Article Text

Abstract
Objectives To systematically review the efficacy of collaborative care (CC) for depression in adults with coronary heart disease (CHD) and depression.
Design Systematic review and meta-analysis.
Data sources Electronic databases (Cochrane Central Register of Controlled Trials MEDLINE, EMBASE, PsycINFO and CINAHL) were searched until April 2014.
Inclusion criteria Population, depression comorbid with CHD; intervention, randomised controlled trial (RCT) of CC; comparison, either usual care, wait-list control group or no further treatment; and outcome, (primary) major adverse cardiac events (MACE), (secondary) standardised measure of depression, anxiety, quality of life (QOL) and cost-effectiveness.
Data extraction and analysis RevMan V.5.3 was used to synthesise the data as risk ratios (RRs), ORs and standardised mean differences (SMD) with 95% CIs in random effect models.
Results Six RCTs met the inclusion criteria and comprised 655 participants randomised to CC and 629 participants randomised to the control group (total 1284). Collaborative depression care led to a significant reduction in MACE in the short term (three trials, RR 0.54; 95% CI 0.31 to 0.95, p=0.03) that was not sustained in the longer term. Small reductions in depressive symptoms were evident in the short term (6 trials, pooled SMD −0.31; 95% CI −0.43 to −0.19, p<0.00001) and depression remission was more likely to be achieved with CC (5 trials, OR 1.77; 95% CI 1.28 to 2.44, p=0.0005). Likewise, a significant effect was observed for anxiety symptoms (SMD −0.36) and mental QOL (SMD 0.24). The timing of the intervention was a source of between-group heterogeneity for depression symptoms (between groups p=0.04, I2=76.5%).
Conclusions Collaborative depression care did not lead to a sustained reduction in the primary MACE end point. Small effects were observed for depression, depression remission, anxiety and mental QOL.
Trials registration number PROSPERO CRD42014013653.
- CARDIOLOGY
- MENTAL HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Systematic review of randomised controlled trials and a priori defined primary and secondary outcomes.
Exhaustive literature search and additional unpublished data provided by 5 of 6 trials.
GRADE rating of strength of evidence as moderate.
Heterogeneity observed between studies.
Few studies performed outside of the USA.
Insufficient healthcare cost data.
Introduction
Depression is widely reported to lead to an adverse coronary heart disease (CHD) prognosis,1 ,2 poorer quality of life (QOL)3 ,4 and high healthcare costs.5 Despite ongoing efforts to better identify and treat depression,6 prior psychological and pharmacological interventions designed especially for the CHD population have reported markedly lower effect sizes than has been observed among other chronic diseases such as diabetes.7 ,8 Moreover, large trials such as the landmark Enhancing Recovery in CHD (ENRICHD) study9 did not lead to a significant reduction in major adverse cardiac events (MACE), raising questions about the design10 and acceptability11 of depression interventions in the population with CHD.
Collaborative care (CC) is emerging as a promising model of healthcare among populations with complex mental health needs12 and mental disorders comorbid with chronic diseases including diabetes and CHD.13 ,14 CC is defined by a multiprofessional approach to patient care delivered by a primary care physician (PCP) and at least one other health professional, involving a structured patient management plan and interventions, scheduled patient follow-ups, and enhanced interprofessional communication between the multiprofessional teams.13 Prior systematic reviews have not reported on the efficacy of CHD studies in particular,15 ,16 although mixed CHD and diabetes samples are commonplace.13 Several large prospective randomised controlled trials (RCTs) of CC versus usual care have been reported recently,17–19 making it feasible to examine the efficacy and early benefits of CC, which might in turn assist in the design of subsequent trials and inform clinical practice. This systematic review extends beyond previous studies by reporting the efficacy of CC for depression in adults with comorbid depression and CHD.20
Methods
Search strategy
This review conformed to the PRISMA guidelines21 and a protocol has been published elsewhere.20 Electronic databases were searched without language restrictions until April 2014: the Cochrane Central Register of Controlled Trials (CENTRAL) on The Cochrane Library, MEDLINE, EMBASE, PsycINFO and CINAHL. The search string exploded the topics CHD, depression and RCT, as reported previously.20 Hand searching reference lists of articles selected for full text supplemented electronic searches. The principal investigators of studies were contacted to ascertain unpublished data and their knowledge of any other CC trials not included in our primary search. Additional data were provided for five trials17 ,18 ,22–24 and no response was received from the TrueBlue study authors.19
Inclusion criteria
Population: RCT studies were performed among adults (18 years and older) with comorbid depression and CHD. Depression was defined as depression disorder or clinical depression assessed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD) by a standardised interview (eg, Structured Clinical Interview, Composite International Diagnostic Interview) or a validated self-reports or rating scales with specific cut-off points for depression. Mixed samples (eg, heart failure, arrhythmia, diabetes) were eligible if ≥50% of the sample had a CHD diagnosis.
