Article Text

Abstract
Introduction Gout is increasing despite effective therapies to lower serum urate concentrations to 0.36 mmol/L or less, which, if sustained, significantly reduces acute attacks of gout. Adherence to urate-lowering therapy (ULT) is poor, with rates of less than 50% 1 year after initiation of ULT. Attempts to increase adherence in gout patients have been disappointing. We aim to evaluate the effectiveness of use of a personal, self-management, ‘smartphone’ application (app) to achieve target serum urate concentrations in people with gout. We hypothesise that personalised feedback of serum urate concentrations will improve adherence to ULT.
Setting and design Primary care. A prospective, cluster randomised (by general practitioner (GP) practices), controlled trial.
Participants GP practices will be randomised to either intervention or control clusters with their patients allocated to the same cluster.
Intervention The intervention group will have access to the Healthy.me app tailored for the self-management of gout. The control group patients will have access to the same app modified to remove all functions except the Gout Attack Diary.
Primary and secondary outcomes The proportion of patients whose serum urate concentrations are less than or equal to 0.36 mmol/L after 6 months. Secondary outcomes will be proportions of patients achieving target urate concentrations at 12 months, ULT adherence rates, serum urate concentrations at 6 and 12 months, rates of attacks of gout, quality of life estimations and process and economic evaluations. The study is designed to detect a ≥30% improvement in the intervention group above the expected 50% achievement of target serum urate at 6 months in the control group: power 0.80, significance level 0.05, assumed ‘dropout’ rate 20%.
Ethics and dissemination This study has been approved by the University of New South Wales Human Research Ethics Committee. Study findings will be disseminated in international conferences and peer-reviewed journal.
Trial registration number ACTRN12616000455460.
- Gout
- Urate
- Adherence
- Self-management E-health Applications (apps)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The study tests an app designed with input from people with gout to enhance adherence to urate-lowering therapy.
The intervention delivers personalised feedback on achievement of target serum urate concentration.
Serum urate concentration is a very good surrogate for the likelihood of future gout attacks.
Not all people use apps.
A large number of participants need to be recruited to provide sufficient power to demonstrate a relevant effect size.
Background
Gout is increasingly prevalent and its incidence is rising. It afflicts 7% of men in the UK over 65 years and is the most common inflammatory arthritis in men, affecting 1%–2% in Western countries.1–5 Australian research indicates that gout is a significant and an increasing problem, with at least 1.5% of the general population affected.6 Further complicating management, there is a high incidence of comorbidities recognised in gout patients especially insulin resistance and diabetes, heart failure, hypertension and chronic kidney disease.4 7
Gout is a chronic disease triggered by the crystallisation of urate within joints, leading to inflammation, painful flares and eventual joint damage and destruction.5 8 Individuals who suffer acute attacks of gout recurrently endure debilitating pain, disruption of their life and significant costs.9–14 Gout results from excessive accumulation of urate due to a combination of genetic and lifestyle factors with the latter including diet, alcohol and smoking habits.5 15 Recent evidence indicates that elevated urate is an independent risk factor for accelerated cardiovascular and renal disease.16–19 However, if urate concentrations in the blood are reduced to ≤0.36 mmol/L, attacks of gout can be eliminated and the risks of kidney disease and possibly premature cardiovascular disease reduced.20 Existing urate-lowering therapies (ULT) are relatively safe and effective in reaching these target serum urate concentrations. The predominately prescribed ULT is allopurinol which works via inhibiting the synthesis of urate. Probenecid is an alternate ULT that enhances the renal clearance of urate, however, this is rarely used. More recently available is febuxostat that also inhibits the formation of urate.21
Poor adherence to long-term ULT is likely to be the most important contributor to the suboptimal outcomes experienced by patients with gout.22 Medication non-adherence is substantial in patients with gout, with studies consistently reporting that less than half of patients are adherent with treatment.23–26 Recent research suggests that non-adherence may be worse in gout than in any other chronic disease.27 Many reasons for non-adherence have been identified including limited knowledge about the causes and consequences of gout, lack of understanding about the different therapeutic approaches, uncertainty about therapeutic options to take if an attack occurs, insufficient appreciation of the importance of adherence to ULT, confusion regarding contributions of diet and lifestyle to gout and stigma associated with the diagnosis.23 25 26 28 In many patients with recurrent gout attacks, the adherence standard required is demanding, as ULT needs to be taken every day to avoid a recurrence. An important factor that impinges on adherence during the early months of therapy is a paradoxical increase in the risk of acute attacks even though serum urate concentrations are falling. The natural reaction of patients is to stop the therapy if not forewarned. Not surprisingly, patients can quickly lose confidence in their ULT.23 Fortunately, the risk of acute attacks can be significantly lowered during ULT initiation by taking an additional medicine as prophylaxis against acute attacks, such as regular, low-dose colchicine or non-steroidal anti-inflammatory drug.29 Additionally, it is likely but not yet finally established, that commencing ULT with a low dose and increasing the dose at 2–3 week intervals will lower the risk of a hypersensitivity reaction to allopurinol but also the risk of an acute attack.5 30 The key message for patients and their doctors is to continue taking ULT every day during this period even if an attack occurs.
