Article Text

Abstract
Introduction Atrial fibrillation (AF) affects >6% of people aged 65 years or older. Left undetected and untreated, patients may develop significant cardiovascular complications and have a fivefold increased risk of suffering a stroke. For 40% of all sufferers, AF can be asymptomatic. Every year in the UK, £2.2 billion is spent on AF-related strokes, so there is an urgent need to improve early detection of AF. This study aims to determine the feasibility of using trained clinical pharmacists based in general practices, to screen for AF, using pulse palpation and a single-lead ECG device on participants aged 65 years or older, attending influenza vaccination clinics.
Methods and analysis Seven clinical pharmacists will be trained by a cardiologist to pulse palpate and record single-lead ECGs using the AliveCor Kardia Mobile device. Quantitative analysis will assess the accuracy and ability of the clinical pharmacist to identify pulse irregularities using pulse palpation and to record and interpret a single-lead ECG. The level of agreement of pulse irregularities detected by pulse palpation will be compared with those detected by the single-lead ECG device, as will the level of agreement between the cardiologist and the device’s interpretation of the ECG. The proportion of people identified with AF (confirmed by the cardiologist) will be determined. Additional demographic data will be obtained from all participants through a questionnaire. Qualitative data will be captured from the participants, from the clinical pharmacists and from the general practitioners and practice staff to determine their views on this method of AF screening. We aim to recruit 600 participants across general practices within Kent.
Ethics and dissemination This protocol was approved by the London–Riverside Research Ethics committee. The findings of this study will be disseminated through forums including, but not limited to, peer-reviewed journals, national and international conferences.
- cardiology
- stroke
- stroke medicine
- preventive medicine
- public health
- healthy policy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a single time-point screening study that combines with the influenza vaccination clinics, to target a relevant at-risk proportion of the population (over 65 years), with an interest in their own personal well-being.
The screening strategy is likely to be convenient for patients and cost-effective when used in combination with current healthcare infrastructure and other patient services, such as the influenza vaccination clinics.
The sample size of 600 will allow us to evaluate the proficiency and accuracy of the clinical pharmacist to screen patients for AF. It will also inform the design of any future large-scale screening studies.
Screening in combination with the influenza vaccination season could prove disruptive to the clinics and recruiting patients on the day could be suboptimal.
Introduction
Atrial fibrillation (AF) is the most common sustained cardiac rhythm disorder and represents an urgent and significant global health challenge.1 AF is an age-related condition which affects ~6% of people over the age of 65 years, with an estimated >33 million people thought to be suffering with this condition globally.2 3 In the UK, AF affects ~2.5% of the population and >10% of people aged >80 years.4 5 The lifetime risk of developing AF is 1 in 4 for those >40 years compared with 1 in 8 for breast cancer in age-matched women.6 7
AF occurs when structural and/or electrophysiological abnormalities alter atrial tissue to promote abnormal pulse formation and/or propagation. The consequence of this is inefficient blood flow through the heart, resulting in an increased risk of clot formation. AF is frequently associated with other pathophysiological conditions, including, for example, hypertension, heart failure, obesity, diabetes, renal failure and stroke.8–10 Untreated AF is associated with significant cardiovascular complications, a fivefold increased risk of stroke and a twofold risk of dementia (figure 1).11 12 Cardioembolic strokes arising from AF are often fatal (19%, 28-day mortality rate) and survivors have a 50% risk of severe disability.13 14 In the UK, approximately 20 000 strokes occur as a result of AF each year.15 Strikingly, AF is often asymptomatic, with 40% of AF sufferers unaware of their condition and 25% of these asymptomatic patients present with stroke as their first symptom.16 17 In Kent, Surrey and Sussex, an observed prevalence of AF of 2.02% suggests that >65 000 people are living with undiagnosed AF across the region.18

A summary of key reasons underlying the need for pilot clinical studies to support the development of the national atrial fibrillation screening programme in the UK led by general practice-based clinical pharmacists.