Intervention: CC intervention is defined as a coordinated model of care involving multidisciplinary healthcare providers, including: (1) at least one health professional (eg, nurse, psychiatrist, psychologist) in addition to the PCP; (2) a structured patient management plan that delivers either a pharmacological or a non-pharmacological depression intervention; (3) scheduled patient follow-up and (4) enhanced interprofessional communication between the multiprofessional team. CC may include usual CHD care or blended depression-CHD care.
Comparison: control group was defined as either (enhanced) usual care, wait-list control (WLS) group or no further treatment for comorbid depression-CHD.
Outcomes: primary; all-cause and CHD-related mortality as well as MACE (eg, subsequent myocardial infarction (MI), coronary revascularisation procedure, incident heart failure (HF), stroke).
Secondary: secondary outcomes include depression, anxiety and QOL (measured either dimensionally or categorically) following the intervention assessed by validated self-report questionnaires or standardised interviews. In addition, we considered economic evaluations of healthcare costs or resource utilisation including cost-effectiveness (incremental cost-effectiveness ratio) and cost-utility (quality-adjusted life years).
Study selection process, risk of bias and assessment
Two reviewers (PJT and HB) independently screened abstracts and articles for eligibility. In the case of title/abstract disagreements, the study was subjected to full-text review and disagreements were resolved by discussion. Two reviewers (PJT and HB) independently assessed included studies using the Cochrane Collaboration's tool for assessing risk of bias.25 The tool covers sequence generation, allocation concealment, selective outcome reporting and other sources of bias. Adjudication of the strength of evidence for each end point was made according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria with GRADE Profiler 3.6.1.26
