Article Text

Abstract
Objectives To investigate how young and older people perceive the harms associated with legal and illegal drugs.
Design Cross-sectional study: adults aged 18–24 years versus 45+ completed an online survey ranking the perceived harms associated with 11 drugs on 16 drug-related harm criteria.
Setting Online survey.
Participants 184 participants aged 18–24 years (113 female: mean age 21: SD 1.3) and 91 participants aged 45+ (51 female: mean age 60: SD 8.5).
Main outcome measures ‘Perception of drug-related harms’: This was measured using a rating scale ranging from 1 (no risk of harm) to 4 (high risk of harm). Participants were also asked about sources which informed their perception on drug-related harms as well as their own personal self-reported drug experiences.
Results Of the illegal drugs, heroin, methamphetamine and cocaine were rated as the most harmful and cannabis was rated as the least harmful. Alcohol and tobacco were also rated as less harmful. The results showed that perceptions of drug-related harms were inconsistent with current knowledge from research on drugs. Furthermore, perceptions on drug harms were more conservative in the 45+ group for a number of illegal drugs and tobacco. However, the 45+ age group did not perceive alcohol as any more harmful than the younger group.
Conclusions This survey demonstrates that the greatest misperception was in relation to alcohol-related harms which did not change with age. In order to minimise harms, this misperception needs to be addressed through education and policies that legislate drug use.
- alcohol
- young
- risk perception
- drug related harms
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to use an appropriate survey tool and method to understand age-related public health perceptions for legal and illegal drugs and how they relate to current research and legal frameworks.
Replicability of the present findings in young people has been demonstrated.
This study used a convenience sample and not a representative sample of participants.
Introduction
Whether legislative or harm reductionist in approach, drug (including alcohol) related public health policies are focused towards reducing drug use and related harms. The most comprehensive work quantifying drug harms was conducted by Nutt et al 1 2 in the UK. Using a multicriteria decision analysis approach where different harm criteria, for example, acute overdose, injury, family adversity were weighted relative to their importance, alcohol was ranked as the most harmful drug overall. Whereas heroin, crack cocaine and methamphetamine were rated as most harmful to the user, alcohol was rated as most harmful to society. Similar results have been reported in European studies3 adding to the growing clinical and epidemiological data that alcohol results in the greatest harm and thus economic cost.4
Drug use normally initiates in adolescence5 with current evidence suggesting that use among young people is on the increase.6 However, due to the neuroplasticity that occurs during this ontogenetic period, the young brain is more susceptible to the harmful effects of drugs.6 Adolescent use of alcohol increases the risk of alcohol dependence7 8 and young people are more likely to end up in hospital following acute alcohol intoxication and are at most risk from alcohol-related road traffic accident morbidity and mortality.5 Thus, reducing alcohol consumption and related harm in young people particularly through the use of brief interventions is key to England’s and Scotland’s Alcohol Strategy.9–11 Of the illicit drugs, cannabis is the most widely used by young people7 who perceive this drug as less harmless compared with the legal drugs alcohol and tobacco.8 9 Explanations offered for this are that unlike legal drugs, cannabis has potential medical benefits10 11 and is not associated with an increased risk of mortality from cancer and alcohol-related road traffic accidents. However, adolescent cannabis use increases vulnerability to its harmful effects7 with early onset of use being associated with a greater loss of IQ (average 8 point decline) and poorer neuropsychological functioning than adult-onset cannabis use.12 Furthermore, it has also been proposed by the contested gateway hypothesis that early exposure to cannabis may increase the likelihood of use of harder illegal drugs (eg, cocaine and heroin), with clinical and epidemiological studies evidencing a link between early use of cannabis and later exposure to other illicit drugs.13 14 A number of vulnerability factors have also been associated with early-onset cannabis use including depression and anxiety15 and high cannabis use is seen in patients with psychosis.16 17 There has also been a consistent increase in drug-related deaths in England and Wales with highest rates of registered deaths being recorded in 2016.18 Although over half of these deaths were related to the respiratory depressant effects of opiate poisoning, there was also a 16% rise in cocaine-related deaths from 2015 to 2016. Finally, the picture of drug-related harm has been complicated by the introduction of new psychoactive substances or the so-called ‘legal highs’. Although these synthetic agents were made illegal under the Misuse of Drugs Act 1971, deaths from these substances have also increased from 114 registered deaths in 2015 to 123 in 2016.18
