Article Text

Abstract
Introduction Low rates of accrual of African-American (AA) patients with cancer to therapeutic clinical trials (CTs) represent a serious and modifiable racial disparity in healthcare that impedes the development of promising cancer therapies. Suboptimal physician–patient consultation communication is a barrier to the accrual of patients with cancer of any race, but communication difficulties are compounded with AA patients. Providing tailored health messages (THM) to AA patients and their physician about CTs has the potential to improve communication, lower barriers to accrual and ameliorate health disparities.
Objective (1) Demonstrate the efficacy of THM to increase patient activation as measured by direct observation. (2) Demonstrate the efficacy of THM to improve patient outcomes associated with barriers to AA participation. (3) Explore associations among preconsultation levels of: (A) trust in medical researchers, (B) knowledge and attitudes towards CTs, (C) patient-family member congruence in decision-making, and (D) involvement/information preferences, and group assignment.
Methods and analysis First, using established methods, we will develop THM materials. Second, the efficacy of the intervention is determined in a 2 by 2 factorial randomised controlled trial to test the effectiveness of (1) providing 357 AA patients with cancer with THM with 2 different ‘depths’ of tailoring and (2) either providing feedback to oncologists about the patients' trial THM or not. The primary analysis compares patient engaged communication in 4 groups preconsultation and postconsultation.
Ethics and dissemination This study was approved by the Virginia Commonwealth University Institutional Review Board. To facilitate use of the THM intervention in diverse settings, we will convene ‘user groups’ at 3 major US cancer centres. To facilitate dissemination, we will post all materials and the implementation guide in publicly available locations.
Trial registration number NCT02356549.
- Health Disparities
- Physician - Patient Communication
- Tailored Health Messages
- Randomized Controlled Trial
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study is designed to overcome significant health disparities by improving African-American–oncologist communication about therapeutic clinical trials.
This study will extend our knowledge of tailored health messaging.
This study is a randomised controlled trial of tailored health messaging in a novel setting, cancer clinical trial communication.
We have limited capacity to assess the differential efficacy of the intervention between phase I, II and III clinical trials.
This study is being conducted at one academic cancer centre, thus communication issues particular to the community oncology setting will not be assessed.
Introduction
The cancer mortality rate in the USA is 33% higher for African-Americans (AA) than for white Americans and AA have the lowest 5-year survival rates when compared with all other racial groups.1 In the USA, the National Cancer Institute, the American Cancer Society and the American Society for Clinical Oncology have recognised and reported the unequal burden of cancer in AA patients and their low representation in clinical trials (CTs). The effectiveness of this translational process is greatly dependent on the number and representativeness of participants enrolled in trials, yet <5% of all adult patients with cancer enter CTs and even lower participation rates are reported in minority populations, including AA.2–4
Inequitable participation in state of the art cancer care contributes to health disparities in cancer mortality and survival between AA and whites.5 ,6 Specifically, low representation of AA patients in CTs compromises the generalisability and external validity of trial results,7 ,8 and may fail to identify important positive or negative treatment effects among under-represented populations.9 ,10 Barriers to minority patients' participation in CTs include systemic factors,11 ,12 such as strict exclusion criteria,11 which limit AA opportunities to participate.12 However, studies suggest that racial differences in patient barriers to participation are due in part to non-clinical factors related to poor trial information,13 ,14 mistrust of medical research,15 family pressures12 and poor communication with physicians.5 ,11 ,16 Thus, high-quality physician–patient communication is key to increasing the active engagement of AA patients in decision-making about CTs. Yet, there is mounting evidence about the communication challenges present in treatment discussions,16–31 including CTs that are compounded with AA patients.32 ,33 Racial disparities in communication could lead to less informed decisions34 and lower trust in physicians.34 As such, there is a critical need to develop communication interventions to modify barriers to recruitment and hopefully ameliorate health disparities and optimise the benefits of CTs.5 ,6 ,11 ,35
One communication method that has demonstrated efficacy to promote patient activation (characterised by asking questions, expressing concerns and being assertive) in consultation communication is providing tailored health messages (THM).36 THM increase the relevance of health information by targeting individuals' personalised needs based on a rigorous assessment of their characteristics and preferences37 and have been successfully used to promote AA cancer screening behaviours.38 The process of tailoring health messages involves collecting data (usually by way of a comprehensive survey) about the receiver's needs and preferences and then preparing individually customised materials (eg, print materials or online tools) that meet these needs.
