Article Text

Abstract
Objective To assess the diagnostic accuracy of thermal imaging (TI) in the setting of focal consolidative pneumonia with chest X-ray (CXR) as the gold standard.
Setting A large, 973-bed teaching hospital in Boston, Massachusetts.
Participants 47 patients enrolled, 15 in a training set, 32 in a test set. Age range 10 months to 82 years (median=50 years).
Materials and methods Subjects received CXR with subsequent TI within 4 hours of each other. CXR and TI were assessed in blinded random order. Presence of focal opacity (pneumonia) on CXR, the outcome parameter, was recorded. For TI, presence of area(s) of increased heat (pneumonia) was recorded. Fisher’s exact test was used to assess the significance of the correlations of positive findings in the same anatomical region.
Results With TI compared with the CXR (the outcome parameter), sensitivity was 80.0% (95% CIs 29.9% to 98.9%), specificity was 57.7% (95% CI 37.2% to 76.0%). Positive predictive value of TI was 26.7% (95% CI 8.9% to55.2%) and its negative predictive value was 93.8% (95% CI 67.7% to 99.7%).
Conclusions This feasibility study confirms proof of concept that chest TI is consistent with CXR in suggesting similarly localised focal pneumonia with high sensitivity and negative predictive value. Further investigation of TI as a point-of-care imaging modality is warranted.
- Paediatric Radiology
- Chest Imaging
- Respiratory Infections
- Diagnostic Radiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Proof of concept suggesting that thermal imaging (TI) is a valid, innovative and inexpensive technology useful for diagnosing bacterial pneumonia.
Proof of concept suggesting that TI is a rapid means of diagnosing focal pneumonia in high-throughput settings.
Proof of concept suggesting that TI is a valid and innovative technology useful in diagnosing pneumonia in resource limited regions of the world.
As this is a proof of concept study, it does not have adequate power to be definitive and cannot replace chest X-ray for detecting focal pneumonia.
As this is a proof of concept study, limitations of the technology have not been fully discerned, and at present include adipose tissue and interpretation, but may include other concerns which will require higher numbers of patients enrolled.
Introduction
This study investigates the degree to which thermal imaging (TI) and chest X-ray (CXR) are concordant in detecting similarly localised focal pneumonia. Often a clinically challenging diagnosis, bacterial pneumonia remains a major cause of morbidity and mortality worldwide, particularly in under-resourced environments.1–3 Expert panels, including the WHO, have formulated algorithms to enhance clinical accuracy,4 typically focusing on aspects of the medical history and physical examination to determine the likelihood of bacterial pneumonia. Despite having these algorithms, CXR is generally performed to confirm the diagnosis in severe infections.5–16 If TI results are similar to CXR, it might substitute for CXR when CXR is not available. In resource-limited environments, where 2/3 of the world’s population has no access to diagnostic imaging,17 18 the potential use of TI in point-of-care screening could aid decision-making to treat for pneumonia.
Point-of-care imaging using ultrasonography to diagnose pneumonia is attracting interest.19 20 However, ultrasonography requires costly equipment and specific expertise for image acquisition and interpretation.
Anecdotal reports suggest that TI has potential for detecting pneumonia.21 22 These case reports and methodologies have not been subjected to systematic blinded assessment. In this initial proof of concept investigation, we compared TI to CXR in patients suspected of having acute pneumonia.
With recent advances in infrared technology and increasing use assessing home heat loss, low-cost thermal cameras have become available, currently costing as little as US$200–US$300 (www.flir.com). Installation of shielded radiographic rooms can cost hundreds of thousands of dollars. Portable X-ray units capable of performing CXR can cost as little as US$600–US$800 (www.dotmed.com). If uninsured, patient cost of a CXR in the US is US$200–US$400 or, if insured, a copay of US$10–US$50.23
For TI there are no additional costs beyond cost of the camera. TI cameras are portable and operate with rechargeable batteries. TI is essentially identical to taking a ‘snap and shoot’ photograph and can be done in seconds during the primary patient encounter without the camera physically contacting the patient. Digital storage and transfer of TI is simple, using a memory card in the TI device that can be uploaded to a computer.
