Article Text

Abstract
Objectives To identify the use and adverse drug reactions associated with azithromycin in neonates.
Setting Databases MEDLINE (1948–August 2015), EMBASE (1980–August 2015) and Pubmed (August 2015) were searched for studies on azithromycin in neonates.
Participants All studies involving neonates (<28 days old) who have received at least a single dose of azithromycin for which safety was evaluated.
Primary and secondary outcome measures The primary outcome was adverse event (AE) associated with use of azithromycin. Use of azithromycin in neonates was the secondary outcome.
Results A total of 11 articles involving 473 neonates were identified. 371 AEs were reported. Adverse events were mainly respiratory (358/1000 neonate), neurological (273/1000 neonates) and gastrointestinal (196/1000 neonates) in origin. Azithromycin significantly reduced the risk of bronchopulmonary dysplasia (BPD) in extremely premature neonates (RR=0.83, 95% CI 0.71 to 0.98, p=0.02). There was no significant difference in the incidence of elevated liver enzymes between the azithromycin and placebo group (p=0.76). There were four cases of infantile hypertrophic pyloric stenosis (IHPS).
Conclusions Azithromycin significantly reduces the risk of BPD in preterm neonates. The relationship between azithromycin and IHPS requires further investigation.
- CLINICAL PHARMACOLOGY
- NEONATOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review assessed the quality of all the randomised controlled trials (RCTs).
RCTs, cohort studies and case reports were reviewed.
Only a few studies of azithromycin in neonates have been published.
Introduction
Azithromycin is a macrolide derivative of erythromycin. It is one of the most commonly prescribed antibiotics in children, with a prescription rate of between 4% and 14%.1–3 Since its approval in the USA and Europe,4 ,5 it has been used extensively for the treatment of several paediatric infectious diseases.6 Prescription rate for respiratory tract infection in children is increasing.3
Owing to lack of efficacy and safety studies, oral and intravenous formulations are not recommended for children less than 6 months7 and 16 years,8 respectively. The safety of azithromycin eye drops in children aged under 1 year is also unknown.9 ,10 Gastrointestinal disorders such as diarrhoea, vomiting and abdominal pain are the most commonly reported side effects in paediatrics.11 Increased risk of arrhythmia and cardiovascular-related death in adults has been reported.12 ,13
The potential of azithromycin as a chemoprophylactic agent for bronchopulmonary dysplasia (BPD) in neonates is still under exploration. ureaplasma infection, which has been shown to be susceptible to the drug,14 ,15 is associated with BPD.16 ,17 Despite limited efficacy and safety data, the US Centre for Disease Control (CDC) considers azithromycin as the first choice treatment and chemoprophylaxis of choice for pertussis in neonates. Treatment is recommended for 5–7 days.18
There is currently insufficient information on azithromycin treatment in neonates; therefore, this systematic review aims to evaluate all published data and reports on the safety and use of the drug in this age group.
Methods
This review was carried out as per PRISMA guidelines. The systematic review protocol was not published.
Search strategy
The databases MEDLINE (1948–August 2015), EMBASE (1980–August 2015) and Pubmed (up to August 2015) were searched. Search words: ‘preterm or neonat* or neonate* or newborn* or infan*’ in title and abstract were combined with ‘azithromycin’ in title and abstract for all databases. Manual search of bibliography was also undertaken.
Eligibility criteria
Any published literature with documented involvement of neonates (birth to 28 days) administered azithromycin via any route of administration for any disease condition was included. There was no restriction on the type of study included, publication date and language of publication or inclusion of abstracts. Any article with involvement of the specified age group taking at least a single dose of azithromycin was assessed. Only articles with information on the safety of azithromycin were included, such as any mention of an adverse drug reaction, drug toxicity, drug, side effects or adverse event.
Data quality assessment
The randomised controlled trials (RCTs) were assessed using Cochrane collaboration's tool for assessing risk of bias,19 by two independent reviewers (figure 1). Studies with low risk of bias in at least four of the six parameters were included in the meta-analysis.

Summary of risk of bias.