Evidence indicates that THM interventions are effective;39 however, research is still needed to explicitly explore factors that most contribute to their success. The exact number of variables needed and the level and intensity of tailoring (depth of tailoring) required to achieve research goals is not known. Physician–patient communication is known to be a dynamic process; yet, no studies, to the best of our knowledge, have explored the impact of involving patients and physicians in THM interventions that target cancer CT consultations. The goal of this study is to test the efficacy of (1) providing AA patients with cancer with tailored CT messages with two different depths of tailoring and (2) either providing feedback to oncologists about the patients' tailored CT messages or not.
To the best of our knowledge, this is the first randomised controlled trial (RCT) which assesses the efficacy of a THM intervention on AA patients with cancer (1) active communication in CT consultations as measured by objective coding of consultation audio recordings, (2) self-reported barriers to joining CTs, and (3) satisfaction and decision-related outcomes.
Methods and analysis
Study design
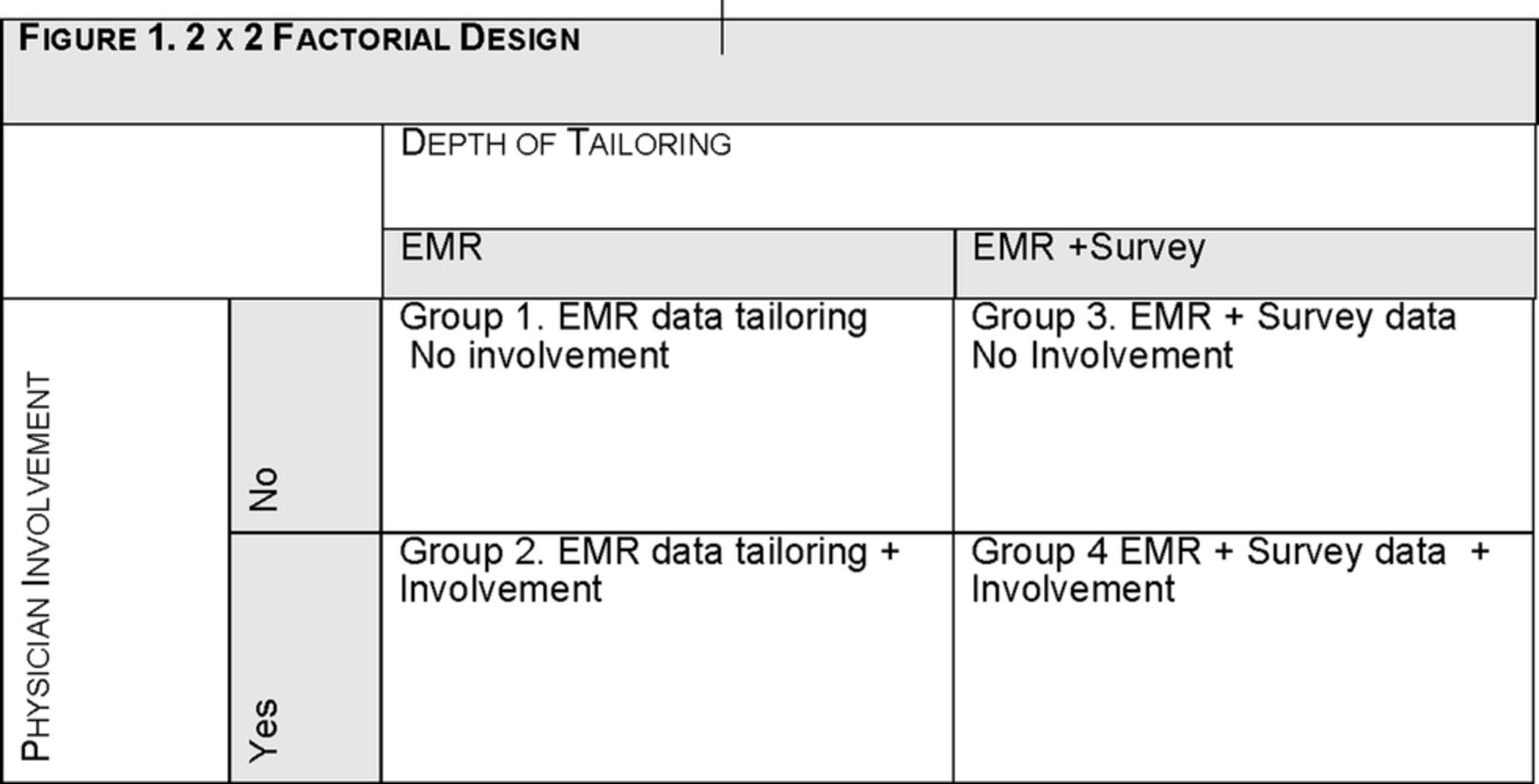
This study is an RCT using a two by two factorial design. Equal numbers of participants are randomly assigned to one of four intervention groups.