The population consumption theory suggests a direct link between alcohol consumption and alcohol-related harm.4 Older populations, however, are more vulnerable to the burden of chronic alcohol related disease, for example, cirrhosis, fatty liver, pancreatitis, Wernicke’s encephalopathy5 with recent findings from a longitudinal study suggesting that drinking habits remain stable over a 30-year period.19 A report by the Lancet Liver commission found that alcohol-related mortality in England peaked in 2008. However, by reducing the affordability of alcohol in the same year via a 2% increase in alcohol tax duty, there was a consistent decrease in alcohol-related deaths. While Scotland has introduced a fiscal policy of minimum unit pricing for alcohol, the tax levy on alcohol in England was dropped in 2014, thus making alcohol more affordable again. Thus, a potential consequence of regional differences in policy could result in decreases in alcohol-related mortality in Scotland whereas England may again see a rise in alcohol-related death rates.4
In summary, there is robust evidence for the harm and public health threat posed by drugs including alcohol and how the harms of different drugs may differ by age. However, little is known about the public’s perceptions of harms associated with these same drugs. Thus, the aim of the present study was to investigate how young versus older people (18–24 years old vs 45+) understand drug-related harms and whether perceptions towards drugs become more conservative with age. Given the normative role of alcohol within society, the latter question was considered particularly pertinent to this drug. Furthermore, as the largest predictor for alcohol use in adolescence is peer drinking,20 data on where young versus older people acquired knowledge about drug harms as well as their own personal self-reported experiences with drugs including alcohol were collected.
Method
Materials
To measure perception of ‘drug harms’, the 16 harm criteria developed by Nutt et al 2 were used. These distinguish between harm to the user versus society and are grouped into five subheadings of physical, psychological and social harm to users and physical and social harm to society. Harms of 11 commonly used drugs were assessed: heroin, crack cocaine, cocaine, ecstasy, methamphetamine, Lysergic acid diethylamide (LSD), amphetamine, cannabis and ketamine, alcohol and tobacco. The 16 harm criteria were carefully explained to the respondents and for each criterion, drugs were ranked on a rating scale of 1–4; no risk of harm,1 low risk of harm,2 medium risk of harm3 and high risk of harm.4 The next section of the questionnaire (adapted from21) required respondents to rate from a list of possible different sources, the top three sources which they believe had most informed their knowledge on drug harms. In addition to the sources of information used in the21 study, ‘popular culture, for example, books, television (TV), movies, famous people’ was also included. The final section of the questionnaire (adapted from Morgan et al 22) required respondents to self-report their most accurate lifetime experience with the drugs listed. For the survey questionnaire, see online supplementary information section.
Supplementary file 1
The present research was undertaken in two parts: study 1 and study 2. In study 1, the harms questionnaire was administered to a group of young adult respondents aged 18–24 years. In study 2, responses on the harms questionnaire were compared between two different age groups: 18–24 years old versus 45+.
Study 1 respondents
Eligible respondents had to be aged between 18 and 24 years, but no other inclusion criteria were applied and demographic information on age, gender, ethnicity and level of education was collected. The questionnaire was uploaded onto ‘http://www.surveymonkey.com’ and was available online from October 2014 to January 2015. It was advertised on various social media networks including Facebook and via email. A total of 119 responses were collected, but there were missing data in 23 of these cases, so they were removed from the analysis. This left 96 respondents who completed the entire questionnaire. On inspection of the data, nine of the respondents said that they had not heard of at least 1 of the 11 drugs and since respondents are not able to rank drugs which they had not heard of, their data were removed from the analysis. This left a total 88 of respondents. Table 1 represents demographic data for these participants. Sixty per cent of the sample were females with an average age of 22 (SD=1.28). Sixty-six per cent of the respondents were of white ethnicity with most respondents being university students.
