementing agency. The ceremony will follow a step-by-step lottery and documentation procedure that will include the use of 20 sequentially numbered (1–7 ‘Urban’ and 1–13 ‘Rural’), opaque, sealed and stapled envelopes independently prepared by the lead investigator. Aluminium foil inside the envelope rendered the envelope impermeable to intense light. First, envelopes will be drawn by urban villages, followed by rural villages. The ceremony will be video-recorded.
Eligible families in each village will be identified before randomly assigning villages. In each village, the implementing agency will create a list of 50 eligible families through review of village administrative records and discussion with local providers and authorities. The research team will randomly select participants from these lists and verify eligibility until successfully recruiting and consenting 36 families per village.
Intervention sites
In addition to the standard, government-run services that are currently provided by community health volunteers in West Java, intervention sites will receive a 10-week programme of group sessions with caregivers and four home visits, each session/visit lasting approximately 1.5 hours. Three groups of 12 caregivers each who are anticipated to be mostly mothers will be offered the programme in each village.
Control sites
Control sites will receive the standard, government-run services that are provided by community health workers in West Java. Once the evaluation of the intervention arm is completed, participants in the control arm will be offered the intervention.
Programme delivery and training
The intervention will consist of 10 group sessions and four home visits to provide parents with information on child development, parenting and positive discipline practice (table 1). The intervention follows the PDEP curriculum that has been adapted as Families First for the Indonesian context (Families First Programme).38 The main changes introduced entail the addition of home visits, the cultural adaptation of examples and illustrations, and the translation of all materials into Bahasa Indonesia. Following the delivery of the adapted programme in 2015 and 2016 in Bandung Barat and seven villages in Cianjur other than the ones in the trial sample, materials and language were refined before commencement of the trial. The 10 group sessions will combine group activities and case studies with didactic teaching by facilitators. The home visits will use visual materials and role-plays to promote positive parenting approaches. Community facilitators will provide referral to social protection and other community services, as needed. Each parenting group will be led by two programme facilitators, who will also conduct the home visits. Catch-up sessions will be arranged individually with the community facilitators by participants who are unable to attend a session.
Intervention topics by type of delivery
The programme will be managed by Save the Children-Indonesia and delivered to parents by locally recruited programme facilitators, who are paraprofessionals, such as community health workers and preschool teachers, and other social auxiliary workers who live in the community and are recommended by local village authority. Facilitators must be mothers themselves or be at least 19 years of age and have experience in working with families; be open minded and have listening and facilitation skills; have at least high school education and ability to read and write in Bahasa Indonesia; be interested in the topic; and be available to attend the full training and to deliver the full programme. All programme facilitators will receive a 1 week initial training by Save the Children and the developers of the PDEP from the University of Manitoba, Canada. This training will be participatory and activity based, and training materials with weekly lesson plans will be provided to them in Bahasa and will contain extensive visuals and hands-on exercises. Facilitators will be supervised weekly by Indonesian programme mentors who are fully trained in the programme by PDEP developers and have had experience delivering the programme in the past. Besides the same criteria for the selection of facilitators, mentors must be willing to spend half day per week (excluding travel time) mentoring facilitators throughout the implementation of the programme. Mentors will be, in turn, supported by the University of Manitoba team, Save the Children-Indonesia and a faculty member from the University of Padjadjaran (Indonesia) experienced in delivering and teaching the programme.