There is accumulating evidence to suggest that electronic aids including mobile phone applications (apps) can improve adherence to preventative and therapeutic interventions including medications and lifestyle practices in chronic conditions such as diabetes, hypertension, mental illness and also arthritis.31 32 Apps are an increasingly accessible option via smartphones and tablets. There is also the potential to incorporate personalised feedback against targets such as adherence to medicines into apps. An attractive option for patients with gout is to provide feedback regarding their urate concentrations and whether target concentrations have been achieved, given the close correlation between these values and the risk of attacks of gout.20 Healthy.me is an app for patients developed to improve their health outcomes through better self-management. Research using this app has shown that personally held information improved health decision-making, uptake of therapy and organisation of health-related tasks.33 34 Users also valued social interactions and peer support provided by this app. Yet there are too few rigorous, controlled investigations of the effectiveness of such consumer electronic health (eHealth) applications.35 36 Also, the few apps available for self-management for patients with gout had multiple limitations and had not been tested in patients for effectiveness.35 Gout, with its high prevalence and impact despite the availability of proven effective therapy is a good target for enhancing patient self-management with a purpose built app. This study aims to test the effectiveness and cost-effectiveness of an app to enhance self-management in gout patients in primary care.
Aim
The aim of this study is to evaluate whether the use of an app that provides personal feedback and alerts to patients with gout to take their medication (intervention app) in addition to standard care, will significantly increase the proportion of patients reaching a target serum urate ≤0.36 mmol/L at 6 months compared with those using a control app with limited features (gout attacks diary only), which is close to standard care. The duration of the study will be 12 months.
Methods
Study design and recruitment procedures
This 1-year study is a prospective, clustered by primary care practice, randomised, controlled trial. The recruitment of general practitioner (GP) practices and patients with gout from the practices is presented in figure 1. GPs will be recruited from a list of practices in Sydney and rural centres in New South Wales Australia using GP networks, e-mail, direct mail, newsletters and telephone to advertise the study to GPs. Specifically, primary healthcare networks (PHNs) that are federally funded and in NSW are geographically aligned with the 15 hospital networks will be approached to publicise the study. PHNs work with primary healthcare providers including GPs to increase efficiency and effectiveness of medical services and improve coordination of care with the hospital networks.

Patient recruitment and study timeline. ED, Emergency Department; GP, general practitioner.
Inclusion criteria for GPs to participate in the study will be that they use electronic patient records and prescribing systems and have seen patients with gout in the past year. Once a GP has consented to participate, their practice will be randomised, using a pre-prepared, randomisation sequence and designated as ‘intervention’ or ‘control’ practice. Any patient enrolled via that practice would be similarly designated. All GPs in that practice will be approached to participate. Each participating GP will be asked to identify more people with gout. Patient inclusion and exclusion criteria are presented in table 1.
Patient inclusion and exclusion criteria
Patients with a diagnosis of gout by their GP, either new or a flare-up of previously diagnosed gout, who have experienced at least two attacks of acute gout in the previous year will be invited by their GP to participate in this study. Patients may already be taking ULT or be a candidate for restarting or commencing ULT (table 1).
Additional patients with possible or proven gout may also be identified via community pharmacies, emergency departments, specialist rheumatologists or consumer groups for example, Arthritis Australia, who are aware of the study. If these patients are willing to be considered for study entry they will be asked to contact the study personnel who will prescreen them via phone for potential suitability for inclusion. If apparently eligible, the study personnel will ask the patient’s GP if they are also willing to consent to participate in the study and identify patients with gout to be invited to the study. Once the consent is obtained, the participating GP will be randomised to either an intervention or control practice and requested to recruit patients for the study. The apparently eligible patient and subsequently recruited patients (if any) will be allocated into the same intervention or control group as the participating GP. The patients will be screened against inclusion and exclusion criteria and formally invited by their GP to consent to participate.
After giving informed consent, patients in the intervention and control groups will be commenced on or continue ULT and will be treated as is customary by their GPs. We expect to begin enrolment of participants in October 2017.