Demographics of the study respondents
Study 2 respondents
Eligible respondents had to be adults aged between 18 and 24 or 45+, but no other inclusion criteria were applied and demographic information on age, gender, ethnicity and level of education was collected The questionnaire was distributed electronically via Qualtrics Survey Software and for the group aged 18–24 years the online survey was available from November 2015 to March 2016. The 45+ group were recruited via Pureprofile, a commercial online survey management system. Thisgroup of participants were recruited in July 2016 and received £3.50 each for their participation.
In total 96 respondents aged 18–24 years and 91 aged 45+ completed the online questionnaire. Again any respondents who said they had not heard of any one of the drugs were removed from the analysis leaving a total of 88 and 86 respondents in each group, respectively. The two samples differed in terms of ethnicity (χ2=21.68, p<0.001) with the older sample being less ethnically diverse. There were also significant differences in level of education (χ2=66.83, p<0.001) with the younger sample being university students and the older sample being educated to GCSE level (table 1).
Procedure
Respondents were required to read and tick a box to acknowledge that they had read the online information sheet. Participants were then required to answer six informed consent statements including confirmation that they were 18 years old or over. The questionnaire took approximately 30 min to complete and all responses were anonymous.
Patient and public involvement
The current study did not include patient and public involvement.
Data analysis
Data were exported to SPSS V.20 for analysis. An overall harm rating was obtained for each drug by averaging scores for all 16 harm criteria across all participants. Spearman’s rank correlations were used to investigate relationships between respondent’s knowledge of the harms of different drugs in comparison to expert’s harm rating2 and to the legal status of a drug according to the UK Misuse of Drugs Act.23 The present study used a perceived harm ranking scale ranging from 1 to 4. This scale was adapted from Morgan et al 22 with the absence of a 0 score, whereas Nutt et al 2 used a scale from 0 to 100. Similarly, the Misuse of Drugs Act23 has three classifications (classes A, B and C) as well as the tacit classification of legality which pertains to tobacco and alcohol. This was coded on a scale from 1 to 4, with 1 indicating legality and 4 indicating a class A drug. In study 2, Student’s t-tests were conducted to compare the perception of drug harms between the two age groups. The significance threshold was set to p<0.05 and values reported are for two-tailed hypotheses.
Results
Study 1
Overall perceived harm rankings
Figure 1 shows in rank order the mean perceived harm rating for each drug along with its classification under the Misuse of Drugs Act. The class ‘A’ drugs heroin (3.76), methamphetamine (3.66), crack cocaine (3.66) and cocaine (3.43) were perceived as the most harmful, and alcohol was perceived as the third least harmful drug (3.13). The class ‘B’ drug cannabis (2.75) was perceived as the second least harmful drug, with tobacco (2.41) being perceived as least harmful. A Spearman’s rank correlation revealed a significant positive relationship between the respondents harm ratings of drugs and its legal classification (r=0.70, n=11, p=0.01) with higher perceived harm ratings given to drugs that were within a higher drug class. However, there was no statistical relationship between the young people’s perceived harm ratings against those of Nutt et al’s2 expert panel (r=0.38, n=11, pNS; see figure 2).

Drugs ordered by their overall harm rating in 18–24 years old. Classification under the Misuse of Drugs Act (class A, B and legal) is colour coded.