Data collection and statistical analysis
A single reviewer undertook eligibility assessment. Each title and available abstract was screened for appropriateness and relevant articles obtained. Articles were examined independently by a second reviewer to confirm they met inclusion criteria. Hand searching of references of articles was performed. Data were extracted from relevant articles on methodology, characteristics of trial participants (including condition and gestational age), number of neonates receiving azithromycin, number of participants in study, route of administration, dose, duration of azithromycin treatment, comparator drugs and adverse events.
Meta-analysis was carried out in Revman V.5.3. Relative risks and 95% CIs were estimated for each RCT. Overall relative risks were calculated from the RCTs. Begg and Mazumdar's rank correlation tests were used to assess publication bias. No significant publication bias was found. Between-studies heterogeneity was assessed using a χ2 test where a p value less than 0.05 indicated significant heterogeneity. Fixed effect models were used to produce summary relative risks and 95% CIs where heterogeneity did not exist. If statistical heterogeneity did exist then random effects models were applied.
Results
A total of 11 articles involving 473 neonates were identified (figure 2). The majority of the studies (4 studies) were RCTs. There were three pharmacokinetic studies and three cohort studies (table 1). One case report was identified. The RCTs involved 211 neonates who received azithromycin and 198 controls. The cohort studies and PK studies involved 218 and 43 neonates, respectively. Three hundred and seventy-one AEs were reported. Adverse events were mainly respiratory (358/1000 neonate), neurological (273/1000 neonates) and gastrointestinal (196/1000 neonates) in origin. Vomiting (44/1000 neonates), diarrhoea (15/1000 neonates), abdominal tenderness (22/1000 neonates) and feeding intolerance (37/1000 neonates), were the most frequently reported gastrointestinal symptoms. The majority of the respiratory and neurological AEs were usually associated with prematurity (table 2).
Summary of all studies involving term and preterm neonates
Classification and risk of adverse events from RCTs and observational studies (n=324)

Flow chart of included articles.
Evidence from RCTs
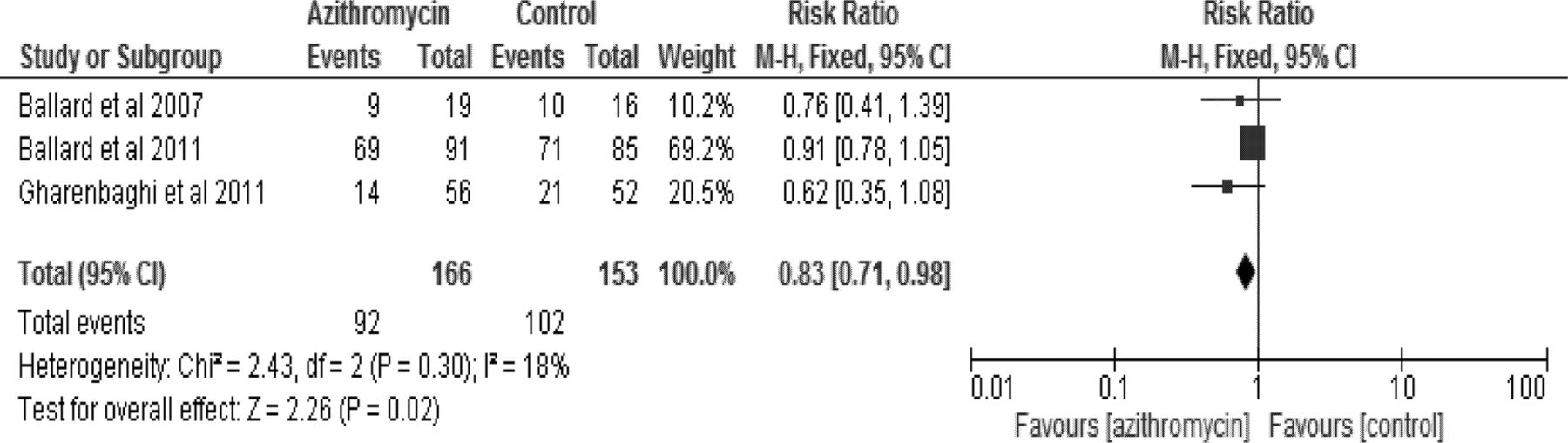
Two of the four RCTs were placebo controlled. Intravenous azithromycin, 10 mg/kg/day, was administered for 1 week followed by a 5-week course of 5 mg/kg/day as prophylaxis for BPD in both studies.20 ,21 A third study administered 5 mg/kg/day for 1 week after an initial 1 week course of oral 10 mg/kg/day.22 The patients in the comparator arm of this study were not given any treatment. Meta-analysis of the incidence of BPD between neonates administered azithromycin and the control group in the three studies showed that azithromycin significantly reduced the risk of BPD in extremely premature neonates (RR=0.83, 95% CI 0.71 to 0.98, p=0.02) (figure 3): 55% of preterm neonates given azithromycin developed BPD compared to 67% of those without treatment or those given placebo. Funnel plots of these RCTs show no publication bias (figure 4). The fourth study compared the efficacy of azithromycin with erythromycin for the treatment of chlamydia conjunctivitis.23 Ninety-six per cent of children treated with 3 days intravenous 10 mg/kg and subsequent 4 days oral dose azithromycin recovered compared with 76% of those given twice daily 10 mg/kg erythromycin for 3 days followed by 11 days of thrice daily oral erythromycin. A significantly higher cure rate (p=0.03) was achieved with azithromycin than with erythromycin.