Randomisation
GP practices will be randomised by an independent researcher to either intervention or control group with a 1:1 allocation using random block size of 2 or 4 and computer-generated randomisation sequence. After the study personnel have obtained consent from patients recruited from the participating GP practices, the independent researcher will send the patients an e-mail containing a link to install either the intervention app or the control app on their smartphone or tablet. Neither GPs from the participating practices nor the participating patients will be informed of whether the patients are in the intervention group or control group although each patient can see what their app contains and each GP will receive a description of contents of the app provided to their patients. Two researchers, who will independently conduct data analyses, will be blinded to group allocation to minimise bias.
Gout-specific eHealth self-management app (Healthy.me Gout)
The intervention group will be provided with access to the Healthy.me app tailored for the self-management of gout. Healthy.me is a self-management eHealth app available on smartphones and tablets that contains features to help patients manage their chronic diseases. It has been designed and validated in a two-group, parallel, randomised controlled trial as effective in increasing consumers’ vaccination rates.33 34 The app has been tailored to promote effective self-management of gout and long-term adherence to ULT. The app was developed, using dimensions of the Health Belief Model: perceived susceptibility, perceived severity, perceived benefits and perceived barriers.34 In addition, input provided by patients with gout in focus group discussions informed the development of the app.36 While education materials from the app raise awareness of consequences of uncontrolled gout, susceptibility to gout attacks when serum urate concentrations are high, and the importance of keeping a low-serum urate level, the key feature of the app, ‘Uric Acid Tracker’, is designed to provide personalised feedback on susceptibility to and severity of gout by presenting individual patients’ serum urate levels and gout attack data on a graph. This personalised feedback will enable the patients to relate their high-serum urate levels to the occurrence of gout attacks (perceived susceptibility and severity) and recognise attack-free benefits of ULT adherence behaviour when their serum urate is consistently low. Low medication adherence is a major barrier to keeping gout under control,23 and thus the app is designed to include educational content and pop-up alerts to remind the patients to take their ULTs. Specifically, the intervention app contains these features:
Uric acid tracker
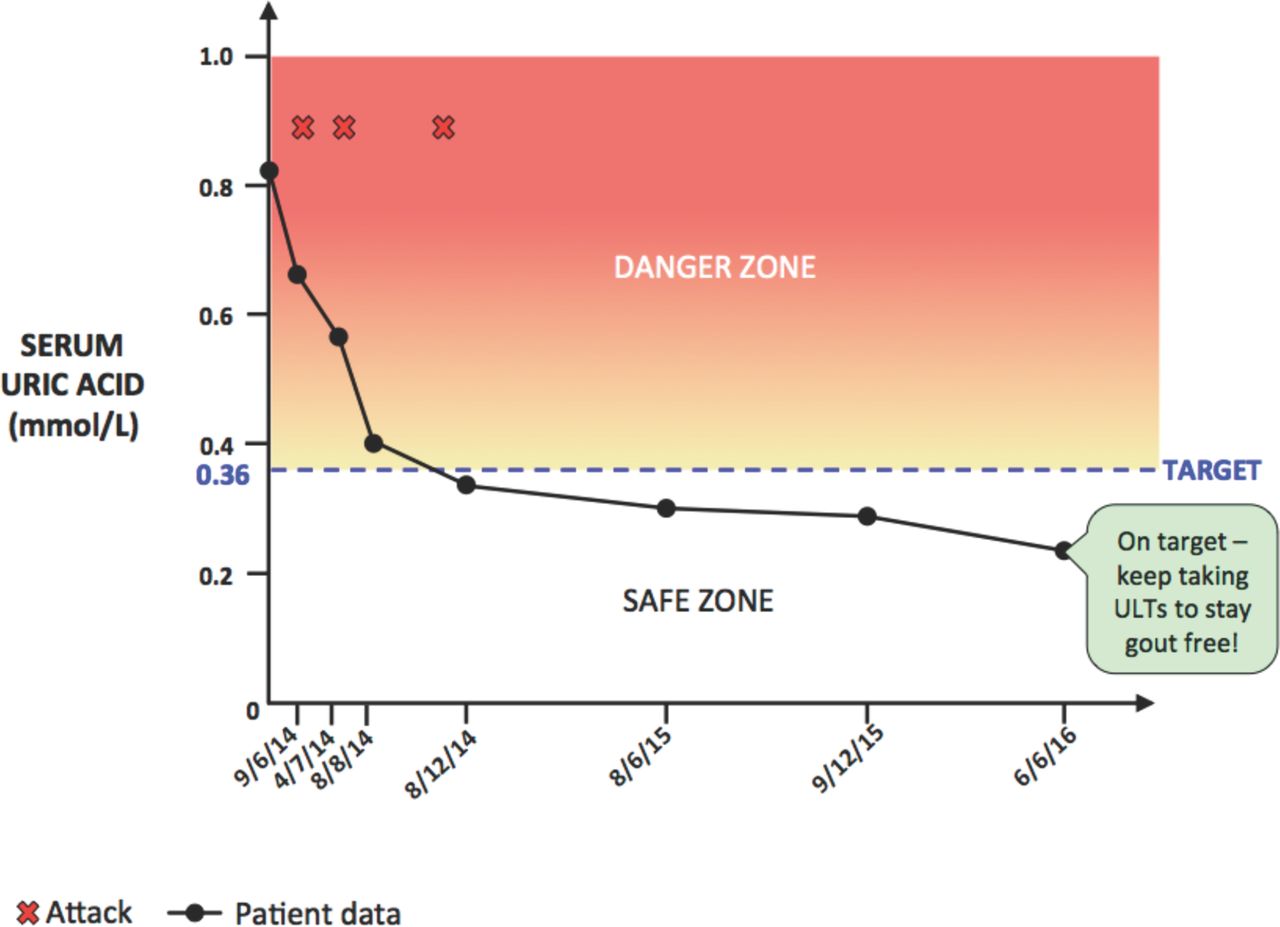
Serum urate results will be recorded and graphed under the ‘uric acid tracker’ function. Patients will be asked to obtain their serum urate results from their GP or pathologist after every test and promptly enter the results into this feature of the app. Alerts within the app will be triggered if serum urate is not in the target range, recommending that patients discuss their gout management with their GP. The patient’s serum urate concentrations will be represented in a graph over time and in relationship to the target serum urate (≤0.36 mmol/L) (figure 2).

{kind=link}
{kind=link}
‘Urate tracker’ personalised for each ’intervention' participant. ULT, urate-lowering therapy.
Gout facts
Educational materials including written information and a video animation about gout and its management for people with gout will be available via the app. The following topics are covered: what is gout, why take ULT medication, the effects of ULT, what to do in a gout attack and the importance of ULT adherence.