This study presents a prospective comparison of TI to CXR using a commercially available thermal camera to determine the similarity of TI and CXR in the setting of possible focal pneumonia and thus proof of concept and feasibility of TI to detect focal pneumonia.
Materials and methods
Subjects
Participants came from the Emergency Department of Massachusetts General Hospital (Boston, Massachusetts, USA). On admission to the Emergency Department, adult patients and families of children who had CXR included for evaluation of pneumonia were approached to discuss study participation. Written informed consent and, when applicable, participant assent was obtained from all participants. Enrolment occurred Monday–Friday, 07:00–23:00 when research staff was available. Partners Human Research Committee approved the Health Insurance Portability and Accountability Act compliant study protocol (#2013P001247).
In an initial training set, subjects were excluded if they had chronic lung disease, congestive heart failure, prior chest surgery or immunosuppression. In a subsequent test set, these exclusions were not used. Patients had TI within 4 hours of CXR. Patients were male older than 28 days or female older than 28 days and younger than 8 years. After age 8, only males were included because of concerns for modesty.
Forty-seven patients were enrolled. The first 15, comprising the training set, were not included as a part of the study’s statistical assessment. These 15 cases provided a spectrum of results with 10 concordant for focal pneumonia, two concordant for no focal pneumonia and three discordant for pneumonia. The remaining 32 subjects comprised the test set. Analysis of the test set included 31 patients (28 men, three women), one patient had no usable thermal images. Patient age ranged from 10 months to 82 years (median=50.0 years, (25th, 75th) quartiles=(11.5, 60.5 years), with eight subjects ≤18 years and 23 subjects >18 years.
Imaging and interpretation
The radiologist interpreting CXR and TI (RHC) is an American Board of Radiology certified diagnostic radiologist and subcertified paediatric radiologist with 40 years experience.
CXRs were assessed in random order blinded to TI. If focal opacities were found, the lobe(s) were recorded. The lobes involved were precisely determined with posterior–anterior (PA) and lateral examinations. When only a portable anterior–posterior (AP) image could be obtained, the lobe(s) involved was determined by lung zone and presence/absence of silhouetting of the mediastinum. CXRs were taken in PA and lateral projections (n=19). If PA and lateral imaging could not be performed, because of clinical care requirements, a portable AP image was acquired (n=12).
TI of the chest were taken from the neck down, similar to CXR, with both posterior and anterior views whenever possible (n=29). If a patient was too ill to be positioned for two views, only one view was obtained. Depending on the patients’ condition and preferred position, one patient had a posterior view and one an anterior view. Oblique images were not obtained since TI interpretation depends on assessment of asymmetric heat distribution. TI were acquired with the commercially available FLIR i7 infrared thermal camera (www.flir.com). The subject was encompassed in the field of view; a ‘snapshot’ was obtained so the patient’s chest filled the field of view with the entire chest from side to side included from the level of the shoulders to bottom of the chest (or below). Patient to camera distance varied based on patient size. Subjects could be sitting or recumbent with the chest exposed. Clothing was removed from the chest prior to TI acquisition.
The camera used in this study has a resolution of 19 600 pixels detecting a temperature range −4°F to 482°F (−20°C to 250°C) with sensitivity to 0.1°C. Images filled the 2.8 inch LCD TI screen. TI were interpreted while displayed on a desk top computer at a size comparable to the size of the CXR, filling roughly 50% of the computer monitor screen. TI image size varies depending on the imaging device. TI stored in the camera’s memory can be uploaded to a computer and displayed at whatever size preferred.
TI were evaluated in random order blinded to CXR. Any area(s) of increased heat were recorded as upper, mid or lower lung zone, and identified as in the right or left lung (figures 1–3). Following initial assessment of blinded TI and CXR, to shed light on possible causes for TI/CXR discrepancies, cases with disagreement were reviewed in non-blinded fashion, using prior CXR when available.

