Article Text

Abstract
Introduction Flexible intensive care unit (ICU) visiting hours have been proposed as a means to improve patient-centred and family-centred care. However, randomised trials evaluating the effects of flexible family visitation models (FFVMs) are scarce. This study aims to compare the effectiveness and safety of an FFVM versus a restrictive family visitation model (RFVM) on delirium prevention among ICU patients, as well as to analyse its potential effects on family members and ICU professionals.
Methods and analysis A cluster-randomised crossover trial involving adult ICU patients, family members and ICU professionals will be conducted. Forty medical-surgical Brazilian ICUs with RFVMs (<4.5 hours/day) will be randomly assigned to either an RFVM (visits according to local policies) or an FFVM (visitation during 12 consecutive hours per day) group at a 1:1 ratio. After enrolment and follow-up of 25 patients, each ICU will be switched over to the other visitation model, until 25 more patients per site are enrolled and followed. The primary outcome will be the cumulative incidence of delirium among ICU patients, measured twice a day using the Confusion Assessment Method for the ICU. Secondary outcome measures will include daily hazard of delirium, ventilator-free days, any ICU-acquired infections, ICU length of stay and hospital mortality among the patients; symptoms of anxiety and depression and satisfaction among the family members; and prevalence of burnout symptoms among the ICU professionals. Tertiary outcomes will include need for antipsychotic agents and/or mechanical restraints, coma-free days, unplanned loss of invasive devices and ICU-acquired pneumonia, urinary tract infection or bloodstream infection among the patients; self-perception of involvement in patient care among the family members; and satisfaction among the ICU professionals.
Ethics and dissemination The study protocol has been approved by the research ethics committee of all participant institutions. We aim to disseminate the findings through conferences and peer-reviewed journals.
Trial registration NCT02932358.
- delirium
- family
- health personnel
- critical care
- intensive care unit
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The present study is the first large-scale trial aimed to evaluate the effects of different intensive care unit (ICU) visiting policies on relevant outcomes among patients, family members and ICU professionals.
This study is designed as a cluster-randomised crossover trial, which reduces the risk of contamination and improves covariate balance between the two study arms and statistical efficiency.
This study uses strategies to enhance the implementation and evaluation of complex interventions such as some degree of adaptability to local circumstances, a learning period to study interventions and assessment of fidelity and quality of the implementations.
The infeasibility of blinding patients, family members and ICU professionals to the study interventions is a limitation.
The results of this study will allow healthcare professionals, researchers and policymakers to draw conclusions about the efficacy and safety of a flexible family visitation model for delirium prevention in adult ICUs.
Introduction
Adult intensive care unit (ICU) visitation policies vary worldwide; generally, patients admitted to the ICU are only allowed visitors during certain periods of the day.1–3 Congruent with this scenario, most Brazilian ICUs have a restrictive policy of family visits in which visiting hours typically last from 30 min to 1 hour, two to three times a day.4 These restrictive ICU visit policies are rooted mainly in a theoretical increased risk of physiological stress, infectious complications and disorganisation of care.5 However, these theoretical risks have not been consistently confirmed by the scarce literature on this subject,6–9 and flexible ICU visiting hours have been proposed as a means to improve outcomes through patient-centred and family-centred care and delirium prevention.10–12
