Article Text

Abstract
Objective Informed consent is central to ethical medical practice, but little is known about how the process takes place in clinical practice. Percutaneous coronary intervention (PCI) is a common revascularisation procedure. Studies report that patients overestimate benefits, forget the risks and are unaware of alternative treatments. The aim of this study was to describe PCI patients’ and cardiologists’ experiences of the informed consent process in acute care settings.
Design/setting/participants A qualitative study with a maximum variation sample of elective and acute PCI patients and cardiologists taking their consent, recruited from a district general hospital and tertiary centre. In-depth interviews were conducted, and consent discussions were audio recorded. Data collection, coding and theorising occurred simultaneously.
Findings Forty-one (26 male) patients scheduled for elective (20) or urgent (21) PCI and 19 cardiologists (5 female) participated. Despite diversity in patients’ experiences of informed consent, elective and acute patients experienced a common four-stage process of consent. Most patients made the decision to have treatment at PCI referral and took a passive role in the discussions we recorded. They recognised cardiologists as experts, trusted the medical system to ‘fix’ their health problem and were unaware of their role in the informed consent process. Informed consent discussions functioned as a formal ‘event’,enabling cardiologists to check patients’ understanding and enabling patients to access treatment.
Conclusions The configuration of services and patients’ perceptions of their role in informed consent underpin a mismatch between legal and ethical principles of informed consent and current practice. The variation in patients’ experiences of the current place of informed consent in service delivery represents a missed opportunity for cardiologists to work in decision-making partnerships with patients. In light of recent changes in the law, a new approach to informed consent is required.
- adult cardiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study provides a robust, in-depth account of patients’ and cardiologists’ experiences of the in-hospital informed consent process for percutaneous coronary intervention in England.
Findings can be used to inform service improvements with educational interventions to support the comprehensive implementation of professional and legal frameworks in practice.
Findings add a new perspective to current knowledge on this topic, which largely reflects an American viewpoint.
The study focuses on the in-hospital informed consent process, which does not fully account for earlier discussions that may have occurred.
Introduction
Percutaneous coronary intervention (PCI) (also known as coronary angioplasty) has become one of the most common medical procedures worldwide.1 PCI is a revascularisation technique which is used either electively, to treat angina symptoms in patients with stable coronary artery disease, or urgently, for those with acute coronary syndrome.2 A key advantage of PCI is that when successful it improves myocardial perfusion without the need for coronary artery bypass surgery which has a prolonged recovery period. Serious complications are uncommon, but death is one of them.3
Patients are required to give informed consent in advance of any medical procedure. Informed consent constitutes good medical practice,4 is a universal patient right5 and reflects key ethical principles.6 The partnership and collaboration between the doctor and patient in supported decision-making is central to this process. For consent to be valid it must be freely given by patients who are informed and deemed to have capacity. In being fully informed patients should understand the full range of treatment options including the risks, benefits, alternative treatments and the outcome should they decide to have no treatment. Although it should be presumed that a patient wishes to be fully informed about the risks and benefits, patients' specific information preferences should be respected and documented.7 While legal frameworks differ across countries, the recent judgement in Montgomery v Lanarkshire Health Board8 will have a significant impact on discussions about risk that are both fact and case specific during the informed consent process. Consent conversations will now need to demonstrate discussion about material risk, that is any risk that a ‘reasonable’ person, in the patient’s position, would consider important in making their decision about their treatment. 7
Studies that describe PCI patients’ perceptions about their treatment show that they tend to overestimate the benefits,9–11 forget the risks and are often unaware of alternative treatments,9 suggesting that treatment decisions may not be fully informed or that recall is poor. Theoretical models of the informed consent process acknowledge that informed consent can be perceived as a ‘single event’ or an ongoing ‘process’, with the latter perceived as being optimal.12 The ‘single event’ model is unlikely to foster a doctor-patient partnership that enables supported decision-making13 and such discussions often occur once the patient has already committed to surgery.12–14 Informed consent practice varies widely across hospitals and treatments,11 15 and the amount and quality of information provided to patients is inconsistent.16 The process is complex and often involves interactions with several health professionals. The features of such discussions, including how risk is explained, influence patients’ decision-making.17 18 The quality of the PCI consent process is influenced by individual and contextual factors such as a lack of time, patients’ unwillingness to participate in the process and the expertise of participating doctors.19
In summary, we know that the PCI informed consent process is complex and variable and could be improved. To identify how we can optimise informed consent for PCI we need to understand the experiences of those involved, in the context in which the interactions take place. Given this gap in knowledge, the aim of this study was to describe PCI patients’ and cardiologists’ experiences of the informed consent process in acute care settings. This is the first qualitative study that describes patients’ and cardiologists’ experiences of the PCI informed consent process.