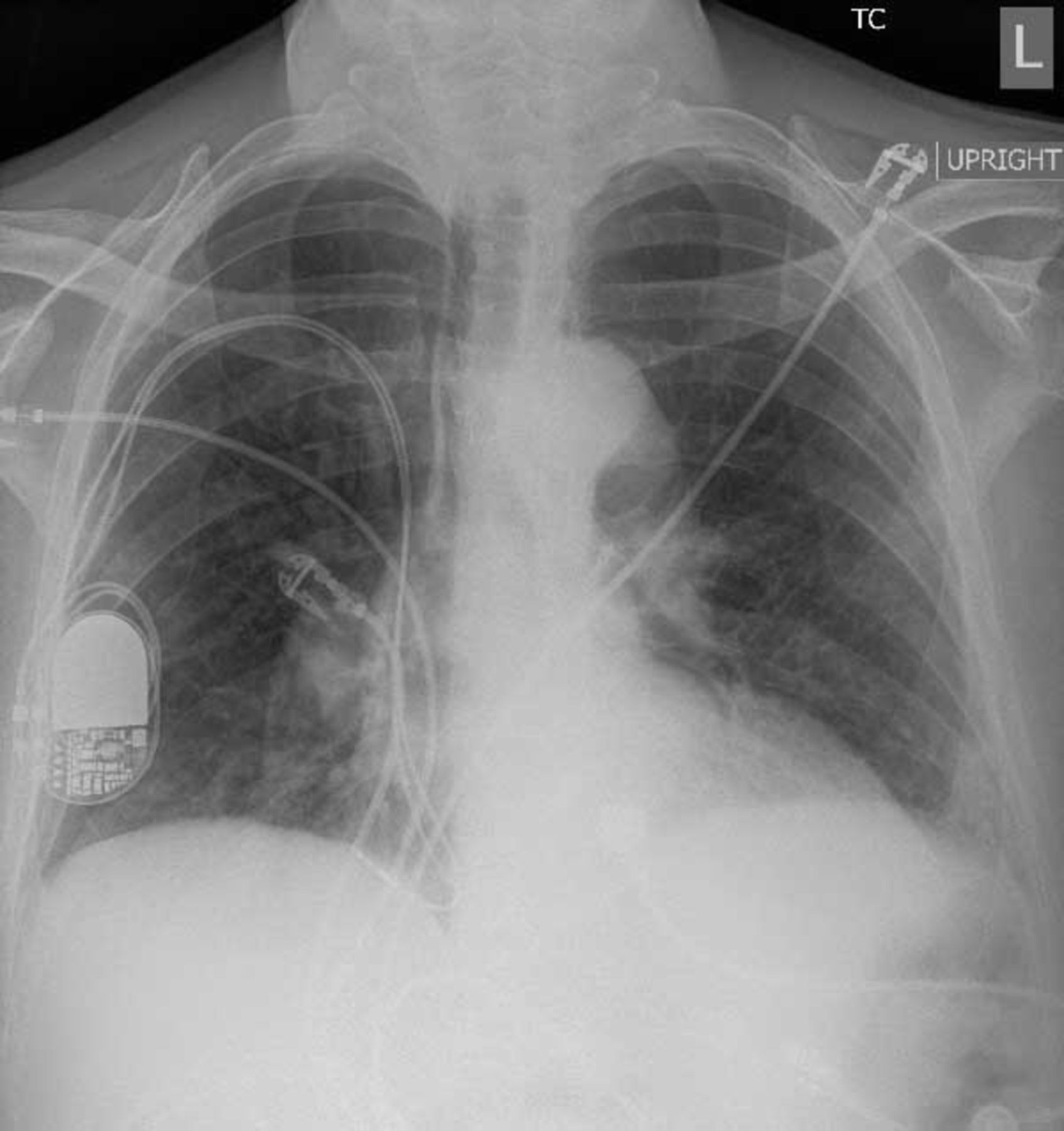
Chest X-ray shows an opacity in the right lung base consistent with pneumonia.