Measurement strategy and measures
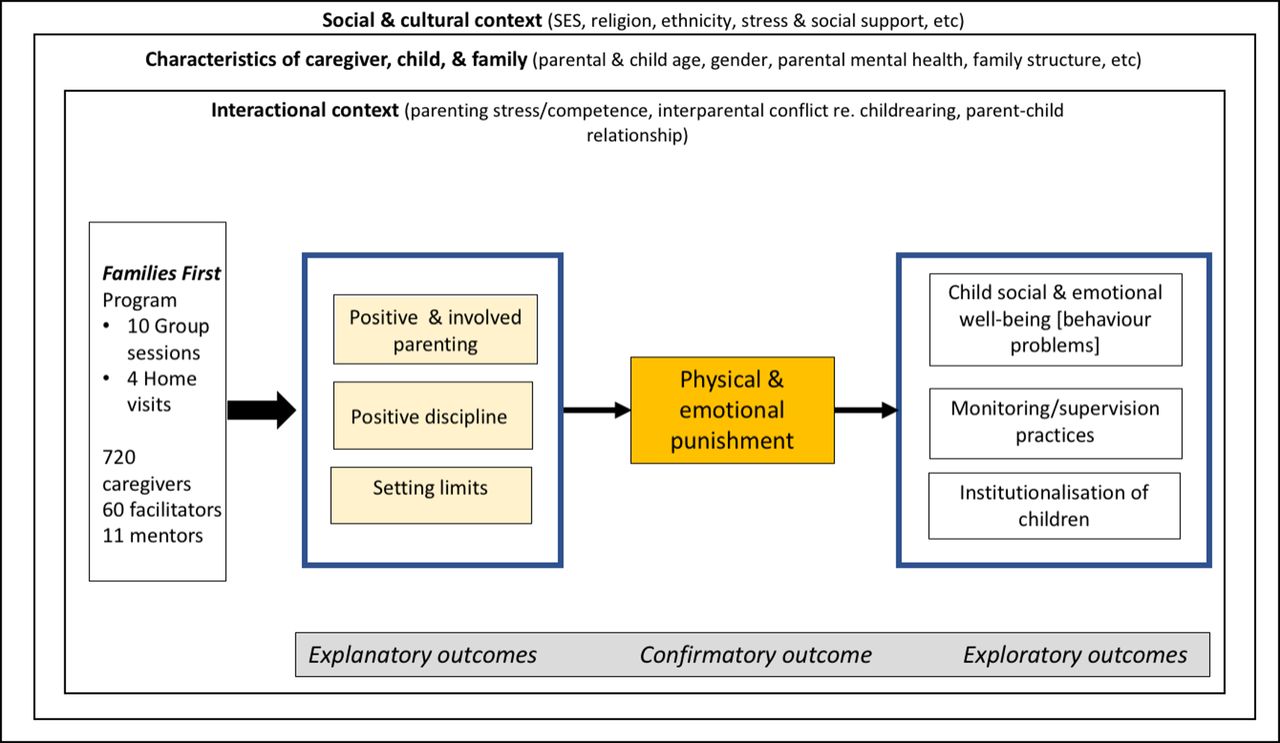
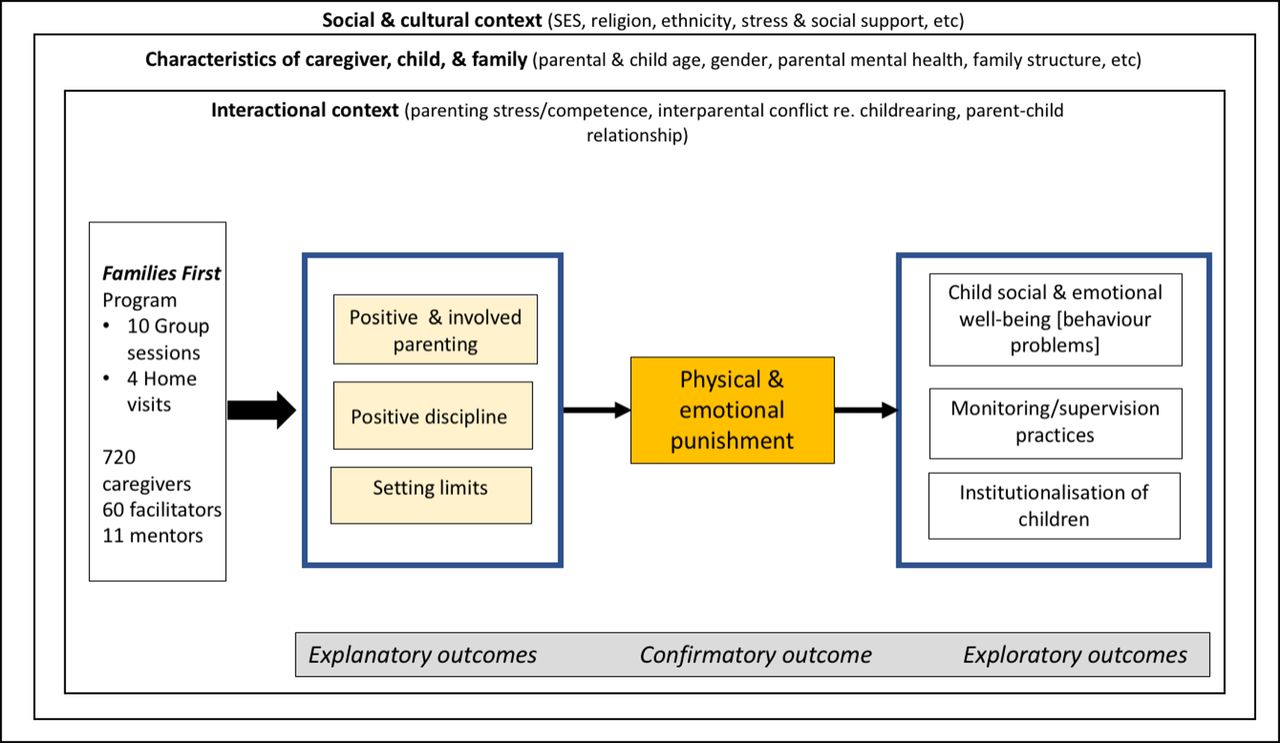
Child discipline behaviours occur in sociocultural, personal and family contexts that are depicted by three nested squares.45 Within these contexts we illustrate three types of outcomes46: one primary or confirmatory outcome and several explanatory and exploratory outcomes. Explanatory outcomes are those that are proposed to be directly targeted by the activities of the Families First programme. Changes in the primary outcome, frequency of physical or emotional abuse, are hypothesised to occur because of changes in knowledge, attitudes and behaviours in these domains. As a result of changes in these outcomes, we hypothesise that positive changes will occur in measures of child well-being, monitoring and supervision, and caregiver attitudes to institutionalisation of children.
To operationalise this measurement strategy, well-established measures were initially identified, prioritising the use of measures that are available without cost, have been used in LMICs, are culturally appropriate for the Cianjur context and use a language focused on parental change. However, pilot testing of full measures that had been previously applied in this field raised concerns about the number of measures and items and that many items would not be appropriate or relevant to the context. Thus, an alternative measurement strategy, using outcome indicators, was adopted. Outcome indicators could be single items, indices based on summing responses over several related items; or full measures or subscales with total scores validated using Rasch Analysis to test the extent to which the items fit a unidimensional hierarchical model with interval-like properties such that the total score can be used in mathematical transformations.47–49 All measures were independently forward and back-translated (Bahasa and Sundanese) by local consultants.
Families will be assessed against the main outcomes at study entry/baseline (T1), immediately after the end of the intervention (T2) and 6 months postintervention (T3). All measures except for programme satisfaction (only assessed postintervention) will be administered at the three measurement points. To maximise sample retention and document any relevant community changes, we will visit all sites and meet with local authorities prior to returning for data collection. They will in turn be able to inform residents of the upcoming visit of the research team.
In families with more than one child, one child (index child) will be randomly selected at the beginning of the baseline interview, and data collection will focus on that child. Only data on reasons for non-participation will be collected from participants who withdraw from the study.
Outcomes
Measures that were created or adapted for the trial are included in the online supplementary appendix and items relevant for specific outcomes are indicated below.