This study follows CONSORT guidelines (figure 1).40

Consort diagram. EMR, electronic medical records.
Group 1 (n=89): shallow tailoring—Patients receive THMs based only on demographic and disease information extracted from their electronic medical records (EMR). These variables include (1) demographic information: age, income, education and health insurance status; (2) disease variables: cancer type and severity; and (3) trial variables: phase of trial being offered and prior trial participation.
Group 2 (n=89): shallow tailoring+physician involvement—Patients receive THMs based on EMR data, and their physicians receive a summary of the THMs that are provided to the patients.
Group 3 (n=89): deep tailoring—Patients receive THMs based on EMR data as well as data derived from a survey that patients completed on enrolment.
Group 4 (n=89): deep tailoring+physician involvement—Patients receive THMs based on EMR and survey data, and their physicians receive a summary of the THMs that are provided to the patients (figure 2).

A 2×2 Factorial design. EMR, electronic medical records.
Intervention
Tailored message development
THMs were developed using guidelines presented in the health communication literature.41 ,42 Many THM interventions are based on the input of data collected by means of a comprehensive survey to produce messages that are matched to an individual recipient's needs and preferences. However, patient data to inform tailoring can also be generated by accessing patient data through EMR.37 As we intend to explore the impact of different ‘depths’ of tailoring, we use both comprehensive surveys and EMR data to generate patient data to produce two types of THM.
The first step to develop the THMs is to generate patient data to develop tailored messages about CTs. To achieve this, we extract patient demographic and disease variables and information about their CT experience from patients' EMR and use these data to generate a ‘shallow’ level of tailoring. These data include: (1) demographic information such as age, education level, income; (2) health information such as disease site and severity; and (3) trial information such as the phase of trial offered and previous trial involvement.
Tailoring survey
We use standardised, psychometrically sound measures to gather information about patients, including their levels of trust in medical research and use these data, augmented by their EMR data, to develop a ‘deeper’ level of THM. These measures are listed in box 1.
Standardised measures to be used for survey tailoring
Knowledge/attitudes towards clinical trials43
Health literacy44
Trust in medical researchers45
Trust in physician46
Communication self-efficacy47
Information preferences48
Decision involvement preferences49
Participants randomised to deep tailoring complete these measures as part of the tailoring survey in order to develop THM. We include these measures in patient assessment surveys for the other intervention groups. Knowledge/attitudes towards trials and health literacy will be assessed as potential confounding variables. The other variables are assessed as outcomes.