The associated cost of AF-related strokes is significant. £2.2 billion is spent each year in the UK, corresponding to ~1% of the National Health Service (NHS) budget.19 The costs can be expected to escalate further. The incidence of AF has doubled since the last decade and is predicted to double again over the next 30 years.3 20–22 Early detection of AF and treatment with oral anticoagulants has been shown to significantly reduce the risk of stroke from an incidence of 3.9% to 1.3% and of death from 7.2% to 4.2%.23 Stroke avoidance through appropriate detection and treatment would save the NHS ~£147 million a year.24 It has been proposed that in many cases a simple pulse check may be sufficient to detect AF.25 Despite evidence to show that appropriate oral anticoagulation significantly reduces the risk of stroke in patients with AF, 27% of these patients do not receive any treatment.26 Despite AF fulfilling all of the criteria, listed by the WHO, necessary to justify mass screening,27 28 there is still no international screening programme for AF.
A growing medical consensus backed by public health policy, agrees there is an urgent need to improve AF diagnosis before the first complications occur.29–31 Guidelines and initiatives directed at primary and secondary care (eg, European Society of Cardiology, National Institute for Health and Care Excellence (NICE) and Primary Care Atrial Fibrillation) have fallen short of the expected outcomes of early detection of AF, such as to reduce AF-related strokes.32–34 Interestingly, numerous opportunistic case findings of AF in patients in primary care (often alongside other screening initiatives for hypertension, diabetes and enhanced care services) and by various healthcare professionals (HCPs) have been reported.35–43 In response to this, clinicians and policy-makers are now exploring primary care as an appropriate setting for improved AF diagnosis. This is likely to be convenient for patients and cost-effective if used in combination with current healthcare infrastructure and other patient services such as influenza vaccination clinics.5 44 In Medway and Kent, >65% of the people aged 65 years or older attend influenza vaccination clinics.45
The NHS Five Year Forward View focused on the need to provide integrated care for patients and placed a new focus on the prevention of ill health in order to keep the general public well.46 However, there are currently significant problems with patient access to general practice services and the heavy workload of general practitioners (GPs) is currently under assessment by the NHS. It is widely recognised that pharmacists are an underused resource. The GP Workforce 10 Point Plan, Building the Workforce—the New Deal for General Practice, agreed in January 201547 aims to address immediate workload issues of GPs by building a workforce in new models of care, including the Clinical Pharmacist in General Practice scheme pilot, part funded by NHS England.48 In this new workforce structure, the role of the experienced clinical pharmacist is to work alongside GPs as a member of the practice team, to reduce GP workload pressure by consulting with and treating patients directly. This pilot study aims to build on the successes of general practices that already employ clinical pharmacists either as part of their team or as partners. It will contribute to an evidence base to determine if clinical pharmacists can be involved in case-finding programmes for conditions which can have significant consequences if not identified. The need to develop an evidence base for pharmacists working within new models of care has been highlighted by the recent review into community pharmacy clinical services.49
This study aims to determine the feasibility of using trained clinical pharmacists based in general practices, to screen for AF, using pulse palpation and a single-lead ECG device. Using a single time point screening strategy which selectively targets the people aged >65 years attending influenza vaccination clinics, we aim to recruit a large and relevant (at-risk) study population for this initial study. In addition, we aim to evaluate the use of the AliveCor Kardia Mobile device compared with pulse palpation alone, as the latter is the current recommendation for screening.32 33
We hypothesise that trained clinical pharmacists, working in collaboration with GPs and using existing healthcare infrastructure, are ideally placed to undertake an AF screening programme, within a primary care setting.
Study population
Participants aged 65 years or older who are eligible for the influenza vaccination and are patients at one of the participating general practices will be invited to have a manual pulse check and a single-lead ECG using the AliveCor Kardia Mobile device with a clinical pharmacist who has been trained by the specialist study cardiologist to assess the rate and rhythm of the heart.
Persons excluded from the study will be anyone under the age of 65 years; patients aged ≥65 years, fitted with a pacemaker; with severe coexisting medical condition (eg, terminal illness); insufficient cognitive capacity (eg, severe dementia) to provide informed consent or who do not provide informed consent at the time of screening. Patients with already identified AF will not be excluded from the study, unless they have a pacemaker.
In Medway and Kent, <65% of the people over 65 years attend influenza vaccination clinics, making them an ideal setting for successful AF screening.45
Recruitment
The screening study will be advertised by poster and leaflet within the participating practices, during October 2017–January 2018; via text message and via verbal contact at the practice during the influenza vaccination clinics. There will be no charge for participation. Participants will be recruited using a consecutive sampling approach.
