Article Text

Abstract
Objectives To analyse developments (and their causes) in the number and proportion of clinical trials that were registered in different parts of the world after the International Committee of Medical Journal Editors (ICMJE) announced in 2004 that it would require registration of clinical trials as a condition for publication.
Setting The International Clinical Trials Registry Platform (ICTRP).
Design The ICTRP database was searched for all clinical trials that were registered up to 31 December 2013.
Results The ICTRP database contained data on 186 523 interventional clinical trials. The annual number of registered clinical trials increased from 3294 in 2004 to 23 384 in 2013. Relative to the number of clinical trial research publications, the global number of registered clinical trials increased fivefold between 2004 and 2013, rising particularly strongly between 2004 and 2005. In certain regions, especially Asia, the annual number of registered trials increased more gradually and continued to increase up to 2013. In India and Japan, two countries with marked but more gradual increases, these increases only happened after several local measures were implemented that encouraged and enforced registration. In most regions, there was a trend toward trials being registered at local registries.
Conclusions Clinical trial registration has greatly improved transparency in clinical trial research. However, these improvements have not taken place equally in all parts of the world. Achieving compliance with registration requires a coalescence of global and local measures, and remains a key challenge in many countries. Poor quality of registered trial data and the inaccessibility of trial protocols, results and participant-level data further undermine the potential benefits of clinical trial registration. National and regional registries and the ICTRP have played a leading role in achieving the successes of trial registration to date and should be supported in addressing these challenges in the future.
- MEDICAL ETHICS
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To show how global clinical trial registration has developed globally from 2004 to 2013, this study analysed the countries of recruitment in 186 523 clinical trials that were registered at 16 clinical trial registries around the world and provide data to the WHO's International Clinical Trials Registry Platform (ICTRP).
By analysing differences in trends in clinical trial registration between countries and regions, the study shows that increases in trial registration have had different trajectories in different parts of the world, and that a coalescence of global and local measures is needed to increase the proportion of trials that is registered in countries.
Reporting on other information of interest besides trials’ countries of recruitment (eg, health problems or interventions studied) was not possible because most data fields in the data set did not consist of standardised categories.
In the absence of data on actual numbers of trials that were conducted during this period (we analysed trials that were registered), this study sheds light on developments in the proportion of trials registered by comparing developments in numbers of registered trials to developments in annual numbers of publications about clinical trial research and various countries' expenditures on health research.
Introduction
More than half of all clinical trials are never published and outcomes of clinical trials are frequently selectively reported.1 Besides resulting in a waste of resources, this has led to a situation in which clinical decision-making is based on biased evidence and in which patients participate in research that is never used.2 ,3 To help increase the ethical and scientific value of clinical trial research, calls for registration of all clinical trials before the start of recruitment of participants increased in the 1990s and 2000s. These calls received broad support, including from the WHO4 and from the International Committee of Medical Journal Editors (ICMJE) who announced in September 2004 that starting from July 2005, all clinical trials must be registered at a clinical trial registry to be eligible for publication.5 More recently, the AllTrials campaign has drawn attention to the need for greater transparency on clinical trials’ methods and results.6
To show how clinical trial registration has developed since the ICMJE's announcement that all trials must be registered, we provide an analysis in this article of how many clinical trials have been registered in different parts of the world up to 2013. By drawing comparisons to numbers of published articles on clinical trial research and to countries’ expenditures on health research, we shed light on how the proportion of clinical trials that is registered has changed. By studying developments in the number of registered clinical trials, differences in those developments between regions and countries, and differences in the events that have driven registration, we also provide insight into the measures that are needed to achieve improved compliance with trial registration. Finally, we discuss the main challenges that remain and lie ahead in achieving the goal of full accessibility to information on all clinical trials’ methods and results.
Methods
We searched the database of the International Clinical Trials Registry Platform (ICTRP) on 8 February 2014 for all studies that were registered up to 31 December 2013. The registered records of these studies were downloaded to Excel. For studies that were registered in more than one registry (‘duplicate’ registration), only the record with the earliest registration date was included (all ICTRP data that are publicly available are automatically ‘deduplicated’, meaning that duplicate records of trials that have been registered at more than one registry have been removed). Of the studies that we found, we excluded all observational studies on the basis of entries in the ‘Study Type’ field.
About the data
The ICTRP was established at the WHO in 2006 to bring together data on trials registered in national and regional registries around the world, thus providing one single point of access to all registered clinical trials globally.7 When this study was conducted, there were 16 national and regional clinical trial registries in Africa, Asia, Europe, Latin America and the Caribbean, Northern America and Oceania that provided data on registered clinical trials to the ICTRP. For each trial, information is publicly available in the registered record on a range of data items that differ per registry, but contain at least the items in the WHO Trial Registration Data Set (box 1).8
The WHO Trial Registration Data Set (TRDS) (V.1.2.1)
The 20-item WHO Trial Registration Data Set (TRDS) outlines the minimum amount of information about a trial that must appear in a register for a given trial to be considered fully registered:8
1. Primary Registry and Trial Identifying Number
2. Date of Registration in Primary Registry
3. Secondary Identifying Numbers
4. Source(s) of Monetary or Material Support
5. Primary Sponsor
6. Secondary Sponsor(s)
7. Contact for Public Queries
8. Contact for Scientific Queries
9. Public Title
10. Scientific Title
11. Countries of Recruitment
12. Health Condition(s) or Problem(s) Studied
13. Intervention(s)
14. Key Inclusion and Exclusion Criteria
15. Study Type
16. Date of First Enrolment
17. Target Sample Size
18. Recruitment Status
19. Primary Outcome(s)
20. Key Secondary Outcomes
Analyses
To analyse how clinical trial registration has developed around the world between 2004 and 2013, we conducted analyses of: (1) developments in clinical trial registration globally; (2) developments at each of the 16 registries where clinical trials were registered; (3) developments in trial registration in different parts of the world; (4) changes in annual numbers of registered trials for a select number of countries as compared to their annual health research expenditures; (5) developments in clinical trial registration in Japan and India; (6) additional characteristics of trials, such as their study phase and target sample size.