Primary outcome
Frequency of use of physical and emotional punishment as measured with three self-report items inspired on the International Society for Prevention of Child Abuse and Neglect Child Abuse Screening Tool (ICAST-Parent),50–52 including an item on severe physical abuse, an item on moderate physical abuse and an item on emotional abuse. Each item asks caregivers how many times they have applied physical or emotional punishment such as the ones described in the item with the index child in the past month and ever (online supplementary appendix A). Frequency will be calculated for each person at each time point by creating a total punishment event-days. Item responses for each of the three items are almost every day, at least once per week, once a month, sometimes but not in the last month and never. Responses to each item will be assigned a value in days over the month: almost every day=30; at least once per week=8; once a month=1; sometimes but not in the last month=0.5; never=0. These values will be summed over physical and emotional punishment. This format gives more weight to changes from almost every day to at least once per week. A sensitivity analysis will be used to determine if different weighting values affect the results.
Supplementary file 1
Explanatory outcomes
Positive and involved parenting will be measured with self-report items adapted from the Positive Parenting Subscale (six items) and the Involvement Subscale (one item) of the Alabama Parenting Questionnaire (APQ)53 54 (online supplementary appendix B1). Positive discipline will be measured with four items from the Non-violent Subscale of the ICAST50 51 (online supplementary appendix B2). Setting limits will be measured with two items from the Setting Limits Subscale of the Parenting Young Children55 (online supplementary appendix B3). Opinion on discipline will be measured with two items from the ICAST-Parent50 51 (online supplementary appendix B4).
Exploratory outcomes
Child social and emotional well-being will be measured with the Strengths and Difficulties Questionnaire (SDQ) parent versions for 2–3 year-olds and 4–17 year-olds.23 56 57 The emotional, conduct problem, hyperactivity and peer problem scales will be included in full and, as per SDQ guidelines, their scores will be summed to generate a Total Difficulties score for each index child. Items from the prosocial scale (ie, Helpful if someone is hurt, Kind to younger children, Often volunteers to help others) will be excluded from this calculation. Attitudes towards institutionalisation of children will be measured with four items adapted from the Child Protection Knowledge, Attitudes and Practices58 and four new items (online supplementary appendix C1). Monitoring/supervision will be measured with items from the Poor Monitoring/Supervision (10 items) of the APQ and the Parent Supervision Attributes Profile Questionnaire (one item)59 (online supplementary appendix C2).
Contextual and other influencing factors in parenting and child abuse
Parenting stress will be measured with the Parental Stress Scale (18 items).60 Caregiver mental health will be measured with the WHO Wellbeing Index (WHO-5) (five items).61 Perceived social support will be measured with items from the Tangible/Instrumental Support (four items) and Emotional Support (four items) Subscales of the modified Medical Outcomes Study Social Support Survey.62 One item from instrumental support subscale (‘help when confined to bed’) will be replaced with ‘help you care for a child’. One item from the emotional support scale (‘to love and make you feel wanted’) will be changed to read ‘to love you and show you affection’ (online supplementary appendix D1). Stimulation in the home environment will be measured with items from the Early Childhood Development Module (six items) of the Multiple Indicator Cluster Survey,63 64 one item adapted from the Involvement Subscale of the APQ and two additional items (sharing meals and exploring toys alone) (online supplementary appendix D2). Interparental conflict regarding childrearing will be measured with 11 items from the Parent Problem Checklist65–67 (online supplementary appendix D3). Sociodemographic characteristics that will be documented include: (A) Child: age, gender, siblings and orphanhood status, physical health/disability and schooling; (B) Caregiver: age, gender, marital status, education level, physical and mental health, ethnicity and cultural background, employment status; (C) Family: urban/rural location, type of residence, household structure, and family structure, functioning, and socioeconomic status.
Blinding
It will not be possible to blind the investigators to the allocation of participants because it is a behavioural intervention and the outcomes are self-reported. However, data collection research assistants will be trained on consistent administration of measures and awareness of biases.