Sample size
The prevalence of true AF detected among the screened participants aged 65 years or older using pulse palpation and a single-lead ECG is at least 5%,37 but may be as high as 10%.50 Assuming the lowest published estimate of 5%, a sample size of 600 would give 30 cases (95% CIs 22 to 38). With a minimum AF prevalence of 5%, at least 30 patients with AF would be expected to be identified from a sample size of 600 and this is sufficient to allow us to evaluate the proficiency and accuracy of clinical pharmacists to detect AF. This will inform the design and refinement of any future large-scale screening studies.
Clinical pharmacist recruitment
Clinical pharmacists will be recruited from a pool of clinical pharmacists working within the Kent Community Health Trust, from pharmacists already embedded in participating practices and one clinical pharmacist will be provided by the Medway School of Pharmacy.
Clinical pharmacist training
All pharmacists will be offered pulse palpation and ECG training sessions in the evenings and at weekends with the study cardiologist. These sessions will occur at the Medway Maritime hospital on general cardiac wards and cardioversion clinics to expose them to a variety of patients. Training will also involve online ECG evaluation tests and presentations.
Quality processes
The accuracy of the pharmacist interpretation of the ECG will be continually monitored. Continued training and feedback will be offered throughout the study for those who require extra assistance. The pharmacist will be asked to fill in a training evaluation form at the end of the study in order to better inform future training sessions.
Study practices
General practices will be recruited from the multispecialty community provider, Encompass, which is composed of 13 medical practices across the Canterbury and Coastal clinical commissioning area including Whitstable, Faversham, Canterbury, Ash and Sandwich in Kent.
Interventions
All eligible participants will be provided with a participant information leaflet (PIL) about the AF screening study, which will include information about the purpose of the study; what the screening process will involve; eligibility; what happens to the ECG and any collected data; what happens if they withdraw; what happens if they have AF; information about how to contact the investigators or to make a complaint and information about who is funding the study. Those who are interested will be either screened immediately or booked into another clinic at a later date. Those who are deemed eligible and proceed to screening will be assigned an information pack containing all the forms necessary for the session (demographic form, consent form, recording sheet, participant questionnaire and focus group invite) which will have assigned a patient ID code (excluding the participant satisfaction questionnaire and the focus group invite, which will be completely unidentifiable). The patient ID code, the patient name and date of birth will be recorded on a sheet, which will remain at the practice within the research study folder. This will allow participants who require any follow-up treatment to be identified from their patient ID number. The clinical pharmacist will provide them with a brief explanation of the procedure as outlined in the PIL, including management of data and verification of all ECGs by a specialist cardiologist and answer any questions that they may have. The participant will then be asked to provide informed written consent to the study, before the clinical pharmacist proceeds with the screening.
Screening protocol
The screening process including all associated paper work should take on average 10–15 min and will follow the process outlined in figure 2.
The clinical pharmacist will ensure that the participant understands what the study is about by taking them through the PIL, showing them the AliveCor Kardia Mobile device (figure 3) and answering any questions that the participant may have. They will then confirm if the patient wishes to proceed.
The clinical pharmacist will then take the participant through the consent form and ask them to initial all boxes, with the exception of the focus groups participation, which is optional. They will then be asked to date and sign the form, which will be countersigned by the clinical pharmacist. One copy will be retained by the practice and another will be given to the participant to keep.
The clinical pharmacist will then fill in a basic demographic form with the participant (age, gender, ethnicity, height, weight, smoking and drinking habits).
The clinical pharmacist will then perform manual pulse palpation of the radial pulse for 30–60 s and record the number of beats per minute (bpm) and whether they felt the pulse was regular or irregular.
The clinical pharmacist will then use the AliveCor Kardia Mobile device to check the regularity and the bpm of the heart. To minimise noise they will ask any participants wearing hearing aids to temporarily switch them off and to remain silent while recording. The clinical pharmacist will then record a ≥30 s ECG. Only one ECG will be recorded unless the ECG was of poor quality, then a second ECG will be recorded.
The clinical pharmacist will assess the recorded ECG and explain to the participant what they can see. The clinical pharmacist will rate the quality of the recorded ECG (excellent, acceptable, poor or unreadable). They will then record if they can see P waves, if the P wave is followed by a QRS complex and if the intervals between the QRS complexes are regularly spaced. They will then record whether they felt the ECG was normal sinus rhythm (SR), possible AF, unclassified (unreadable or potentially some other arrhythmia) or unreadable (ECG too poor to make any judgement). The clinical pharmacist will also have space to write any additional comments about the ECG or the patient.