1. Developments in clinical trial registration globally
We assessed how many clinical trials were registered each year to develop insight into trends in the number of registered clinical trials globally, from 1994 (the earliest year of registration of a trial at one of the registries included in the ICTRP database) to 2013. To shed light on developments in the proportion of trials registered each year, ideally we would have compared these numbers to the actual number of clinical trials conducted each year. However, this was not possible, since data on the actual number of clinical trials that are conducted are not available. Therefore, we also assessed the annual number of published articles resulting from clinical trial research, under the assumption that if the number of clinical trials that were registered increased relative to the number of publications, the proportion of trials that were registered may have increased. To do so, we searched PubMed, on 6 January 2015, using a search algorithm for the year of publication9 and a search filter for clinical trial research (clinical trial [pt]) (corrected for sensitivity and precision).10 Finally, to shed light on the significance of retrospective registration, we mapped all trials both by year of registration and by year of first enrolment.
2. Developments at the 16 clinical trial registries that provide data to the ICTRP
We assessed how many clinical trials were registered each year at each of the 16 clinical trial registries that provided data to the ICTRP, for the period 2005–2013 (we chose this period because trials from before 2005 were only registered sporadically). For this analysis, we did not use our own data set as the ICTRP data that are publicly available are ‘deduplicated’.11 We collected data on numbers of interventional, non-deduplicated registered trials from the websites of the registries, and contacted the 16 registries and the ICTRP to ask for this information when it was not available online.
We also assessed at which registries trials were registered for each major geographical region of the world separately. As only our deduplicated data set contained information on a trial’s country of recruitment, we used this data set for the latter analysis.
3. Developments in trial registration in different regions of the world
We assessed how many clinical trials were registered for recruitment annually in various regions of the world. An algorithm was developed to extract the countries of recruitment from the country of recruitment field for each registered record in the ICTRP data set. Following this, the trials’ countries of recruitment were classified using the World Bank income group classification (February 2014 update) and the United Nations Statistics Division classification for geographical regions (downloaded on 23 July 2014). If a trial recruited in multiple regions, it was counted multiple times.
4. Comparison of registered trials with countries’ expenditures on health research
To be able to provide an insight into developments in the proportion of trials that were registered in various countries, we compared the annual number of trials registered for recruitment in these countries to the countries’ combined public and private expenditures on health research (under the assumption that if the number of trials registered increased relative to countries’ health research expenditures, the proportion of trials that was registered may have increased). Data on countries’ public and private health research expenditures combined were derived from publications by Chakma et al12 and Young et al,13 ,14 and were available from 2007 to 2012 for Australia, Canada, China, Europe, India, Japan, South Korea and the USA.
5. Case studies of India and Japan
Since the comparison of the annual number of trials registered for recruitment in the countries listed above to these countries’ health research expenditures showed especially marked increases for India and Japan (see Results, section 4), developments in clinical trial registration in India and Japan were analysed in more detail to understand what drove the increases in numbers of clinical trials registered in these countries. For trials that were registered for recruitment in these countries, we determined at which clinical trial registries these trials were registered. We also collected information on key events that may have driven clinical trial registration in these countries.
6. Additional characteristics of trials
To understand more about additional characteristics of the trials in our data set and to shed light on what types of trials were registered between 2004 and 2013, we also collected information on trials’ study phase and target sample size in addition to the information that we collected on trials’ countries of recruitment, and calculated aggregates for the period 2005–2013 (we chose this period because trials from before 2005 were only registered sporadically). Collecting information on other characteristics of interest was not possible for our data set because most data fields in the ICTRP data set do not consist of standardised categories; these are free-text. Several studies have been conducted on samples of the ICTRP data set in the past that have shed light on trials’ characteristics in terms of primary sponsor type, intervention type, study design, disease or other health problem under study and age and sex of study participants.15 ,16 In addition, some individual registries that provide data to the ICTRP do use standardised categories and provide opportunity for automated analyses of such characteristics.17 ,18
Results
Our search of the ICTRP database resulted in 223 181 studies, of which 36 658 studies were excluded because these were observational. In total, 186 523 interventional clinical trials with a registration date up to 31 December 2013 were included.
1. Trends in global clinical trial registration up to 2013
Figure 1 shows how many trials were registered each year globally from 1998 to 2013, and mentions several key events in clinical trial registration. The annual number of registered clinical trials increased substantially between 2004 and 2013, particularly between 2004 and 2005: from 3294 in 2004, to 15 752 in 2005, to 23 384 in 2013. This entails a sevenfold increase between 2004 and 2013, and a fivefold increase relative to the number of clinical trial publications. From 1999 to 2004, the ratio of the number of registered trials to the number of publications about clinical trials was 0.10, while from 2005 to 2013, this ratio was 0.61 (the ratios were 0.12 in 2004 and 0.53 in 2005).