Methods
Study design
A qualitative methodology was appropriate to explore how PCI informed consent took place.20 Principles of constructivist grounded theory were used to generate an understanding of the phenomenon.21 In-depth interviews were chosen as the most appropriate qualitative methods and these data were triangulated with consent discussions that occurred when the consent form was signed.
Sample, setting and recruitment
Following ethical approval we planned a series of in-depth interviews with a maximum variation sample of patients and cardiologists, recruited from two centres. We purposefully selected sites that differed in their service provision to provide a diversity of participant experiences; a district general hospital (<400 PCI procedures annually) and a tertiary PCI centre (<1900 PCI procedures annually). Participant recruitment was conducted sequentially across sites and continued until no new themes were evident in the interviews. All cardiologists at both sites were invited to participate by a researcher not involved in direct care provision. All eligible patient participants (<18 years of age receiving PCI electively or urgently for non-ST elevation myocardial infarction) were either sent study information in advance, or approached by a research nurse prior to giving informed consent. Patient participants were recruited purposively to ensure maximum variation with regard to characteristics which may have potentially influenced their experiences: age, gender and elective or acute treatment.
Data collection
All participating cardiologists audio recorded the informed consent discussion during which the consent form was signed, with participating patients. We then subsequently interviewed these patients and their cardiologists, using the consent discussion as a starting point for the interview. Participants completed a brief questionnaire (age, gender, procedure, occupation). For consistency one experienced postdoctoral researcher (JP), with training in qualitative research methods, who was not involved in care provision, conducted all semistructured interviews between April 2014 and March 2015. Patients and cardiologists were interviewed in a setting of their choice (hospital or home–patients only) with patient participants interviewed up to 14 days post-PCI. Semistructured interview guides were developed from existing literature and piloted with service users and cardiologists (see online supplementary material 1). Patient interviews explored not only the experiences of the consent discussion that was audio recorded but also their views of the wider consent process. Cardiologists recorded informed consent discussions in the clinical setting; consent forms were signed at this time. All interviews were audio recorded and professionally transcribed verbatim. Field notes and memos were recorded after each interview, including initial observations and reflections about emerging codes and concepts. These data informed the initial coding. Data analysis and participant recruitment took place simultaneously, to allow for the exploration of emerging concepts in keeping with constant comparison methodology.22 A group of five cardiology service users provided feedback on the findings.
Data analysis
Data analysis was conducted by JP, FA and JG. During this process transcripts were independently read and reread and all transcripts open coded by JP. The analytical process was progressed through a series of meetings with researchers, health professionals and service users. A coding framework was developed which was then systematically applied to the corpus of data. Contributors discussed their own personal views at the meetings and how these might influence the analytical process, to support reflexivity. A process of constant comparison characterised the analysis22 supported by qualitative software (NVivo V.10) to manage and retrieve data. This process allowed comparison of the informed consent process, behaviour and perceptions of the participants including deviant case analysis. The coding process was supported by written memos, which underpinned the development of higher level codes, themes, categories and the resulting core category. The methodology was reported using Consolidated Criteria for Reporting Qualitative Research (COREQ) criteria (see online supplementary material 2).23
Findings
Ninety-eight eligible patients and 22 cardiologists were invited to participate. Patient and cardiologist interviews lasted an average of 37 minutes and 42 minutes respectively. The pre-PCI consent discussion between patients and cardiologists lasted an average of 7 minutes. The final sample (see table 1) comprised 41 patients (42% response rate) and 19 cardiologists (13 consultant cardiologists and 6 cardiology registrars; 86% response rate). Informed consent discussions were audio recorded for 37 of the 41 patient participants. Thirteen acute patients withdrew before interview, nine changed their mind and four were not contactable.