Process evaluation and qualitative assessments
Process evaluation68 69 will be conducted to assess variability in implementation and to identify the contextual and operational factors most likely to lead to successful implementation in other settings. Figure 2 is a theoretical model for how we hypothesise the intervention impacts on physical and emotional punishment. The variables in the pathway from intervention to outcome (punishment) are considered mediators and include positive and involved parenting, positive discipline and setting limits. The contextual factors are considered to be effect modifiers or confounders. We will also look at attendance and participation in the intervention and implementer fidelity. Process evaluation outcomes will be assessed through checklists to track implementation fidelity and programme exposure/attendance, and a brief programme satisfaction questionnaire for caregivers in intervention sites, facilitators and mentors postintervention. Facilitator’s tracking forms will be used to record attendance and level of engagement by caregivers, as well as the extent to which facilitators followed the programme manual. The programme satisfaction questionnaire will be administered to all participating caregivers (17 items), facilitators (23 items) and mentors (22 items) in intervention villages. They will all be asked to identify up to two of their favourite and least favourite sessions, and to rate the likelihood that they will (A) use the material and (B) recommend the programme to others (4-point scale). An open-ended question will elicit recommendations for improving the programme and how it is provided. Caregivers and facilitators will be asked to rate how satisfied they are with different aspects of the programme (eg, duration, frequency and ease of access to meetings) and overall satisfaction with the group sessions and home visits (5-point scale). Facilitators and mentors will be asked to assess the facilitators they worked with on a range of skills (eg, explaining programme material according to the curriculum and engaging families). Implementer records of programme attendance and fidelity in the delivery of the intervention (as assessed by observation of sessions by mentors) will also be reviewed. Detailed information about implementation and experiences of intervention will also be obtained from a purposively selected sample of participants using qualitative methods.
{kind=link}
{kind=link}
General conceptual model of programme influences on parenting and child well-being. SES, socioeconomic status.
Linked qualitative methods will be used to develop and validate data collection measures (pilot) and to add depth and understanding of process and outcomes.70 71 Following delivery of the programme, they will explore caregivers and implementers’ experiences in the programme and how service delivery, socioeconomic, cultural and other factors may impact the effectiveness and scalability of the intervention. Qualitative methods (in Bahasa and Sundanese) will include semistructured interviews with caregivers, implementers (Save the Children staff, mentors and facilitators) and community leaders (n≈35); focus group interviews with participating caregivers and implementers (n≈10–15); independent observation of group sessions; and record analysis. Interviews will explore factors that support or hinder the implementation of the intervention, perceived effects (positive and negative) of the intervention and comparison to other local community services for children and families. Participants will be selected from all 36 groups in intervention villages and also include special cases (eg, dropouts and ‘model participants’) identified through observations and programme satisfaction questionnaires.
Data collection
Data collectors will be selected by the local research team among female university graduates fluent in Sundanese and Bahasa and who have prior interviewing experience and are available during predetermined data collection periods. Data collectors will be trained in the interview protocol, interviewing techniques and how to avoid bias, ethical conduct of research, use of the tablet and visual scales (for survey), safeguarding of children and data management and communication procedures. Training will include lectures, demonstrations, role-play and several days of field-testing before data collection.
A systematic review was conducted to identify existing measures for the outcomes of interest which had been used in Indonesia and/or other LMICs. The measures most appropriate for the Cianjur context were complemented with sociodemographic items adapted from Indonesia’s yearly socioeconomic survey.72 The questionnaire was forward and back-translated in Bahasa, pilot tested with 10 comparable respondents in two villages in Cianjur not included in the sample and refined before translation into Sundanese and programmed into the Census and Survey Processing System (CSPro). Tablet-based questionnaires will be administered orally to caregivers in their homes.