Annual numbers of registered clinical trials on the International Clinical Trials Registry Platform (ICTRP) and annual numbers of publications about clinical trials on PubMed from 1998 to 2013. The first trials in the ICTRP database were registered in 1994; 15 trials registered from 1994 to 1997 are not shown in the figure (all registered at the Australian New Zealand Clinical Trials Registry (ANZCTR)). CONSORT, Consolidated Standards of Reporting Trials; EMA, European Medicines Agency; FDA, Food and Drug Administration; FDAAA, Amendments Act; ICMJE, International Committee of Medical Journal Editors; ICTRP, International Clinical Trials Registry Platform; ISRCTN, International Standard Randomised Controlled Trial Number Register.
Figure 1 also maps the numbers of registered clinical trials by year of first enrolment. By comparing these with the numbers of registered clinical trials by registration year, it becomes clear that the peak of trials registered in 2005 consisted partially of a ‘catch-up’ of trials with dates of first enrolment in earlier years. Moreover, this comparison shows that there is a gap of increasing size between these two time lines from 2010 to 2013. This gap exists because many trials are registered retrospectively (24.9% of all trials registered in 2013 reported a date of first enrolment in 2012 or in an earlier year; 12.2% in 2012, 5.2% in 2011, 2.8% in 2010, 1.7% in 2009, 1% in 2008 and 2% in 2007 or earlier). This means that an increasing proportion of trials with dates of first enrolment in these years had most likely not been registered yet on 31 December 2013.
2. Registered trials at the 16 clinical trial registries that provide data to the ICTRP
Figure 2 shows at which clinical trial registries clinical trials were registered from 2005 to 2013. ClinicalTrials.gov was the largest registry, with 128 976 registered interventional trials up to 31 December 2013. However, trials were increasingly registered at other registries from 2005 to 2013. This becomes clear particularly when the registries are mapped for each major world region separately (see online supplementary file 1). This analysis shows that in most regions, trials were increasingly registered at local registries, except in Europe, where rules and regulations around clinical trials were criticised for being excessively bureaucratic during this time period.19

Proportion of clinical trials on the International Clinical Trials Registry Platform (ICTRP) that is registered at each of the 16 national and regional registries that provide data to the ICTRP. Figure (A) shows the proportion of trials on ClinicalTrials.gov versus the 15 other registries. Figure (B) shows the proportion of trials on all registries except ClinicalTrials.gov. Legend is ordered by numbers of registered trials in 2013. In (B), registries with less than 500 registered clinical trials in 2013 were combined into ‘Other’ for legibility. The earliest registration date of a trial for each of the 16 national or regional registries that provided data to the ICTRP was in the following years: 1994, Australian New Zealand Clinical Trials Registry (ANZCTR); 1999, ClinicalTrials.gov; 2000, International Standard Randomised Controlled Trial Number Register (ISRCTN); 2004, EU Clinical Trials Register (EU-CTR); 2004, The Netherlands National Trial Register (NTR); 2005, Japan Primary Registries Network (JPRN); 2006, Chinese Clinical Trial Registry (ChiCTR); 2007, Clinical Trials Registry—India (CTRI); 2007, Sri Lanka Clinical Trials Registry (SLCTR); 2008, Cuban Public Registry of Clinical Trials (RPCEC); 2008, German Clinical Trials Register (DRKS); 2008, Iranian Registry of Clinical Trials (IRCT); 2008, Pan African Clinical Trial Registry (PACTR); 2010, Clinical Research Information Service (CRiS), Republic of Korea; 2010, Thai Clinical Trials Registry (TCTR); 2011, Brazilian Clinical Trials Registry (ReBEC). Totals do not add up to 100% because trials can be registered at more than one registry. For the same reason, the ‘Total non-ClinicalTrials.gov’ category in (A) and the ‘Other’ category in (B) may be slight overestimations. For CTRI and JPRN precise data on the annual number of registered interventional clinical trials could not be acquired; data were approximated from the overall number of studies (interventional and observational) on these registries’ websites and the distribution of interventional and observational trials from these registries on the ICTRP.
3. Developments in trial registration in different regions of the world
Information on trials’ country(ies) or region(s) of recruitment was available for 179 724 trials. Figure 3 provides an overview of how many trials were registered every year for participant recruitment in different parts of the world. From 1999 to 2004, the figure shows small increases in the annual numbers of trials registered for recruitment in Northern America and in Europe, corresponding to increases in numbers of trials registered at ClinicalTrials.gov, the International Standard Randomised Controlled Trial Number Register (ISRCTN), and the EU Clinical Trials Register (EU-CTR) (see figure 2). In 2005, the year that trial registration became a prerequisite for publication according to ICMJE guidelines, annual numbers of registered trials showed marked increases in all regions, particularly in Northern America and in Europe. In other regions, particularly Asia, the annual number of registered clinical trials increased more gradually and continued to increase up to 2013. Numbers of registered clinical trials were lowest in Africa, and in Latin America and the Caribbean. Finally, registration appears to show a second peak in Northern America in 2008.

