Article Text

Abstract
Objectives Ischaemic heart diseases (IHDs) are a leading cause of death worldwide. Although prescribing according to guidelines improves health outcomes, it remains suboptimal. We determined whether interventions targeted at healthcare professionals are effective to enhance prescribing and health outcomes in patients with IHDs.
Methods We systematically searched PubMed and EMBASE for studies published between 1 January 2000 and 31 August 2017. We included original studies of interventions targeted at healthcare professionals to enhance prescribing guideline-recommended medications for IHDs. We only included randomised controlled trials (RCTs). Main outcomes were the proportion of eligible patients receiving guideline-recommended medications, the proportion of patients achieving target blood pressure and target low-density lipoprotein-cholesterol (LDL-C)/cholesterol level and mortality rate. Meta-analyses were performed using the inverse-variance method and the random effects model. The quality of evidence was assessed using the Grading of Recommendations, Assessment, Development, and Evaluation approach.
Results We included 13 studies, 4 RCTs (1869 patients) and 9 cluster RCTs (15 224 patients). 11 out of 13 studies were performed in North America and Europe. Interventions were of organisational or professional nature. The interventions significantly enhanced prescribing of statins/lipid-lowering agents (OR 1.23; 95% CI 1.07 to 1.42, P=0.004), but not other medications (aspirin/antiplatelet agents, beta-blockers, ACE inhibitors/angiotensin II receptor blockers and the composite of medications). There was no significant association between the interventions and improved health outcomes (target LDL-C and mortality) except for target blood pressure (OR 1.46; 95% CI 1.11 to 1.93; P=0.008). The evidence was of moderate or high quality for all outcomes.
Conclusions Organisational and professional interventions improved prescribing of statins/lipid-lowering agents and target blood pressure in patients with IHDs but there was little evidence of change in other outcomes.
PROSPERO registration number CRD42016039188.
- ischaemic heart disease
- quality In health care
- preventive medicine
- guideline adherence
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is a systematic review and meta-analysis of randomised controlled trials, conducted following the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
This review focused on interventions targeted at healthcare professionals to enhance prescribing of individual medications for acute coronary syndrome. Interventions were classified according to the Cochrane Effective Practice and Organization of Care Review Group. But more detailed analyses, for example, on duration or intensity of intervention implementation, were impossible due to the limited number of studies.
We may have missed relevant unpublished or locally published studies as we restricted our search to English publications and did not search for grey literature.
Introduction
Ischaemic heart diseases (IHDs) are a leading cause of death worldwide accounting for 13.2% of all deaths globally.1 IHDs include angina pectoris and myocardial infarction.2 International guidelines recommend using a combination of an antiplatelet agent, a beta-blocker, an ACE inhibitor or an angiotensin II receptor blocker (ACEI/ARB) and an HMG coenzyme A reductase inhibitor (statin) to treat eligible patients with IHDs.3–8 This combination is an effective secondary prevention after myocardial infarction, reducing morbidity and mortality.9–13 Despite such evidence, rates of patients being prescribed medications according to guidelines varied from <5.0% to >95.0%, leaving a substantial proportion of patients with IHDs not receiving guideline-recommended care.14–17 Changing clinicians’ behaviour to improve prescribing guideline-recommended medications is challenging. Different types of interventions have been developed and classified as professional interventions (eg, education,18–21 reminders,22 audit and feedback23), organisational interventions (eg, computerised clinical guidelines,24 pharmacist-led intervention25), financial interventions (eg, financial incentives26) and regulatory interventions (eg, cap and copayment policies27).
Interventions to improve prescribing guideline-recommended medications for cardiovascular diseases, in general, have been reviewed recently.28 29 Moreover, Murphy et al have evaluated the effect of organisational interventions for patients with IHDs.30 The interventions aimed to improve mortality and hospital admissions and targeted physicians and patients to adhere to recommendations of secondary prevention of IHDs (lifestyle modification, prescribing medications or both).30 No work has been done synthesising the evidence on interventions to enhance prescribing according to guidelines for patients with IHDs as far as we are aware. In this review, we focus on interventions targeted at health professionals. Other factors influencing prescribing, such as patient behaviour, organisational factors or resource constraints are outside the scope of this review.31 We conducted a systematic review and meta-analysis to determine whether interventions targeted at healthcare professionals are effective to enhance prescribing and health outcomes in patients with IHDs.