Relative risks of BPD in azithromycin and untreated/placebo treated preterm neonates. BPD, bronchopulmonary dysplasia.

Funnel plot to determine publication bias.
There was no significant difference in the incidence of elevated liver enzymes between the azithromycin and placebo group (p=0.76) (figure 5). All cases of elevated transaminases (16 cases) were reported in a single RCT.20 There were 13 cases of elevated transaminases in the control group of this study. Only one placebo/no treatment controlled trial reported vomiting as an adverse event, with no significant difference between the azithromycin group and the neonates without treatment (p=0.79). The other AEs reported in the placebo/no treatment controlled RCTs were usually associated with prematurity (intraventricular haemorrhage, periventricular leucomalacia, necrotising enterocolitis, patent ductus arteriosus and hearing abnormalities) and there were no significant differences between azithromycin and the comparator arms.20–22 A Chinese study reported more cases of diarrhoea, abdominal pain and reduced appetite in the children treated with oral erythromycin (after 3 days of intravenous treatment), compared with those administered azithromycin.23

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relative risk of elevated transaminase in azithromycin and placebo treated neonates.
Evidence from observational studies
Two cohort studies were identified. One of these studies involved a cohort of neonates given either azithromycin or erythromycin following exposure to a patient with pertussis.24 Fifty-eight neonates received azithromycin while 18 were given erythromycin. None of the neonates developed infantile hypertrophic pyloric stenosis (IHPS). Fourteen (24%) of those given azithromycin experienced AEs. These included three cases each of irritability, candidiasis and vomiting; two cases of rash and one case each of diarrhoea, abdominal pain and blood in the stool. Ten (56%) of the neonates given erythromycin experienced AEs. There was a significantly lower incidence of diarrhoea (p=0.01) in the azithromycin-treated compared with erythromycin-treated neonates. The incidences of other AEs were not significantly different.
The second observational study involved 12 neonates who received varying doses of azithromycin suspension for the treatment of chlamydia conjunctivitis.25 Three of the 5 neonates (60%) administered a single dose of 20 mg/kg became culture negative; while 6 of the 7 (86%) given 20 mg/kg/day for 3 days became culture negative. No AEs were reported in this study.