Annual numbers of clinical trials on the International Clinical Trials Registry Platform (ICTRP) registered for recruitment in country income groups (A) and geographical regions (B) from 1998 to 2013. Legend is ordered by numbers of registered trials in 2013. Numbers for further regional disaggregation for the year 2013 do not add up to regional totals because trials were regularly registered for recruitment in multiple regions. Information on countries or regions of recruitment was available for 179 724 interventional trials. A total of 113 trials only specified a region of recruitment (eg, Asia) and not a country of recruitment, and were not included for the income group analysis.
4. A more detailed look at Asia: numbers of registered trials versus countries’ expenditures on health research
Given the marked, yet gradual increase in numbers of registered clinical trials between 2005 and 2013 in Asia, we took a closer look at developments in clinical trial registrations in this region. Was a gradually increasing proportion of trials registered in this region? Or, given the large increases in the annual health research expenditures of several Asian countries in recent years, was simply more money spent on health research, with larger numbers of clinical trials being the conducted as a result?12 ,13
To answer these questions, we compared increases in the numbers of clinical trials registered for recruitment in several Asian countries to these countries’ annual health research expenditures between 2007 and 2012. We did the same for Australia, Canada, Europe and the USA. Since these analyses took 2007 as a starting point, they provide insight specifically at increases in registration that occurred after the initial global registration peak of 2005. As figure 3 shows, most increases in Asia occurred after this initial peak, but increases in Northern America and Europe mostly occurred before this time period; so in these latter two we would expect little growth between 2007 and 2012.
The results of this analysis are presented in table 1. Indeed, the USA and Europe showed only marginal increases in annual numbers of registered trials from 2007 to 2012, in absolute terms and relative to their annual expenditures on health research. Compared to increases in the USA and Europe, increases in Canada and Australia were larger between 2007 and 2012. China and South Korea showed substantial increases in annual numbers of registered trials in the same period, but also saw large increases in their national health research expenditures. Finally, India and Japan saw large increases in annual numbers of registered clinical trials, in absolute terms and relative to the countries’ health research expenditures. The next section will look in more detail at what happened in these two countries that might have resulted in an increasing proportion of trials being registered.
Proportional increases in the annual number of registered clinical trials between 2007 and 2012 relative to proportional increases in national health research expenditures in eight selected countries
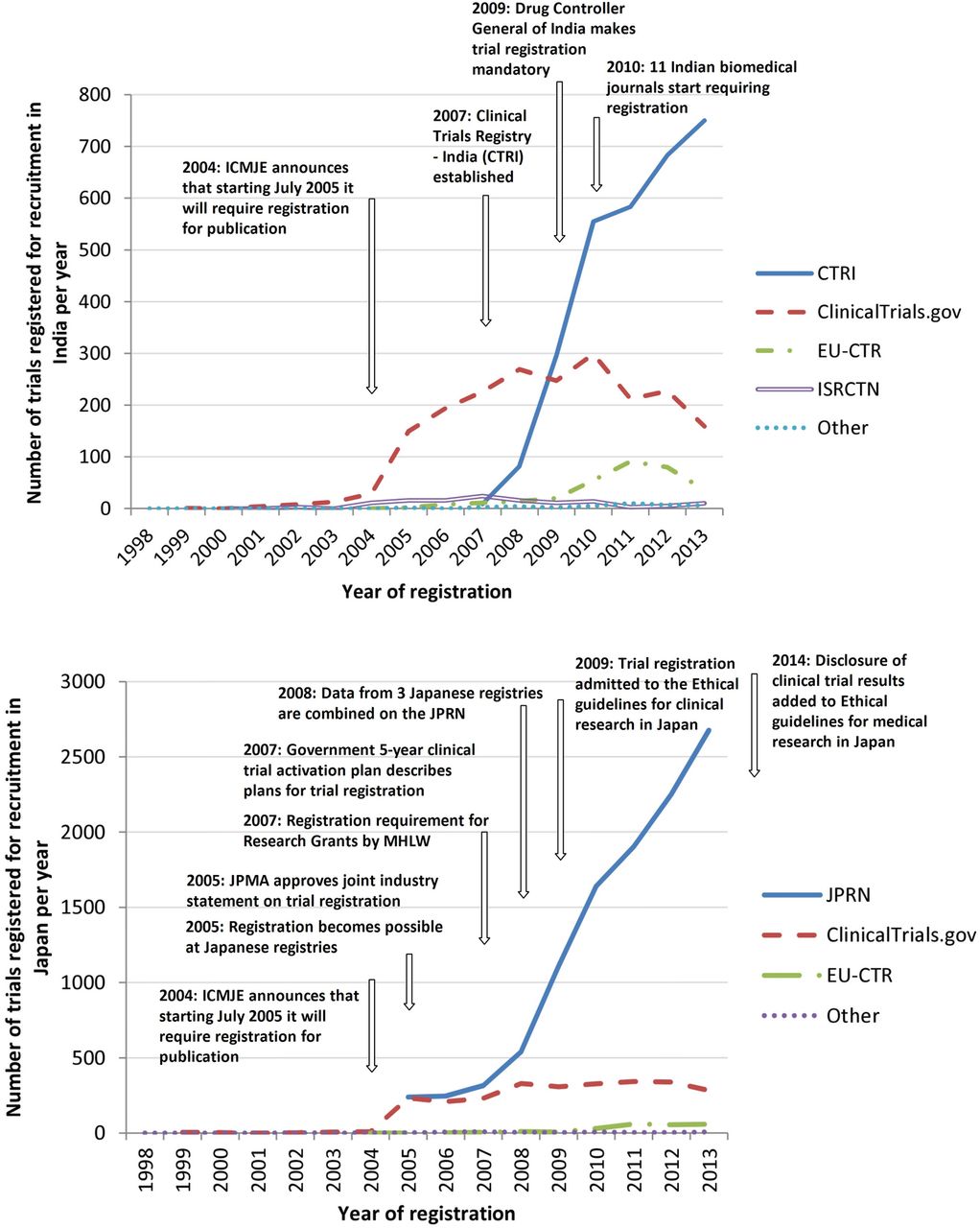
5. A more detailed look at India and Japan
Figure 4 provides more insight into developments in clinical trial registration in India and Japan. In both countries, the annual number of registered trials increased somewhat in 2005 after the ICMJE's statement on trial registration, but not as prominently as in Europe or Northern America. The annual number of trials registered only really gained momentum in these countries after several local measures were taken to enforce and encourage clinical trial registration. Notably, a large majority of the trials in India and Japan were registered at the countries’ national trial registries.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Developments in clinical trial registration in India and Japan. Legend is ordered by numbers of registered trials in 2013. Details on events related to clinical trial registration were mostly derived from Pandey et al,46 Shiokawa80 and Tang et al.48 Data are from our deduplicated data set that was downloaded from the ICTRP. A proportion (15.6%) of registered records of trials was excluded from this data set because the corresponding trials were registered at more than one registry. Thus, numbers of registered records for individual registries are in reality somewhat higher than in the graph. The non-deduplicated number of interventional trials registered for recruitment in India in 2013 at ClinicalTrials.gov, for example, was 199 (in graph 159) and for recruitment in Japan in 2013 was 363 (282 in graph) (numbers from ClinicalTrials.gov website). JPMA, Japanese Pharmaceutical Manufacturers Association; JPRN, Japan Primary Registries Network; MHLW, the Ministry of Health, Labour and Welfare; ICMJE, International Committee of Medical Journal Editors.