Methods
We conducted a systematic review and meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement32 and the Cochrane Handbook for Systematic Reviews of Interventions.33 We registered our protocol with the International Prospective Register of Systematic Reviews Registry (CRD42016039188).34
We searched the electronic bibliographic databases PubMed and EMBASE as these are considered to be the most important sources for reports of trials.33 The search strategy included MeSH terms and relevant keywords in various combinations relating to guidelines, guideline adherence, drug therapy, IHDs and randomised trials (see online supplementary appendix A). We restricted our search to studies carried out in humans and published in English. Studies published between 1 January 2000 and 31 August 2017 were sought. References of included articles were manually screened to identify additional eligible studies.
Supplementary file 1
We included original studies reporting results of randomised controlled trials (RCTs) or cluster randomised controlled trials (cluster RCTs) in patients with IHDs eligible for receiving secondary preventive treatment. Studies had to evaluate interventions targeted at healthcare professionals to enhance prescribing of guideline-recommended medications. The trials had to include at least one prospectively assigned concurrent control group. The control group had to receive usual care (not receiving the intervention), or an intervention of lower intensity or shorter duration than the intervention group. Studies had to report patient-level outcomes. We excluded duplicate reports, post hoc analyses or abstracts from meeting proceedings unless published as full-text reports in a peer-reviewed journal. We excluded studies on patients receiving acute treatment in hospital only; or interventions predominantly targeting patient medication-taking behaviour or lifestyle modifications.
All titles and abstracts retrieved from the electronic searches were archived in the web-based bibliography and database manager RefWorks. After removing duplicates, two reviewers (TN and HQN) independently screened the titles and abstracts. They also independently assessed the full text of potentially eligible studies. Disagreements between the reviewers whether to include or exclude a study were resolved by consensus.
Two reviewers (TN and NNW) independently extracted data from the trials’ primary texts, the online supplementary appendices and protocols using a data abstraction form. We extracted the following information: trial name, year of publication, sources of funding, setting and time of recruitment, study design, study population characteristics, details of the intervention and control conditions, main outcomes and evidence for assessment of the risk of bias. Disagreements were resolved by discussion with a third reviewer (KT).
Two reviewers (TN and NNW) independently assessed the risk of bias of each study using the tool of the Cochrane Effective Practice and Organization of Care Review Group (EPOC).35 The nine standard criteria were: (1) random sequence generation, (2) allocation sequence concealment, (3) similarity of baseline outcome measures, (4) similarity of baseline characteristics, (5) blinding of outcome assessment, (6) adequately addressing incomplete outcome data, (7) adequate protection against contamination, (8) free from selective reporting and (9) free from other risks of bias (eg, recruitment bias or not adjusting for clustering effect in cluster RCTs).35 Disagreements were resolved by discussion with a third reviewer (KT). We judged trials with four or more high-risk domains, or three or more high-risk domains plus three or more unknown domains as having a high risk of bias.
The primary outcomes were the proportion of eligible patients receiving the following guideline-recommended medications: aspirin/antiplatelet agents, beta-blockers, ACEIs/ARBs, statins/lipid-lowering agents and a composite of these medications. The secondary outcomes were: the proportion of eligible patients achieving target blood pressure and target LDL-C/cholesterol level, and the mortality rate.