Correlation between the mean harm ratings of 18–24 years old and those reported by drug experts in Nutt et al.2
Sources reported to acquire knowledge on drug harms and self-reported experiences with drugs in young people
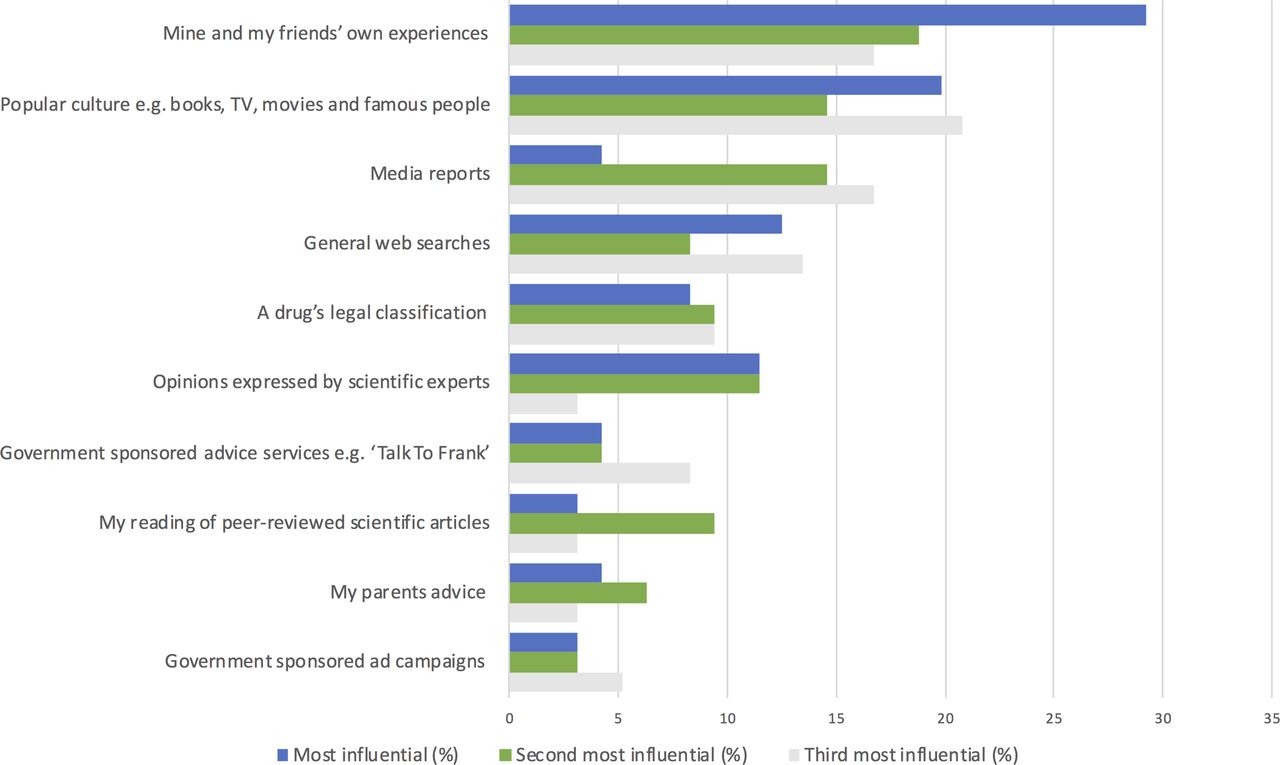
The most influential source of information from which 18–24 year olds self-reported acquiring knowledge on drug harms were ‘Mine and my friends own experiences’ (29.2%) and ‘popular culture, for example, books, TV, movies, famous people’ (19.8%) (see figure 3). Least influential included ‘peer-reviewed articles’ (3.1%) and ‘government sponsored ad campaigns’ (3.1%).

Sources rated as most influential by 18–24 years old on acquiring knowledge on drug-related harms ordered by cumulative influence. TV, television.
When asked about their own experiences with the 11 drugs, respondents were most likely to have used alcohol (63.2%), followed by cannabis (45.3%) and tobacco (44.2%). 29.5% of respondents described themselves as regular users of alcohol, 7.4% as regular tobacco users and 5.3% as regular cannabis users (table 2). 24.2% of the study respondents reported having tried ecstasy and 1% of the respondents appeared to describe themselves as poly-drug users. The drugs that respondents were least likely to have heard of were LSD and ketamine.