The clinical pharmacist will also record the device’s interpretation of the ECG (eg, normal, possible AF, unclassified or unreadable).
The clinical pharmacist will then provide the participant with a letter (normal, possible AF and unclassified/unreadable) dependent on their assessment of the ECG. They will reassure the participants that the cardiologist will over read all ECGs to confirm diagnosis and should there be any issues, they will be contacted by their practice. Participants assigned a possible AF or unclassified diagnosis will be contacted within 2 weeks by the practice to arrange any follow-up care (eg, 12-lead ECG) or to confirm that none is required (eg, if the participant is already on the register and receiving appropriate treatment). Participants who are assigned a normal diagnosis will only be contacted if the cardiologist thinks that this diagnosis is incorrect, otherwise they will expect no further contact. All participants with possible AF will also be given further information about AF before they leave in the form of a British Heart Foundation leaflet (‘Atrial Fibrillation Your Quick Guide’ and ‘I’m in control of my Atrial fibrillation (AF)’).
All participants will then be asked to fill in a short participant questionnaire about the experience.
Any participants who are willing to participate in later focus groups will be given a focus group pack containing an invite letter, participant focus group information leaflet, expression of interest form and a prepaid envelope.
The clinical pharmacist will then add the patient ID code to the ECG and forward it to the study cardiologist via the NHS.net email system. All ECGs (normal, AF or unclassified/unreadable) will be over read by the cardiologist and their result returned within 72 hours to the study team. All ECGs recorded will be uploaded to patient’s medical records. The pharmacists detecting atrial fibrillation (PDAF) study team will collate all the results from the cardiologist and forward a list of patient ID numbers that require follow-up and the type of follow-up required (eg, 12-lead ECG) to the practice. All patient interventions are organised by the GP practice in accordance with normal practice procedure.
The PDAF study team will follow-up all patients given an AF diagnosis (new or existing) by the cardiologist to ensure they have been offered a 12-lead ECG and appropriate treatment from their practice. From those identified patients, enhanced demographic information (eg, medical history, CHA2DS2VASc and HAS-BLED scores, medication history and AF treatment) will be collated.
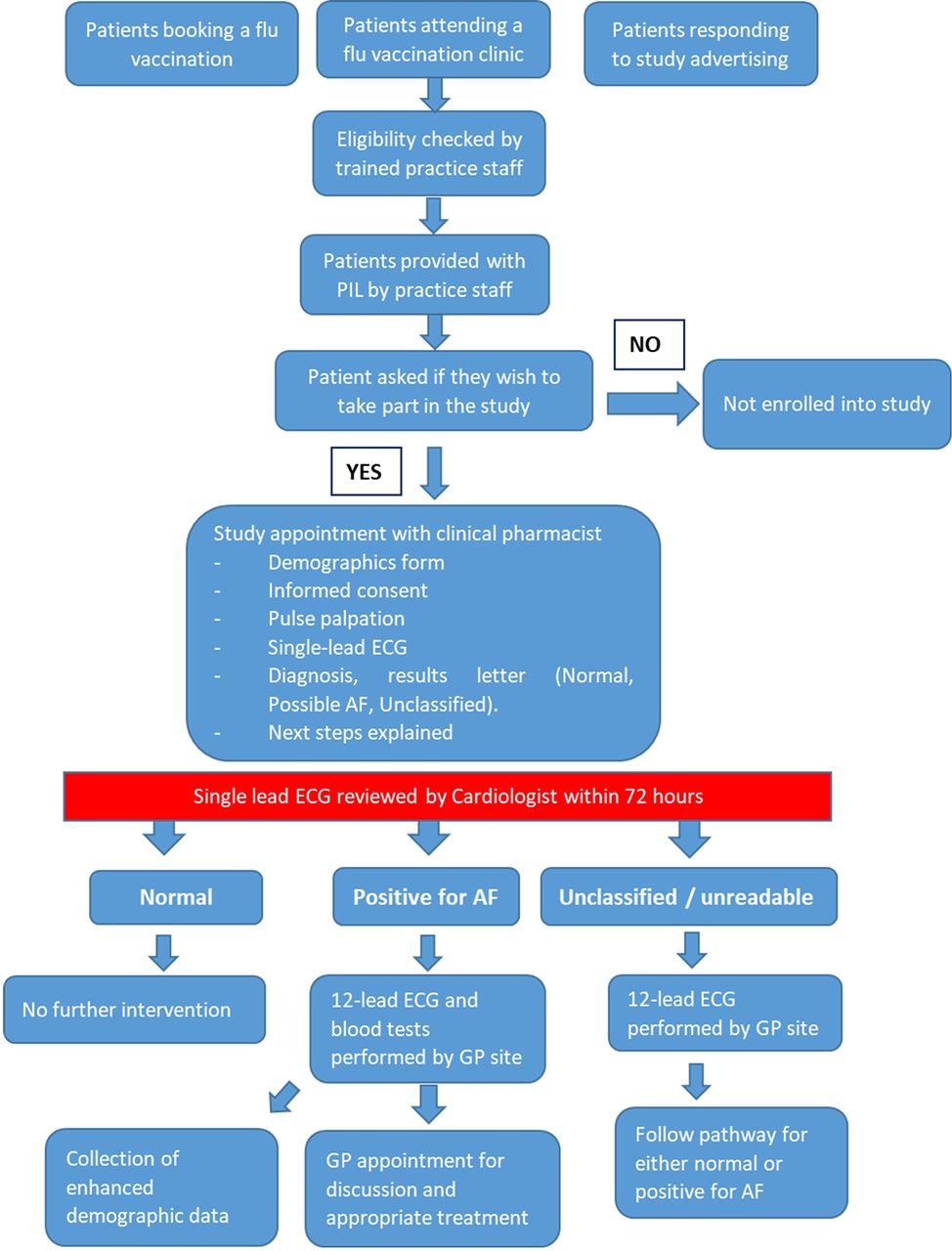
Pharmacists detecting atrial fibrillation study intervention flow chart. AF, atrial fibrillation; GP, general practitioner; PIL, participant information leaflet.

{kind=link}
{kind=link}
{kind=link}