The interventions were classified according to the taxonomy of the EPOC36 as professional, financial, organisational or regulatory interventions. We performed meta-analyses for outcomes when the necessary data were available. Meta-analyses were performed in the Review Manager V.5.3 (RevMan 5)37 using the inverse-variance method and the random effects model. The main outcomes were measured as dichotomous variables. The OR with corresponding 95% CI was calculated for each outcome of interest to generate a forest plot. For studies with more than two trial groups, we combined relevant groups to create a single pair-wise comparison.33 A Z-test was used to assess the statistical significance of the results of the meta-analysis with a two-tailed P value of <0.05. The intracluster correlation coefficients (ICCs) for cluster RCTs were used to calculate the effective sample size to ensure the clustering effect was taken into account in our analyses. When an ICC was not reported in a cluster RCT, we contacted the trial authors. In case of non-response, we used the mean of corresponding ICCs reported in the other included cluster RCTs to adjust for the clustering effect.38 39
Two reviewers (KT and TN) independently assessed the quality of evidence across included studies of all outcomes of interest using the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) approach.40 The following criteria were used: serious limitations in study design and implementation, indirectness, substantial heterogeneity, imprecision and publication bias. The GRADE approach specifies four levels of quality: high, moderate, low and very low. The quality rating was downgraded by one level for each factor having a serious limitation, up to a maximum