Synthesis of data and summary measures
Standardised mean differences (SMD) for continuous variables, risk ratios (RR) for MACE and ORs for dichotomous end points are reported with 95% CI. Data were pooled together with random effects models using the inverse-variance method.25 ,27 To evaluate the presence of publication bias, the funnel plot was inspected. All analyses were performed with RevMan V.5.3.
Results
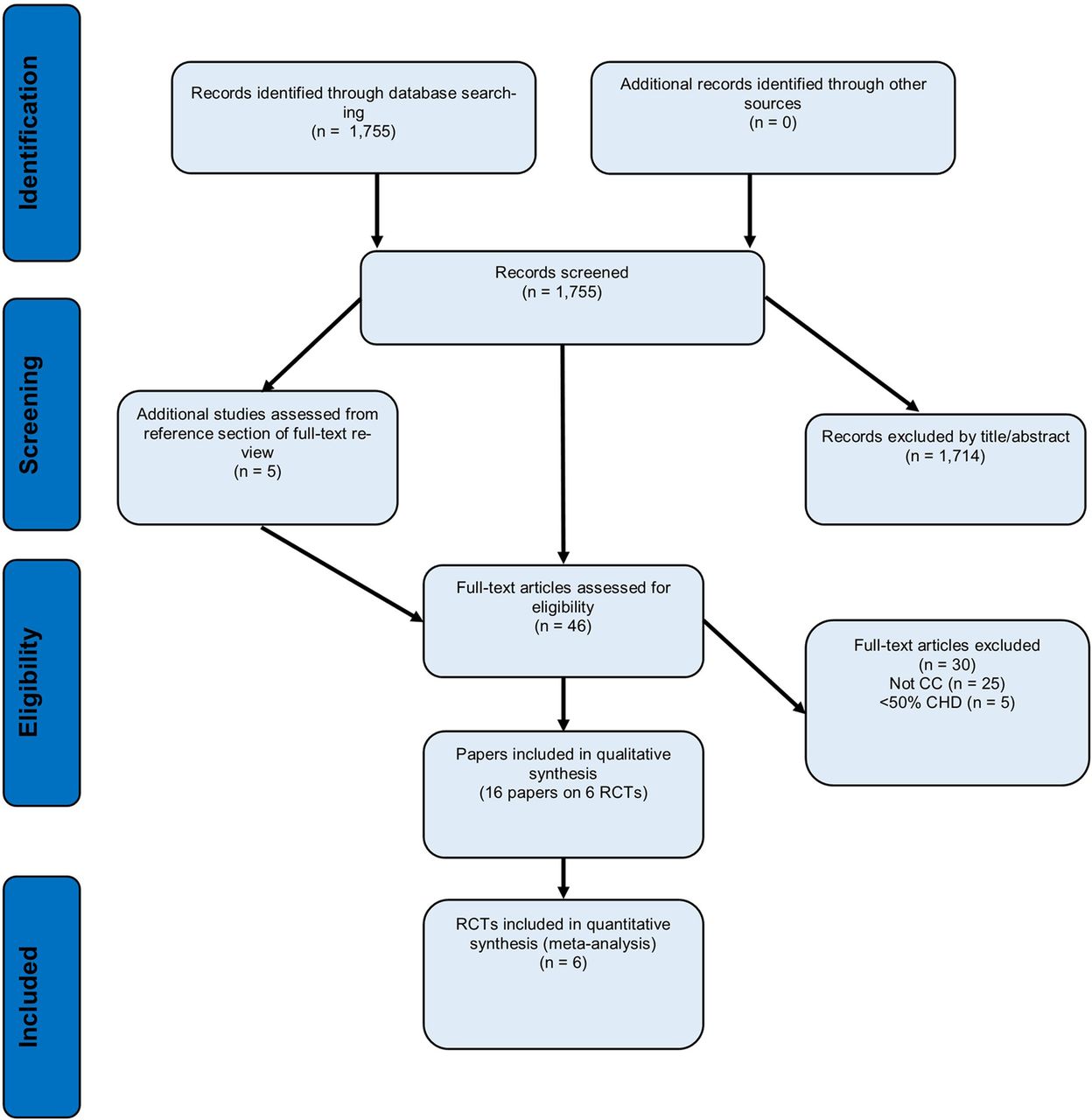
The search yielded 1755 citations from which 46 articles were reviewed in detail, and 16 papers were retained which reported on 6 RCTs (figure 1). Five CC trials performed with diabetes and CHD or mixed chronic disease populations were excluded as they did not meet the threshold of more than 50% of patients with CHD.13 ,28–31 Two trials were close to meeting the definition of CC for depression comorbid with CHD, but were excluded. The Identifying Depression as a Comorbid Condition (IDACC)32 study was excluded as the intervention did not initiate pharmacological or non-pharmacological depression treatment and did not involve structured follow-up of participants to augment treatment if necessary. The UPBEAT-UK study33 was excluded as the intervention was a case-management intervention and did not incorporate other healthcare professionals such as the PCP.
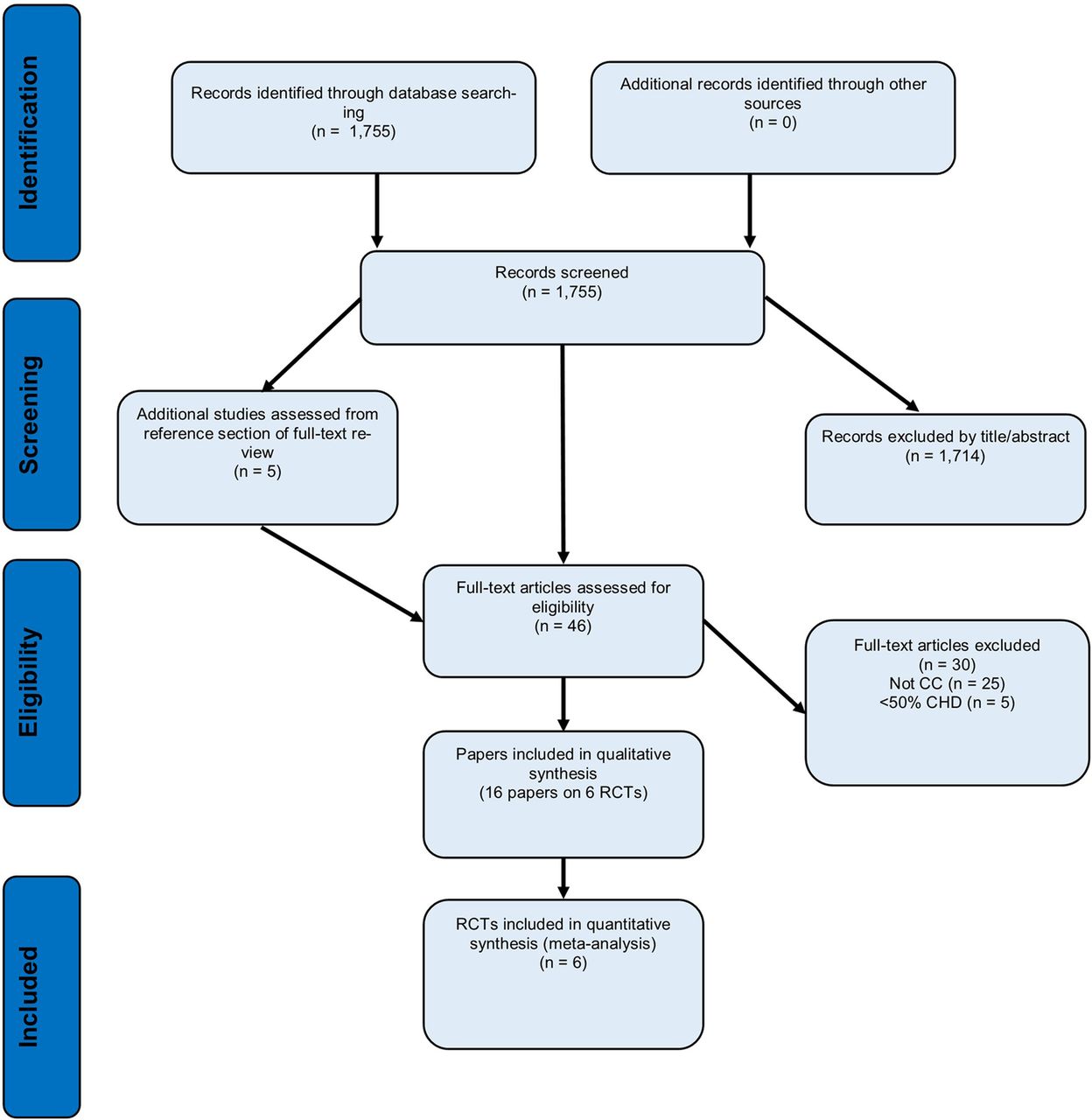
Flow chart of article selection (CC, collaborative care; CHD, coronary heart disease; RCT, randomised controlled trial).
The 6 RCTs that met the inclusion criteria comprised a total of 1284 patients with comorbid depression and CHD: 655 participants randomised to CC and 629 participants randomised to a control group. A description of the included trials is shown in table 1. The median proportion of participants with CHD in the trials was 78.9%, suggesting a high representative