Article Text

Abstract
Objectives and setting Although psychotropic drugs are used to treat mental health disorders, little evidence analyses the effects the 2008 economic downturn had on psychotropic drug consumption in the case of Spain. We analyse these effects, considering both gender and employment situation.
Participants We used the microdata from the face-to-face cross-sectional population-based Spanish National Health Survey for two periods: 2006–2007 (n=28 954) and 2011–2012 (n=20 509). Our samples included adults (>15 years old).
Methods The response variables are consumption (or not) of antidepressants or sedatives and the explanatory variables are the year of the survey, gender and employment status. Covariates are mental health problems, mental health index General Health Questionnaire (GHQ-12) and self-reported health outcome variables such as self-rated health, chronic diseases, smoking behaviour, sleeping hours, body mass index, physical activity in the workplace, medical visits during the past year, age, region of residence (autonomous communities), educational level, marital status and social class of the reference person. Finally, we include interactions between time period, gender and employment status. We specify random effects logistic regressions and use Bayesian methods for the inference.
Results The economic crisis did not significantly change the probability of taking antidepressant drugs (OR=0.56, 95% CI 0.18 to 2.56) nor sedatives (OR=1.21, 95% CI 0.26 to 5.49). In general, the probability of consuming antidepressants among men and women decreases, but there are differences depending on employment status. The probability of consuming sedatives also depends on the employment status.
Conclusions While the year of the financial crisis is not associated with the consumption of antidepressants nor sedatives, it has widened the gap in consumption differences between men and women. Although antidepressant use dropped, the difference in consumption levels between men and women grew significantly among the retired, and in the case of sedatives, risk of women taking sedatives increased in all groups except students.
- economic downturn
- mental health
- psychotropic drugs
- drug utilisation
- health surveys
- cross-sectional studies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- economic downturn
- mental health
- psychotropic drugs
- drug utilisation
- health surveys
- cross-sectional studies
Strengths and limitations of the study
Microdata from the Spanish National Health Survey 2006–2007 and 2011–2012.
Random effects logistic regressions so the intercept is different for the various levels considered.
The Bayesian estimation provides greater flexibility (a consequence of its hierarchical strategy).
We use penalising complexity priors. These priors are invariant to re-parameterisations and have robustness properties.
The cross-sectional study design has difficulty in establishing a relationship between explanatory variables and outcomes.
Introduction
Since the Great Depression in 1930, concern about the effects of economic downturns on the health of a population has increased1–3 and while there are some controversial conclusions in the literature, most studies agree that mental health problems worsen during economic crises.4–6 As the current financial crisis represents the worst macroeconomic shock since the Great Depression,7 and government-introduced austerity measures are only aggravating an already grave situation (eg, in the third quarter of 2007 the unemployment rate was roughly 8.1%, meanwhile by the same quarter of 2011 it had increased to approximately 21.3%), and investigating the association between economic downturn and mental health is more important than ever.8–14
The Organization for Economic Co-operation and Development countries all experienced the effects of the 2008 financial crisis, but the Spanish economy was one of the hardest hit and its citizens had to rapidly come to terms with its consequences. In this context,15–19 Spain provides a unique opportunity to analyse the impact on financial crisis has on the health of a population. Spanish data agrees with the association made between a financial crisis and mental health problems.20–25 Although psychotropic drugs are used to treat mental health disorders, little (and contradictory) evidence analyses the effects the 2008 economic downturn had on psychotropic drug consumption.
Barceló et al 26 concluded that the increase in psychotropic drug consumption post 2009, is significantly higher among those most likely to be unemployed and those who were consumers before 2009. Moreover, the use is usually higher for those whose probabilities of consuming other drugs or alcohol are lower (eg, women).27 Interestingly, Colell et al 28 do not find any changes in sporadic use of hypnotics/sedatives between 2005–2007 and 2009–2011 and while they find unemployed men have a higher probability of reporting sporadic use than employed men do, this is lower for unemployed women.