Electronic gout attacks diary
This feature provides the ability to record gout attacks including pain intensity, location of attack(s) or joint(s) affected and triggers. The gout attack data that patients enter will be presented in the graph next to serum urate levels.
Schedule
This feature can be used as an alternative to the calendar function of smart devices if patients prefer to use it for management of their gout. Patients can schedule their tasks, such as having blood tests and collecting results, seeing their GP or other members of their care team and recording gout attacks.
Team
Contact details of GP, pathology service, researchers and others such as rheumatologist, physiotherapist and so on can be listed.
Diet tips
An evidence-based list of foods that can raise or lower serum urate will be available.
Baseline data collection
Patients will be asked to complete demographic (including age, sex, marital status, ethnicity, socioeconomic status, level of education), quality of life, workplace productivity and medication adherence questionnaires. They will also provide details of their medical history—of gout (onset, frequency of attacks, treatments), ULT and dose, alcohol history, other medications (especially diuretics and low dose aspirin) and comorbidities (cardiovascular, renal, endocrine, etc). These data will be collected via electronic tablets provided by the researchers, paper forms or via the study internet site. Researchers will be available to assist patients at all stages of this process either face to face, via the internet or by phone. Electronic or online questionnaires will be the preferred method for collection of this information to minimise non-complete or incomplete response as the respondent can be reminded if all questions have not been answered. Completing questionnaires provides an opportunity for any questions from the patient to be answered by researchers. Data from GP records (see below) will be accessed to complete and cross-check relevant details of the patient’s medical histories.
Intervention group
Patients in the intervention group will be provided with their personal login details to access and download the Healthy.me gout management app and installation guide. They will have access to a short introduction to the ‘Healthy.me app’ and its features via an e-mail or in paper form. There will be an opportunity for patients to ask researchers any questions via the website, e-mail, phone or face to face. Patients will have access to the app for 12 months. Patients’ GPs will also have access to the introductory material about the app and the content of educational materials in the app.
Control group
The control group patients will be provided with their personal login details to access and download the Healthy.me modified gout app and installation guide. The full version of the Healthy.Me app tailored for patients with gout will be modified to remove all functions except the gout attack diary, which contains fields to record only the date of attack, pain intensity and location of attack but not triggers. Thus, the control group patients can neither enter their serum urate data into the app nor view the graph. They will be provided with this control app to collect gout attack data as an important secondary outcome measure of this study. They will be informed that the study is tracking their gout experience over the year following entering the study. They will be asked to return to their GP for assessment and serum urate and ULT concentrations at 6 and 12 months independent of other visits they may make to their GP. Reminders to visit their GP and have blood tests will only occur via short message service (SMS) and/or e-mail immediately prior to 6 and 12-month visits to optimise their retention in the study.