of three levels for all factors. Heterogeneity across trials for each outcome of interest was investigated using the Cochran’s Q test and was measured by the I2 statistic. An I2 exceeding 50% indicated substantial statistical heterogeneity.33 41 Publication bias was evaluated visually by inspecting funnel plots and quantified by the Egger’s test for outcomes comprising at least 10 trials.33 42
We performed subgroup analyses and sensitivity analyses when the necessary data were available. Subgroup analyses were performed for type of study designs, type of intervention, comparators and setting of the intervention. We examined the robustness of our findings in sensitivity analyses excluding studies with high overall risk of bias, and analyses without adjusting for clustering effect.33
Results
The search of PubMed and EMBASE databases provided a total of 8424 citations, and 452 citations were added from the lists of references from included studies. After removing duplicates, 7535 remained. Of those, 7219 papers were discarded after screening titles and abstracts. The full text of 316 studies was examined in more detail, 303 studies did not meet the inclusion criteria. A total of 13 studies43–59 were identified for inclusion in the review (figure 1). These were 4 RCTs45 49 51 59 involving 1869 patients and 9 cluster RCTs43 47 50 52 53 55–58 involving 599 healthcare centres and 15 224 patients. Trials were carried out between 1997 and 2012 and published between 2001 and 2015. Control groups received usual care (nine studies43 45 49–52 55 58 59) or less intensive interventions (four studies47 53 56 57). Seven studies43 49 52 53 55 57 59 reported patients’ health outcomes (table 1). The overall risk of bias was rated as low in all included studies (table 1 and more details in online supplementary appendix B).