Participant characteristics
We identified three themes and six categories describing the role of the informed consent discussion in patients’ decisions to have PCI treatment (table 2). These themes underpinned an overarching category, "I just want to be fixed". In summary, the informed consent discussion that took place in hospital did not facilitate partnership and supported decision-making. Instead it represented a confirmation exercise enabling doctors to encourage continued compliance with treatment, and for patients to access to treatment.
Themes and categories
Theme 1: the informed consent experience
This theme describes how the informed consent process takes place. During the discussions, cardiologists delivered and patients received information about risks and benefits and checks were made to establish whether patients were satisfied with this information. Patients’ experiences of the informed consent process varied according to their clinical presentation (elective or acute) and the hospital they attended, but the decision to have treatment, had in most cases, already been made before the discussion took place.
Category 1: diverse consent journeys
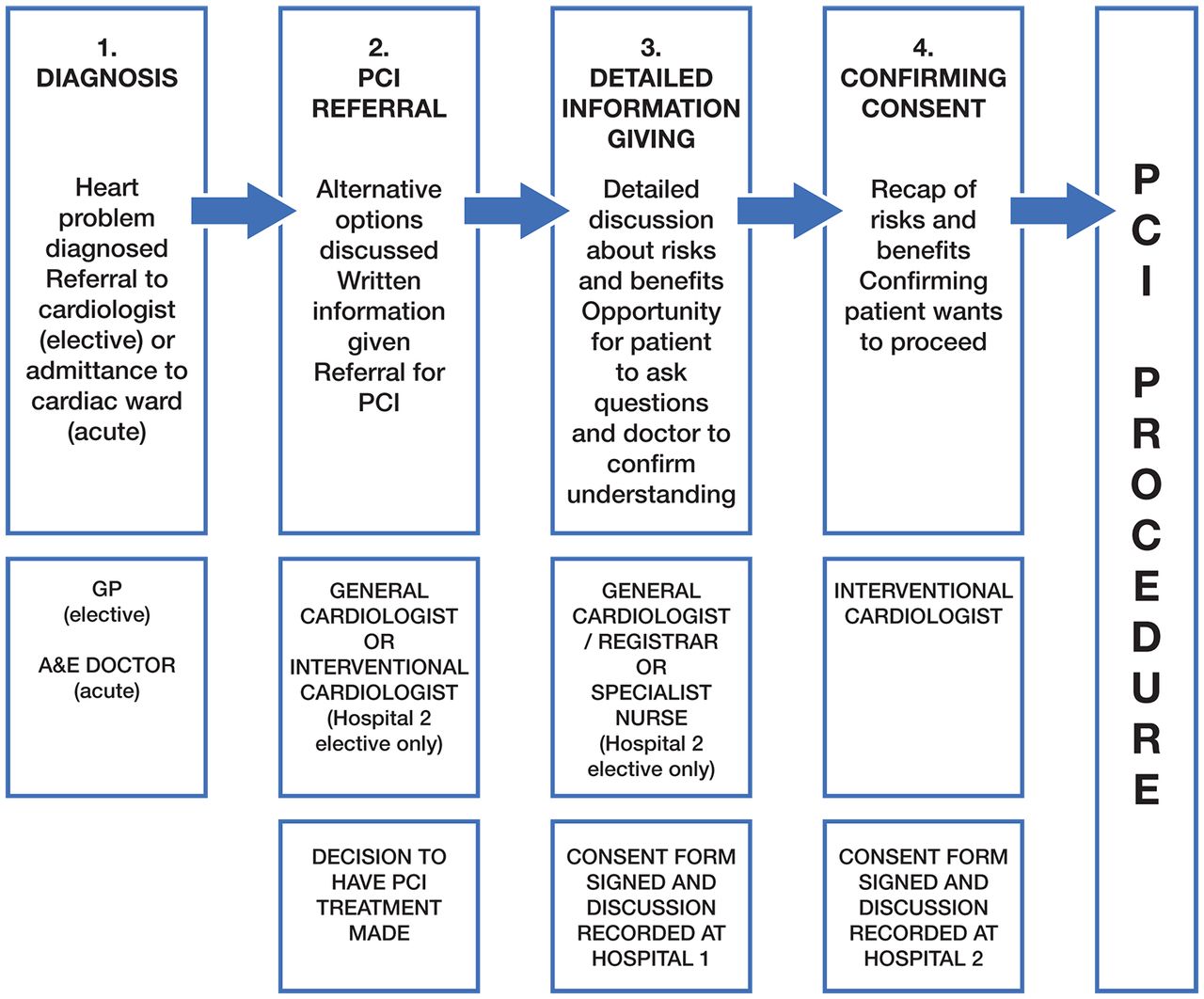
The pattern of service delivery varied by both procedure and site but all patients, regardless of acute or elective presentation described experiencing the four stages of consent shown in figure 1. There were three ‘types’ of patient journey: acute (admitted to hospital urgently with myocardial infarction and retained on ward for PCI treatment 12–48 hours later) (female acute patient 6, table 2); ‘treat and send’ (admitted to a non-PCI hospital urgently with myocardial infarction and retained on ward until transfer to Hospital 1 or 2 for PCI treatment 1–7 days later) (male 'treat and send' patient 33, table 2; and elective (referred to cardiologist by a general practitioner (GP) with angina symptoms and referred for elective PCI) (interventional cardiologist 3, table 2)

{kind=link}
The four-stage informed consent process experienced by acute and elective patients at both hospital sites. Key: A&E, accident and emergency; GP, general practitioner; PCI, percutaneous coronary intervention.
Patients accessing acute PCI treatment had their first contact (stage 1: diagnosis, fig 1) with a health professional either by ambulance, through accident and emergency, or were transferred from another hospital in the region. Patients had a preliminary consultation in a ward setting with a general cardiologist or in a minority of elective cases at one hospital, the interventional cardiologist, that would conduct the procedure (stage 2: PCI referral, fig 1) and it was at this consultation that the decision to have treatment was made. They were given written information about the procedure to read and this was followed by ‘detailed information giving (stage 3: detailed information giving, fig 1)’ discussion 2–24 hours later. The recorded