Thermal imaging obtained shortly after the chest X-ray (CXR) (figure 1). The image is taken from the patient’s back so that the patient’s right is on the viewer’s right. There is an area of increased heat (white area) in the right lung base concordant with the CXR.
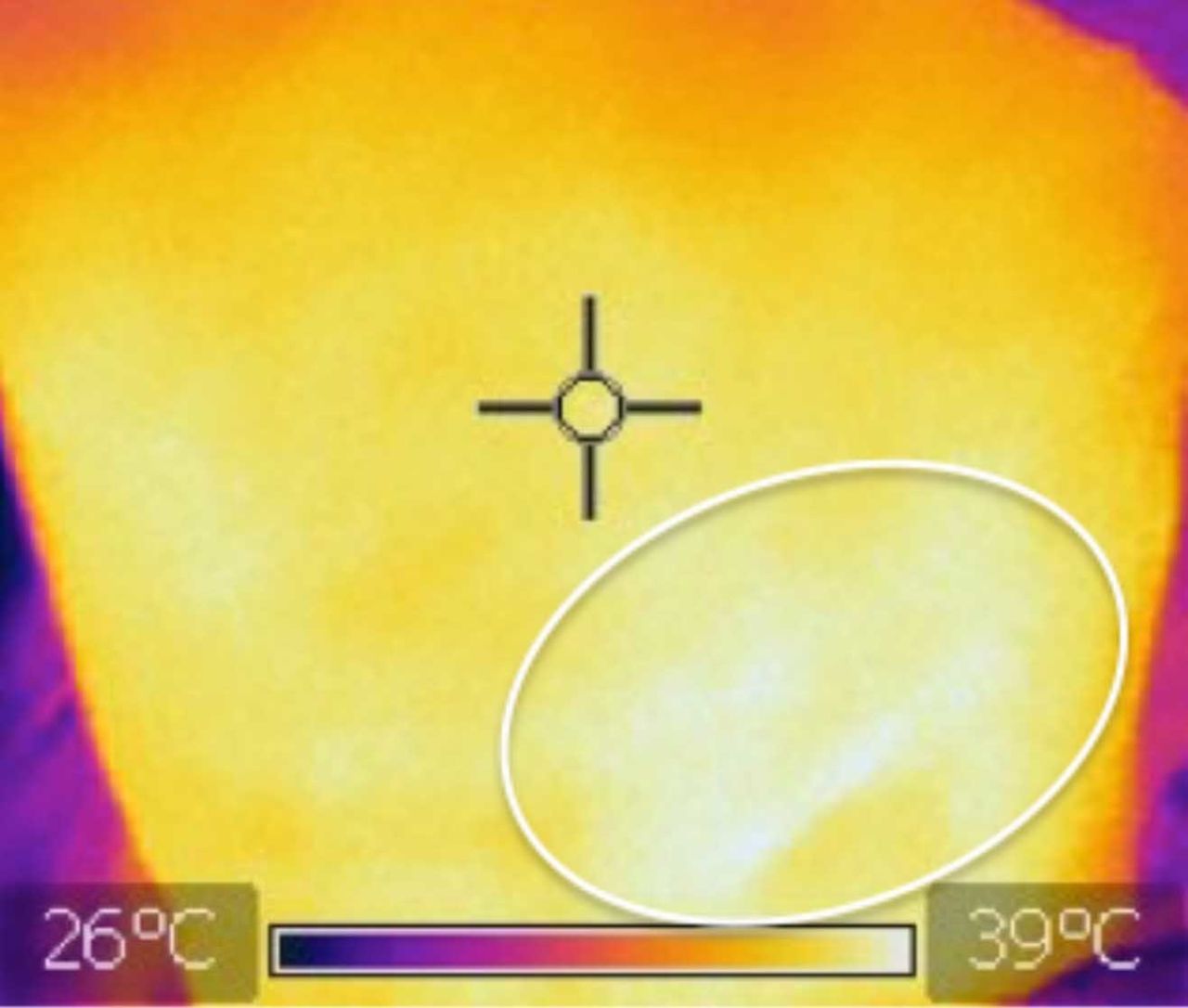
Same image as figure 2 with the area of pneumonia (white area) encircled by an oval ring.