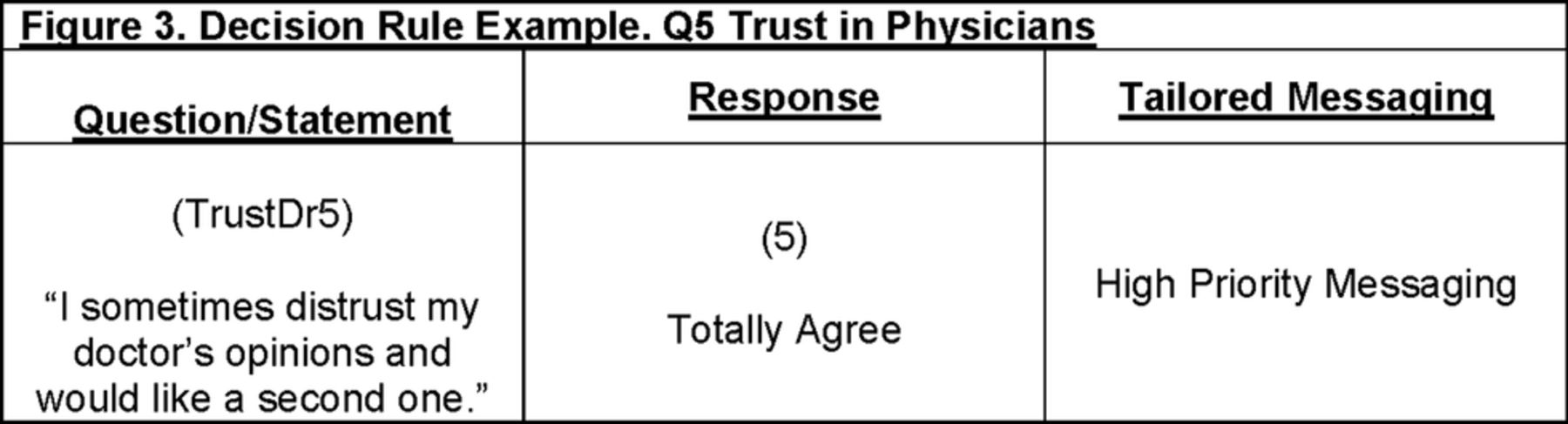
The second step is to develop the three necessary components to deliver tailored messages: (1) the design template; (2) message concepts and (3) tailoring algorithms. We use the Michigan Tailoring System (MTS) software program to support the development of the three components. The MTS is an open-source software toolkit which can create THM for a variety of delivery modes, such as print, web and mobile devices.50 We first developed a design template to visualise the message layout, with the goal of producing a two-page, double-sided brochure for participating patients and a one-page summary of the brochure content for the physicians. The design template shows where each message will appear on the page, how blocks of messages relate to each other and information about the content of each block of messages.37 Next, we developed message concepts, for example, shallow versus deep messages concerning medical mistrust, which are the detailed ideas about the content of the THMs. Specific concepts are created for each potential message.37 Then, we created a set of tailoring algorithms, which are decision rules that guide every judgement about which THMs each patient will receive37 (see figure 3 below for an example).

{kind=link}
{kind=link}
{kind=link}
Decision rule example. Q5 trust in physicians.
Implementing and assessing the intervention
Data from study participants in groups 1 and 2, who are randomised to receive THMs based on their EMR data alone, are entered into the MTS system and their brochures are prepared. These brochures are mailed 1 day after participants have assented to the study. To standardise our data collection across all groups, participants complete the survey described above in box 1. One week before their scheduled appointment to discuss a CT with their physician, a study research assistant (RA) calls the participant to administer the survey over the telephone. If a participant does not have a telephone, we mail the survey along with a prepaid return envelope and ask the participant to complete and return the survey within a 24-hour time frame.
Study participants randomised to groups 3 and 4, who are randomised to receive THMs based on both their EMR data and survey responses, complete the survey within 1 week of the participant's scheduled appointment with their physician to discuss a CT. The study RAs call participants to complete the survey over the telephone, with follow-up by mail, as described above for groups 1 and 2, if the participant cannot be reached by telephone. Once the survey responses are received, they are entered into the MTS software along with patient EMR data, and the personalised THMs are instantly generated and colour printed in the format described above. The brochures are mailed to participants to read and participants are encouraged to bring their THM brochure to their consultation to discuss a CT.
Prior to the consultation, physicians of patients randomised to groups 2 and 4 receive a printed summary of each patient's THMs in the patient's notes.