Evidence from small observational and before-and-after studies suggests that flexible ICU visitation policies are associated with higher satisfaction among patients and patients’ families and with reduction of patient stress.13 14 Accordingly, one pilot randomised trial showed reduction in cardiocirculatory complications among ICU patients admitted during periods of unrestricted visiting hours, possibly due to reduction of anxiety and establishment of a more favourable hormonal profile.6 Moreover, some studies suggest the potential role of presence of family members as a strategy to prevent ICU delirium.15–17 One small prospective single-centre before-and-after study found a reduction of 50% in the cumulative incidence of delirium by changing the visitation policy from a restrictive model (4.5 hours/day) to an extended model (12 hours/day); the length of delirium and ICU stay was also reduced in this study.12 In this regard, the presence of family in the critical care setting is suggested as a means to achieve better pain control, reduce the use of sedatives and participate in the reorientation and cognitive stimulation of patients. These benefits have been associated with lower incidence of delirium in studies evaluating multicomponent non-pharmacological interventions to prevent delirium and constitute the rationale for the F (Family Engagement and Empowerment) component of the ABCDEF bundle, an evidence-based approach to prevent delirium.18–21
Regarding possible risks associated with flexible ICU visit policies, some studies have shown that ICU professionals sometimes perceive visits as a source of increased workload and disorganisation in patient care, instead of considering families as ‘one’ with the patient and as potential sources of reassurance and comfort.22 23 In a single-centre study,23 59% of ICU staff members stated that the open visitation policy impaired the organisation of patient care, and 72% believed that their work suffered more interruptions due to the extended presence of families in the ICU. Congruent with these data, one before-and-after study with nine ICUs8 showed a significant increase in burnout levels among ICU professionals after a partial liberalisation of visiting policies. The impact of educational strategies directed to ICU visitors in the context of flexible family visitation policies to prevent disorganisation of patient care and burnout among ICU professionals is not known. In relation to the risk of infection, this topic has been evaluated by few underpowered studies.7 12 15 Although one study15 showed greater environmental microbial contamination during an open policy of ICU visitation, published studies7 12 15 failed to show an association between flexible ICU visiting hours and nosocomial infection. Lastly, the impact of flexible ICU visiting hours on symptoms of anxiety and depression of family members is not well studied: there is plausibility for decreased anxiety and depression with flexible ICU visiting hours as a result of improved access to information and more effective sharing of the decision-making process24; conversely, it is also plausible to assume that anxiety and depression will increase as a result of higher exposure of family members to complex situations such as terminality and the patient’s emotional and physical suffering.25 26
The implementation of a flexible family ICU visitation policy, although promising due to its low cost and potential to improve quality of care, is a complex organisational process, given that multiple populations involved in this context may be affected by the intervention in different ways. Additionally, most evidence regarding this intervention is originated from underpowered observational and before-and-after studies. Specifically, no large-scale randomised trial so far has evaluated the potential impact of different ICU visitation models on patient, family and ICU staff outcomes. We hypothesise that compared with the restrictive family visitation model (RFVM), a flexible family visitation model (FFVM) supported by visitor education will reduce the cumulative incidence of delirium among adult ICU patients, reduce symptoms of anxiety and depression and increase satisfaction with care among family members without increasing burnout levels among ICU professionals.
Objectives
Primary objective
The aim of the present study is to assess if an FFVM, compared with an RFVM, can prevent delirium in adult ICU patients.
Secondary objectives
Our secondary objective is to compare the efficacy and safety of both ICU visitation models with regard to three sets of variables: ICU/patient-related variables (daily hazard of delirium, ventilator-free days, ICU-acquired infections, ICU length of stay, all-cause hospital mortality, need for antipsychotic use, coma-free days, need for mechanical restraints and unplanned loss of invasive devices), family-related variables (symptoms of anxiety and depression, satisfaction and self-perception of involvement in patient care) and ICU staff variables (prevalence of symptoms of burnout syndrome and satisfaction).