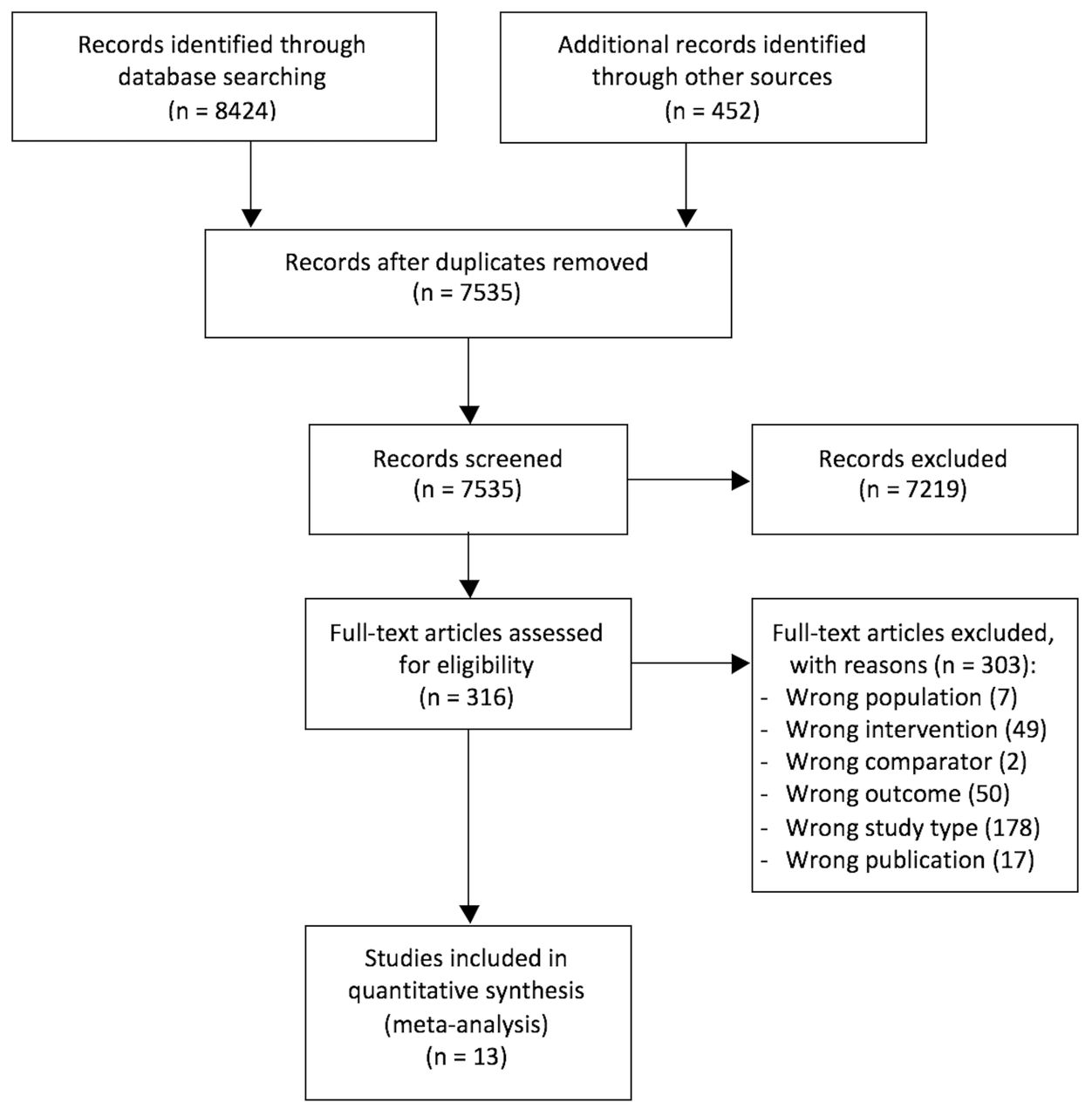
Flow chart diagram of study selection.
Characteristics of included studies
Five studies45 49 50 52 59 used organisational interventions, four studies51 53 55 58 professional interventions and four studies43 47 56 57 a combination of organisational and professional interventions. Distribution of educational materials, educational outreach visits, audit and feedback and reminders were the four professional interventions most frequently used. Continuity of care, communication and case discussions between distant healthcare professionals were the two organisational interventions most frequently used (table 2 and more details in online supplementary appendix C).
Intervention description
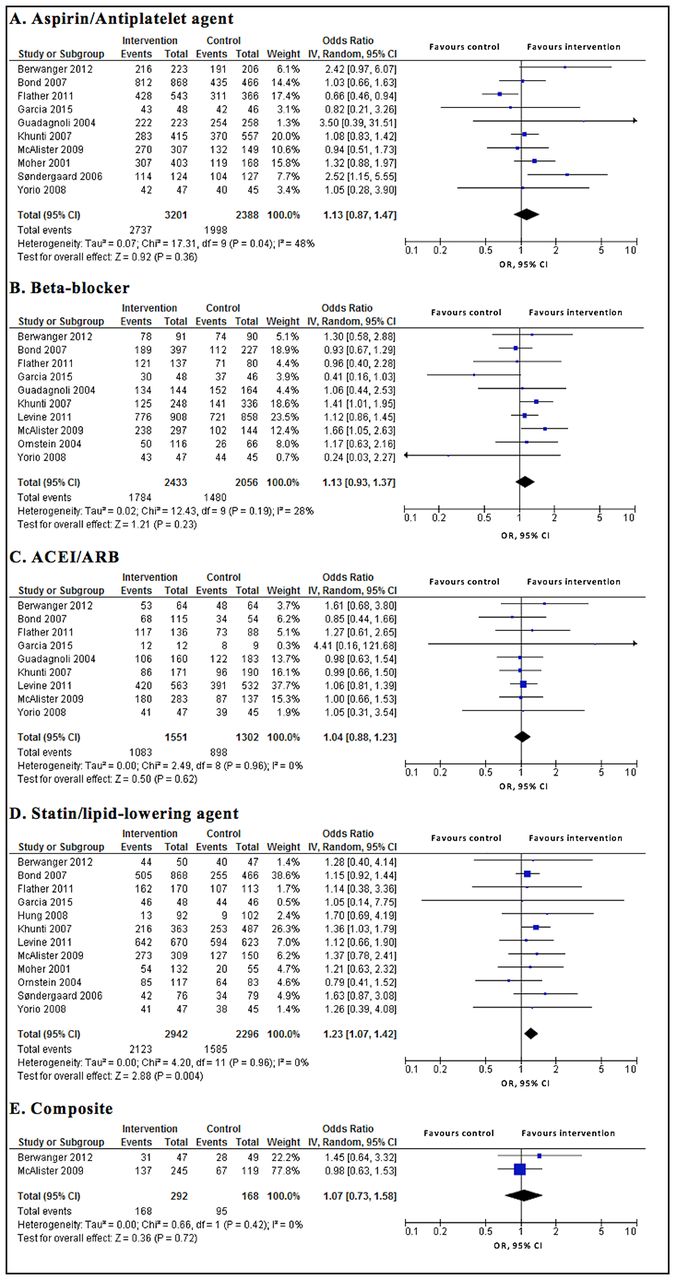
Interventions had no significant effect on prescribing guideline-recommended medications, that is, there was no significant difference in the proportion of eligible patients receiving guideline-recommended medications between intervention and control groups except for statins/lipid-lowering agents. The findings were aspirin/antiplatelet agents (OR 1.13; 95% CI0.87 to 1.47; P=0.360), beta-blockers (OR 1.13; 95% CI 0.93 to 1.37; P=0.230), ACEIs/ARBs (OR 1.04; 95% CI 0.88 to 1.23; P=0.620) and statins/lipid-lowering agents (OR 1.23; 95% CI 1.07 to 1.42; P=0.004), the composite of medications (OR 1.07; 95% CI 0.73 to 1.58; P=0.720). The evidence was of moderate or high quality for the primary outcomes (figure 2 and table 3).
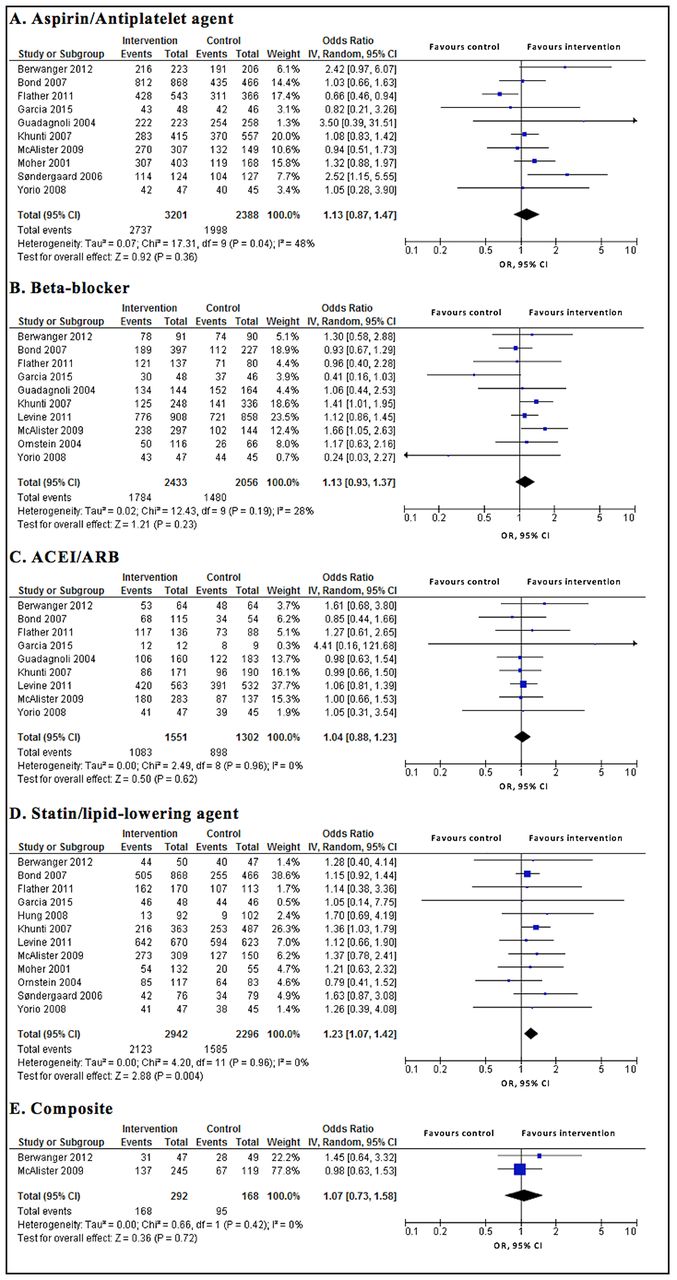
Primary outcomes of intervention vs control. ACEI, ACE inhibitors; ARB, angiotensin II receptor blocker.