This paper analyses differences in psychotropic drug consumption (antidepressants and sedatives), among the Spanish population between 2006–2007 and 2011–2012 (ie, before and during the financial crisis) by considering two of the most important determinants of health inequalities: gender and employment status.29
Methods
Data setting
We used the microdata from the face-to-face cross-sectional population-based Spanish National Health Survey (SNHS) for two periods: 2006–2007 and 2011–2012.30 31 The SNHS is a stratified tri-stage sample design representative of the Spanish population. Our samples included individuals (>15 years old) responding to both adult and household questionnaires (n=28 954 for 2006–2007 and n=20 509 for 2011–2012). The difference between the sample sizes is because the SNHS 2006–2007 increased its initial sample size in Aragón, Baleares, Cantabria, Galicia, Murcia and Navarra (six out of the 17 Spanish regions) to reach the specific goals of obtaining more accurate estimations for the smaller geographical areas in those regions (eg, NUTS4 or health areas). However, the SNHS 2011–2012 did not include those specific goals.
The response variables are consumption (or not) of antidepressants or sedatives, because in the SNHS questions related to mental health problems these are the only ones asked for.
The explanatory variables are: the year of the survey (ie, 2006–2007—prior to the economic downturn, and 2011–2012—during the financial crisis), gender and employment status.
Covariates are age, region of residence (autonomous communities), educational level, marital status, social class of the reference person,32 mental health problems (represented by whether the individual has suffered from depression, anxiety or other mental health disorders in the past 12 months), a mental health index (GHQ-12)33 and self-reported health outcome variables such as self-rated health, chronic diseases, smoking behaviour, sleeping hours, body mass index,34 physical activity in the workplace and medical visits during the past year. For further information, see the appendices material (supplementary appendix A).
Supplementary file 1
Finally, we include interactions between time period and gender, time period and employment status and between gender, time period and employment status.
Patient and public involvement
Patients and or public were not involved in this research.
Statistical methods
We specify random effects logistic regressions. In mixed model terminology, we allow the intercept to be random effect so it will be different for the various levels considered, that is, year, autonomous community and the interaction between year and autonomous community. We allowed heterogeneity at the level of autonomous community, thus capturing (unobserved) variables not already included in the model which could explain the probability of consuming psychotropic drugs. With the interaction with year, we allowed for this heterogeneity to vary along time because allowing random effects for year is equivalent to including a non-linear trend in the model.
For random effects at the autonomous community level, we assume that they are identical and independent of Gaussian random variables with constant variance.35 36 Random effects for year and interaction are modelled by a random walk of order 1 (ie, independent increments) for the Gaussian random effects vector.37
As the Bayesian estimation provides greater flexibility (a consequence of its hierarchical strategy), we chose to do the analyses using a Bayesian framework. In summary, the initial uncertainty about the effect measures (ie, ORs) and on extent of their variation, was first expressed through prior distributions. Next, we combined prior distributions with the so-called likelihood (ie, the current data), to obtain posterior distribution for the quantities of interest (again, ORs) and then we summarised the posterior distributions by point estimates and credible intervals (analogous to the classical CIs. A small modification in the standard priors (eg, increasing their precision) can imply very different inferences. That is why we need robust priors such as penalising complexity priors, which are invariant to re-parameterisations and always provide the same inferences.38 One of the advantages of Bayesian analyses (with respect to the classical (or frequentist) analyses) is that it is the most suitable for accounting for model uncertainty, both in the parameters and in the specification of the models. Furthermore, only with Bayesian approach is it possible to model variability with relatively sparse data and it is also easier to specify more complex scenarios. Here we followed the integrated nested laplace approximation (INLA) approach,39 within a (pure) Bayesian framework.
The sampling weights (corrected for non-response and improved through ratio and calibration techniques) were used in the population estimations. All analyses are carried out with the free software R,40 available through the INLA library.35 39
Results
Table 1 shows the descriptive characteristics of the two samples (SNHS 2006–2007 and SNHS 2011–2012) according to the consumption of antidepressants and sedatives for the variables of interest (see online supplementary appendix B of the appendices material available online for more in-depth information). In the total sample in SNHS 2006–2007 (49.1% men), 5.8% take antidepressants and 10.7% sedatives. In SNHS 2011–2012 (48.8% men), 4.3% consume antidepressants and 11.1% sedatives.