GP role
GPs will be asked for access to eligible and consenting patients’ (both intervention and control) medical records at baseline, 6 and 12 months. Details about each patient’s medical history of gout (onset, frequency of attacks, treatments), ULT dose, alcohol history, other medications (especially diuretics and low-dose aspirin), comorbidities (cardiovascular, renal, endocrine) and medical examination details (weight, height, blood pressure) will be extracted from the medical record by the researchers to complement and cross-check the data collected from participants. GPs will also provide patients’ blood (serum urate, creatinine and oxypurinol or febuxostat) test results throughout the study or approve copies being sent to the research team direct from the pathology service.
Pathology service role
One to 2 weeks prior to scheduled or recommended follow-up appointments, reminders will be sent to patients via SMS and/or e-mail to have a blood test for serum urate, creatinine and oxypurinol (the active form of allopurinol) or febuxostat concentrations at their GP or pathology service. Researchers will then collect these results via letter or fax from the GP, practice staff or from the pathology service, confirm via the patient’s Healthy.me account the accuracy of the serum urate data that patients entered in the ‘intervention’ app and record other blood test data in the study’s database (for assessment purposes). Depending on which ULT a patient is prescribed, either oxypurinol or febuxostat concentrations will be forwarded from pathology services to the Clinical Pharmacology Department at St Vincent’s Hospital for measurement, as this laboratory has validated assays for these drugs. Assays for probenecid are not available for this study.
Data collection during the study
Intervention and control participants will be asked to attend their GP clinic at 0, 6 and 12 months (see table 2). Participants will be asked to complete the same questionnaires at each of these visits using a tablet provided, paper forms or the internet. Additional visits to GPs, serum urate and creatinine concentrations and gout attacks will be recorded. These data will be sourced from apps, GP records, Medicare data (which will include details of healthcare consultations) and pathology services for each study participant. These overlapping sources of information will be used to verify the accuracy of data collected. At the 6 and 12 months visits, participants will have the opportunity to discuss their progress, adverse events or questions or concerns they may have with researchers and their GPs. Participating patients will be reimbursed for their time with a AUD$30 gift voucher after completing both a blood test and the survey at each time point of the study: the start, 6 months and 12 months. Assuming that they complete the study in its entirety, they will receive a total of three $30 gift vouchers ($90).
Schedule of enrolment, interventions and assessments
Primary outcome
Serum urate concentration
Patients in both control and intervention groups will attend their GP and/or pathology clinic at 6 months to have their serum urate concentration measured. Consistency between laboratories will be ascertained according to quality control protocols established by the National Association of Testing Authorities, Australia.37 The proportion of patients in the intervention and control groups whose plasma urate is less than or equal to the target urate of 0.36 mmol/L will be compared.
Secondary outcomes
Serum urate concentrations
All urate concentrations, along with creatinine concentrations performed in the 1 year of the study, will be collected. An expectation is that the intervention group will have more urate tests performed especially in the first 6 months of the study. The 12-month urate concentration measurement will indicate whether achievement of target concentrations at 6 months is sustained. The number of serum urate concentration tests undertaken over 6 and 12 months in each group will be compared. Change in serum urate concentrations from baseline to 6 and 12 months will be evaluated also.
Adherence
Along with serum urate concentrations, serum oxypurinol or febuxostat concentrations will be measured in patients at the same time they have their blood collected and tested at their GP or pathology service. Oxypurinol, the active metabolite of allopurinol, or febuxostat concentrations will give an indication of a patient’s adherence to ULT.
In addition to serum oxypurinol and febuxostat concentrations, patients will complete a validated Medication Adherence Scale.38 This will be completed at baseline, 6 months and 1 year and focused on ULT.
Gout attacks
The occurrence and intensity of gout attacks will be self-reported by intervention and control participants via the ‘gout attacks diary’ on the app as attacks occur. Patients will be able to enter the date and duration of their attack, as well as rate the intensity of the pain using a rating scale from 1 to 10.
Impact of gout and health-related quality of life
Impact of gout on health-related quality of life will be measured using the gout impact section of the Gout Assessment Questionnaire V.2.0,39 which contains questions on well-being during gout attacks, gout medication side effects, unmet gout treatment needs and gout concerns overall and during attacks. Utility scores derived from the EuroQoL 5 Dimensions 5 Levels (EQ-5D-5L) will also be used in a secondary analysis.40 Both instruments will be administered at baseline, 6 and 12 months.