Methods
The present study protocol follows the Standard Protocol Items: Recommendations for Interventional Trials statement recommendations.27 The items from the WHO trial registration data set are described in online supplementary file 1. This study protocol was registered at Clinicaltrials.gov before the randomisation of the first cluster (NCT02932358) .
Supplementary file 1
Study design
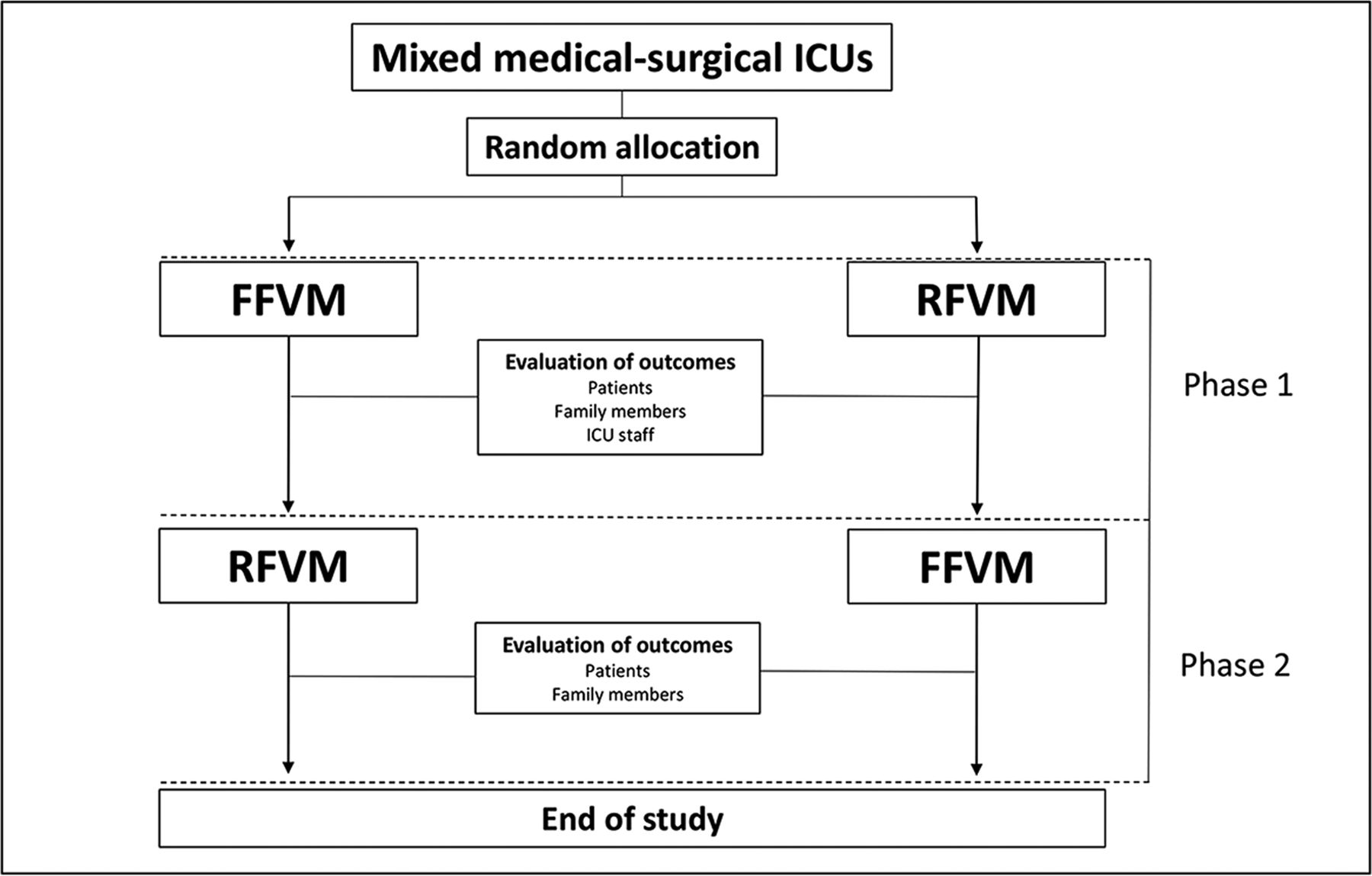
The present study was designed to be a cluster-randomised, crossover trial involving mixed medical-surgical ICUs. In this study, the unit of randomisation is the ICU, since the proposed intervention involves components at the organisational level and is intended to be implemented in the whole ICU and not for selected patients. All ICUs will receive both FFVM and RFVM, and the randomisation will determine in which order the visitation models will be evaluated in each ICU (figure 1). The initial intervention (phase 1) will involve ICU randomisation to either an FFVM or an RFVM. In phase 2, each ICU will be crossed over to the other visitation model. The study analysis will be performed at the subject level according to the intention-to-treat principle and accounts for the cluster-randomised crossover design.

Study design. During the study, the ICU intervention (FFVM or RFVM) will be applied to all admitted patients apart of meeting inclusion criteria for the study. The length of study phases in each ICU will be determined by the patient recruitment rate (25 patients in phase 1 and 25 patients in phase 2). Patients and family members will be recruited during phases 1 and 2. ICU professionals will be evaluated and followed up only during the phase 1. Following the recruitment of the 25th patient, during phase 1, a 30-day period without subject recruitment will occur to allow appropriate conclusion of the follow-up of all recruited patients for the study outcomes and to avoid contamination of the two study arms. FFVM, flexible family visitation model; ICUs, intensive care units; RFVM, restrictive family visitation model.
Participants
Cluster eligibility, recruitment and exclusion criteria
Brazilian adult ICUs of public and philanthropic hospitals will be invited to participate in the trial. Mixed medical-surgical ICUs with at least six beds and a restrictive policy of family visitation (<4.5 hours/day) are considered eligible. ICUs with structural or organisational impediments to flexible family visitation, according to the Brazilian resolution of minimal operational requirements for ICUs,28 will be excluded.
Patient eligibility, recruitment and exclusion criteria
Consecutive patients aged ≥18 years admitted to the ICU during phases 1 and 2 will be enrolled in each cluster. Subjects in a coma (Richmond Agitation Sedation Scale (RASS)29 −4 or −5) lasting >96 hours from the moment of first evaluation for recruitment and those with delirium at baseline (positive Confusion Assessment Method for ICU (CAM-ICU)30) will be excluded. The following exclusion criteria will also be applied: cerebral death, aphasia, severe hearing deficit, predicted ICU length of stay <48 hours, exclusive palliative treatment at ICU admission, unavailability of a family member to participate in the flexible family visits, unlikelihood to survive >24 hours, prisoner status and, lastly, readmission to the ICU after enrolment in the study.
Family member eligibility, recruitment and exclusion criteria
The sample of family members will include one family member per patient enrolled into the study, with the closest family member being selected. Family members who do not speak Portuguese or have serious impediment in answering the self-applied questionnaires (eg, illiteracy or severe visual or hearing limitations) will be excluded.
ICU professionals’ eligibility, recruitment and exclusion criteria
All bedside ICU professionals (physicians, nurses, nursing technicians and physiotherapists) of each cluster who assist patients during the daytime for at least 20 hours per week will be enrolled. ICU professionals who have a planned leave of absence of >15 days during phase 1 will be excluded.