Data management
The CSPro will be used for collection of data and daily uploading to a secure server hosted by McGill University. For quantitative data to be inputted (eg, tracking forms from facilitators), provisions will be made for double-checking of data entered through preprogramed software. Non-electronic data will be stored securely in a locked cabinet and electronic data text and audio files with ID-identified cases will be maintained in password-protected tablets, computers and online storage space. An ID will be assigned to each case in all analyses. Only a small number of research team members will have access to personal identifiers. Names of individuals and specific study locations will not be provided when reporting study findings. All nominal information will be destroyed 5 years after completion of the study.
Statistical analysis and sample size calculation
The study is powered to detect a change considered to be both meaningful and plausible on the primary outcome. A sample size of 720 families will allow measuring a reduction of 15.2% in parent-reported use of violent discipline at home from the initial estimated prevalence of 30% (SKTA 2013)4 with an α level of 0.05% and 90% power, assuming 0.02 intraclass correlation73 74 and 80% participation rate.75 One child per family will be selected as the index child.
Types of analysis
There will be administrative analyses done to ensure data accuracy on a continual basis. Once all participants have been randomised, descriptive statistics will be used to compare the two groups at baseline, recognising that clustered randomisation does not necessarily achieve balance on covariates at the individual level. Once data collection has ended, analyses of outcomes will commence. The primary outcome, frequency of physical and emotional punishment practices in the past month, will be aggregated into a cumulative rate of number of punishments over 30 days. This rate will be ascertained for all participants in both trial arms at three time points. The main analysis will be Poisson regression using generalised estimating equations (GEE) to test the main hypothesis related to the superiority of the programme in reducing the rate of physical and emotional punishment over a 9-month period. Outcomes will be measured at baseline, end of intervention (3 months postrandomisation) and 6 months after end of intervention (9 months postrandomisation). The superiority of the programme will be tested by including the main effects for programme and for time along with a programme by time interaction. The linearity of the association with time will be considered to allow for the possibility of non-linear associations. Variables which reduce variance in the outcome will be considered for inclusion (eg, sex and position (parent or child) of the reporting family member, number of children in the family, and so on). Although confounding is not expected to be an issue due to the randomisation, villages will be compared on key factors and any variables showing large imbalances by randomisation group will be added to the model. All outcomes will be analysed adopting an intention-to-treat principle and all persons will be analysed in the groups to which they were randomised. Although all efforts will be made to keep missing data to a minimum, any potential bias will be minimised by performing multiple imputation on the longitudinal data. All variables considered for the final analysis will be included in the imputation model.
Secondary analyses will estimate the impact of the programme on the other relevant outcomes. Programme effects will also be examined using GEE to adjust for clustering of members within families and families within villages. Counts will be analysed with Poisson regression, binary outcomes with logistic regression and continuous scales with linear regression.
Additionally, gender-based analysis (sex of the child) and analyses to also determine whether sex of the child or families with more children or children of different age groups, or families with differently abled children respond differently to the programme will be conducted for exploratory purposes. Another subgroup analyses will explore the impact of the intervention among people in single-headed households, first-time parents and teenage parents. Analysis and reporting of the results will follow the Consolidated Standards of Reporting Trials guidelines for reporting RCTs and the extension for non-pharmacological treatment interventions.76–78 Descriptive quantitative process information will accompany the qualitative analysis of data.69 Qualitative data will be transcribed, translated and coded using NVivo.79 Initial codes relating back to the research questions and interview guidelines will be complemented with open coding of the entire data set, refined and grouped into broader headings around factors that facilitate or hinder implementation of the programme and satisfaction of participating families and staff. Compelling quotes will be extracted to illustrate findings. Quantitative and qualitative results will be analysed sequentially to triangulate results, identify convergences/divergences, explain anomalous data and enhance the overall interpretation of findings.80 Preliminary findings will be shared with the advisory committee and interpreted in the context of relevant policies.