Descriptive statistics*
Table 2 shows the results of the mixed models of the variables of interest for antidepressants and sedatives. The results from the mixed logistic estimations without any year interactions concerning adult’s mental health are available on request. Also, in this case, the adjusted OR of the year of the survey was not significant for antidepressant consumption or sedative use.
Mixed logistic estimations of the use of antidepressants and sedatives*
Antidepressant consumption
Table 2 shows that the year of the survey (which indicates the period of the economic downturn) is not significant, indicating that the financial crisis did not significantly change the probability of taking antidepressant drugs (OR=0.56, 95% CI 0.18 to 2.53). Using the results in table 2, we compute the OR by considering the interactions of the variables of interest (see figure 1). Then, we observe that, in general, the probability of consuming antidepressants among men and women decreases and is more marked in men, but differs depending on employment status (above all for short-term unemployed). For retired individuals, we find significant differences because, although women’s risk of consuming psychotropic drugs does not change between 2006 and 2011, the risk for men drops dramatically. However, for the student group, risk of consumption reduces equally for both genders and so we cannot observe any differences between them in 2011. In the home maker’s group (although 96.6% are women) this is where the biggest differences between men and women can be found because it is the only group where the risk of consuming antidepressants increases for women but drops sharply for men.
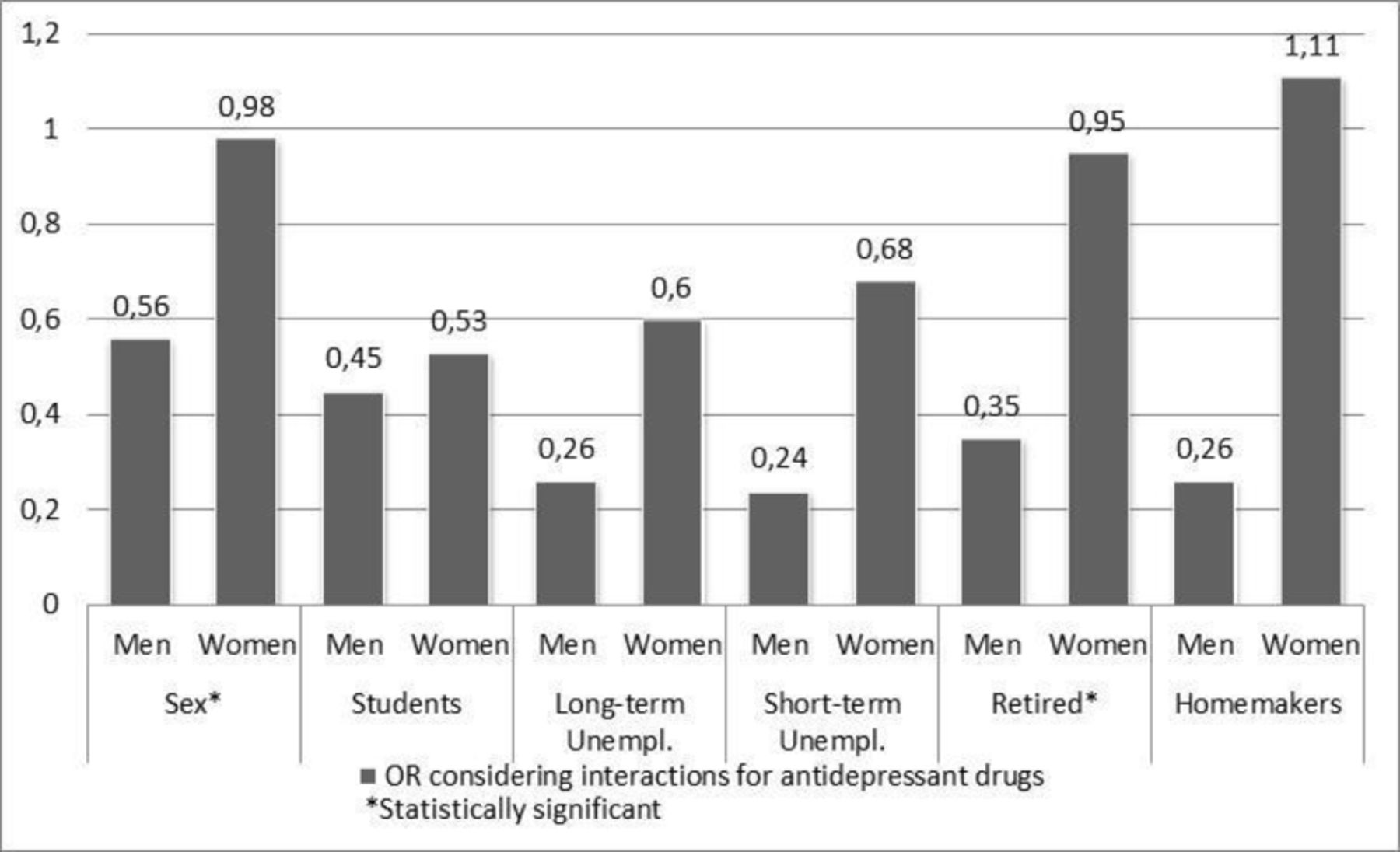
The risk of consuming antidepressant drugs in 2011–2012 compared with 2006–2007.
Sedative consumption
Table 2 shows that the year of the survey is not statistically significant and that the crisis has not significantly changed the likelihood of taking sedatives (OR=1.21, 95% CI 0.26 to 5.49). Using the results in table 2, we compute the OR by considering the interactions of the variables of interest (see figure 2). Again, we observe larger differences between women and men when employment status and 2011–2012 are considered. In the case of individuals in short-term unemployment, both men and women show that between 2006–2007 and 2011–2012 there was an increase in the risk of using sedatives, however, this increase is higher for women than men. Nevertheless, although this group is where we find the biggest increase in the risk for women, it also contains the only status group where there is an increase in risk for men as well. For the long-term unemployed, however, the differences between both groups widen between 2006–2007 and 2011–2012, that is, women increase their risk of using sedatives, whereas men decrease that risk. The trend for retired individuals and home makers is not unlike the long-term unemployed, whereas for students, both groups reduce the risk of consuming sedatives between 2006–2007 and 2011–2012 and no changes are observed in the differences between the two groups in 2011.