Work productivity
Work productivity impairments and impairment in daily activities will be assessed at baseline, 6 and 12 months using the validated ‘Work Productivity and Activity Impairment’ (WPAI) questionnaire.41 This information will be used in the cost-effectiveness analysis.
Statistical considerations
Sample size calculation
An intracluster (practice) correlation coefficient of 0.01 for the primary outcome, within the range for similar cluster randomised studies in Australian and international general practices, was used for power calculations.42–44 The primary outcome is the achievement of the target serum urate concentration, that is, less than or equal to 0.36 mmol/L at 6 months. This serum concentration outcome, if maintained, is a very strong predictor that gout attacks will no longer occur. Rates of achievement of target urate in gout patients, with approximately the same inclusion criteria and offered standard treatment, lie anywhere between 28% and 69%.45 Based on these studies, we have assumed that 50% of the standard care group will achieve the target urate concentration at 6 months. We expect that this is an optimistic prediction. Although there are few studies published on effect sizes achieved for interventions centred on eHealth tools, this study will attempt to demonstrate that 65% of participants in the intervention group will achieve the target, that is, a relative increase of 30% compared with the 50% of participants expected to achieve the target in the control group at 6 months (an absolute increase of 15%). The investigators believe that this effect size will be significant clinically and also at a population level. To demonstrate an effect of this size with 80% power and statistical significance level for a two-sided test of 5%, we will need 186 patients in each study arm to complete the study. To accommodate a 20% drop-out rate of participants at 6 months, and assuming no GP practices drop-out but accounting for the effect of the cluster design,46 558 patients will be recruited in total. A target of at least 3 patients per practice will mean 186 practices would need to be recruited.
Data will be analysed using SAS V.9.4. Missing-at-random data will be handled using multiple imputation. The intention-to-treat principle will be applied and the significance level will be set at 0.05. Intracluster (practice) correlation coefficients will be determined. The primary outcome at 6 months of the control and intervention groups will be compared using the method of general estimating equations, and also for each outcome, to account for the correlation within practices. The effects on adherence will be explored and correlations with primary and secondary outcomes sought.
Baseline comparisons of demographic variables will be performed using independent samples t-tests. Random effects mixed modelling will be used with baseline, 6 and 12 months and group allocation (intervention, control) as the fixed factors. Sociodemographic factors will be controlled for in the analysis. If the proportion of participant’s baseline serum urate less than 0.36 mmol/L is greater than 20%, stratification will be performed.
Economic and process evaluations
An economic evaluation will be conducted to understand the potential investment case of the intervention for the Australian health system. First, the within trial cost-effectiveness of the intervention compared with usual care plus control app will be estimated in terms of the incremental cost per (1) patient achieving the primary outcome and (2) quality adjusted life year gained using the utility scores derived from the EQ-5D-5L, given the previous use of EQ-5D in economic evaluations of ULT.40 Costs will be derived from all aspects of the intervention (eg, software implementation and maintenance, training) as determined from project files and direct medical costs (eg, GP visits, medications, pathology tests, hospitalisations) as determined from GP records and valued at prevailing rates. In addition, indirect (productivity) costs incurred (or avoided) by patients will be collected by participant self-report using the WPAI questionnaire that will be administered at baseline, 6 and 12 months.41 These costs will be included as a sensitivity analysis to estimate the impact of these costs on cost-effectiveness estimates.
Second, to understand the cost-effectiveness of the Healthy.me gout app beyond the trial, a Markov model will be used to track a group of surviving patients at the end of the trial over time in which they potentially progress through a number of health states including serum urate concentrations controlled, uncontrolled and death.47 48 49 The transition probabilities across various defined health states, costs and quality of life attached to various health states will be based on published evidence. Using appropriate discounting, estimates of long-term costs and outcomes will emerge from the model and an incremental cost-effectiveness ratio estimated. A series of sensitivity analyses will be conducted including on discount rates, uncertainty in outcome estimates and variations in costs that may occur across different settings so as to explore important questions about the potential scalability and generalisability of this intervention.
A process evaluation will also be undertaken using qualitative research methods to understand how and why the intervention was (or was not) working in practice. At the completion of the study, a random sample of patients and GPs will be interviewed employing a semistructured interview. Interview questions will be open ended and will be developed to appreciate participants’ views on the app and its value to them.50 Interviews will be audiorecorded and transcribed verbatim. A general inductive approach will be used for analysis. Two researchers will independently analyse transcripts and meet periodically throughout data collection to discuss emerging themes, resolve any discrepancies and determine when theme saturation occurs and thus no further interviews are needed. Back-end data from the app, which give information on the app usage, will also be included in the analysis. These data will be considered secondary outcomes of the study.