Coordinating centre
The research and academic staff at McGill University provide scientific support and oversight and coordinate all trial activities. The research staff at the SMERU Research Institute in Jakarta run the fieldwork and coordinate with the advisory committee and with local actors for permits and dissemination of findings.
Monitoring
The study will be monitored for quality, contextual appropriateness and regulatory compliance. During data collection, close supervision of interviewers, instant messaging (WhatsApp and email) and timely data monitoring between researchers in Canada and Indonesia allows early correction of problems. An independent advisory committee composed of academics and specialists with an expertise in child protection in Indonesia from government, non-governmental organisations (NGO) and donor agencies will participate in the continuous monitoring of the study. Programme implementers will monitor the intervention through facilitators and mentors’ weekly meetings, and local visits by other programme staff. Any adverse event affecting participants on the study observed by researchers or implementers will be assessed by the principal investigator and partner NGO to decide whether additional investigation or a modification of the intervention may be indicated. All data collectors and other research team members in contact with children will be trained in and commit to respect the SC child safeguarding policy,81 including an obligation to report child abuse cases. Referrals to relevant services will be made when appropriate with consent from the participant. This plan will be explained to trial participants during the consent process.
Participant and public involvement
The experiences of caregivers in West Java who participated in the pilot programme informed the refining of the intervention and the development of outcome measures. The perspectives of caregivers were also key to testing and refining the study materials and procedures (eg, shortening questionnaires and data collection forms, rewording/replacing several items, and planning data collection around individual availability/preferences and community events). Participant satisfaction with the intervention, including burden, will be assessed as part of the process evaluation. Results will be shared through community meetings and all participants will be invited to attend.
Ethics and dissemination
Ethics approval was obtained from the McGill University Faculty of Medicine Institutional Review Board (IRB, Montreal, Canada) and the Universitas Katolik Indonesia Atma Jaya Research Ethics Committee (Jakarta, Indonesia). The IRB requires renewal every 12 months and approval for any protocol modifications when indicated. Additional approvals were obtained from Badan Kesatuan Bangsa dan Politik at national, provincial and district levels as well as from subdistrict and village offices in Indonesia. Informed consent will be obtained in the local language first for randomisation, from the village chief, and then from participants at each data collection point. Signed informed consent will be obtained at the start of the trial. Participation in the trial will be voluntary and no incentives will be provided. Only a small compensation such as an umbrella or a tote bag will be provided to participants. Transportation costs will be reimbursed for focus group interviews. To guarantee confidentiality, individual interviews will be conducted in a private space, permission will be obtained to audio-record and an ID will be assigned to each case in all analyses. All data collectors will sign a contract letter on protecting confidentiality of any information given to them by respondents.
Results of the main trial and other evaluation findings will be submitted for publication in international peer-reviewed journals and presented at international and regional scientific conferences and webinars. Public presentations and research briefs will provide study findings in the local language(s) to all participating villages, local leaders, government departments, Unicef and major NGOs working with children in Indonesia and internationally. Investigators will be involved in reviewing drafts of the manuscripts, abstracts, press releases and any other publications arising from the study. Furthermore, community public engagement with various forms of media will also be used to disseminate study information. On completion of the trial, and after publication of the primary manuscripts, data requests can be submitted to the researchers at McGill University.