TI is similar to nuclear medicine imaging in that it is not the precise size, configuration or margins that are of importance, but rather the temperature pattern with presence or absence of focal areas of increased heat, ‘hot spots’, that is informative for focal pneumonia. Heat emanating from the patient’s skin determines the TI image. Generalised skin temperature does not affect TI recognition of a hot spot. Since clothing recently removed from the chest might affect skin temperature globally but not focally, it is unlikely that previously removed clothing would affect recognition of a hot spot. Areas of symmetric increased heat were considered to represent normal variation in heat pattern and areas of increased heat over the neck, sternum, supraclavicular space, spine and axillae were determined to be normal on the initial 15 training cases. Abdominal heat pattern is similar to that of the chest without focal temperature changes relating to abdominal viscera. Unlike CXR, TI does not require that patients hold their breath. Therefore, minor patient motion will have minor, if any, effect on TI quality.
Statistical methods
Paired data were constructed for each patient with CXR the standard for disease and TI the test variable. Each image was dichotomised as normal or showing focal pneumonia. TI sensitivity, specificity, positive predictive value and negative predictive value and their respective 95% CIs were estimated. Agreement between CXR and TI (modelled as a binary outcome with agreement=1 and disagreement=0) and as a function of patient age and sex was assessed using simple logistic regression models, as well as 2×2 contingency tables with age dichotomised as >18 years for adults and ≤18 years for children. Fisher’s exact test was used to assess significance of correlation between age (or sex) and similarity between CXR and TI. Finally, despite the small sample, Cohen’s kappa was also used as an imperfect measure of agreement between the two modalities.24 25 A significance level of 0.05 was assumed.
Results
This study assessed the diagnostic sensitivity and specificity of TI using the chest x-ray (CXR) as the gold standard. For the overall cohort, five patients were identified as having focal pneumonia by CXR and 26 did not have focal pneumonia. For the paediatric cohort, there were two with focal pneumonia and six without, by CXR.
Eleven cases were TI positive and CXR negative (false positives). One case was TI negative and CXR positive (false negative).
Table 1 summarises the TI sensitivity, specificity, positive predictive value, negative predictive values and their corresponding 95% CIs.
Sensitivity analysis of thermal imaging (TI) assuming the chest X-ray (CXR) as the outcome parameter
The relationship between TI and CXR agreement with patient demographics was assessed using logistic regression models and simple contingency tables. There was no significant association between modality agreement and patient age (treated as a continuous variable or dichotomised as adult vs paediatric) or sex (age: P=0.3 (95% CI for the regression coefficient −0.01 to 0.004), OR=0.99 (95% CI 0.99 to 1.00)); sex: P=0.16 (95% CI −0.16 to 1.05), OR=1.53, (95% CI 0.85 to 2.85). Similar results were obtained when individual contingency tables for sex (P=0.54) or dichotomised age (>18 vs ≤18 years; P=0.53) were used. Despite its limitations in small samples,24 25 Cohen’s kappa was also estimated as an imperfect measure of agreement between TI and CXR (kappa=0.21, 95% CI −0.1421 to 0.5591). Even when CXRs were non-blinded, kappa=0.48 (95% CI 0.16 to 0.79). The wide 95% CIs are a further indication of the limitations of kappa to quantify agreement in small samples.
Since this is an exploratory proof of concept study, the sample size is not based on statistical power. In order to achieve a power of 0.80, with the conditions encountered in this study, a power calculation showed 138 patients would be required. Furthermore, the sample size required to detect even modest agreement quantified by kappa is n≥40 patients.