6. Trial characteristics
Besides looking at developments in clinical trial registration in different regions of the world, we also analysed the characteristics of the trials that were registered. Study phase and target sample size were assessed for all trials on the ICTRP that were registered between 2005 and 2013 (table 2). For 53.3% of these trials, the study phase was not available. When it was available, the distribution of trials was quite evenly spread across phase I trials (9.3%), phase II trials (13%), phase III trials (10.1%) and phase IV trials (8.7%).
Characteristics of all interventional clinical trials on the International Clinical Trials Registry Platform (ICTRP) registered from 2005 to 2013 (N=173 532)
The target sample size was not available for 6.9% of trials. For the remainder, the median target sample size was 74 (IQR: 34–200). Most trials were small and recruited between 10 and 100 participants (50.5%).
Table 2 also presents aggregate data for the period 2005–2013 for the registries at which the trials were registered and for trials’ regions of recruitment. To provide a recent overview of where registered clinical trials recruited participants globally, we also analysed the regions of recruitment for trials registered in 2013. In this year, 73.8% of trials with information on the country of recruitment were registered for recruitment in high- income countries, 20.2% in upper middle-income countries, 6% in lower middle-income countries and 0.8% in low-income countries. For the same year, 39% of trials were registered for recruitment in Asia, 28.1% in Northern America, 26.6% in Europe, 6% in Oceania, 3.6% in Latin America and the Caribbean and 2.4% in Africa (figure 3).
Discussion
Increasing utilisation of registered clinical trial data
Patients, healthcare workers, researchers and policymakers are increasingly making use of the information that is collected and made publicly available by clinical trial registries.7 ,15 Registration has brought improved access to information about clinical trials for patients, healthcare workers and researchers, particularly because all registered trials are now accessible through one global portal (the ICTRP search portal).11 Trial registration has also made important contributions to increasing the scientific value of clinical trial research. A key example of this is that trial registration is already helping to address the pertinent problems of publication bias and selective reporting bias by allowing reviewers to find non-published trials and non-published outcomes when conducting systematic reviews.20 ,21
Another useful application of clinical trial registration is that registered clinical trial data are increasingly being used to shed light on what clinical trial research is being conducted, where it is being conducted, by whom and how.16 ,22 Such insights into the global clinical trial enterprise can help in targeting the research that has the greatest potential public health benefit, and the ICTRP will likely constitute a useful data source for the recently established Global Observatory on Health Research and Development (R&D) (a new initiative at WHO that will aim to provide insight into what health R&D is being conducted globally).22 ,23 For example, this study showed that in recent years there were more clinical trials registered for recruitment in Asia than in Europe or the USA. Other studies have made clear that registered clinical trials are dominated by research into non-communicable diseases (80%), less than 20% of trials recruit children, more than 60% are sponsored by universities or hospitals and more than 50% investigate drugs.15 ,16 ,24
The use of registered clinical trial data for these purposes is valuable; however, it also raises questions. How many trials and what proportion of trials are registered at this moment? Also, how much information, and of what quality, is available about these trials?
Increases in the number and proportion of trials that are registered
This study shows that the number of trials that was registered every year increased from 3294 in 2004, to 15 752 in 2005, to 23 384 in 2013. Moreover, the proportion of trials registered each year globally appears to have increased substantially between 2004 and 2013, particularly between 2004 and 2005. In 2013, the number of clinical trials that was registered was fivefold that of what it was in 2004, relative to the number of publications about clinical trial research.