Summary of findings and quality assessment
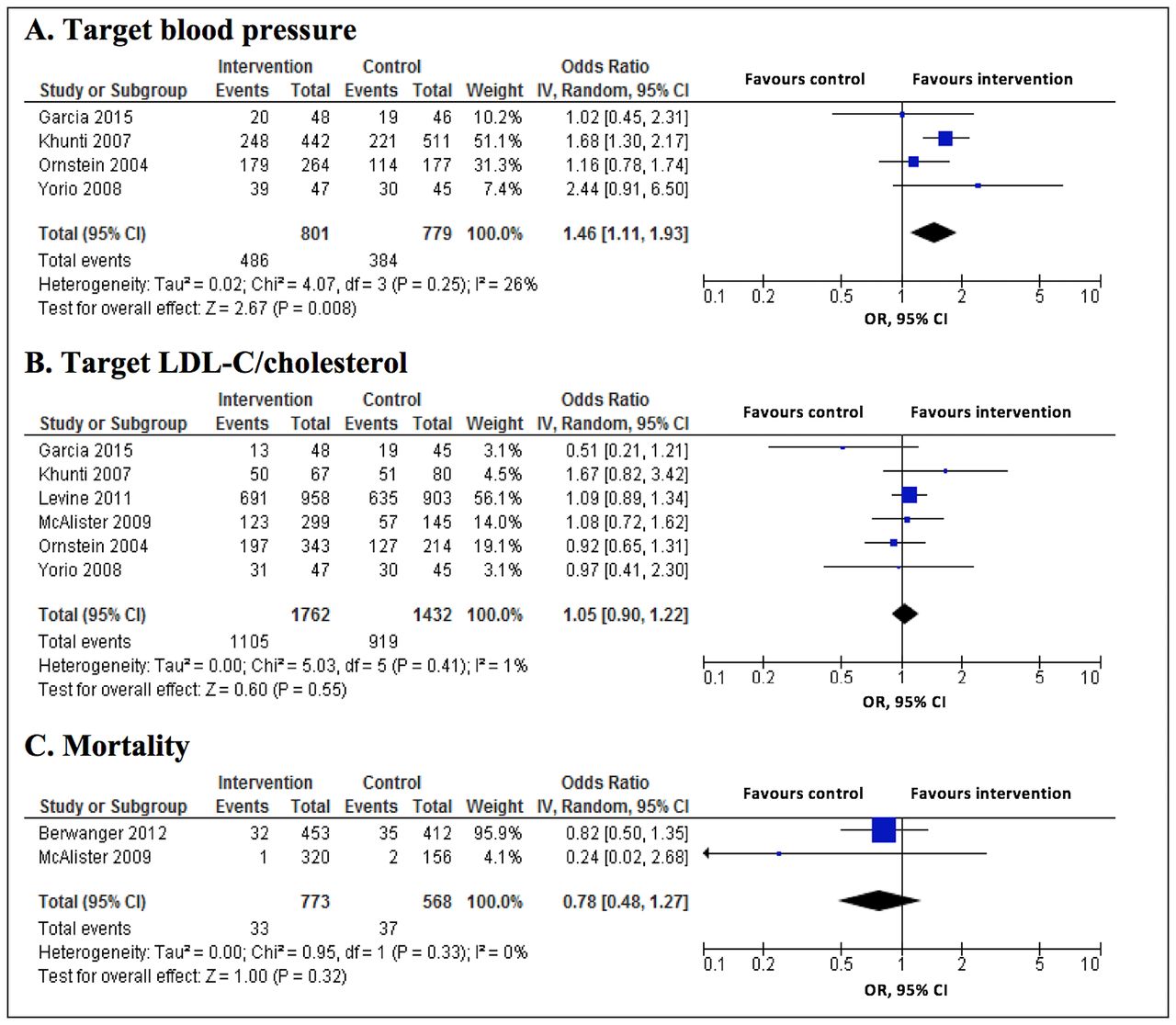
The interventions significantly increased the proportion of patients achieving target blood pressure (OR 1.46; 95% CI 1.11 to 1.93; P=0.008), but there was no significant difference in the proportion of patients achieving target LDL-C/cholesterol (OR 1.05; 95% CI 0.90 to 1.22; P=0.550), and in mortality rate (OR 0.78; 95% CI 0.48 to 1.27; P=0.320) between intervention and control groups. The evidence was of moderate quality for the secondary outcomes (figure 3 and table 3).