Data management
Data will be managed using Microsoft Office Excel and stored in password-protected files. To ensure that each patient and participating GP’s personal identifiers and relevant data sets are deidentified, each participant will be allocated an identification number instead of a name for analysis. Analysis of the transcripts from the focus groups/interviews and patient medical data will occur only after the transcripts and medical data are deidentified by the researcher who undertook the data collection, hence protecting the personal details of the participants. The number allocated to a participant will be recorded in a separate file from the data. This ensures that their confidentiality is maintained throughout the study. The chief investigators and statisticians in the research team will have access to the final trial dataset.
Dissemination
Throughout the duration of the study, clinical data will be available to the patients if they wish. At the conclusion of the study, participants will be given a written report of the study’s findings. The results will also be disseminated via publication in journals and presentations in scientific meetings by the investigators. Additionally, partners in this project may also release general information of findings on their associated websites and media releases.
Ethical approval
This study has received ethical approval from the University of New South Wales Human Research Ethics Committee and is registered with the Australian New Zealand Clinical Trials Registry (Trial Registration: ACTRN12616000455460, Date registered: 7 April 2016). Any important modification to the protocol, made in this version (dated 8 August 2017), will need to be approved by the project steering committee and be submitted to the ethics committee and the trial registry through appropriate channels before the trial begins.
The protocol conforms to the SPIRIT statement (2013)51 and study results will be presented according to the CONSORT statement for cluster, randomised clinical trials.52
Discussion
Improved gout management offers benefits at both an individual and societal level. Adherence with long-term treatment can alleviate gout flares and the associated decreased quality of life, disability and long-term sequelae due to the chronic inflammation of gout. At a societal level, improved management of gout can significantly reduce the substantial economic burden associated with uncontrolled gout.53 There are little available data on the Australian-specific burden of disease due to gout, but because of similar health demographics, the USA is often accepted as having a comparable health outcome profile to Australia. Total annual direct medical costs related to gout in the USA have been estimated to be about $4 billion and total annual indirect costs at $2.6 billion.54 It has been shown that gout patients with poorly controlled serum urate concentrations incur on average higher healthcare costs than patients whose serum urate concentrations are better controlled.55 56 In light of this, cost-effective means of maintaining ULT adherence, and thereby reducing the prevalence of gout, is likely to be highly valuable.
Poor adherence, failure of initiation and under dosing of ULT all contribute to the unacceptably high prevalence of uncontrolled gout. The hypothesis for this study is that effective education for patients with gout about how to manage their condition combined with personalised feedback regarding serum urate concentrations will significantly enhance adherence to ULT, thereby reducing the incidence of acute gout attacks. This study will be the first comprehensive examination of the effectiveness of an eHealth tool designed to help patients self-manage their chronic gout. The process involved in establishing and undertaking this proposed intervention will also be evaluated along with an economic evaluation of the intervention. Cluster, randomised, controlled trials are ideally suited to test interventions where individual patient randomisation is not possible.57 These types of studies commonly use a parallel group design, in which the clusters are randomised to either the intervention or control arm of the study. It is expected that the real world, primary care setting of the study and identification and recruitment of patients from additional sources, including other health services and community-based sources, will optimise the generalisability of study findings. In addition, the study findings will be relevant to promoting adherence to therapy in people with other chronic illnesses.
Behaviour change needed to improve adherence to medications and other therapeutic interventions for chronic health conditions is notoriously difficult to accomplish.58–60 Attempts to improve adherence to ULT in individuals with gout have also been generally unsuccessful or marginally effective and difficult to sustain. There are particular additional impediments to improved adherence in patients with gout. For most chronic conditions such as hypertension, adequate adherence to medications that should be taken regularly, usually daily, is deemed to be about 80% although the evidence supporting this level of adherence is difficult to find.61 This level of adherence for a patient with recurrent attacks of gout however, is unlikely to be satisfactory. These patients are prone to attacks during the periods of both stopping and starting ULT and 1 or 2 days missed therapy is enough to precipitate an attack in many gout sufferers. To reduce the risk of attacks during the establishment of ULT, it is recommended that doses are escalated over weeks and prophylactic comedications such as colchicine are given.29 Even with these measures that are complex for patients to understand, there is still the risk of an acute attack and the sufferer needs to know that ULT should not be stopped. Therefore, it is not surprising that adherence to the level required is not often achieved and that the interventions to-date have been disappointing.