Self-reported lifetime experiences of drug use in 18–24 years old
Study 2
Overall perceived harm ranking
Figure 4 compares perceived harm ratings in the 18–24 years versus the 45+ group. In general, perceptions on drug harms were more conservative in the 45+group who rated 8/11 drugs as being more harmful than the 18–24 years group. There were, however, three notable exceptions: Heroin and cocaine were perceived as equally harmful by the two age groups (in both cases t (172)<1.24, pNS). Alcohol was perceived as the fourth least harmful drug in the 18–24 years and perceptions towards it as a harmful drug were not more conservative in the 45+ group (t (172)=1.06, pNS). A Spearman’s rank correlation revealed a significant positive relationship between perceived harm ratings between 18–24 years group in study 1 and 2 (r=0.98, n=11, p=0.001) and between 18–24 years old and 45+ age group in study 2 (r=0.94, n=11, p=0.001). Both the 18–24 years and 45+ ratings correlated positively with legal classifications of the drugs (18–24 years old: r=0.62, n=11, p<0.05; 45+: r=0.79, n=11, p<0.01) but not with expert ratings (18–24 years old: r=0.49, n=11, pNS; 45+: r=0.32, n=11, pNS).

Mean harm ratings of individual drugs for the 18–24 years old versus the 45+ age group. *P<0.05, **P<0.01, ***P<0.001.
Sources reported to acquire knowledge on drug harms and self-reported experiences with drugs in young and older people
‘Their own and their friends experiences’ was important in how 18–24 years group (75.5%) self-reported acquiring knowledge on the drug harms whereas the ‘media reporting of drugs’ influences the opinions of both 18–24 years (40.0%) and 45+ group (56.5%). A ‘drugs legal classification’ along with the ‘portrayal of drugs in popular culture’ were also ranked highly by both age groups and the older group also reported valuing ‘the opinions of scientific experts’ (54.1%), figure 5. As shown in table 3, young people were significantly more likely to be regular users of alcohol (x2=9.1, n=174, p=0.01) but there were no significant differences in the use of tobacco between 18 and 24 years old versus 45+ group (x2=4.9, n=172, p=0.78). The 18–24 years group were more likely to have used cocaine (x2=10.09, n=174, p=0.01), and were also more likely to self-report regular use of cannabis (x2=31.46, n=174, p=0.001) and ecstasy (x2=31.96, p=0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of the sources rated as most influential in 18–24 years old versus 45+ age group on acquiring knowledge on drug related harms.
Self-reported lifetime experiences of drug use in 18–24 years old versus 45+ age group
Discussion
Principal findings
Both young and older people perceived heroin, cocaine, crack cocaine and methamphetamine as the most harmful and cannabis as the least harmful of the illegal drugs. In this respect, the perceived harm ratings of both age groups correlated with the legal classification of drugs. However, young people perceived alcohol as one of the drugs associated with less harm. Similarly, in the older group, where perceptions of harms for some drugs were more conservative, alcohol was not perceived as any more harmful than that reported by the 18–24 year olds. The fact that the older age group did not see alcohol as more harmful is inconsistent with current knowledge, but could possibly be understood on the basis that for this group, alcohol is their main form of intoxication, source of pleasure and recreation. The drugs both younger and older participants most commonly claimed to be ‘regular users’ of were alcohol and tobacco. Younger participants, however, were also more likely to report regular use of cannabis and ecstasy. Young people ranked ‘mine and my friends own experiences’ as most influential. Government sponsored advert campaigns and to a lesser extent advice service (eg, Talk to Frank) were rated as less influential sources on drug-related harms. However, both the young and the older group ranked ‘popular culture’ and ‘media reports’ as influential sources of information on drug-related harms.