discussion took place at this point at hospital 1. Practices varied regarding the time at which the consent form was signed. This could occur either during the in-depth discussion, or when consent was confirmed, just before treatment. Patients transferred from non-PCI hospitals (‘treat and send’ patients) waited between 1 to 7 days at the admitting hospital before a bed was available at the hospital with PCI services. The duration of the wait depended on the throughput of the hospital providing PCI services. The operating cardiologist recapped information immediately before the procedure and confirmed the patient wanted to proceed (stage 4: confirming consent, fig 1). The recorded discussion took place here at hospital 2.
Elective patients had a similar ‘journey’ except the process took place over a longer period and the settings were different. First contact was typically through a GP (stage 1: diagnosis, fig 1). Preliminary consultation took place in an outpatient setting and it was usually at this consultation that the decision to have treatment was made (stage 2: PCI referral, fig 1). Following this they were sent written information about PCI by post. Attendance at a pre-PCI clinic facilitated ‘detailed information giving’ (stage 3: detailed information giving, fig 1) which could be nurse-led, or doctor-led, with the latter including the completion and signing of the consent form. The recorded discussion took place at this point at hospital 1. As with acute PCI patients, the final part of the informed consent process was ‘confirming consent’ (stage 4: confirming consent, fig 1) conducted by the operating cardiologists just before treatment. The recorded discussion took place at this point at hospital 2. The consent form was signed at different stages at the two sites, either at the preop assessment, or immediately before the procedure. The patient experience from the first point of contact to the PCI procedure was thus influenced by a number of factors, including the amount of time between referral and treatment, the health professionals they had face-to-face contact with, whether they were admitted to a PCI treatment hospital in the first instance and the point at which the consent form was signed.
Category 2: information transfer
The breadth of risk information given to patients in the discussions varied considerably based on cardiologists’ judgements about what level of information was appropriate or comfortable for them to disclose, the amount of time available for the discussion and their knowledge of the patient. Most cardiologists balanced the risks of the procedure with a statement about the benefits (Interventional cardiologist 11 , table 2). Some gave patients a choice as to whether they wanted the information about risk whereas others felt duty-bound to disclose it regardless. In one case a patient requested not to be given any information about risk and the cardiologist respected this choice.