Other studies confirm that the proportion of trials that are registered has shown an upward trend, and show that at least 60% of all trials that were published were also registered in recent years (box 2).25 ,26 However, the proportion of published trials that is registered varies considerably as per type of research, per country and per journal in which the research is published (box 2).25–36 Our study too shows that developments in the number and proportion of trials that are registered have not taken place equally in all parts of the world. In Northern America and Europe, for example, increases in trial registration peaked in 2005, the year after the statement by the ICMJE on trial registration. However, in other regions, particularly Asia, trial registration developed more gradually. By looking in more detail at several Asian countries, our study shows that the annual number of registered clinical trials continued to increase substantially in China, South Korea, India and Japan after the initial global registration peak in 2005. In China and South Korea, these increases were accompanied by substantial increases in the countries’ expenditures on health research. This may suggest that while the number of annually registered trials increased, the proportion of trials registered may not have increased as much (however, caution is warranted in drawing such conclusions; we used countries’ expenditures on health research as a proxy for the number of trials being conducted in a country, but these two are not necessarily linearly correlated). India and Japan saw strong increases in numbers of registered clinical trials in absolute numbers and relative to their annual expenditures on health research, suggesting strong increases in the proportion of trials that was registered. This is why we studied developments in trial registration in these two countries in more detail.
How many published clinical trials are registered?
The proportion of all published clinical trials that is registered varies considerably per research area and per journal. This proportion has been shown to be: approximately 30% for trials published in physiotherapy journals,28 ,29 yet 75% for trials that are published in the top 10% of these journals;28 21% for trials that are published in top psychosomatic and behavioural health journals;30 24% for randomised controlled trials (RCTs) in kidney transplantation;31 59.4% for trials published in urology-related journals, but 71% if the journal mentioned trial registration in its author requirements;32 and 87% for RCTs in the 10 highest ranked surgery journals (by impact factor) that also required trial registration.33
Registration rates also vary per country: among USA-sponsored trials advertised to Russian patients and physicians one-third of the trials on ClinicalTrials.gov did not disclose a Russian location of recruitment, and only 16.9% of publications of RCTs with a Latin American first author reported that the trial was registered.34 ,35
Analysis of RCTs across all research areas and countries shows that 37% of publications of trials in 2007 reported that the trial was registered.26 In 2010, 55% did so, while additional searching showed that at least 61% of the trials was registered (64% in ICMJE journals and 52% in non-ICMJE journals).25 This trend is in line with the increasing numbers of registered trials observed in this study, and with other authors who have reported that registration rates improved over time for their subsamples.29 ,31 ,32 ,36
Finally, it should be noted that the proportion of all trials that is registered—not just the proportion of published trials—is likely lower than the 61% discussed above, assuming that investigators’ reasons for not publishing a trial may overlap with their reasons for not registering a trial (potentially leading to a smaller proportion of trials that is registered among unpublished trials).
Global and local reasons for good and poor compliance with registration in different regions
Global reasons
There have been several global measures between 2004 and 2013 that have helped to provide an impetus for clinical trial registration. Examples include: codes of research practice, such as the SPIRIT and CONSORT statements that have been revised to recommend the admission of trial registration details to both clinical trial protocols and reports;37 ,38 statements from professional organisations supporting trial registration, such as the declaration of Helsinki;39 and statements by pharmaceutical industry associations supporting trial registration.40 A particularly influential global measure was the ICMJE's announcement that it would require trial registration as a condition for publication in 2004, which led to a substantial increase in the number of trials registered in 2005.41
These measures have made an important contribution to stimulating trial registration, but have not been a panacea. The ICMJE's policy, for example, only impacts a subsection of all trials: more than 50% of all trials are never published1 and some trials may not even be conducted with the goal of publication. The ICMJE's recommendations have also lacked widespread implementation: the percentage of English-language journals that actually requires or encourages trial registration is 30%, and even these journals often do little to check compliance with registration.42 This proportion is likely to be lower for non-English language journals, since registration rates are significantly lower in these journals.28 Moreover, this study shows that while the number of trials registered for recruitment in Europe and Northern America rose steeply after the ICMJE's announcement, increases in other regions were more gradual. In Asia, particularly, clinical trial registration only really gained momentum after a range of local measures were implemented (in Europe and the USA, many such measures had already been implemented at the time of the ICMJE's announcement).
Local reasons
Arguably, the most important local measure that can be taken is to make registration mandatory by law.43 Although our analysis was not developed to provide evidence to this end, there may be some indications of the effects of legislation in our results: registration appears to show a peak in Northern America in 2008, 1 year after implementation of legislation that expanded the scope of trial registration in the USA;44 and in Canada and Australia, countries that had no legislation on trial registration, when the ICMJE issued their statement on trial registration in 2004, the number of registered trials increased more slowly than it did in Europe and the USA, where legislation on trial registration already existed at the time.