{kind=link}
{kind=link}
{kind=link}
Secondary outcomes of intervention vs control. LDL-C, low-density lipoprotein-cholesterol.
No substantial statistical heterogeneity was detected in our study outcomes (all eight I2 values were <50%) (figure 2 and figure 3). The publication bias was rated as no risk (in aspirin/antiplatelet agents, beta-blockers and statins/lipid-lowering agents) and unknown risk (in the other outcomes) (see online supplementary appendix D). In subgroup analyses, there was no significant difference in the effect of the interventions on prescribing guideline-recommended medications and patients’ health outcomes between subgroups with all P values for the interaction of >0.05. No subgroup analysis could be done for the composite of medications and mortality rate as there were only two studies available for each of these outcomes (see online supplementary appendix E). We did not perform sensitivity analyses excluding studies with high overall risk of bias because all included studies were rated as low risk. The findings of all outcomes did not change in sensitivity analyses when not adjusting for clustering effects (see online supplementary appendix F).
Discussion
Interventions to enhance prescribing guideline-recommended medications for patients with IHDs were of organisational or professional nature. The interventions significantly enhanced prescribing of statins/lipid-lowering agents, but not other medications. There was no significant association between the interventions and improved health outcomes, except for target blood pressure. The evidence was of moderate or high quality for all outcomes.
Why did the interventions not improve prescribing of most medications? The high baseline performance, especially of antiplatelet agents, might limit the scope for further improvement.45 47 49 50 53 59 The baseline measures were better than expected which may indicate ‘a rising tide phenomenon’, a metaphor for a secular upward trend, being a possible explanation of null results.60 In addition, an increased awareness of treatment recommendations derived from efforts by local organisations and reports documenting poor compliance with recommendations could contribute to this phenomenon.50 60 The Hawthorne effect may also explain the results. Extra attention by researchers and higher levels of clinical surveillance, equally present in treatment and control groups, may over-estimate response in both groups.61 As a consequence, the control groups improved their performance alongside the intervention groups in included studies.52 53 55–58 Furthermore, many other factors impact on prescribing including patients and resource constraints which were not assessed in the studies.31
What are possible explanations for finding effects on prescribing statins/lipid-lowering agents? First, there were more patients eligible for receiving statins/lipid-lowering agents than antihypertensive agents (beta-blockers or ACEIs/ARBs). Furthermore, statins/lipid-lowering agents are recommended to be prescribed for all patients with IHDs, regardless of their LDL-C level.3–8 Physicians tend to be more careful when prescribing beta-blockers because of concerns about their side effects.62 Physicians also possibly favoured other classes of medications to monitor patients’ blood pressure level and survival (eg, calcium channel inhibitors).62 It was surprising that the interventions had an impact on prescribing of statins/lipid-lowering agents, but not on LDL-C/cholesterol level. In contrast, interventions did not have an impact on prescribing antihypertensive agents, but target blood pressure improved. Whether or not adequate dosing had been achieved was not measured in the trials, but this has an effect on patients’ outcomes. For example, the benefits of more intensive therapy with statins have been established.63 Lack of patient adherence with medication could also be an explanation, but this was not measured in the trials. Patient adherence is reported to be better with antihypertensive agents than with statins.64 In addition, lifestyle modifications65 66 also contribute to patients’ clinical outcomes and may have played an important role in improving blood pressure control. More work is needed to disentangle the associations. In particular, because our analyses for blood pressure and LDL-C/cholesterol levels were based on a few studies only.