Risk was rarely individualised for patients even when they had multiple health conditions or had had previous coronary bypass surgery. There was variation in the degree of detailed information about risk given to patients (see table 3). At hospital 1, the consent forms were pre-printed with general risk information. This information was provided as it was usual practice for general and registrar cardiologists to take consent rather than interventional cardiologists. At hospital 2 where interventional cardiologists took consent, cardiologists documented risk calculations on the consent form by hand.
Variations in descriptions of risk by two different cardiologists (acute cases). P (patient); C (cardiologist)
General and registrar cardiologists (those taking consent from patients but not performing the intervention) did not always have the specialist knowledge required to individualise risk information (cardiologist registrar 2 , table 2) and interventional cardiologists were constrained by the short amount of time available for the discussion, particularly as some conducted the discussion immediately before the procedure. Some patients would rather not have known about risks (interventional cardiologist 6 , table 2); others wanted to know every detail. Some patients, who were admitted acutely, struggled to absorb information, probably due to the stress of their emergency admission to hospital. In contrast, some elective patients felt that knowing too much information early on in the process caused them anxiety. Most of the patients who did not want to know about the risks also did not question the doctor’s decision to refer them for treatment. Those who did wish to know about the risks were more proactive in their decision-making and recognised their role in the process. Regardless of the mode of delivery and content of the information given, it was clear that the value patients placed on the benefits of treatment clearly outweighed the risks.
Alternative options for treatment were not usually discussed in stage 4 ‘confirming consent’ (fig 1) of the informed consent discussions with elective or acute patients. When options were mentioned, they were acknowledged as potential options to eliminate rather than a realistic choice to patients (interventional cardiologist 4, table 2), indicating that the decision to proceed with treatment had already been made. Patients were satisfied with the informed consent process, including the amount of information they received. This included information booklets sent out to elective patients in advance and given to acute patients on the ward. Doctors were perceived by patients as a collective medical team. Patients were not concerned that they saw different health professionals at different stages in the process, apart from one incident where communication had failed between stages, leaving the patient with suboptimal information (male elective patient 9, table 2).
Theme 2: roles and expectations
The second theme, ‘Roles and expectations’ describes how patients and cardiologists define informed consent and patients’ expectations of treatment. In all recorded consent discussions, doctors were the information givers and decision-makers and patients accepted this. This was explained in the interview data by the ways in which patients and cardiologists defined informed consent and their roles within the process (i.e. doctor as expert, patient as passive) and their personal contexts that is, diagnosis (patients) and role within the cardiology team (doctors). Neither cardiologists nor patients defined the discussion at which the consent form was signed as a decision-making exercise. Rather, it was an opportunity for patients to be reassured about the need for treatment and for cardiologists to confirm patients’ understanding before the procedure.
Category 1: a ‘formal event’
Cardiologists defined informed consent as an ongoing process supporting patients’ decision-making, and as their professional duty. This was based on best practice guidance, patient-centred care and self-protection against litigation. Interventional cardiologists (those conducting the PCI procedure) saw their role as confirming consent with patients on the day of the procedure (interventional cardiologist 14, table 2). General cardiologists and registrars who took consent at preop assessment saw their role as taking consent on behalf of the operating cardiologist (general cardiologist 7, table 2). If they lacked expertise in interventional cardiology, they were reassured that consent would be confirmed with the patient by the operator on the day of the procedure. When interventional cardiologists took consent immediately prior to the procedure, having not met the patient before, they were forced to make a judgement about the information the patient had previously received.
Due to service delivery schedules, most interventional cardiologists did not meet patients until the day of the procedure (stage 4, fig 1) and there was an assumption that the ‘real’ informed consent had occurred prior to this. All cardiologists confirmed consent by clarifying patients’ understanding, usually by asking the patient if they had any questions. Once questions were answered, understanding was confirmed. Thus, the discussion during which the consent form was signed represented a checking exercise rather than supported decision-making between the doctor and the patient.