Interventions
The proposed study interventions may be classified as complex because31: (A) there is a large number of interacting components within the experimental and control interventions (eg, changes in ICU processes, education of family members and engagement and training of the ICU multidisciplinary team); (B) there are several groups targeted by the intervention (ICU patients, family members and ICU professionals); (C) there is a large number and high variability of outcomes (evaluation of different outcome domains in three different target populations); (D) a limited degree of flexibility in the intervention is allowed (educational components may be tailored considering the educational level of the target population, visit hours may be customised according to internal processes of the ICU and expected acceptability of the target population).
We tested the feasibility and acceptability of implementation of the intervention in a single-centre before-and-after study.12 Table 1 shows the components to be implemented during FFVM and RFVM. During both FFVM and RFVM, all visitors will be required to perform hand hygiene by washing their hands with antiseptic soap or using alcohol-based hand-rub formulations and to wear disposable vests and/or personal protective equipment when appropriate (eg, contact or droplet precautions). All visitors will receive oral and written guidance about the minimum requirements to promote a safe and restful environment to ICU patients. The visitors will be asked to leave the room during some procedures such as intubation, central venous or urinary catheterisation, bronchoscopy, electrical cardioversion and cardiopulmonary resuscitation. As an exception, some patients, during both study interventions, will be allowed to receive visits longer than the maximum limit of visiting hours. This decision will be allowed in the following situations: patient age ≥65 years, terminal illness and conflicts among patients or family and ICU staff.
Components of study interventions
Flexible family visitation model
In the FFVM, two or fewer close family members will be allowed to visit the patient for up to 12 consecutive hours each day. Family members who agree to join the family visits will have to attend a structured meeting at the ICU in which they will receive guidance about the ICU environment, common ICU treatments, rehabilitation and basic infection control practices, multidisciplinary work at the ICU and information on palliative care and delirium prevention. Additionally, family members will receive an information brochure and be encouraged to access a website (www.utivisitas.com.br), both of which are designed to explain, in simple terms, what happens during and after an ICU stay to legitimise emotions and improve cooperation with relatives without increasing the ICU staff workload. In addition to family visitation, patients in the FFVM will be allowed to receive social visits at specific time intervals (according to the local ICU policies). Social visits will be offered to patient’s friends or other family members who did not qualify for family visitation. The number and duration of social visits will be determined by the patient or proxies. Social visitors will not be required to attend the structured meeting.
Restrictive family visitation model
In the RFVM, patients will be allowed visitors according to routine ICU practices but limited to the maximum of 4.5 hour of visitation per day. Visitors will not be required to attend the structured meeting, because this is the standard of care in Brazil. The length of ICU visiting hours will be similar to that of social visits in the FFVM. The number and duration of visits will be determined by the patient or proxies taking into the account the limits of visiting hours dictated by local policies.
Randomisation
The randomisation unit is the ICU. In hospitals where there is more than one ICU, each ICU will be considered a distinct randomisation units as long as the ICU staff are different. If the staff are the same, all ICUs in the hospital will be considered a single unit of randomisation. The allocation of the initial intervention (ie, FFVM or RFVM) will be performed through blocks of different sizes and stratified by number of ICU beds. A randomisation list will be generated, and ICUs will be consecutively randomised as per the date of approval by the local research ethics committee. In order to guarantee allocation concealment, a statistician will receive an identification code for each unit but will remain blinded to the identity of the ICU. The statistician will then inform the allocation for each unit identification code to the research coordinator. Lastly, the research coordinator will inform the ICUs regarding the group to which they were initially allocated.
Blinding
It is not feasible to blind the researchers, patients, family members or ICU professionals to the study interventions.
Outcomes
Primary outcome
The primary outcome is the cumulative incidence of delirium during the ICU stay. Diagnosis of delirium will be made using the validated Brazilian translation of the CAM-ICU,32 which will be applied at least once per 12 hours shift in patients with RASS ≥−3, by trained ICU professionals. The cumulative incidence of delirium is defined as the presence of delirium (at least one positive CAM-ICU) on at least one 12-hour shift during the ICU stay. Before study initiation, all professionals responsible for CAM-ICU assessment will receive training concerning the CAM-ICU. This specific training will be given both during investigator meetings and on-site. Furthermore, inter-rater reliability measurements of the CAM-ICU and RASS will be performed before study initiation to evaluate the quality of assessments and, if necessary, additional training will be provided. A sensitivity analysis of the primary outcome adjusted for the baseline risk of developing delirium determined by the PREdiction of DELIRium in ICU patients (PRE-DELIRIC) score33 will be conducted to check the consistency of the results. There will be three a priori defined subgroup analyses for the primary endpoint: (1) effectiveness of FFVM versus RFVM in ICUs according to the PRE-DELIRIC score (patients with a predicted risk <25%, 25%–50%, 50%–75% and >75%); (2) effectiveness of FFVM versus RFVM in ICUs according to patient group (medical vs surgical, and neurocritical vs non-neurocritical); and (3) effectiveness of FFVM versus RFVM in ICUs according to Acute Physiology and Chronic Health Evaluation II (APACHE-II) scores (≤15 vs >15 points). Additional exploratory subgroup analysis will be performed based on the level of patient’s exposure to sedation, ICU professional’s workload and proportion of private ICU beds.