AliveCor Kardia Mobile single-lead handheld ECG (Image used with permission from AliveCor).
Primary outcomes
To determine the accuracy and reliability of the clinical pharmacist identifying pulse irregularities, when using pulse palpation, when compared with the single-lead ECG.
To determine accuracy and ability of the clinical pharmacist to record and interpret a single-lead ECG, using the AliveCor Kardia Mobile device, when compared with the cardiologist interpretation of the ECG.
Secondary outcomes
The level of agreement of the cardiologist’s interpretation of the ECG compared with that of the device’s automated algorithm.
The proportion of people with newly identified AF as confirmed by the cardiologist’s review of the single-lead ECG.
The proportion of newly diagnosed patients that remain in AF by the time of their follow-up 12-lead ECG.
The proportion of participants, newly diagnosed with AF that have pre-existing chronic conditions (eg, hypertension, diabetes and kidney disease) as confirmed by their medical records.
Evaluation of the feasibility of screening for AF by practice-based clinical pharmacist at influenza vaccination clinics, using patient and HCP questionnaires.
Establish the financial impact of the proposed screening strategy on the NHS and adult social care resources using the National Institute for Health and Care Excellence (NICE) cost–utility model.
Quantitative data analysis
Any missing index test data will be excluded from the final analysis without data imputation. Participants with indeterminate index or reference test data will be offered a 12-lead ECG follow-up. For single-lead ECG interpretation, the diagnostic accuracy of the clinical pharmacist and the in-built device’s algorithm will be compared with the scores of the cardiologist using an appropriate paired categorical data test (eg, McNemar’s), where two-tailed p values of <0.05 will be considered significant. The accuracy of the palpation test will be compared with the cardiologist’s scores of ECG regularity from the AliveCor Kardia Mobile ECG recording, again using McNemar’s paired categorical data test. The level of inter-rater agreement between the pharmacist’s, device’s and cardiologist’s interpretations will be determined using Cohen’s kappa statistic, where two-tailed p values of <0.05 will be considered significant.
To quantify the accuracy of detection of genuine episodes of AF, primary analysis will be conducted using IBM Statistical Package for Social Sciences (SPSS V.24). Episodes of AF will be expressed as true positives divided by the total number screened with accompanying 95% CIs.
Analysis of the potential moderating effects of demographic factors such as age, gender or AF risk factors, as well as the difference between sample groups will be performed using multivariate Poisson regression. Two-tailed p values of <0.05 will be considered significant.