sampling of the chronic disease understudy. The median sample size was 179 participants per study with a median of 47.6% female participants. Four trials recruited participants from multiple sites11 ,34–36 and two trials were performed at a single centre.17 ,37 Five trials were from the USA17 ,18 ,22–24 and one trial was performed in Australia.19 The comparison group was usual care or enhanced usual care in five studies consisting of informing participants’ PCP17 ,18 ,22–24 and one trial used a WLC group.36
Characteristics of included CC studies in the treatment of comorbid depression and CHD
Depression screening questionnaires varied only minimally. Depression was assessed with the Patient Health Questionnaire (PHQ) to determine study eligibility in four trials.17 ,19 ,23 ,24 Specifically, three trials used a two-step screening approach with the PHQ-2 and a PHQ-9 for participants with an initial positive depression response on the PHQ-2.17 ,35 ,37 These trials used a moderate depression threshold consisting of PHQ-9 total scores ≥10.17 ,35 ,37 The TrueBlue study36 included patients with mild depression symptoms consisting of PHQ-9 scores ≥5. In the Coronary Psychosocial Evaluation Studies (COPES) and Comparison of Depression Interventions after Acute Coronary Syndrome (CODIACS) trials, the Beck Depression Inventory (BDI) was used for screening and trial eligibility.11 ,34 The clinical cut-off was set at ≥10 on at least two different screening occasions in COPES.11 In CODIACS,34 the clinical cut-off was set at BDI ≥10 on at least two different screening occasions or BDI ≥15 on one occasion. Five of the trials utilising either the PHQ-917 ,36 ,37 or BDI11 ,34 to determine trial eligibility also used the same measure for depression symptom response at the conclusion of the trial. The Bypassing the Blues trial employed the Hamilton Rating Scale for Depression24 for depression symptom clinical response.