Secondary outcomes
Secondary outcome measures include daily hazard of delirium, ventilator-free days, any ICU-acquired infections (pneumonia or urinary tract infection or bloodstream infection according to Centers for Disease Control and Prevention guidelines34–36), ICU length of stay and all-cause hospital mortality among patients; symptoms of anxiety and depression measured by the Hospital Anxiety and Depression Scale (HADS)37 and satisfaction measured by the Critical Care Family Needs Inventory (CCFNI)38 among family members; and prevalence of symptoms of burnout syndrome measured by the Maslach Burnout Inventory (MBI)39 among ICU professionals. The daily hazard of delirium will be evaluated using a joint modelling approach,40 which is recommended to account for days at risk for delirium (ie, ICU days in a non-comatose state).
All cases of ICU-acquired infections will be adjudicated by an infectious disease physician blinded to the study interventions. Family members and ICU professionals will be evaluated through self-administered questionnaires.
Tertiary outcomes
Tertiary outcomes will include need for antipsychotic agents and/or mechanical restraints, coma-free days, unplanned loss of invasive devices and ICU-acquired pneumonia, urinary tract infection or bloodstream infection among ICU patients; self-perception of involvement in patient care (ie, reorientation activities, pain control, mobilisation, feeding, comfort, emotional support and communication (helping patients to interpret ICU staff orientations and ICU professionals to understand patient needs)) among family members; and satisfaction among ICU workers.
Length of ICU intervention, participant recruitment and timeline, data collection, management and monitoring
The length of study phases will be determined by the patient recruitment rate. During phase 1, 25 patients per ICU will be enrolled. After enrolment of the 25th patient, a 30-day period without subject recruitment (ie, washout period) will occur to allow appropriate conclusion of the follow-up of all recruited patients for the study outcomes and to avoid contamination of the two study arms. After this period, each ICU will be crossed over to the other visitation model (phase 2), with enrolment of an additional 25 ICU patients per ICU.
The study flow diagram is shown in figure 2, and the schedule of enrolment, interventions and assessments is shown in online supplementary file 2. Patients and family members will be recruited during phases 1 and 2. ICU professionals will be evaluated and followed up only during the phase 1 in order to avoid the carryover effect. Patients will be followed up from study enrolment to hospital discharge or death, or a maximum of 30 days. Family members will be evaluated at two time points: within the first 48 hours of patient inclusion into the study (for baseline data) and within 7 days from patient discharge from ICU or death, or a maximum of 30 days (for outcomes assessment). ICU professionals will be evaluated at two time points: 2 weeks before initiation of the first randomised ICU intervention (for baseline data) and during phase 1 (for outcome assessment).
Supplementary file 2

Study flow diagram. FFVM, flexible family visitation model; ICUs, intensive care units; ITT, intention-to-treat; RFVM, restrictive family visitation model.
Trained research personnel at the local sites will prospectively collect data on printed case report forms that will be entered into an electronic data capture system (REDCap, Vanderbilt University, Tennessee, USA).41 In order to allow intention-to-treat analyses, data will be collected and analysed independent of adherence to study interventions. We will deploy the following procedures to enhance the implementation of study interventions and ensure data quality:
All local principal investigators and subinvestigators will attend an on-site training session before the beginning of the study to standardise procedures including data collection.
All ICUs will have a learning period within the first 15 days of phases 1 and 2. During this period, ICUs will receive the intervention (FFVM or RFVM) but will not recruit subjects. Local investigators will use this period to adapt the ICU staff to the organisational aspects of study intervention, including rules about visiting hours (for both FFVM and RFVM periods), guidance to visitors about the minimum requirements to promote a safe and restful environment to ICU patients (for both FFVM and RFVM periods), role of ICU professionals during family visiting hours (for FFVM period) and conduction of family members-directed structured meetings (for FFVM period). Furthermore, local investigators will use this period to test the study measurements (CAM-ICU, HADS, CCFNI and MBI) and address concerns regarding case report filling.
The investigators will be able to contact the coordinating centre to solve any potential issues or problems.
Data cleaning will be applied continuously to identify inconsistencies and missing data. The centres will be notified of any inconsistencies and missing data and prompted to solve them.
The coordinating centre will review detailed reports on screening, inclusion, follow-up and data consistency and completeness on a weekly basis. The coordinating centre will take immediate action to solve any problems.
Centres will be monitored throughout the study. On-site monitoring visits will occur during phases 1 and 2. A trained professional appointed by the coordinating centre will perform the monitoring visit. During the monitoring visits, all information will be considered strictly confidential.
To assess the fidelity and quality of the proposed interventions, we will perform on-site monitoring visits, with a standardised checklist, in order to evaluate if the processes are consistent with the intended intervention or if there are important deviation from the proposed protocol; perception of effectiveness and barriers for implementation will be assessed qualitatively, through semistructured interviews with healthcare professionals involved in the study.42 In addition, we will collect data related to the length of visits for included patients, study website access and family members characteristics. A data monitoring committee is not required as the risk of study interventions causing significant harms is low.