To investigate causes for TI/CXR discrepancies, cases with disagreement were reviewed in a non-blinded fashion, using prior and subsequent CXR (comparison images were not included in the blinded, original CXR assessments). This review of discrepant cases is not included in the study’s statistical analysis.
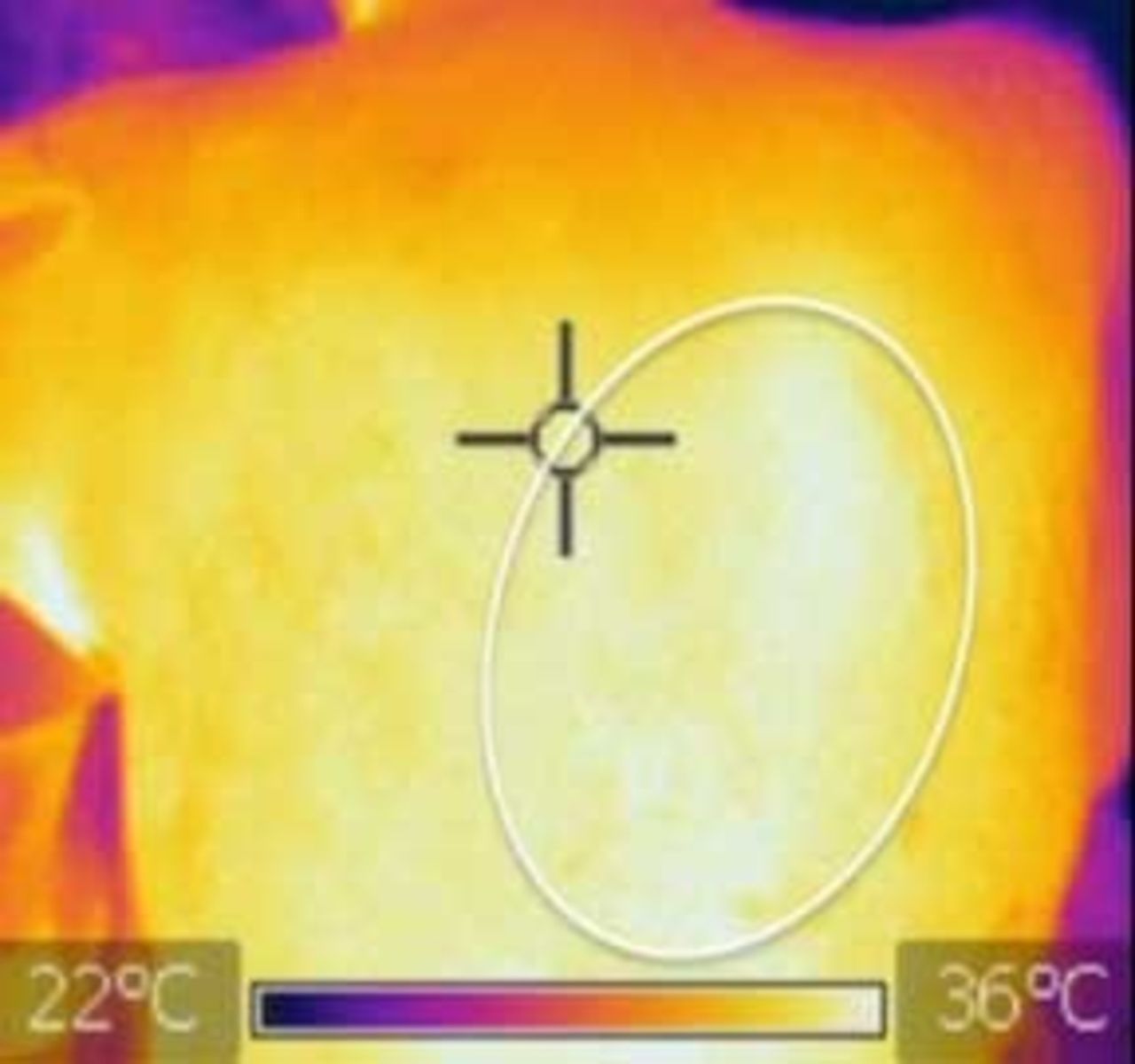
For the 11 false-positive TI cases, prior CXRs were available in only three cases. Each of these three cases had diffuse findings confounding CXR interpretation. One had diffuse changes of cystic fibrosis, one had changes of chronic obstructive pulmonary disease and one had low lung volumes. When CXR was reviewed with prior CXR, the CXR interpretation was changed to focal pneumonia (figures 4–6) concordant with TI (figures 7 and 8) in each instance. Follow-up images provided no additional information.