Personalised feedback is a proven method of changing behaviour.60 Sustained reduction of urate concentrations to 0.36 mmol/L or below is a very well established surrogate indicator for elimination of recurrent attacks of gout.62 The use of electronic tools especially apps to provide personalised feedback on urate concentrations and high-quality education and alerts may be an effective approach to positively impacting adherence to ULT.
Focus group discussions with patients with gout during the app development phase indicated their strong beliefs that certain foods and beverages precipitated their attacks and their desire to be able to record this information in their gout attack diaries. Thus, ‘Diet Tips’ feature with dietary information is provided in the app. While there is insufficient evidence on the clinical effectiveness of dietary intervention alone in lowering urate levels in gout patients, we cannot exclude the evidence on associations between certain foods and risk of gout, for example, higher levels of meat and seafood consumption and an increased risk of gout.63 In addition, the existing guidelines on gout management recommend patient education on diet and lifestyle.64
It is possible that the control app containing the ‘gout attacks diary’ feature only may have some effect on self-management of the control group although it does not actively provide personalised feedback. One alternative to obtain the gout attack data (a secondary outcome measure) was to provide paper diaries to the control group to record acute attacks, whereas the intervention group would be able to record their attacks on the app. Another option was to ask the control group to recall acute attacks and their intensity at the 6 and 12-month assessments. Neither would escape a reporting bias favouring the apparent efficacy of the control app. If power and resources were not a constraint, a third study arm with no app could have been included. Providing the control group with the app (containing this limited feature) may also reduce the risk of selective withdrawal of participants in this group and poor response in the follow-up assessments due to disappointment for being in the control group and not receiving an app.65
Customary management of gout in primary care can be suboptimal. This study is testing the effectiveness of the app in the existing primary care context, and the design of the intervention does not include educating GPs in best practice. With the trust that randomisation works, the suboptimal gout management will be balanced between intervention group and control group, and the study will be testing the effectiveness of the app only. There is an expectation that patients with the test app could ‘reverse’ educate their GPs to some extent, and this would contribute to the effectiveness of the intervention.
The results from this prospective, cluster randomised controlled trial will provide important insights into the effectiveness of an app designed to promote enhanced self-management of gout. Information about the reactions of patients to the features of the app and the rates of use of these features will also be valuable when considering potential modifications to the app. It will also provide data for the cost-effective analysis. On a larger scale, results from this study will deliver significant evidence-based guidance for future clinical eHealth initiatives relevant to chronic disease.
This protocol has been reviewed and endorsed by The Australia and New Zealand Musculoskeletal (ANZMUSC) Clinical Trials Network (http://anzmusc.org/).
References
Footnotes
Contributors All authors contributedto study design and the final manuscript; ADN, MTB, AYSL, NZ, JR, AM, WR, RC-W,EC, JB, DH, KP, IP and KMW contributed to selection outcomes; ROD conceived thestudy, led the grant application to seek funding, led the discussions regardingstudy design and led the revision of draft manuscripts; LJF was projectmanager*, wrote the draft manuscript, revised multiple versions and liaisedwith investigators; ADN led and contributed to pilot testing of the ‘app’; MTB contributedespecially to the human factors aspects of the app development; EA becameproject manager after LJF, revised the manuscript, consolidated outcomemeasures and prepared the response to referees and editor; AYSL contributed tothe modification of the Healthy.Me app for people with gout; NZ contributed especiallyto the primary care aspects, analytical considerations particularly the clusterdesign; JR contributed especially to the primary care aspects; TL-L contributedto the design relevant to cost-effectiveness, analytical considerations; LL contributedespecially to the power calculations; AM advised on pharmaceutical aspects; WR andRB contributed especially to the educational material in the app; RB providedexpertise with respect to gout; RC-W contributed to the design and modificationof the HealthyMe app for people with gout; EC contributed to the eHealthaspects of the study; JB, contributed to the ‘health systems’ aspects of thestudy; HPM, DH, KP and IP provided expertise with respect to gout, especiallythe educational content of the app; JIW contributed to the eHealthmethodological aspects of the study.* Resigned December 2016.
Funding This study is supported by a National Health and Medical Research Council (Australia) Partnership Grant APP1094708 and Programme Grant APP1054146. The Trial Investigator and the research team will conduct study design development, trial coordination, data management and interpretation, writing of the report and submitting the report for publication independent of the funding agency.
Competing interests None declared.
Ethics approval University of New South Wales Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data from this study will be made available freely without limitation.
Correction notice This article has been corrected since it first published. The author ’Kevin J Pile' has been corrected to ’Kevin D Pile'.