Strengths and limitations
There are several strengths to the present study. This is the first study to understand perceptions towards drug harms in two samples differing in age. Furthermore, perceptions of the harms associated with alcohol are not more conservative in an older group that is more likely to be assessing the long-term harms of alcohol. This finding is in direct contrast to tobacco, which the older participants did perceive as more harmful. Furthermore, in the present paper, the young sample were tested twice in two different studies and a strong correlation was reported between both studies, suggesting the data are replicable and the methodology robust. Other strengths include being able to compare our findings with the legal classification of a drug and against those of experts within the field. Limitations include the use of two different methods to recruit participants to the second study which investigated the effects of age on perceived drug harm rankings. The young sample was recruited via social media but it was felt the older age group were less likely to use social media, and this guided the decision to recruit them through a different channel, using an online agency which involved a financial incentive. The present study also used a cross-sectional study design which could mean that the finding that alcohol was not perceived as more harmful in the older group is due to cohort differences. However, that tobacco was perceived as more harmful in the older group would not support such an explanation. It is clear, however, that some of the differences between groups may be mediated by factors other than age. Our demographic data show a narrow range of ethnicities and a broader range of educations. We were not able to fully explore the effects of these factors as we had limited data in many of the categories (eg, older age group had 95% white participants). A further limitation is that the two samples were recruited through convenience sampling and are thus not representative of the general population and the results may thus be affected by sampling bias. Therefore, future research should aim to confirm the present findings in representative samples. Furthermore, most of the young people recruited to our study were university students who were more likely to be well educated and they were more ethnically diverse compared with the predominately white population in the older age group. Indeed the ethnic diversity and the inclusion of religious groups where alcohol is prohibited would explain the result that 6.1%–7.4% of the young population reported no direct experience with alcohol. This study used the Nutt matrix of harm2 and some have suggested that there are limitations to this approach since a drugs harms cannot be reduced to a single score. This is because the concept of harm is based on a multitude of factors including the pharmacology of a drug, how, in the case of poly-drug use; it interacts with other drugs, the user’s own behaviour, environmental factors and policies that legislate drug use. Furthermore, even the most objective harm criteria can be subject to some degree of social construction, for example, cases when drug-related mortality is attributed as the cause of death.24 However, Nutt’s work is still the most comprehensive model for quantifying the harms associated with different drugs and thus considered a good starting platform for understanding people’s perception of harms associated with different drugs compared with the scientific evidence. As the use of new psychoactive substances or the so-called legal highs within young people in the UK is on the rise,25 the inclusion of these drugs would have helped to establish a more complete understanding of young people’s perceptions of the harms of drugs and how this interacts with sociocultural factors. This is considered pertinent as the use of synthetic cannabinoid receptor agonists, for example, spice has shifted from affluent student groups exploring legal highs as a form of recreation to more vulnerable young people including the poor, unemployed and young adults in prison. While this group perceive legal highs as dangerous and dirty drugs, use in these vulnerable populations is driven by cheap price and availability.26 Finally, we have not focused on some of the benefits that are associated with recreational drug use nor on the reasons why drugs are used recreationally.
Comparisons with other studies
Both young and older people perceived heroin, cocaine, crack cocaine and methamphetamine as the most harmful drugs. These findings paralleled the classification of these drugs under the Misuse of Drugs Act 197123 and research findings reported by the scientific community on drug harms.2 Although the legal classification of cannabis was upgraded from class ‘C’ to ‘B’ in 2009, our study sample perceived it as the least harmful of the illegal drugs. Furthermore, although alcohol is rated as the most harmful drug by the scientific community,2 3 specifically due to the damage it causes to the users physical health, for example, cirrhosis, fatty liver, cardiomyopathy, and its direct and indirect economic costs (eg, healthcare, prison, social services, insurance, crime, absenteeism and loss of productivity) an accurate perception of the harms of alcohol in relation to other drugs was not evident in the current study.