Portable chest X-ray taken in the Emergency Department during assessment for acute pneumonia reveals low lung volumes and what was assumed to be resultant crowding of pulmonary parenchyma in both lung bases medially. The interpretation at that time was that there was no acute pneumonia.
This chest X-ray (CXR) was performed 5 days before the CXR in figure 4. The lung volumes are comparably low, but the small opacity in the right infrahilar region on figure 4 is not present. This indicates that there was a pneumonia in the right lung base on the CXR in figure 4 rather than normal crowding of lung tissue.

Same image as figure 4 with the right infrahilar pneumonia indicated by arrows.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Same image as figure 7 with the area of pneumonia (white area) encircled by an oval ring.
For two other cases, knowledge of TI findings resulted in a change in the CXR interpretation. For one case, the CXR interpretation was changed to a faint opacity, consistent with focal pneumonia and in one case, there was the question of a very subtle opacity, both concordant with the TI images.
Three other CXRs had what appeared to be atelectasis in regions of TI hot spots. In light of the TI results, these areas of presumed atelectasis may actually represent pneumonia. These opacities on CXR were, in one case each, in the right upper lobe, left upper lobe and left lower lobe. Three of the 11 false-positive TI cases had no change in CXR interpretation. The one false-negative case had no change to TI or CXR interpretation. There were no tumours, pulmonary oedema or other abnormalities identified on CXR that might affect TI results. Non-blinded review produced no changes in interpretation of TI images.
Discussion
This study suggests that TI is sensitive and modestly specific compared with CXR in detecting focal pneumonia.
There currently is no experimental data assessing the mechanism of increased focal heat, as detected by TI, associated with focal pneumonia. The assumption is that the focal hyperaemia associated with focal inflammation, in this case pneumonia, produces focally increased heat. It presumably is this increased heat radiating from the site of pneumonia that is detected by TI. Consequently, an area of atelectasis which is not associated with hyperaemia, will not produce an area of focally increased heat.
It is focal increased heat that is the indicator of focal pneumonia on TI. Thus any bacterial organism (which organism cannot be determined) may be the culprit. Viral pneumonias are generally diffuse and do not typically generate a focal pneumonia. Some atypical pneumonias, such as mycoplasma, may have a focal consolidative component which might be detected as a hot spot. It has been reported in a case report that acute consolidative tuberculosis caused a TI hot spot but subacute tuberculosis did not.21 It is not the precise lobar distribution but rather presence or absence of a focal hot spot that is the informative aspect of TI.
The purpose of this study was to assess the sensitivity and specificity of TI, in detecting a focal consolidation, using CXR as the gold standard given its wide use for diagnosis of pneumonia,19 20 26–31 including studies assessing effectiveness of WHO clinical diagnostic criteria.31 Ultrasound is the only other point-of-care imaging procedure widely studied for diagnosis of pneumonia and in virtually all of its validation studies and it is compared with CXR.28–30 While clinical signs and symptoms have been used, collecting accurate data and correlation with the ultimate diagnosis of pneumonia is inconsistent.32 However, it is not the purpose of this study to assess the accuracy of imaging to detect pneumonia as compared with the clinical diagnosis. Ultimately, other methodologies such as inflammatory markers may play a role, but currently these are in relatively early stages of development.