{kind=link}
{kind=link}
The risk of consuming sedative drugs in 2011–2012 compared with 2006–2007.
The results from the mixed logistic estimations of the covariates are provided in the appendices material (see online supplementary appendix C).
Discussion
While the current financial crisis has not statistically changed the risk of using psychotropic drugs, our results do indicate that women in situations of long-term unemployment, retirement or home-making, seem to be at greater risk than men of using psychotropic drugs during this financial crisis. Results are adjusted by mental health status, presence of relevant mental health disorders and other health conditions associated with mental health status.
Some possible explanations are that during financial crisis women intensify their work to compensate for the losses in household income41 and their mental health deteriorates. In addition, it has been shown that some of the most serious and common situations created by the crisis in question, such as evictions, affect women’s mental health more than men’s.42 Likewise, women in Spain occupy positions inferior to men in the socio-labour sphere and, furthermore, the crisis has had an impact on the informal sectors of the economy which are occupied mostly by women.43
Cost and financial stress may reduce access to health and pharmaceutical services, as vulnerable populations or those who are financially better off increased the use of psychotropic drugs. Regarding the access to health services, the waiting time is found an important barrier for those who are limited in their daily activities by a chronic physical or mental health problem or disability, and in Spain the waiting time has sharply increased during the financial crisis.44
Like our study, Colell et al,28 did not find significant changes in the sporadic use of hypnotics/sedatives for men or women (regardless of employment status) before and during a financial crisis either, nor did Nicieza-García et al 45 confirm that the rise in psychotropic medication consumption in the region of Asturias was a result of the financial crisis. However, our results differ from other similar studies. For example, in the case of Pérez-Romero et al,46 using SNHS data they establish that for both men and women the use of these drugs increased during the financial crisis. However, they analyse antidepressant and sedative consumption together and only for employees.