Patients interpreted informed consent as necessary for them to access treatment ("red tape") (male elective patient 5 and interventional cardiologist 1, table 2) and to protect the doctor against litigation. Patients were anxious about their health, focused on getting well and felt obliged to accept the treatment offered. A small minority of patients defined it as a decision-making exercise; in one case this was because the patient was given a choice between bypass surgery and PCI. Although this patient was given adequate information, he was not confident he had made the ‘right’ decision, indicating the importance of the doctor-patient partnership in decision-making.
Category 2: expectations of treatment
Elective and acute patients had different expectations of treatment based on the information they had been given, although both types of patients focused on the outcome of treatment, rather than the treatment itself. Elective patients focused on getting ‘back to normal’ and improving their quality of life with reduced angina symptoms and increased energy (female elective patient 21, table 2), whereas acute patients focused on staying alive and prevention of future heart attacks (male acute patient 11, table 2). A small number of patients who had undergone previous angiograms, felt reassured and knew what to expect (male acute patient 15, table 2). Patients were disappointed when their expectations of treatment were not achieved, and they were not ‘fixed’; for example in two cases where PCI could not be done and other options such as a bypass were being explored (male elective patient 8, table 2).
Theme 3: deciding to have treatment
This theme explains how patients’ perceptions of doctors and the availability of medical treatment influenced their decisions to have PCI treatment. Patients perceived medical authority to override their autonomy for decision-making and felt obliged to accept National Health Service (NHS) treatment recommended to them if they had the will to get well. This meant that the informed consent discussion was often an information delivery exercise rather than a supported decision-making discussion, as the decision had usually been made at the referral stage (stage 2, fig 1).
Category 1: ‘You’re the expert doctor’
Cardiologists took a leading role in discussions that occurred during the signing of the consent form; most were short, concise and standardised, with little involvement from the patient. Some lasted as little as 3 minutes when occurring immediately prior to the procedure. It was unusual for patients to ask questions even when prompted by the doctor. Patients who asked questions were motivated by contextual factors such as the impact of the procedure on caring responsibilities and their career (male patient 36 and interventional cardiologist 13, table 2). Patients distinguished levels of expertise between themselves and cardiologists. Most patients felt they did not need information about the procedure on the basis that they trusted the doctor, and that it was their role to listen but not to question (female elective patients 18 and 22, table 2). Patients and cardiologists valued the interaction during the discussion for different reasons. For interventional cardiologists it was important to meet their patients to develop a ‘rapport’ with them before the invasive procedure. For patients, having the procedure explained to them by a doctor was the authority confirming that the procedure would be carried out.
Category 2: a ‘Hobson’s choice’
Patients talked about having a ‘Hobson’s choice’ (a phrase describing the choice between accepting or refusing only one available option) to make about treatment. This was especially prevalent when the patient was told that a bypass and/or medication alteration were not options for them early on in the informed consent process, or when acute patients were told that it was necessary to prevent future risks of a heart attack (patients 20, 24 and 10, table 2). They acknowledged they were given adequate information to make a decision, but ultimately they felt that if they wanted to be well again, they had an obligation to accept the treatment recommended to them. Thus, most patients made the decision to have treatment at stage 2 (referral, fig 1). Interestingly, elective and acute patients both felt this, although the outcome of the elective procedure was solely symptom improvement rather than the prevention of future heart attacks. This indicates that when the in-depth discussion and consent form signing occurs at stages 3 or 4 (fig 1), the decision to have treatment has already been made. Some cardiologists believed that elective patients were more likely to have made the decision to have treatment before the discussion than acute patients, given the longer duration of time they had to consider.
Core category: ‘I just want to be fixed’
The informed consent discussion was part of a four-stage process of informed consent taking place either at the patient’s preop assessment (elective), or immediately before the procedure (acute). Patients’ journeys prior to the consent discussion involved discussions with a range of different health professionals but varied based on symptom presentation and the hospital attended. In most cases the discussions we recorded did not support decision-making as the decision had already been made at stage 2 (PCI referral, fig 1). Rather, discussions acted as a formal event to check patient understanding for cardiologists and as access to treatment for patients. Patients wanted to be ‘fixed’, trusted the medical profession and felt obliged to accept the treatment offered. Cardiologists (particularly those taking consent immediately before the procedure) had rarely met patients prior to the discussion. This meant they had limited time with, and knowledge of, patients and had to make assumptions about the information patients had been given prior to the discussion. This was particularly difficult when dealing with ‘treat and send’ patients from another hospital as cardiologists were unaware of earlier interactions and discussions they may have had.