Accuracy of CXR in determining the presence of focal pneumonia will vary depending on quality of imaging and experience of the observer, as is true for TI. Although CT has greater accuracy in detecting pneumonia than CXR,33 34 CT cannot be used as routine imaging for pneumonia because of concerns of radiation exposure and cost.31
There was only one false negative in the cohort of 31 patients with 11 false positives (sensitivity=0.80, specificity=0.58). Thus the ability of TI to accurately detect focal pneumonia (as determined by CXR), in this cohort was relatively high. For a screening test, this ability to not miss focal pneumonia is the most critical criterion. The higher rate of false positives would lead to either overtreating or further testing in a limited number of patients, which, although important, is a less critical issue.
The changes in CXR interpretation on non-blinded review of discrepant TI/CXR revealed the following. (1) TI had hot spots in cases where CXR findings were initially not definitive for focal pneumonia (n=5). For two, CXR diagnosis was confounded by pre-existing chronic lung diseases and in one by shallow inflation. For two others, the suggestion of focal pneumonia on CXR was too subtle for definitive diagnosis. (2) TI revealed hot spots in cases where the blinded CXR suggested atelectasis (n=3). This suggests that TI may be able to detect focal pneumonia in cases where pre-existing lung disease or imaging technique confound the diagnosis on CXR or when diagnosis on CXR is too subtle to be convincing (as possibly with early onset or resolving focal pneumonia). TI may be able to differentiate between focal pneumonia and atelectasis.
These findings suggest TI may be comparable to CXR in recognising focal pneumonia. Relatively low cost and portability of thermal cameras, some of which can be used with mobile phones, potentially enable TI as a point-of-care screening tool for focal pneumonia. Other advantages include minimal training to perform images, lack of ionising radiation exposure, off-site interpretation of digitised images and possible software interpretation algorithms. Lack of physical contact with the patient enhances infection control. Possible additional uses include following progression of disease in combination with other modalities such as respiratory rate and oximetry.
Limitations of TI include learning to interpret TI, presence of prior disease affecting TI and the possibility that increased adiposity may interfere with its accuracy.
Conclusions
This feasibility study confirms proof of concept that TI can demonstrate focal pneumonia. Therefore, these findings support further investigation with larger trials of patients that will be adequately powered to robustly assess the similarity between TI and the outcome parameter. This technology is potentially most useful in resource-limited environments where pneumonia is the second most common cause of death in young children and where CXR equipment and expert readers are unavailable.35 It also could be of benefit in high-throughput healthcare settings, such as emergency departments or busy doctors’ offices and rural areas where access to CXR is limited.
References
Footnotes
Portions of this material were presented at RSNA 2016, Chicago, Illinois, 1 December 2016.
LTW and RHC contributed equally.
Contributors LTW: conception and design of the study, acquisition of data and analysis, interpretation of data, and drafting the work and revising it critically. RHC: conception and design of the study, data analysis, interpretation of data, and drafting the work and revising it critically. WB: design of the study, acquisition of data and analysis, interpretation of data, drafting the work and revising it critically. TP: data analysis, interpretation of data, and drafting the work and revising it critically. CS: data analysis, interpretation of data, and drafting the work and revising it critically. MS: conception of the study, acquisition of data, interpretation of data, revising the work critically. KH: conception and design of the study, analysis of the data, interpretation of data, and drafting the work and revising it critically. PS: analysis of the data, interpretation of data, drafting the work and revising it critically. RGZ: conception and design of the study, data analysis, interpretation of data, and drafting the work and revising it critically. PH: conception and design of the study, interpretation of data, and drafting the work and revising it critically.
Funding The Bacca Foundation and the Consortium for Affordable Medical Technologies (CAMTech) (Fund # is 223707).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from the study. Data are available to any researcher who is interested in the data, and will be able to access it through Dyad and/or through correspondence with the contributing authors.