CC was managed by an allied health team in two trials,11 ,34 by nurses in two studies35 ,36 and by social workers in two studies.17 ,37 The CC intervention duration ranged from 3 to 12 months and the median duration was 6 months. The psychotherapy component of the CC package consisted of problem-solving therapy in two studies,11 ,34 telephone-delivered manualised CBT in one study,37 referral to community mental health services in two studies,35 ,36 and was mixed in another study.17 The pharmacological component of the trials varied. In Bypassing the Blues,35 depression pharmacotherapy consisted of citalopram, serotonin norepinephrine reuptake inhibitor (SNRI) or bupropion. In CODIACS,34 depression pharmacotherapy consisted of sertraline, citalopram or bupropion. In COPES,11 pharmacotherapy consisted of sertraline, escitalopram, venlafaxine, bupropion and mirtazipine. In Management of Sadness and Anxiety in Cardiology (MOSAIC),37 depression pharmacotherapy consisted of selective serotonin reuptake inhibitor (SSRI, most commonly citalopram), SNRI, bupropion, mirtazapine and anxiety treatment with SSRI or benzodiazepine. In Screening Utilization and CC for More Effective and Efficient Treatment of Depression (SUCCEED),17 depression pharmacotherapy consisted of SSRI. No specific depression pharmacotherapy regimen was reported in TrueBlue.36
Risk of bias
Risk of bias varied in the included primary trials (see eSupplement 1). Missing trial characteristics were common despite all studies having published a trial protocol. In four trials, the allocation concealment was unclear. Blinding to subjective end points was rated as high in all studies. Selective reporting was noted in three studies because of discrepancies in the study end points reported in the protocol in comparison with the primary trial results.
Primary outcome: major adverse cardiac events