Sample size and sampling
A minimum of 33 ICUs with recruitment rate of 50 patients per ICU (25 patients per study phase) will be needed (total of 1650 patients) to detect an absolute difference >6.0% in the cumulative incidence of delirium between the two study arms (considering an outcome incidence rate of 20.5% in the RFVM), with 80% power, and two-tailed 0.05 alfa. Two levels of intraclass correlation coefficient (ICC) were considered to calculate the sample size: 0.05 for subjects in the same cluster/time period and 0.01 for subjects in the same cluster/different time periods. Estimates of sample size for the primary outcome were made on the basis of the cumulative incidence of delirium found in a single centre before-and-after study that evaluated the effect of different policies of family visitation on the incidence of delirium.12 In order to compensate for potential ICU and patient losses, the present study plans to recruit 40 ICUs.
Statistical analysis
A detailed statistical analysis plan will be prepared before data analysis and is intended to be published or made available online. All analyses will be conducted with the intention-to-treat principle. The comparison of cumulative incidence of delirium will be performed using models for correlated data considering the ICU as a cluster and presented as risk ratios and 95% CIs. The same models will be used for analysis of secondary and tertiary outcomes, that is, considering the ICU as a cluster and each outcome with its adequate probability distribution. A statistical significance level of 0.05 will be adopted for all statistical comparisons. The R-Development Core Team will be used for analysis.
Discussion and trial status
Flexible ICU visiting policy is a complex intervention, with multiple components, targeting different populations with specific outcomes. Figure 3 describes the logic model for the FFVM. Although several outcomes are expected to have a positive impact, we chose incidence of delirium as primary outcome because it combines a strong potential for causal and direct association and an important clinical impact. Delirium is a highly prevalent ICU complication and is associated with increased mortality, longer ICU and hospital stay, higher cost of care and long-term cognitive impairment.43–45 Therefore, identifying interventions that may reduce the risk and burden of delirium in ICU patients is of paramount importance to improve healthcare quality. Other important outcomes, such as ICU-acquired infections and length of stay, levels of burnout among ICU professionals and symptoms of anxiety and depression and satisfaction among family members may have both a direct and indirect relation with the proposed intervention and, therefore, may represent important markers of effectiveness and safety of the proposed intervention. An FFVM rooted in education of family members may reduce the theoretical risk of increase in ICU staff workload, disorganisation of care and ICU-acquired infections. The higher access to information may have a positive effect on family members’ satisfaction and interactions with the patients and ICU professionals. Moreover, an FFVM may result in shorter ICU stay, mediated, for instance, by a lower incidence of delirium; additionally, a better understanding of the condition by the family may avoid delays in ICU discharge.

Logic model for flexible ICU visiting hours. FFVM, flexible family visitation model; ICUs, intensive care units; MDR, multidrug-resistant; PTSD, posttraumatic stress disorder; RFVM, restrictive family visitation model.
To the best of our knowledge, this will be the first large-scale, multicentre randomised trial evaluating the effects of different policies of ICU visitation on patients, family members and ICU professionals. Results of this study will allow healthcare professionals, researchers and police makers to draw conclusions about the efficacy and safety of a FFVM in adult ICUs.
Our study has some limitations. First, high variability across institutions is expected; although the chosen ICCs may be considered conservative, there are no estimates in the literature for the proposed intervention, which may result in lack of power if the actual ICC is larger than the estimate. Also, no masking of outcome assessors may result in measurement bias for delirium specially with the use of an instrument with some degree of subjectivity46; although blinding is not feasible for the proposed intervention, in order to minimise risk of bias, we chose validated methods for delirium evaluation and will make efforts in order to standardise data collection through continuing education of outcome evaluators. As the number of patients is small for each cluster, the estimate time for data collection for each study phase is from 2 months to 3 months; this length of time may not be enough to properly assess burnout in healthcare professionals. Finally, our trial is not designed to evaluate long-term outcomes, such as posttraumatic stress disorder in patients and family members, as well as microbiological changes in ICU flora due to a higher circulation of individuals from the community. These issues should be assessed in future studies.
The study design and protocol were finalised in March 2016. All site investigators were required to participate in at least one of two investigator meetings (November 2016 and April 2017). Currently, this study is recruiting subjects in 34 ICUs representative of the Brazilian geopolitical territory (figure 4). Another six ICUs are in the process of preparation for study initiation. We expect that this study will be completed in June 2018.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Geographical distribution of participating intensive care units.