A detailed evaluation of the screening process will be undertaken to ascertain the opinions and perceptions of the patients, clinical pharmacists, cardiologist, GPs and practice staff in relation to the PDAF screening protocol. All patient participants will be encouraged to fill in an anonymous participant satisfaction questionnaire, immediately after they have been screened. The pharmacists and GPs will be asked to complete separate questionnaires postscreening to capture initial feedback and to inform the subsequent focus groups.
For cost analysis, the NICE costing report for the management of AF will be used as a platform.32 The costs for screening, treatment and adverse events will be adopted and adjusted for the UK inflation in 2017 (average inflation rate 1.74%). The screening costs per patient will take into consideration the acquisition of single-lead ECG devices and the cost of the clinical pharmacist’s time (average appointment time of 10 min). In addition each new AF diagnosis will include the cost of a 12-lead ECG and consultation with GP and the yearly anticoagulation and monitoring costs as proposed by NICE.2
Qualitative data
A computer database (SPSS V.24) will be developed for responses to completed questionnaires. A 10% quality check of the database will be carried out by a member of the team prior to analysis. The data will be analysed using descriptive statistics.
Focus groups will also be used to explore in depth the patient’s views and experience of the screening process, building on the data collected from patient questionnaires. These will be undertaken 1–3 months after the screening clinics. Focus groups with HCPs and support staff from GP practices will also be used to explore the acceptability and feasibility of adopting this screening service in the future. Barriers and enablers to implementation will be identified.
Interviews will be digitally recorded and transcribed. Data analysis will focus on Flick’s approach51 using the development of predetermined themes connected to the interview schedule. NVIVO 10 will be used to facilitate this process.
Ethics and dissemination
This protocol was approved on 31 October 2017 by the London–Riverside Research Ethics committee and NHS Health Research Authority IRAS. The study will be submitted for site specific assessment at each participating site. The study will be conducted in accordance with the recommendations for physicians involved in research on human subjects adopted by the 18th World Medical Assembly, Helsinki 1964 and later revisions. The findings of this study will be disseminated through forums including, but not limited to, peer-reviewed journals, national and international conferences.
Discussion
The NHS Five Year Forward View is to provide integrated care for patients with a focus on prevention of ill health, in order to keep the general public well.46 However, problems with patient access to general practice services and heavy GP workloads mean that attention is being shifted to other HCPs, with pharmacists being identified as an underused resource that could assist GPs in delivering this. This has led to heavy investment by NHS England into the ‘Clinical Pharmacists in General Practice Scheme’, a pilot study designed to assess the role of the clinical pharmacist based within GP practices.48
This is a multisite research healthcare study between academics at the University of Kent, GPs in primary care and a consultant clinician in secondary care, designed to explore the feasibility of using clinical pharmacists based within GP practices, to accurately screen and diagnose patients with AF using a simple pulse check and a single-lead ECG, during the influenza season, in accordance with the Medical Research Council’s framework for complex interventions.52 We believe that if successful, this comprehensive AF screening strategy will provide a relatively inexpensive mechanism, that capitalises on existing healthcare infrastructure within general practice, to reduce AF-associated stroke (through early AF diagnosis and subsequent oral anticoagulant management, where appropriate) and raise general awareness of AF among the general population and healthcare practitioners. As a consequence, this will improve patient outcomes, benefit healthcare and social care systems, while minimising the associated work load for GPs and clinicians.
Study status
We began recruitment in November 2017.
Acknowledgments
We are grateful to Francis White from AliveCor, UK, who granted permission and provided the image of the AliveCor
Kardia Mobile device.
References
Footnotes
Contributors ELV conceived the original concept of the study. ELV, AJS, AM, SAC, SKL, MR-R and SKB were involved in the design of the study. ELV, AM and VS were involved in the drafting of the article. All the authors were involved in the critical revision of the article and final approval of the submitted article. AM provided statistical expertise. SAC provided qualitative analysis expertise.
Funding This work was supported by a Medical Educational Grant from Bayer UK (UKBAY09170342a) and Faculty of Science Research Funding, University of Kent. Training for pharmacists was additionally supported by a grant from Kent Surrey and Sussex Community Education Providers Network (CEPN).
Disclaimer Bayer UK had no involvement in the design or implementation of this study.
Competing interests None declared.
Patient consent Not required.
Ethics approval This protocol was approved by the London–Riverside Research Ethics committee and NHS Health Research Authority IRAS project ID: 232663.
Provenance and peer review Not commissioned; externally peer reviewed.