Three trials reported MACE18 ,24 ,38 and pooling all data irrespective of follow-up showed that CC did not reduce MACE (RR=0.87; 95% CI 0.53 to 1.42, p=0.20, I2=39%). CC was associated with significant reduction in MACE during the short to medium term (RR=0.54; 95% CI 0.31 to 0.95, p=0.03) that was not sustained in the long term (>12 months follow-up) where only the COPES trial39 reported MACE (RR 1.04; 95% CI 0.51 to 2.14, p=0.91) (figure 2). There was no association with mortality (5 trials, RR 1.38; 95% CI 0.53 to 3.58, p=0.51).

Forest plot showing the risk ratio for MACE postintervention in collaborative care studies versus usual care or waiting list control (short and medium terms). MACE, major adverse cardiac events; IV, inverse variance; CODIACS, Comparison of Depression Interventions after Acute Coronary Syndrome; COPES, Coronary Psychosocial Evaluation Studies.
Secondary outcomes
Depression symptoms and remission
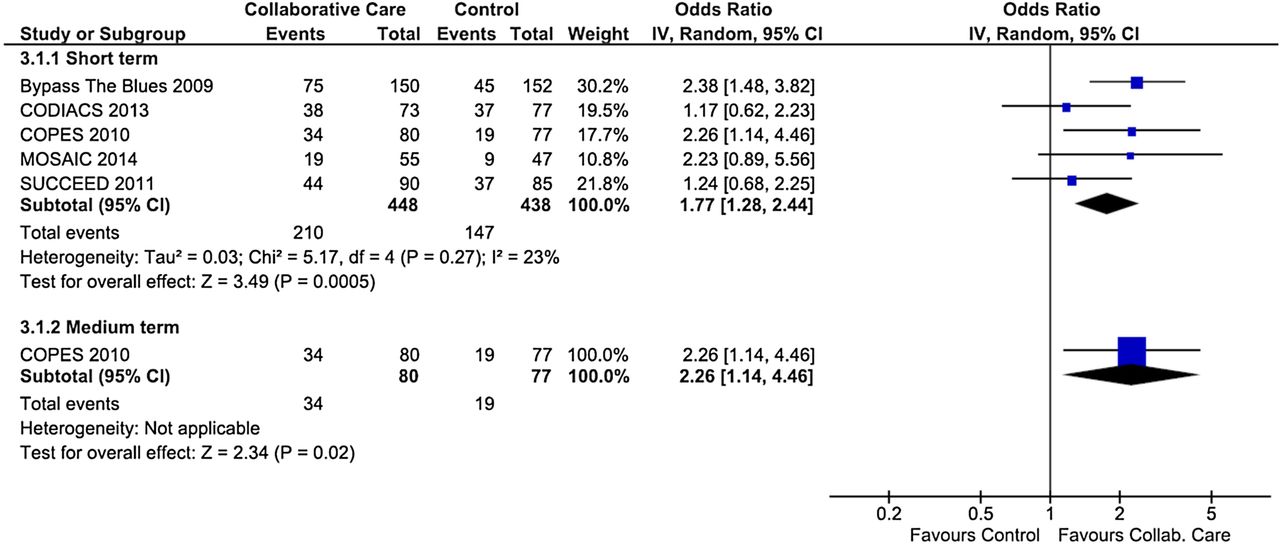
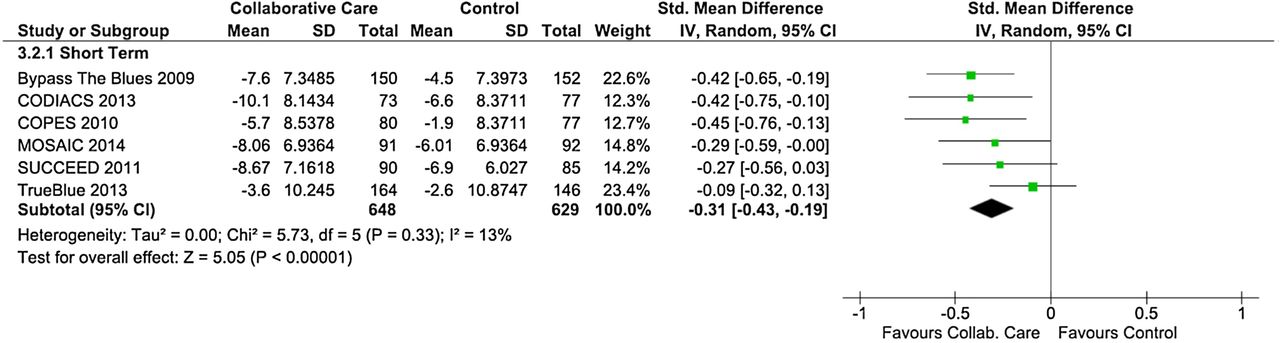
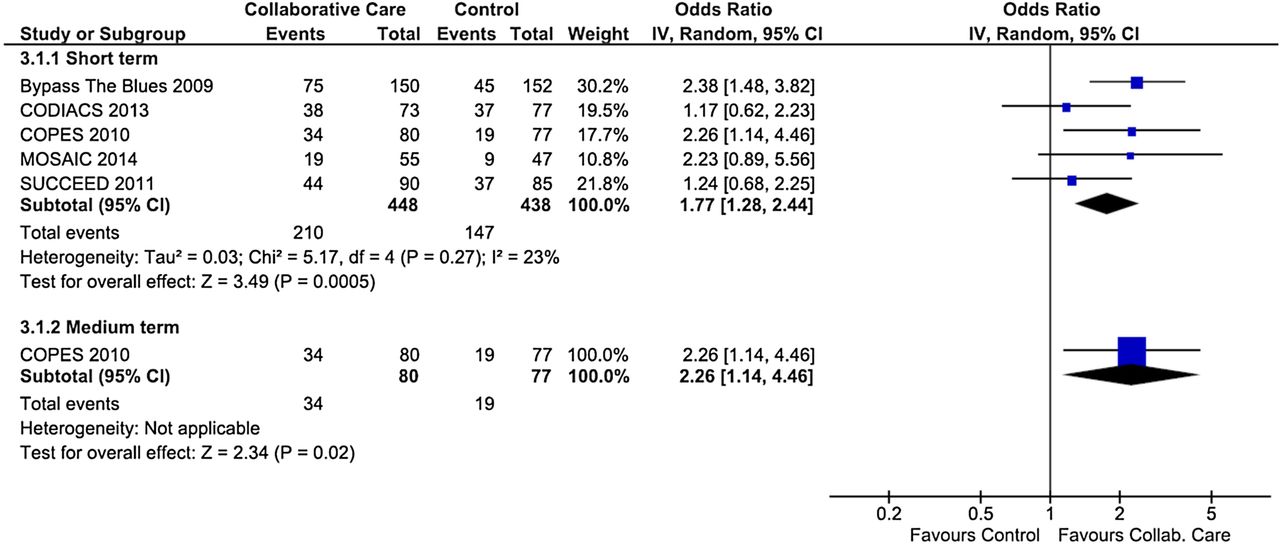
All six trials reported a change in self-reported depression symptoms by 6 months postintervention. CC was associated with a significant reduction in depressive symptoms (pooled SMD −0.31; 95% CI −0.43 to −0.19, p<0.00001: I2=13%) (figure 3). There was no depression symptom data available in the medium or long term. Four trials reported depression remission or clinically significant depression response and additional data were provided by the MOSAIC trial.23 CC was significantly associated with depression remission (OR=1.77; 95% CI 1.28 to 2.44, p=0.0005: I2=23%) (figure 4). In the medium term, only the COPES trial39 reported depression response based on the BDI ≤10 (OR 2.26; 95% CI 1.14 to 4.46, p=0.02). Since the COPES trial39 reported similar depression remission results in the short to medium term, pooling all depression remission data in the five trials, irrespective of the time frame, indicated similar results.