In general, patients were passive in decision-making during the consent discussions we recorded as they believed they had no other choice, trusted medical staff to ‘fix’ them and ultimately had already made the decision to have treatment. This underpins the overall theory that the discussions we recorded (when the consent form was signed) functioned as a pre-treatment gate-keeping exercise for both parties. Such discussions enabled the ‘fixing’ of the patient but decision-making takes place at the earlier 'referral' stage.
Discussion
Summary
Our findings show that patients had a variety of encounters with health professionals before meeting the operating interventional cardiologist immediately before the procedure. Most had already made the decision to have treatment by this point after reading written information given to them on the ward (acute), or sent to them by post (elective), and having had a referral discussion with a cardiologist. Patients recognised cardiologists as experts and trusted the medical system to ‘fix’ their health problem. Most were typically unaware of their role in the consent process and had limited autonomy and participation in the consent discussion that occured when the consent form was signed. This informed consent discussion functioned as a formal ‘event’ enabling cardiologists to check patients’ understanding and enabling patients to access treatment.
Strengths and limitations
This study builds on the limited qualitative research available on informed consent for PCI12–14 19 and adds a new perspective to current knowledge on this topic as earlier studies have largely reflected an American viewpoint.9 10 12–14 17 18 Our study is original because of the triangulation of data from ‘real’ informed consent discussions together with in-depth interviews with participants. Our model of the informed consent process adds to, and extends on, existing yet dated research,12–14 and is grounded in the reality of the English practice setting. The qualitative nature of the findings may limit transferability to other sites but the triangulation of methods supports the trustworthiness of the study findings. Informed consent is a universal patient right and a process that occurs globally for all invasive procedures. Accordingly it is likely that findings will have application across other healthcare settings in which informed consent is required. We only directly observed one part of patients’ informed consent journeys (the signing of the consent form) and we relied on patient and cardiologist reports of earlier discussions and the overview of the consent process. Furthermore, although this was unknown at the time of data collection, the consent discussions were recorded at different points in the consent journey at the two sites. Thus, further research is needed to explore all stages of informed consent to determine whether the current service delivery model supports patients to make fully informed decisions about PCI treatment. Although cardiologists were asked to conduct the informed consent discussions as per standard practice, the audio recording of consultations could affect the nature of the consultation thereby introducing potential bias.
Comparison with existing literature
Our model of the in-hospital informed consent process, based on patients’ and cardiologists’ accounts, supports an earlier published model.12 However, our findings show that the first four stages of Lidz and colleagues' (establishing, responsibility, defining the problem, setting goals for treatment and selecting an approach to treatment) take place in the PCI referral consultation, and patients made the decision to have treatment at this point. Given that previous research has shown that how cardiologists present information has a strong influence on patients’ perceptions of PCI treatment,17 18 exploring what happens in these initial discussions as part of the informed consent process is vital. In the discussions we recorded, alternative options for treatment were rarely mentioned. Although they may have been mentioned in previous discussions patients had with other health professionals, patients were not always reminded of this before signing the consent form. Other evidence suggests that PCI patients are not always aware of alternative treatments9 and that cardiologists’ perceptions of the benefits of PCI are more optimistic than the evidence available, with PCI being the preferred treatment despite prognosis.24
Risk information given to patients was variable across discussions as shown elsewhere15 16 but because of its placement in this discussion, it did not influence patients’ decisions to have treatment. To confirm understanding before consent, cardiologists asked patients if they understood the information given and usually gave them the opportunity to ask questions. Patients rarely asked questions and this passive role in decision-making could explain why patients in studies of informed consent for various surgical procedures often have difficulty recalling information.25 26 Passivity in decision-making (ie, feeling they had 'no choice’) was underpinned by threatening symptoms, angina pain (elective patients) or a (NSTEMI) heart attack (acute patients) and a desire to get well. Patients had faith in the medical profession to ‘fix’ them, and saw PCI treatment as their only option. Other studies have reported that patients see PCI as a ‘fix’27 and are somewhat reluctant to participate in decision-making discussions. Moreover informed consent discussions studied in other settings, such as non-emergency surgical procedures have been reported to function as an interaction that confirms rather than facilitates supported decision-making. .19 When patients see only one realistic option in a health decision, the collaboration envisioned in the literature on supported decision-making is probably unrealistic.28