Retrospective study
A single retrospective cohort study was identified. This study explored the risk of IHPS in neonates exposed to azithromycin and erythromycin, using the US military health system (MHS) database. Of the one hundred and forty-eight neonates (0–14 days old) treated with azithromycin, 3 (2%) developed IHPS. Nine (3%) of the 291 neonates (0–14 days) given erythromycin had IHPS.26
Pharmacokinetic studies
A single dose of 20 mg/kg was administered in a pharmacokinetic study27 and a 10 mg/kg single dose was administered in two other pharmacokinetic studies.28 ,29 All the AEs reported in two of these studies were usually associated with prematurity and none was attributed to azithromycin.27 ,28 There were four cases of intraventricular haemorrhage, three of hearing loss, two of necrotising enterocolitis, one each of periventricular leucomalacia, respiratory distress syndrome, pneumomediastinum and hyperbilirubinaemia. No AEs were observed in the third study.29
Case report
There was one case report of pyloric stenosis in a 5-week old infant who had received 5 days of oral azithromycin at 3 weeks of life as treatment for chlamydia conjunctivitis.30
Discussion
Only a small population of neonates have been treated with azithromycin and no major AE has been documented. This systematic review shows that azithromycin significantly reduces the risk of BPD in neonates and is also effective in the treatment of chlamydia conjunctivitis. A previous systematic review has also demonstrated the efficacy of azithromycin in the prevention of BPD.31 Macrolide antibiotics are inhibitors of ureaplasma. The relationship between ureaplasma infection and BPD has been explored with varying outcomes reported from different studies.15 ,17 ,32 We have also identified two off-label studies demonstrating the efficacy of azithromycin against chlamydia trachomatis in neonates. Previous studies have reported the susceptibility of chlamydia to azithromycin.33 Azithromycin was administered once daily in all studies because of its long half-life, which is estimated to be between 26 and 83 h in neonates.25 The dose and duration of treatment with azithromycin varied across the studies. This may be due to its off-label use and the absence of a standardised dosing regimen for the drug in this age group. Very few studies have been conducted in neonates; hence the safety and efficacy of different dosing regimens for different indications have not been established.
The majority of the AEs reported in preterm neonates were related to prematurity and were unlikely to be caused by azithromycin. Results from one of the studies, however, showed that azithromycin had a better safety profile than erythromycin in neonates. Diarrhoea, abdominal discomfort and reduced appetite were less frequent in azithromycin treated neonates. In another study, 2% and 3%, respectively, of neonates exposed to azithromycin and erythromycin within 14 days of life developed IHPS.26 Both erythromycin and azithromycin are gastric motilin receptor agonists.34 Activation of these receptors by erythromycin with consequent increased pyloric contractions has been hypothesised as a possible cause of pyloric hypertrophy in neonates.35 The association between erythromycin and pyloric stenosis has been demonstrated in previous studies. High dose and early neonatal exposure to the drug within the first 14 days of life are known risk factors.36 Azithromycin, similarly to erythromycin, binds to and activates the motilin receptors.37 Erythromycin is, however, believed to have a stronger gastrointestinal prokinetic effect than azithromycin.38 These drugs are slightly structurally different, with erythromycin having a 14-C member heterocyclic ring and azithromycin a 15 member ring.39 The effect of the structural differences on motilin receptor binding and IHPS requires further exploration. Postnatal exposure to macrolides from breast milk has also been associated with IHPS.40 Further studies are required to determine the relationship between neonatal azithromycin use and IHPS.
Although prolonged QTc interval and torsades de pointes had been reported in azithromycin-treated adults,41 none of the reviewed studies evaluated neonates for arrhythmia. There is a documented case of arrhythmia in an infant following azithromycin overdose,42 and spiramycin, which is a structurally similar macrolide, has been associated with neonatal arrhythmia.43 Prolonged QTc interval can be normal in the first few days of life in premature neonates, hence it is difficult to identify drug-induced aetiology during this period.44
In conclusion, azithromycin significantly reduces the risk of BPD in preterm neonates and it is effective for the treatment of chlamydia conjunctivitis. It has a better safety profile than erythromycin in the limited number of treated neonates. The relationship between azithromycin and IHPS requires further investigation. More studies are required to determine a safe and effective dose for azithromycin in neonates.
Acknowledgments
This work is part of the TINN2 network (Collaborative Project) supported by the European Commission under the Health Cooperation Work Programme of the 7th Framework Programme (grant agreement number 260908). The authors wish to thank Sally Hinchcliffe, Medical Statistician at the Royal Derby Hospital, for her statistical advice on this paper.
References
Footnotes
Contributors IC, SK, EJ-A and HS conceived the idea; CS performed the literature search and extracted the data. OE updated the search and verified the extracted data. OE produced the first draft of the manuscript. All the authors contributed to the subsequent and final drafts of the manuscript.
Funding Supported by the European Commission under the Health Cooperation Work Programme of the 7th Framework Programme (grant agreement number 260908).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.