Forest plot showing depressive symptoms in collaborative care studies versus usual care or waiting list control (short term). IV, inverse variance; SD; CODIACS, Comparison of Depression Interventions after Acute Coronary Syndrome; COPES, Coronary Psychosocial Evaluation Studies; SUCCEED, Screening Utilization and CC for More Effective and Efficient Treatment of Depression, MOSAIC, Management of Sadness and Anxiety in Cardiology.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing depression remission in collaborative care studies versus usual care or waiting list control (short and medium terms). IV, inverse variance; CODIACS, Comparison of Depression Interventions after Acute Coronary Syndrome; COPES, Coronary Psychosocial Evaluation Studies; SUCCEED, Screening Utilization and CC for More Effective and Efficient Treatment of Depression, MOSAIC, Management of Sadness and Anxiety in Cardiology.
Other secondary outcomes
The forest plots for each of the secondary end points are reported in eSupplements 2 to 5. Four trials reported anxiety symptom change. It was found that CC led to a small, but significant reduction in anxiety symptoms in the short term (SMD −0.36; 95% CI −0.54 to −0.17, p=0.0001: I2=25%). CC was also associated with a significant improvement in mental QOL in the short term across five trials (SMD 0.23; 95% CI 0.08 to 0.38, p=0.003: I2=27%), while effects for physical QOL were non-significant (SMD 0.11; 95% CI −0.03 to 0.25, p=0.12: I2=13%). In terms of cost-effectiveness, there was no significant benefit afforded by CC based on two trials in the short term (SMD −0.09; 95% CI −0.32 to 0.13, p=0.42: I2=0%). Medium-term results were reported by Bypassing the Blues,40 which did not indicate significantly lower costs with CC (SMD 0.07; 95% CI −0.22 to 0.35, p=0.65).
Ancillary analyses
We performed ancillary analysis with each constituent of the MACE end point encompassing acute coronary syndrome hospitalisations, coronary revascularisation, HF and stroke. There was no significant effect for CC to reduce any of these more specific cardiovascular end points (see eSupplements 6 to 9). Also, since five trials differentiated between MACE and cardiac-cause hospital readmissions, we performed an analysis according to the latter outcome, which occurs more frequently. Analysis of five trials showed no significant reduction in cardiac-cause hospital readmissions (RR=0.89; 95% CI 0.66 to 1.19, p=0.43: I2=35%) (see eSupplement 10).
Sensitivity analyses
For depression change, a sensitivity analysis was performed excluding the trials comprised by patients with diabetes without CHD19 and non-depressed patients with CHD with anxiety.23 The sensitivity analysis revealed a small increase in the effect size (pooled SMD −0.39; 95% CI −0.53 to −0.25, p<0.00001: I2=0%). We also evaluated the trials comprising patients with only CHD (excluding other cardiac disorders) and assessed the depression response. The trials were associated with depression remission (OR=1.94; 95% CI 1.40 to 2.70, p=<0.0001: I2=39%) and depression symptom reduction (pooled SMD −0.43; 95% CI −0.59 to −0.27, p<0.00001: I2=0%).
The timing of depression onset41 and intervention11 after a cardiac hospitalisation has been raised by several scholars as an important methodological consideration. Thus, we stratified studies as providing CC immediately on screening or as an inpatient17 ,36 ,37 versus those which considered depression chronicity with a secondary screener at a later stage and as an outpatient.11 ,34 ,35 It was found that timing of depression intervention was a source of between-group heterogeneity for depression severity in six trials (between groups p=0.04, I2=76.5%) (see eSupplement 11), but not for depression remission (between groups p=0.50, I2=0% (see eSupplement 12).
When analysing the effect of CC in relation to components of depression treatment, as described in our protocol,20 it was found that CC was not associated with a higher prescription rate of antidepressant medication (6 trials, OR=1.38; 95% CI 0.91 to 2.10, p=0.13, I2=62%). There was no increase in the initiation of psychological therapy with CC (6 trials, OR 2.01; 95% CI 0.85 to 4.76, p=0.11, I2=84%) (see eSupplements 13 and 14).