When participants arrive for their appointed consultation, they are met by a study RA. The RA gains written informed consent (see recruitment plan below) and remains present to audio record the consultation. The RA places a digital audiorecorder in the consulting room and then leaves for the remainder of the consultation. The RA collects the audiorecorder at the conclusion of the consultation. At this time, participants complete a second brief survey asking about the tailored message brochure. One family member/caregiver of consented participants is also recruited or identified for recruitment at this time. Consented family member/caregivers are asked to complete the Communication Assessment Tool for Patients and Families (CCAT-PF), a measure of perceived congruence over the treatment decision (see recruitment plan below).
If a CT was not discussed the participants' involvement in the study is complete and their data and the audio recordings are stored along with all other participant data. If a CT was discussed during the consultation, patients are asked to complete a third survey to assess their immediate, postconsultation impressions of the CT conversation. At this time, the RA identifies a convenient time for the patient to receive a follow-up telephone call at ∼1 month after the consultation visit to complete a final survey. At the appointed time, the RA will call to administer this postconsultation evaluation survey. Patients who do not have a telephone will receive the questionnaire via mail 1 month after the visit along with a prepaid return envelope. These participants will be asked to complete and return the survey within a 24-hour time frame. We chose to collect data 1 month after the consultation in order to ensure that patients have had time to (1) make a treatment decision and (2) have started cancer treatment.
Fidelity plan: We have developed a comprehensive fidelity plan. In summary, we will (1) conduct regular checks to ensure that participants complete the phone-administered surveys, (2) use a preconsultation questionnaire to monitor whether participants redeive and understand the THM brochure, (3) conduct regular interviews with physicians in groups 2 and 4 to ascertain that they are reading the THM summary.
Setting
This study is being conducted at the Massey Cancer Center (MCC), a National Cancer Institute designated centre in Richmond, Virginia, USA. MCC is a safety net hospital that provides inpatient and outpatient services to patients with cancer from a broad catchment area. MCC has a diverse patient population and thus consistently recruits minority patients to trials, mostly AA, at rates above the national average. Thirty-six oncologists have been recruited from the surgical, hematology and radiation oncology services between June 2015 and December 2015.
Sample and recruitment
Physician identification and accrual
There are 40 oncologists currently practising at MCC who are eligible to participate in this communication study. Physicians who recruit AA patients to CTs at MCC are eligible to participate. To inform oncologists about the study, a detailed description is presented at clinical conferences and individual discussions are held with physicians as needed. Written consent to participate is obtained at these meetings.
Patient/family member identification and recruitment
Patient identification and recruitment
This study will recruit 357 patients, which is a feasible number given the patient resources available at MCC. This study recruits AA patients who are eligible for a phase I, II or III therapeutic CT, regardless of whether they join the therapeutic trial or not. Eligible patients have a cancer diagnosis, self-identify as AA, are eligible for a therapeutic phase I, II or III CT at MCC, are able to provide informed consent, and are 21 years of age or older.
Study personnel use the Virginia Commonwealth University Health system EMR database to identify all potentially eligible patients with cancer.51 ,52 RAs attend weekly multidisciplinary disease team meetings where patient eligibility for CTs is discussed. Once therapeutic trial eligible patients have been identified, RAs obtain physician approval to approach each patient.
The steps involved in patient recruitment are as follows:
Step 1: The RA sends the identified patient a letter that provides a brief description of this study and indicates that they will call the patient within 1 week to discuss the patient's possible participation. Step 2: The RA calls the patient to inform them about the purpose and requirements of the study and asks him/her to consider participation. Each patient who verbally assents is then randomised to one of the four study groups. Step 3: On the day of the trial consultation, patients receive an information sheet and are asked to provide written consent. (see online supplementary file).
supplementary file
Family member recruitment
We also recruit one family member/caregiver of each participating patient in order to assess the level of congruence between the patient and their family member over the eventual treatment decision. Consented patients will not be excluded from this study if their family member declines to participate. We recruit family members/caregivers who are nominated by the consented patient as important to the trial decision. Within 1 week of the consultation family members complete a measure of decisional congruence, the CCAT-PF53 in person or over the phone.
Randomisation
The randomisation is conducted off site according to protocols developed by the study statistician. We make use of the randomisation procedures in SAS/STAT. The allocation sequences are stored in a computer file and are unknown to the researchers until the patient is randomised. Block randomisation is used to minimise large imbalances between the four groups. Patients are unaware of the treatment allocation: however, it is not possible to blind oncologists to their patients' treatment allocation. The raters who code audio recordings of the consultations are not aware of the patients' group allocation.