To explain the differences found in the literature, it is important to consider that our analysis is the first to treat antidepressants and sedatives separately. While the unexpected decrease in antidepressant use could be because of a misclassification problem or changes in diagnosis and treatment practices, the existing literature can also be misleading because, unlike our study, the two drugs are not treated separately. Furthermore, while our results also show that the financial crisis is not associated with psychotropic drug use, we must consider that we are using data reported by individuals and so our response variables may be influenced by misreporting (or under-reporting) as the result of the stigma47 often associated with mental health issues and substance abuse. Parry et al 48 studied the validity of responses from those using psychotropic drugs and observed that about 29% of males and 18% of females give invalid responses. They attribute the under-reported answers among men (compared with the higher rates of consumption by females, especially in the case of sedatives) to the negative stigma men associate with these drugs.
Our study has some limitations. Even though we use two large samples of individual-level data, we use cross-sectional data which does not allow us to conclude direct relationships between the financial crisis and psychotropic drug use. Besides, even though self-reported measures of health are strongly correlated with mortality,49 there could be a reporting bias affecting individuals’ self-reported responses. Moreover, the (seemingly) marginal effect the financial crisis has had on mental health problems and psychotropic drug use could be explained by a reluctance to respond to (for some) sensitive questions in a personal face-to-face interview.
Sample size (more than 40 000 representative interviews in Spain before and during the financial crisis), is one of the fundamental strengths of this study and provides meaningful results to discern the effects economic recessions have on mental health. Our key contribution is to have identified (using gender and unemployment status) the groups most vulnerable to a financial crisis. Policy-makers must take these groups into consideration (through research efforts, along with healthcare and social interventions) when planning strategies and implementing policy to mitigate health inequities.
Future lines of research could focus on determining the role new medications are currently playing, as their development and rapid spread is quickly displacing the conventional psychotropic drug market.
Acknowledgments
We appreciate the comments of the attendees at the XXXIV Reunión Científica de la Sociedad Española de Epidemiología (SEE) 2016, on September from 14 to 16, 2016, in Sevilla, Spain and at the Third EuHEA PhD student-supervisor and early career researcher conference, from 7 to 9 September 2016, in Barcelona, Spain. We appreciate the comments from four anonymous reviewers, which have undoubtedly helped to improve this work.
References
Footnotes
Patient consent for publication Not required.
Contributors EA had the original idea for the paper. EA, MS and AC-L designed the study. The bibliographical search and the writing of the introduction were by EA, AC-L, CS, GR and LSS. The choice of methods and statistical analysis was performed by MS. EA, CS, LSS, GR and AC-L built the tables and figures. All authors wrote the results and the discussion. The writing and final editing was done by EA, MS, AC-L, AD and CS. All authors reviewed and approved the manuscript.
Funding This work was partly funded by the CIBER of Epidemiology and Public Health (CIBERESP) through the strategic subprogram ‘Crisis and Health’, by the Catalan Government Project, AGAUR, ‘Compositional and Spatial Analysis’ (COSDA), 2014SGR551, and by the University of Girona through the Research Grant to Improve the Scientific Productivity of the Research Groups of the University of Girona 2016-2018 (MPCUdG2016/69). The first author carried out this research with the support of the Short Term Grant Abroad for PhD European, CIBER of Epidemiology and Public Health (CIBERESP), Spain, the support of the Mobility Fellowship among intra-groups of CIBERESP, CIBER of Epidemiology and Public Health (CIBERESP), Spain, and was also beneficiary of the Grant for Pre-doctoral Studies from the University of Girona (BR 4/2013), Girona, Spain.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We used Spanish Health Survey data in all cases. Public and freely accessible at: http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2006.htm and http://www.msssi.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2011.htm (both in Spanish).