Publication bias and GRADE strength of recommendations
Testing for publication bias was inappropriate as fewer than 10 RCTs were eligible. All of the primary and secondary outcomes were graded as being of moderate strength according to the GRADE26 criteria (see eSupplement 15).
Discussion
This systematic review adds to the extant literature by reporting the efficacy and healthcare costs of CC interventions in comorbid depression and CHD populations. It was found that CC was associated with a significant reduction in MACE in the short term (<6 months) that was not sustained in the longer term. The absence of significant reduction in MACE in the longer term is comparable to other findings with pharmacological or psychological interventions.8 ,42 The results pertaining to the secondary depression end points indicated a small albeit significant reduction in depression symptoms with CC, and depression remission was also more likely in the short term. In addition, CC was associated with a significant reduction in anxiety symptoms and an improvement in mental QOL. The findings did not suggest a significant benefit for physical QOL or healthcare costs. Taken together, the findings generally support previous systematic reviews regarding more specific depression treatments such as antidepressants or psychotherapy in the population with CHD.8 ,42
The significant reduction in MACE in the short term is in contrast to a prior Cochrane review8 and other systematic reviews reporting on medical outcomes.43 ,44 However, the generalisation of our findings is limited as only three trials reported the primary MACE end point in the short term. Thus, it is most likely that there were simply too few MACE reported, resulting in low statistical power. This is further exemplified by comparing the cumulative sample in our analyses to the ENRICHD study9 which randomised 2481 patients with MI to cognitive–behavioural therapy supplemented with SSRIs versus usual care. At the 29-month follow-up in the ENRICHD trial, there was no difference in event free survival from death or recurrent MI (75.8% intervention vs 75.9% usual care).9 The longer term MACE findings of our review align with the general consensus that depression treatment does not lead to a clinically meaningful impact on cardiovascular events in patients with CHD.45–47 With regard to depression remission, short-term results with CC were promising, indicating a higher remission rate with CC. However, only the COPES trial39 reported medium-term follow-up data. With regard to secondary end points of anxiety and mental QOL the results here appear comparable to other systematic reviews on psychological interventions.8
The limitations of the primary studies are that the predominant CC research has been performed in the USA17 ,18 ,22–24 with only one Australian study included here.19 Other CC trials that did not meet our CHD threshold have been performed in the UK28 and the Netherlands.48 Further trials with CHD populations may assist in clarifying the extent to which CC can be readily applied in other healthcare settings outside the USA. As a consequence of low uptake of CC RCTs outside the USA, the total number of RCTs retained for our meta-analysis was low. Moreover, the infrequent reporting of MACE and mortality data in the original studies limited our analyses to three trials. Another limitation was that risk of bias assessment showed that some studies were characterised by methodological limitations, especially a lack of blinding regarding intervention staff and participants (which is not possible in CC interventions when compared to usual care) and blinding of depression assessment (ie, only self-report instruments used).
Diversity in the design of the CC and control group may have also led to heterogeneity between the studies. In favour of a more comprehensive overview of the topic, we included studies with diabetes19 and anxiety.23 As shown in sensitivity analyses, this might have underestimated the effect sizes when compared to cardiac-depression populations only. Indeed, evidence for CC appears to be more firmly established in the population with diabetes,43 highlighting discrepancies between depression intervention efficacy in CHD.7 ,8 Given that CC interventions consist of scheduled follow-up, it cannot be ruled out that depression efficacy was partly attributable to the attention given to participants in the treatment condition. Further RCTs using attention control groups might also explicate whether treatment effects are partly attributable to time spent with patients.
In conclusion, collaborative depression care in the CHD population did not lead to a sustained reduction in MACE. Small reductions in depressive symptoms were evident for CC and intervention participants were more likely to achieve depression remission. Small effect sizes for anxiety symptom reduction and improvement in mental QOL were evident with CC. However, it remains to be shown that collaborative depression care can lead to sustained reductions in cardiovascular events and a moderate depression response in the longer term. Scant RCT data exist outside of the USA and the cost-effectiveness has not been established at this time.
Acknowledgments
The authors thank the collaborative care trial authors for generously providing additional data required in this review: Professor Bea Belnap, Professor Karina Davidson, Professor Jeff Huffman and Professor Bruce Rollman.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Funding This work was supported by the National Health and Medical Research Council of Australia (#1053578) and the article processing charge was funded by the German Research Foundation (DFG) and the Albert Ludwigs University Freiburg in the funding programme Open Access Publishing.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.