Ethics and dissemination
Ethics approval and consent to participate
The research ethics committees of all participant institutions approved the study protocol (online supplementary file 3). The need for patients’ written informed consent was waived in 37 of 40 participating ICUs, because the standard of care encompasses both study interventions. In 3 of 40 ICUs informed, consent will be required for patients or proxies. Informed consent will be required for family members and ICU professionals in all ICUs. Site investigators will be responsible for obtaining informed consent from study participants. Subject confidentiality will be assured through data anonymisation and controlled access to case report forms, electronic data capture system and datasets. Any breaches of confidentiality, study protocol or adverse events attributable to this study will be reported to the above research ethics committees.
Supplementary file 3
Dissemination
We hope to make the study findings widely available and plan to disseminate our results in international conferences and peer-reviewed journals. Authors and collaborators will be involved in reviewing drafts of the manuscripts, press releases and any other publication format arising from this study.
Acknowledgments
The authors would like to thank the data collection team of each participating ICU, as well as the Hospital Moinhos de Vento, the Brazilian Ministry of Health, and the Brazilian Research in Intensive Care Network for their support in conducting the study.
References
Footnotes
Contributors RGR, CT and DBdS developed the main study intervention (FFVM). RGR, CT and MF developed the original concept of this study. RGR, MF, NB, ABC, FB, LCPA, FRM, JIFS, JASP, RBM and CT contributed to study design. RGR, LGdL and CT wrote the first draft of the paper, and MF, NB, ABC, FB, LCPA, FRM, JIFS, JASP, RBM, CCR, RK, RMdM, MMSS, DS, NEG, CE, TR, TH, AA, JMMT, MGB, DCB, IdLF, VN, HMV, LCeC, PADD, RT, SLSB and AG revised the first draft. The final manuscript was reviewed by all the authors. All authors read and approved the final manuscript.
Funding The present study was funded by the Brazilian Ministry of Health through the Program of Institutional Development of the Brazilian Unified Health System (PROADI-SUS).
Competing interests None declared.
Patient consent Not required.
Ethics approval This study will be conducted according to the resolution no 466/12 of the Brazilian National Health Council (http://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html). The study protocol has been approved by the Research Ethics Committee of the coordinating site (approval number: CAAE 57717516.3.1001.5330) and the research ethics committees of all participant institutions (online supplementary file 3).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Hospital de Urgência e Emergência de Rio Branco (AC): Gigliane Maria Angelim de Albuquerque, Márcia Odília Marçal Vasconcelos and Edna Lopes Monteiro. Hospital Geral do Estado (AL): Vania Peixoto Ticianeli and Lucia Regina Arana Leite. Fundação Hospital Adriano Jorge (AM): Ivaneide Teixeira Barbosa, Henri Horstmann, Eliane Aparecida Peixoto Paulo and Enio Barreto. Hospital Geral Clériston Andrade (BA): Paulo Henrique Panelli Ferreira, Lúcio Couto de Oliveira Júnior, Daniela Cunha de Oliveira, Katia Santana Freitas and Eduardo da Silva Oliveira. Incardio – Santa Casa de Misericórdia de Feira de Santana (BA): Patrick Sampaio, Deise Freitas Casaes, Rosa Maria Rios Santana Cordeiro, André Raimundo Franca Guimarães and Ananda Catharina Azevedo Silva. Hospital Estadual de Urgência e Emergência do Espírito Santo (ES): Jander Fornaciari Pissinate, Lucas da Silva Lima, Letícia Sales Araújo, Albano Siqueira Muniz, Wallace Kadratz Klemz, Layla Cavallieri das Neves, Ana Cláudia Freitas Ferraz, Lucas Dornelas Freitas Machado e Silva, Leandro de Oliveira Ferreira and Ivens Guimarães Soares. Hospital de Urgências de Goiânia (GO): Ana Paula Menezes, Marco Antônio Castilho, Durval Pedroso, Janaynna Silva, Lilian Siqueira Costa Correia Pádua, Marco Antônio Castilho, Aline Dias Martins, Julia de Paula Oliveira, Rosangela Fernandes de Oliveira and Luciana Mendonça Carvalho. Hospital das Clínicas da Universidade Federal de Minas Gerais (MG): Christiane de Freitas Mourão Helt Mantuano Pereira, Ronan de Souza and Ana Carolina de Oliveira Paiva. Santa Casa