Implications for research and practice
Our findings, and others’19 illustrate that service delivery and time pressures are key barriers to shared decision-making in informed consent discussions. It is concerning that issues pertinent 20 years ago in Lidz and colleagues’ research,12–14 could continue to jeopardise the quality of informed consent. Detailed information provided to patients often comes after the decision to proceed with treatment has been made and the patient has committed to the treatment thereby reflecting an ‘event’ rather than a ‘process’ model of consent. While this satisfies legal requirements, it does not foster supported decision-making.12–14 We have identified a four-stage consent process underpinning patients’ otherwise diverse informed consent experiences. We have shown that patients sometimes make decisions to have treatment before having an in-depth discussion and that risk information varies in presentation across sites. Further research is needed to understand the context in which these decisions are made at the PCI referral stage, to ensure that opportunities for supported decision-making are optimised. Educational resources for patients and health professionals are needed to raise awareness of their roles in supported decision-making. Research has shown that decision-making processes are improved when practitioners are motivated and perceive that it will have an impact on the clinical process and patient outcomes.29 This is vital as the roles and relationships between doctor and patient can shape the behaviours and attitudes of patients, and support or discourage them to engage in their healthcare.30
Conclusions
Research has shown that the process of informed consent is fraught with limitations regardless of country and setting. Informed consent is defined as a process to enable patients to make informed decisions about their treatment, yet our findings suggest that in the context of PCI the process acts as a formal event to check understanding and enable access to treatment rather than to support decision-making. Patients' decisions to have treatment are largely based on trust and obligation. Our process model of informed consent builds on, and extends, existing research and indicates that cardiologists may unintentionally support patients to be passive, rather than active, in the decision-making process. The configuration of services and patients’ perceptions of their role in informed consent underpin a mismatch between legal and ethical principles of informed consent and current practice. In light of the Montgomery case,8 the emphasis of informed consent has shifted away from doctors’ judgments about what to disclose, to patients’ judgments about what they want to know. In a time of economic restraint in the NHS we need to find ways, through education, to ensure that patients are supported to make decisions about their care. A new approach to informed consent is required. Educational interventions to support decision making have the potential to influence practice internationally. We have focused on just one stage of the informed consent process for PCI. Further work is needed to explore the link between supported decision-making and informed consent through all stages of the consent process to identify strategies for service improvement.
Acknowledgments
The authors thank Mr Keith Marshall, Mr David Openshaw and the team of service users for their invaluable input;Mrs Judith Wright and Mr John Humphreys for research support and Dr Alison Morton who contributed to the development of the funding application.
References
Footnotes
Contributor JP collected the data, led data analysis, drafted the paper, finalised this version and is accountable for all aspects of the work.
JG and JH contributed to the design of the work and data analysis, provided critical comments on drafts of the paper, approved the final version and is accountable for all aspects of the work.
DC contributed to the design of the work, provided critical comments on drafts of the paper, approved the final version and are accountable for all aspects of the work.
FA conceived the idea and led the design and funding application, contributed to data analysis and to writing the paper, approved the final version and is accountable for all aspects of the work.
Funding This paper presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit (RfPB) Programme (Grant Reference Number PB-PG-0712-28089).
Disclaimer The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. This report contains anonymised excerpts from interviews and discussions conducted during the research.
Competing interests We have read and understood BMJ policy on declaration of interests and declare that we have no competing interests.
Ethics approval This study was approved by Yorkshire & the Humber Research Ethics Committee (Ref: 13/YH/0418).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Patients did not give consent for data to be shared beyond the research team.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected theseerrors and the correct publishers have been inserted into the references.