In an increasing number of countries laws that mandate trial registration exist, including: Argentina, Brazil, Canada (since 2014), EU member states, India, Israel, South Africa and the USA.43 ,45 However, in most countries, particularly in low- and middle-income countries, such legislation remains absent. Moreover, even in countries with legislation on trial registration, the law tends to not cover all clinical trials (excluding, eg, non-medicine or device trials and phase I trials),15 ,44 thus explaining the low registration rates that are found for clinical trials that fall outside these parameters, such as physiotherapy trials or behavioural trials (box 2).28 ,30
Besides legislation, there are several other local measures that can have a significant impact on the proportion of trials that are registered in a country. Japan, for instance, a country that lacks a comprehensive law on trial registration, still saw substantial increases in numbers of registered trials in recent years. One particularly important measure has been the establishment of national, local-language registries.7 The number of national and regional registries that provide data to the ICTRP has risen from 3 to 16 since the ICTRP's establishment and in most regions, there has been a trend towards trials being registered at such registries (figure 4; online supplementary file 1). Besides offering opportunity for registration of trials in the national language, these local registries can galvanise the establishment of other enforcement measures by advocating for the establishment of local legislation and policies on registration.7 ,46
Other local measures that have helped to stimulate trial registration include: enforcement of registration by funders, ethics committees and local journal editors;46 ,47 national policies and ethical guidelines that encourage trial registration;48 and self-regulation by universities 45 and the pharmaceutical industry.40 Japan and India provide good examples of how clinical trial registration increased when a range of these measures were implemented (figure 4). A key example also comes from the UK, where registration was recently made a condition for ethics approval for all clinical trials.49 Chalmers’ follow-up suggestion to automatically generate trial registration entries from applications to the UK's integrated research application system appears particularly practical.49 Another example comes from the US National Institutes of Health (NIH) that have recently issued a draft policy for public comment on clinical trial registration.44 Importantly, both the UK ethics initiative and the NIH initiative supplement existing EU and USA legislation by requiring registration for any clinical trial, regardless of the type of intervention and study phase.
The problem is that many of these successful measures have lacked widespread implementation. In most countries, particularly in low- and middle-income countries, the absence of legislation on registration, of a national registry and of policies on registration by ethics committees, funders and journal editors leaves much room for investigators to not register their trials. The low registration rates that have been found for trials in Latin American and Caribbean countries, for example, may well be explained by the relative absence of such developments in these countries.34 The knowledge needed to redress the lack of compliance in these countries exists; implementation of local measures that have proven effective and improved trial registration rates elsewhere would be likely to greatly help improve compliance in these countries as well.
Other remaining challenges for clinical trial registration
The challenge of lacking compliance is key for clinical trial registration, but there are several other issues that will require attention in the future to allow for the benefits of clinical trial registration to be realised, particularly in the areas of: (1) data quality, (2) (in)accessibility of protocols, results and participant-level data, and (3) searchability, data aggregation and linking at the ICTRP and registries. These are discussed here below.
Data quality
Although the ICMJE has stated that “trial registration with missing or uninformative fields for the minimum data elements is inadequate”,50 many registered records of clinical trials are currently incomplete, not accurate, not up-to-date or retrospectively registered.15 ,51 ,52 For example, listed primary outcome measures are often not specific enough to allow for the detection of selective reporting.15 ,21 ,41 ,51
Retrospective registration means that, in contrast with ICMJE and WHO guidelines, many trials are registered after they have begun recruiting participants. In this study, one-quarter of all trials registered in 2013 started recruitment in an earlier year, but the rate of retrospective registration in reality is even higher: when we look per month, instead of per year, 48% of trials registered in 2012 were registered retrospectively.15 This is a major problem because when trials are registered retrospectively, we cannot be sure that they were not registered to favour a particular result.
A key solution to the problem of lacking data quality is to improve the data recording formats and quality control measures at registries (there are large variations between registries in this regard15). The ICTRP has attempted to encourage such improvements by publishing the International Standards for Clinical Trial Registries in 2012.53
(In)accessibility of protocols, results and participant-level data
This study has focused on exploring developments in clinical trial registration in different parts of the world; however, the registration of a trial is just a first step. It is equally important that a trial's protocol, summary results, full study report and participant-level data set can be accessed. However, research has shown that these are only rarely available.2 Moreover, more than half of all trials are never published in journals.1 Several countries, such as the USA, EU, Canada and Japan, as well as the WHO have implemented measures to redress the lack of availability of trial results.19 ,44 ,54–66 Unfortunately, as for improving compliance with registration itself, these local measures have not been widely implemented; similar measures remain absent in many other countries. In terms of achieving sharing of participant-level data sets, less progress has been made.2 ,67 However, there are strong signs that sharing of participant-level data sets is becoming broadly accepted as the new standard in clinical trial transparency and that progress in this area can be expected in the near future.66 ,68–73
Searchability, data aggregation and linking at the ICTRP and registries
The establishment of the ICTRP in 2006 was an important step forward for clinical trial registration. The ICTRP has contributed to the development of standards both for clinical trial registries 53 ,74 and for the data that are collected for each trial.8 Most importantly, the ICTRP has linked data from individual clinical trial registries and its search portal serves as a single point of access to all registered clinical trials for patients, healthcare workers, researchers and policymakers.