In contrast to the findings with alcohol, tobacco was perceived as more harmful in the older group and consistent with this, many of the harmful effects of this drug are seen much later in life.27 It is likely that the results with tobacco are explained by the smoking ban which was introduced in England 10 years ago (1 July 2007). This ban imposed restrictions on tobacco advertising and smoking in public places, for example,workplaces, which led to reduced opportunity to smoke and the creation of social norms around smoking being unacceptable.28 There is also evidence that the smoking ban has reduced prevalence rates and the progression of experimental to habitual smoking in young people29 and also resulted in more quit attempts in young people.30
The findings that the young respondents ranked their own experiences and their own friends experiences in informing their knowledge on drug harms is consistent with similar findings in drug users.21 This finding is also consistent with literature that adolescence is defined by a period in which peer influence has the greatest effect on initiation of substance use.31 Also ranked highly by both younger and older respondents was the influence of popular culture, that is, books, TV, movies and famous people’ on informing on drug-related harms. The integral nature of drugs as cultural commodities is evidenced through the detailed and insightful history of drug messages through film, music and advertising. In fact, imagery normally associated with illegal drugs, that is, dance culture has been used by the drinks industry to promote alcohol to young people with music being the most influential form of popular culture for this group.32
Conclusions and policy implications
In summary, the results from the present study suggest that perceptions of drug harms in the study sample challenge what is currently known from scientific research on legal drugs.1 2 21 Thus, despite study participants understanding the harms associated with illegal drugs, for the most part they were less well informed of the harms of legal drugs especially alcohol. The misperception of alcohol-related harms among the young and older participants is concerning given that it is the most regularly used drug and thus carries the highest public health risk. The present research suggests that although focus on drug-related harms in young people is essential, the importance of population-level strategies should not be underestimated. A recent review established that interventions found to be most effective in reducing alcohol and tobacco intake in young people were taxation, public consumption bans, advertising restrictions and minimum legal age limits.28 Given the pervasive and normative nature of alcohol within society, a huge cultural and political shift is required in order for there to be a more informed perception of alcohol-related harm. Indeed emphasis should be placed on consistency in messages from different sources, that is, the legal system, the media and popular culture and the alcohol industry.
Since many recreational drugs, especially in young people, are not used in isolation, educational strategies to reduce drug-related harms could focus on the potentially dangerous pharmacologically synergetic effects some drugs have when taken with alcohol. For example, severe impairments of driving under the influence of cannabis and alcohol33; concomitant use of alcohol and cocaine leads to the toxic compound cocaethylene34; the suppression of the respiratory system when alcohol and benzodiazepines are taken together and findings that a combination of alcohol with magic mushrooms can be fatal.35 In young people, it is also necessary to increase awareness of the pharmacologically lethal effects of high doses of alcohol, that is, suppression of the respiratory system and death.
In summary, there is a growing need for a better understanding of what constitutes optimal public health policy to approach the growing health issue of drug use and related harms.6 Our findings suggest that younger and older people have poor perceptions of drug-related harms which while consistent with current UK policy are inconsistent with current knowledge. Our findings are consistent with the 2018 Global Drug Survey results which found that the biggest gap in knowledge was in alcohol-related harm.36 As this is the most widely used drug and an inherent part of society, this latter concept has to be intrinsically weaved into all approaches and policies that aim to be effective in reducing drug-related harms.
Acknowledgments
We thank all the respondents for participating in this study. Patients were not involved in this research project. We also would like to thank the reviewers for their comments.
References
Footnotes
Contributors SC and LW were responsible for study design and AH, MK, RZ and ES for data collection. SC, ALW, AH, MK, RZ and ES analysed the data. SC, ALW, AH, MK, RZ and ES drafted the paper. All authors: read, commented on and approved of the final manuscript.
Funding This project was funded through Brunel University London.
Competing interests None declared.
Patient consent Not required.
Ethics approval The present research received ethical approval from the College of Health and Life Sciences Ethics Committee, Brunel University London
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be extracted by emailing the corresponding author SC.