Discussion
This study will provide essential evidence to take the Families First programme ‘as is’, improve it, or discard it as not effective and to inform possible scale-up in Indonesia and replication in other countries. Considering the large number of children who have experienced some type of violence in Indonesia,4 a country home to more than 65 million children under 15 years,82 the potential impact of this study is substantial. Indonesia has declared its commitment to reducing violence against children in line with its ratification of the Convention on the Rights of the Child (1989) and the Child Protection Act No 23 of 2002. The interest shown by the Indonesian government and Save the Children attests to the need to develop, adapt and rigorously evaluate child violence prevention interventions in LMICs. Despite a well-established evidence base in high-income countries, there are few studies to date of the effectiveness of parenting programmes and early childhood home visiting to prevent violence against children in LMICs overall43 and particularly in Indonesia. By increasing external validity, real-world pragmatic trials are of particular value to assist decision-makers. Moreover, the combination of impact and process outcomes within a pragmatic cluster RCT design has the potential to provide scientists and decision-makers with knowledge generalisable to other low-resource areas about factors influencing successful implementation of parenting interventions. Within the limitations stated earlier, this study will contribute to filling this knowledge gap and building capacity by recruiting and training local researchers. By intervening early, the programme also aims to reduce the likelihood that children will be placed in institutional care, either voluntarily by their parents or involuntarily as a result of intervention by social workers.16 Ultimately, it will support Save the Children, other NGOs and governments to design appropriate prevention interventions for this context. Regardless of whether results are positive or negative, the process evaluation will inform commissioners and practitioners about what contextual and operational factors will be most likely to lead to successful implementation in other settings.
Timeline
Recruitment started in March 2017 and baseline information was collected from 736 caregivers in 20 villages. Programme implementation extended longer than 10 weeks in response to local events, including interruption of activities around Eid al-Fitr. Post-test and first round of qualitative data collection took place between September and November 2017, followed by data checks and transcription and translation of qualitative data over a 3-month period in Indonesia. At the time of submission of this protocol in January 2018, the trial was still ongoing.
Acknowledgments
The authors thank other members of the Families First Study Group who contributed to the study: Alice Shirley, Rebecca Smith and Katherine Rice (Save the Children, London, UK); Tata Sudrajat and Andri Yoga Utami (Save the Children-Indonesia, Jakarta, Indonesia); and Nina Toyamah, Ulfah Alifia, Nurmala Selly Saputri, Ridho Al Izzati and Rezanti Pramana (SMERU Research Institute, Jakarta, Indonesia). The author also thank Irwanto for his input in the original grant proposal. MRC and BDT were partly funded by Salary Awards from the Fonds de Recherche du Québec-Santé.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
Footnotes
Contributors MRC and SL conceived the study and drafted the original grant proposal. MRC drafted an extensive study protocol and the manuscript for publication. NM provided overall guidance in RCT design, contributed to the development of the extensive study protocol, performed sample size calculations and registered the trial. BDT and RWP provided overall guidance in RCT design and statistical guidance in the development of the protocol. SS planned the statistical analyses. WI provided feedback on study design and liaised with advisory committee. EH and MA participated in the adaptation of the trial methods to the local context and have responsibilities for day-to-day running of the trial. SL contributed to the conceptualisation of the study and to securing funding. All authors read and approved the final version of the manuscript.
Funding This work is supported by Save the Children Fund (no assigned grant number) and the Children and Violence Evaluation Challenge Fund (grant number 058), a joint initiative funded by the Bernard van Leer Foundation, Oak Foundation, UBS Optimus Foundation and an anonymous donor and hosted by the Network of European Foundations (NEF).
Disclaimer The sole responsibility for the content lies with the authors and the content may not necessarily reflect the positions of NEF/Children and Violence Evaluation Challenge Fund or the sponsoring foundations. SL and the funding sponsors will have no role in the collection, analyses or interpretation of data; and in the writing and decision to publish the results.
Competing interests All coauthors report grants from Children and Violence Evaluation Challenge Fund–Network of European Foundations and from Save the Children Fund, during the conduct of the study. RWP reports personal fees from AbbVie, Amgen, Eli Lilly, Pfizer and Searchlight Pharma, outside the submitted work.
Patient consent Not required.
Ethics approval Study protocols were approved by the Faculty of Medicine Institutional Review Board, McGill University (A10-B53-16B), the Universitas Katolik Indonesia Atma Jaya Research Ethics Committee (/III/LPPM-PM.10.05/01/2017), the Indonesian Ministry of Home Affairs, and the provincial and district governments.
Provenance and peer review Not commissioned; externally peer reviewed.