As the single point of access to all registered clinical trials, it is important that the ICTRP database is searchable for individual records, that it provides opportunity for aggregate analyses, and that it links to the related trial documents and data mentioned in the previous section (protocols, summary results, clinical study reports, publications and participant-level data). There is potential for improvement in how the ICTRP enables these functions. First, in terms of searchability, the ICTRP provides various search functions on its portal, including an advanced search function and a search filter for trials in children. However, improvements to the ICTRP's search interface are possible: Glanville et al75 recently concluded that the ICTRP's search interface lags behind the interfaces of major bibliographic databases. Second, providing opportunities for aggregate analyses is a particular challenge for the ICTRP given that it combines data from 16 different registries. The ICTRP has made good progress in this area since it started, but many of the relevant data fields are still not available in standardised, categorised formats. Looking ahead to the establishment of the Global Observatory on Health R&D,23 and the role that data from the ICTRP might play in this Observatory,16 ,22 it is important that the ICTRP's opportunities for aggregate analysis are improved. Third, as the single point of access to all registered clinical trials, the ICTRP is well-placed to provide links to all related documents and data for each clinical trial, such as protocols, various types of results and participant-level data, but it currently does not provide fields for such links. By making available such links when they exist, the ICTRP could not only become the single point of access to all registered clinical trials, but also for access to all information on each registered trial, which would significantly improve the accessibility of that information.
Since individual registries are the point of access to clinical trials for people living in a specific country or a region, and often provide data in a local language, it is of equal importance that registries provide adequate search functions, aggregate analysis possibilities, and links to protocols, results and participant-level data. However, many of the areas in which there is potential for improvement at the ICTRP are also areas for potential improvement for the 16 registries that provide data to the ICTRP. The search function quality, aggregate analysis possibilities and provision of links vary greatly per registry.15 ,75 ,76 Both registries and the ICTRP could learn more from successful approaches in these areas at other registries.15
Limitations
The ICTRP currently accepts data from 16 national and regional registries around the world that comply with a range of quality criteria.74 There are other registries for clinical trials (eg, for the pharmaceutical industry); so we may not have captured all registered clinical trials globally in this study. However, there is broad endorsement for trial registration in WHO-approved registries; most of the laws that legislate clinical trial registration and the ICMJE's registration policy prescribe that trials must be registered in a registry that provides data to the ICTRP.50 Therefore, any information missed from registries that are not included should be limited.
In this study, we aimed to shed light on developments in the number and the proportion of clinical trials that were registered from 2004 to 2013. However, a key limitation in conducting this analysis was that for calculating the proportion of trials that were registered, information on the denominator for this calculation—the actual numbers of clinical trials that were conducted—was missing. To shed light on developments in the proportion of clinical trials that were registered, we compared annual numbers of registered clinical trials to annual numbers of publications about clinical trial research and to countries’ expenditures on health research, under the assumption that if the number of trials had increased relative to these proxies, the proportion of trials that was registered may also have increased. By demonstrating the strong increases in numbers of registered trials relative to these proxies during a short time period, and by drawing on literature that has also provided indications of trends towards increasing compliance with registration (box 2), we believe to have made it plausible that—like the number of clinical trials that were registered—the proportion of clinical trials that was registered increased between 2004 and 2013, particularly between 2004 and 2005.
This study was limited to investigating how the registration of clinical trials developed between 2004 and 2013 in different parts of the world and what factors drove those developments. However, many of the rationales for registering clinical trials also apply to other types of research.77 ,78 Efforts to enforce and encourage registration of other types of research have progressed much less than for clinical trial research, but observational studies can be registered at most clinical trial registries, and a register for systematic reviews has also been established.79 In our data set, 16% of all studies was observational. Since there has been much less enforcement of registration of observational research to date than of clinical trial research, we excluded these observational studies from our study, so as to not let these distort our findings.
Conclusion
Clinical trial registration has improved transparency in clinical trial research by increasing access to information on clinical trials around the world. More than 20 000 clinical trials are now newly registered every year at 16 national and regional registries, and healthcare workers, researchers, patients and policymakers are increasingly benefiting from the advantages offered by clinical trial registration. However, this study shows that trial registration has not developed equally in all parts of the world, and that good compliance with registration requires a coalescence of global and local measures that enforce and encourage registration. As local measures are not in place in most countries, compliance with registration remains a significant challenge that continues to undermine the potential benefits of clinical trial registration. Other important challenges that remain include substandard quality of data in registered records of trials, inaccessibility of protocols, results and participant-level data, and the potential for improvement in registries’ and the ICTRP's searching, aggregating and linking functions. For most of these challenges, effective solutions are available, but there is lack of widespread implementation. National and regional registries around the world and the ICTRP have played a leading role in the implementation of such solutions in the past. It is important that they are supported to address the challenges that remain in the future, so that we can progress further towards the goal of full accessibility to information on all clinical trials’ methods and results.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors RFV conceived the idea for this study and designed the methods. RFV and KL conducted data collection and analysis for the article. RFV wrote the first draft of the article. KL contributed to writing the article. All authors approved of the manuscript. RFV is the guarantor of the article.
Funding No specific sources of funding for this research project. Both authors were salaried by their institutions while working on the project.
Competing interests All authors have completed the Unified Competing Interests form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work. RV and KL has conducted consultancy projects for the WHO on the topic of clinical trial registration; have no other financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; have no other relationships or activities that could appear to have influenced the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data used for this study can be freely downloaded from the International Clinical Trials Registry Platform (ICTRP) search portal at http://apps.who.int/trialsearch/ and from the websites of some of the 16 individual registries. Some data were sent to us by these registries when they were not publicly available; these can be requested from the authors at rviergever@research4health.org.