Study aims and hypotheses
The specific aims and study hypotheses are listed below.
Aim 1: Demonstrate the efficacy of the THM intervention to increase patient activation as measured by coding consultation audio recordings using the Street Patient Activation Coding system.50
H1: Group 3 will be more active communicators than group 1.
H2: Group 2 will be more active communicators than group 1.
H3: Group 4 will be more active communicators than group 3.
Aim 2: Demonstrate the efficacy of the THM to improve patient outcomes.
H4: Group 3 will report higher scores on: trust in their physician, preference achievement, communication self-efficacy, consultation satisfaction and decision outcomes than group 1.
H5: Group 2 will report higher scores than group 1 on the same group of outcomes as H4.
H6: Group 4 will report higher scores than group 3 on the same group of outcomes as H4 and H5.
Aim 3: Explore the association between preconsultation levels of (1) trust in medical researchers, (2) knowledge and attitudes towards CTs, (3) patient family member congruence, and (4) involvement/information preferences and group assignment.
Study measures
Data collection: All patient identifiers, questionnaire responses and digital audiorecrdings will be stored on a HIPAA compliant server and will only be available to study staff.
Data extraction from EMR
Postvisit, we will extract trial data from the EMR including whether the patient enrolled and if not, whether this was due to systemic factors such as insurance status.
Consultation audio recording
The CT consultation discussions are audio recorded and subsequently coded using the Street Patient Activation Coding system54 to gather data about patient–physician communication, including the level of patient activation in the consultation.
Consultation coding for patient activation
The primary outcome variable used for this study will be patient activation as measured by the Street Patient Activation Coding system.54 The coding system will be used to code for three patient participation behaviours (asking questions, expressions of concern and verbally assertive responses) and two physician patient-centered responses (partnership building and supportive talk). The Street Coding system has been used in multiple studies to assess patient activation33 ,55 and has been used successfully as an outcome variable.56 Once coding is completed, a composite score is calculated and entered and stored in an Excel database that is exported to SAS for analysis.
Measures
Questionnaire data
Physician demographics
Participating clinicians provide information about their age, gender, race, specialty, years of practice and years recruiting patients to phase I, II and III CTs at the time when they are recruited to the communication study.
Patient questionnaires
Patients complete questionnaires prior to their consultation, immediately postconsultation and 1 month after their consultation. All measures have been previously published and are standardised and validated scales. Table 1 below provides the details of each of the scales and an administration schedule.
Questionnaires and assessment tools used in the study Questionnaire content and schedule—preclinical and postclinical trials consultation
Power analysis and sample size calculation
We computed power to detect cross-sectional group differences on the primary outcome, patient activation using 2×2 analysis of covariance (ANCOVA) with two covariates which is the least powered scenario in the proposed analytic plan. Using previous findings reporting a mean count of active patient utterances from the Street Coding system54 used in a sample of African-American patients of 5.9, SD=5.5, we compute sample size needed to detect a ½ SD difference between groups, which represents an effect size of 0.223. Power is 0.90 with an N=357.
Data analyses
All analyses will be conducted as intention-to-treat given available data including outcomes extracted from medical records even if the participant does not complete the full research protocol, for example, becomes too ill. We will conduct post hoc exploratory analyses to examine whether the intervention was more effective for some groups than others, for example, by age and gender.
Aim 1
Once descriptive (univariate) analyses are completed, we will use bivariate statistics and means testing for hypotheses testing. Bivariate analyses will first be used to examine depth of tailoring, physician involvement and patient activation. ANCOVA will be used to evaluate the main effect of depth of tailoring, the main effect of physician involvement and possible interactions between depth of tailoring and physician involvement on patient activation.
Aim 2
Bivariate analyses will first be used to examine depth of tailoring, physician involvement and trust in their physician, levels of achievement of information and involvement preferences, levels of communication self-efficacy, satisfaction with the consultation communication, satisfaction with their decision, levels of decisional conflict and levels of decision regret. Multivariate ANCOVA (MANCOVA) will be used to evaluate the main effect of depth of tailoring, the main effect of physician involvement and possible interactions between depth of tailoring and physician involvement on all dependent variables.