de Misericórdia de São João Del Rei (MG): Jorge Luiz da Rocha Paranhos, Adilson de Carvalho Meireles, Iany Grinésia da Silva and Leonardo José de Oliveira Santos. Hospital Metropolitano de Urgência e Emergência de Ananindeua (PA): Norma Assunção, Viviane Ferreira Paes Monteiro, Giselle Cesar da Silva and Rafaella Ferreira. Hospital Regional do Baixo Amazonas (PA): Marli Sarmento da Silva, Denis Vasconcelos, Renê Augusto Gonçalves e Silva and Antonio Carlos Alves Siva. Hospital Alberto Urquiza Wanderley (PB): Ciro Leite Mendes, Sérgio Luz and Erick Albuquerque. Hospital Universitário Alcides Carneiro (PB): Amanda Manuella Dantas Nobre, Elzilene Costa Araujo Germano, Mayra Ferreira Nascimento, Cybele Cristina Cavalcante Lucena and André Luiz Diniz Costa. Hospital Universitário Lauro Wanderley (PB): Lucrecia Maria Bezerra, Igor Mendonça do Nascimento, Adriana Coutinho Leite, Marcia Abath Aires de Barros and Maria José de Vasconcelos. Hospital Agamenon Magalhães (PE): Marcos Gallindo, Alexandre Roque da Silva, Claudia Raquel Alcantara Manzi and Deyse Queiroz Nogueira. Hospital Universitário da Universidade Federal do Vale do São Francisco (PE): Kátia Regina de Oliveira, Saulo Bezerra Xavier, Rosivania Castro Figueiredo Ribeiro and Ademir Jose de Vlieger Junior. Hospital Universitário da Universidade Federal do Piauí (PI): Rejane Martins Prestes, Danyelle Alves Vieira, Laís Sousa Santos, Francisco Eduardo Viana Brito, Murilo Moura Lima and Elisana Andreia Ferreira Moura. Hospital do Câncer de Cascavel (PR): Raysa Cristina Schmidt and Delmiro Becker. Hospital Universitário do Oeste do Paraná (PR): Lizandra Oliveira Ayres, Gisele Yumi Hoshino and Amaury Cezar Jorge. Hospital Geral de Nova Iguaçu (RJ): Alexander Oliveira Sodré, Tennyson Pereira de Oliveira, Letícia Alves Pereira Entrago, Thiago Matos Barcellos, Cid Leite Vilela and Osvaldo Marques Barros da Silva. Hospital Deoclécio Marques de Lucena (RN): Alessandro da Silva Dantas, José André de Anchieta Monteiro, Pollyanna Iracema Peixoto Gouveia Gomes de Brito, Patrícia Manuella Melo de Oliveira Magalhães and Cleide Medeiros da Silva. Fundação Saúde Pública São Camilo de Esteio (RS): Luciana Caccavo Miguel, Carolina Karnopp, Patrícia Bonatto and Elisabeth Borba da Rosa. Hospital Ana Nery (RS): William Rutzen, Ricardo da Silveira Bastos and Clébio Barreto Teixeira. Hospital Conceição (RS): Wagner Luis Nedel, William Victor Lissa Dalprá, Raquel Lazzari, Andreia Specht and Carla Silva Lincho. Hospital da Cidade de Passo Fundo (RS): Janaína Pilau, Priscila Tonial Foscarini, Juliane Disegna Fraporti and Elsa Zanette Tallamini. Hospital de Clínicas de Porto Alegre (RS): Amanda Andrade Forni, Paula Jordana Pereira dos Santos, Aloma Luz da Silva, Giovana Getelina Ferreira, Maria Renata Pereira dos Santos, Ana Paula Melo Carvalho, Thais Dos Santos Donato Schmitz and Rita Gigliola Gomes Prieb. Hospital Don Vicente Scherer (RS): Edison Moraes Rodrigues Filho, Alexandre Formighieri de Mello, Raquel Hohenreuther and Ruth Susin. Hospital Mãe de Deus (RS): Andrea Beck, Eduarda Cristina Martins, Fabrícia Cristina Hoff, Lilian da Fe Silveira, Adriana Oliveira Prestes, Hígia Pires Pizzato, Fábio Rosa and Rafael Cremonese. Hospital Montenegro (RS): Moreno Calcagnotto dos Santos, Ana Flávia Gallas Leivas, José Pettine and Lourenço Dobrinsky. Hospital Santa Cruz (RS): Rafael Botelho Foernges, Andreia Schubert de Carvalho, Roberto Ritter de Souza and Vanessa Cardoso. Hospital Santa Rita (RS): Andre Peretti Torelly, Martha Hadrich and Gabriele Lobato Marins. Hospital São Lucas da PUCRS (RS): Sérgio Baldisserotto, Brenda Santos, Fernanda Bettega, Guilherme Barcellos and Catia Daiane Souza Silveira. Hospital Tacchini (RS): Carla Flores, Juliana Giacomazzi, Samanta da Costa and Danieli Madruga de Souza. Pavilhão Pereira Filho (RS): Elisiane Gouveia da Silva, Luana Oliveira da Silva, Clarisa Vargas Xis and Taiani Vargas. Hospital Dona Helena (SC): Milton Caldeira Filho, Fabiana Efting Mohr, Kethe de Oliveira Souza, Raquel Souza de Aguiar and Micheli Coral Arruda. Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto (SP): Wilson Jose Lovato, Julia Batista de Carvalho, Maria Aline Sprioli, Rodrigo Barbosa Cerantola, Tânia Mara Gomes and Janaína de Oliveira Perez. Hospital do Coração (SP): Vinícius Avellar Werneck, Rosianne de Vasconcelos, Rafael Trevizoli Neves and Danielle Penha Dassi.