Our findings are consistent with previous systematic reviews28 29 reporting professional and organisational as the two main types of interventions to improve healthcare professionals' adherence to cardiovascular disease guidelines. Our study and a systematic review by Jeffery et al 28 showed only some significant improvements. A systematic review by Unverzagt et al,29 in contrast, showed that a provider reminder system, audit and feedback, provider education or organisational change were effective interventions. However, results are difficult to compare as we measured different outcomes. We analysed the improvement of prescribing for each medication separately while both review articles28 29 took all medication together. Moreover, we focused on patients with IHDs, whereas previous reviews28 29 included different cardiovascular diseases. Although programmes promoting guidelines such as the Guidelines Applied in Practice and Get With The Guidelines programmes also involving organisational and professional interventions demonstrated that it was possible to improve quality of care,67 the design of RCT is needed to confirm the improvement.
Several issues need to be addressed in our study. First, there were seven studies rated as having a high risk of other bias. Of these studies, six cluster RCTs50 52 53 56–58 had a high risk of recruitment bias. In those studies, patients were recruited after the clusters had been randomised and therefore, the knowledge of whether a cluster belonged to the intervention or control group could have affected patient recruitment. Farrin et al 68 showed this in a trial of low back pain randomised by primary care practice; a greater number of less severe participants were recruited to the ‘active management’ practices. However, we did not find significant differences in outcomes between RCTs45 49 51 59 and cluster RCTs.43 47 50 52 53 55–58 Second, there were some cluster RCTs47 50 53 56 58 which did not report the ICCs. We used the mean ICCs for corresponding outcomes reported in the other included studies.39 The sensitivity analyses without adjusting for clustering effects showed similar results. The heterogeneity became substantial for the outcomes of aspirin/antiplatelet agents, the composite of medications and target LDL-C/cholesterol. But overall, the sensitivity analyses confirmed the robustness of our findings. Third, we included studies of all types of interventions targeted at healthcare professionals in the meta-analyses. Subgroup analyses showed that there was no significant difference between subgroups of interventions (professional, organisational and professional plus organisational). But more detailed analyses, for example, on duration or intensity of the intervention, were impossible due to the limited number of studies. The length of patient follow-up varied across studies. This issue might increase the clinical heterogeneity of outcomes measured. Fourth, we included studies reporting patient-level outcomes, and excluded studies only reporting cluster-level outcomes (eg, hospital and practice performance scores).69 70 Fifth, we performed multiple statistical tests which increased the risk of type I error. Adjustment for multiple testing is debatable.71 In our study, three out of four primary outcomes were not significant, P value threshold adjustment would be too conservative. Finally, our review included only studies published in English and we did not search for grey literature. So we may have missed relevant unpublished or locally published studies.
Our results have several implications for practice and research. Eleven out of 13 studies come from North America and Europe, which limits the generalisability of our results to the rest of the world. There maybe a need to develop new interventions, especially for low-income and middle-income countries which have a rising burden of ischaemic heart diseases. There are some types of interventions such as financial and regulatory that have not been tested in this group.26 27 72 Selecting an intervention to enhance prescribing according to guidelines should be based on the local context. Interventions need to consider a range of barriers to change prescribing, including barriers related to patients, organisation of the healthcare system and resource constraints.31 Finally, improving guideline adherence may include strategies for improving clinicians’ awareness, agreement and adoption of guidelines. The cost-effectiveness of such interventions should also be evaluated.73–77
Conclusions
In conclusion, a number of organisational and professional interventions improved prescribing of statins/lipid-lowering agents and target blood pressure in patients with IHDs, but there was little evidence of change in other outcomes.
Acknowledgments
The authors would like to thank Alice Fuller, BSc, and Michael Moher, MD (Nuffield Department of Primary Care Health Sciences, University of Oxford, UK) for providing additional data from their study. None of these individuals was compensated in association with their contributions to this article.
References
Footnotes
Contributors TN had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: TN, KT. Acquisition, analysis or interpretation of data: TN, HQN, NNW, KT. Drafting of the manuscript: TN, KT. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: TN. Obtained funding: TN. Administrative, technical or material support: THN, TTP, KT. Study supervision: THN, TTP, KT.
Funding This study was supported by the Vietnam International Education Development via the Project of Training Lecturers with PhD Degree for Universities and Colleges in the period from 2010 to 2020 (Project 911).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.