Aim 3
Bivariate analyses will first be used to examine depth of tailoring, physician involvement and trust in medical researchers, knowledge and attitudes towards CTs, patient/family member congruence and involvement/information preferences and health literacy. MANCOVA will be used to evaluate the main effect of depth of tailoring, the main effect of physician involvement and possible interactions between depth of tailoring and physician involvement on patient activation using each of these characteristics as well as phase of trial as covariates. Repeated measures MANCOVA will be constructed similarly to the proposed MANCOVA to examine stability and/or change in characteristics assessed over time (eg, decisional conflict).
Expected achievement
Using established methods of THM, we are directly intervening in the physician–AA patient CT consultation communication process to increase patient activation in the consultation to potentially improve a range of relevant patient outcomes. Since we are extending the use of the THM intervention, by assessing depth of tailoring and physician involvement in the intervention, we anticipate that our results will inform scientific knowledge and influence optimal use of THM in multiple clinical settings.
Discussion
Therapeutic CTs test the efficacy of newly emerging cancer treatments, yet few patients with cancer participate, thus slowing the progress of new treatments and their implementation to fight cancer. African-American patients with cancer are among the least likely to be offered to join a CT and among the least likely to join a trial if asked. Ineffective consultation communication has been identified as a significant factor contributing to AA patient refusal to join a trial. We suggest that using THM coupled with physician involvement in the intervention process has the potential to assist AA patients to be more engaged and active communicators, which in turn may help overcome barriers to trial enrolment and improve significant patient outcomes.
THM increase the relevance of health information by targeting individuals' personalised needs based on a rigorous assessment of their characteristics and preferences.37 No studies to date have explored the impact of providing tailored CT information to promote active AA participation in CT consultations. Thus, this project extends the use of THM into a novel clinical context with the potential to reduce health disparities associated with AA recruitment to cancer CTs. This study is innovative in that we will test the impact of shallow versus deep tailoring to provide new information about the depth of tailoring required to increase patient activation. Further, in spite of the dynamic nature of consultation communication, no studies have explored the additional impact of involving patients and physicians in THM interventions. These data can potentially be used to inform and impact optimal methods for using tailored health messaging.
There are three main limitations to this study. First, our own data suggest that communication challenges differ between phases I, II and III trials. For example, physicians may be more paternalistic with patients facing a phase I CT than those facing a phase III trial.21 Our sample size does not allow us to stratify the randomisation by trial phase as this would almost triple the sample required. Second, we will recruit participants from MCC, a safety net hospital. However, we will not cover communication issues particular to the community oncology setting. Third, physician training to use the patients' THM summary will not be provided. Future research could usefully add and assess such a training component.
Ethics and dissemination plan
The study is registered at Clinical trials.gov, identifier—NCT02356549.
Patient recruitment started in April 2016 and is expected to close in June 2018.
This program is designed to be ‘turnkey’, in that all of the core processes needed to implement the program will be finalized on project completion and readily available at no cost and can be downloaded from our own local websites and other national websites. To facilitate use of the THM intervention in diverse settings, we will convene ‘user groups’ at three major US cancer centres. Input from these user groups will be used to develop an implementation guide. To facilitate dissemination, we will post all materials and the implementation guide in publicly available locations. We will also attend scientific meetings and publish manuscripts that detail the study.
References
Footnotes
Contributors RFB, RD, SG, DC and GG developed the initial project idea, contributed to the intervention development, enacted the intervention, aided in developing and reviewing the manuscript. MWG developed the initial project idea, developed the analysis plan, sample size calculation, randomisation techniques. She also aided in developing and reviewing the manuscript. JA, ML and JW contributed to the intervention development, enacted the intervention and aided in developing and reviewing the manuscript.
Funding American Cancer Society Research Scholar Grant (RSG-14-227-01 CPPB).
Competing interests None declared.
Ethics approval Virginia Commonwealth University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement At this time patient data have yet to be collected. Once data are collected it will be available by emailing RFB at Richard.Brown@vcuhealth.org.