Article Text

Abstract
Objectives Left heart disease (LHD) is the main cause of pulmonary hypertension (PH), but little is known regarding the predictors of adverse outcome of PH associated with LHD (PH-LHD). We conducted a systematic review to investigate the predictors of hospitalisations for heart failure and mortality in patients with PH-LHD.
Design Systematic review.
Data sources PubMed MEDLINE and SCOPUS from inception to August 2013 were searched, and citations identified via the ISI Web of Science.
Study selection Studies that reported on hospitalisation and/or mortality in patients with PH-LHD were included if the age of participants was greater than 18 years and PH was diagnosed using Doppler echocardiography and/or right heart catheterisation. Two reviewers independently selected studies, assessed their quality and extracted relevant data.
Results In all, 45 studies (38 from Europe and USA) were included among which 71.1% were of high quality. 39 studies were published between 2003 and 2013. The number of participants across studies ranged from 46 to 2385; the proportion of men from 21% to 91%; mean/median age from 63 to 82 years; and prevalence of PH from 7% to 83.3%. PH was consistently associated with increased mortality risk in all forms of LHD, except for aortic valve disease where findings were inconsistent. Six of the nine studies with data available on hospitalisations reported a significant adverse effect of PH on hospitalisation risk. Other predictors of adverse outcome were very broad and heterogeneous including right ventricular dysfunction, functional class, left ventricular function and presence of kidney disease.
Conclusions PH is almost invariably associated with increased mortality risk in patients with LHD. However, effects on hospitalisation risk are yet to be fully characterised; while available evidence on the adverse effects of PH have been derived essentially from Caucasians.
- Pulmonary hypertension
- left heart disease
- outcome
- mortality
- predictors
- hospitalization
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Our search strategy was likely limited by its focus on a full-report article published in English and French, and traceable via PubMed MEDLINE and/or SCOPUS.
-
Important heterogeneity in the included studies precluded the pooling of data to perform a meta-analysis.
-
This is the first systematic review on determinants of hospitalisations and mortality in patients with pulmonary hypertension associated with left heart disease, which presents the available up-to-date and high-quality evidence on the subject matter.
Introduction
Pulmonary hypertension (PH) describes a group of disorders resulting from an increase in pulmonary vascular resistance, pulmonary blood flow, pulmonary venous pressure or a combination of these features.1 Based on shared pathological and haemodynamic characteristics, and therapeutic approaches, five clinical groups of PH have been distinguished2 with PH associated with left heart disease (PH-LHD) or PH group 2 credited to be the most frequent form of PH in contemporary clinical settings.3 Indeed, PH is common in patients with LHD, where it often reflects the background LHD, but has also been reported to be a maker of disease severity and unfavourable prognosis. Patients with PH-LHD have more severe symptoms, worse tolerance to effort, experience higher hospitalisation rates and are more likely to receive an indication of the need for cardiac transplant3 with major implications for the quality of life of patients and healthcare costs. Several studies have reported PH-LHD to be associated with increased mortality, both in patients with systolic dysfunction and those with preserved left ventricular ejection fraction (LVEF).3–6 Furthermore, the presence of preoperative PH has been associated with poor outcomes in patients with valve disease undergoing valve replacement.7 However, there are still several gaps in the existing evidence, including the prevalence of PH-LHD and measurement of the true impact of PH on symptoms and outcome of various LHDs. Equally, little is known regarding the effect of the severity of PH on hospitalisations, rehospitalisations and death, and their co-factors in patients with LHD. Considering the number of recent advances in the management of PH, it is likely that a better understanding of the impact of PH-LHD on major outcomes might assist the clinical management of patients with PH.
We performed a systematic review of the existing literature to determine the predictors of hospitalisation and mortality in patients with PH secondary to LHDs including systolic dysfunction, diastolic dysfunction and/or valve disease. Additionally, we aimed to assess whether the severity of PH affects the risk of the two outcomes.
Methods
We searched MEDLINE via PubMed and SCOPUS from inception to August 2013 for all published studies on PH-LHD, using a combination of key words described in the online supplementary box 1. All searches were restricted to studies in humans published in ‘English’ or ‘French’ languages. In addition, we manually searched the reference lists of eligible studies and relevant reviews, and traced studies that had cited them through the ISI Web of Science for any relevant published and unpublished data. Two independent reviewers (AD and APK) performed the study selection, data extraction and quality assessment; and disagreements were resolved by consensus or consulting a third reviewer (KS).
Studies that reported on hospitalisation and/or mortality in patients with PH-LHD were included if the following criteria were met: (1) age of participants greater than 18 years; (2) Right ventricular systolic pressure (RVSP) measured by transthoracic Doppler echocardiography (DE) and calculated from the maximum tricuspid regurgitation jet velocity using the modified Bernoulli equation (4v2) and adding right atrial pressure (RAP). RAP could be a fixed value from 5 to 10 mm Hg, could have been estimated clinically using the jugular venous pressure (JVP), or estimated by measuring the inferior vena cava size and change with spontaneous respiration using echocardiography; and/or (3) mean pulmonary artery pressure (mPAP) measured by right heart catheterisation (RHC) or by DE. We excluded narrative reviews and case series. Studies on persistent PH following heart transplantation were not included because of the complexity of the classification of PH in this population.
The following variables were extracted from each study: publication year, country of origin of the study, study design, study population's demographics, the mean/median follow-up duration, the outcome predicted, the proportion of measurable RVSP, the mean/median baseline RVSP or mPAP, the prevalence of PH, the readmission rate, the mortality rate with odds ratio (OR) or hazard ratio (HR) for PH where reported and the predictors of outcome including the tricuspid annular plan systolic excursion (TAPSE). One study8 reported the effect of PH in relation with survival. Effects on mortality were obtained by taking the inverse of the HR for survival.
Quality assessment
The methodological quality of the selected studies was assessed using the Quality In Prognosis Studies (QUIPS) tool, designed for systematic reviews of prognostic studies through an international expert consensus (table 1).52 The QUIPS contains six domains assessing the following: (1) bias due to patient selection; (2) attrition; (3) measurement of prognostic factors; (4) outcome measurement; (5) confounding on statistical analysis and reporting results; and (6) confounding on presentation. In prognosis studies designed to predict a specific outcome based on a combination of several possible prognostic factors, confounding is not an issue. Therefore, the items on confounding were considered irrelevant for our quality assessment. The remaining 17 items of the five categories each were scored to assess the quality of the included studies. For each study, the five domains were scored separately as high (+), moderate (±) or low (−) quality (ie, presenting a low, moderate or high risk of bias, respectively). To strengthen the discriminative capacity of the QUIPS, we used the scoring algorithm developed by de Jonge et al,53 as explained, described in detail in the online supplementary table.
Results of quality assessment of studies on mortality and readmissions for heart failure in patients with pulmonary hypertension associated with left heart disease
Data synthesis
Hospitalisations or rehospitalisations for heart failure and mortality identified by multivariable analysis in individual studies are presented (table 2), including their estimated effect size (eg, OR or HR) and 95% CI. Quantitative analysis of results was not done due to important heterogeneity in study design, study population, PH definition and measurement, outcome definitions in the studies and confounding or other types of prognostic factors. We have therefore presented a narrative summary of the available evidence (table 2).
Study characteristics of studies on mortality and readmissions for heart failure in patients with pulmonary hypertension associated with left heart disease
Results
Studies selection
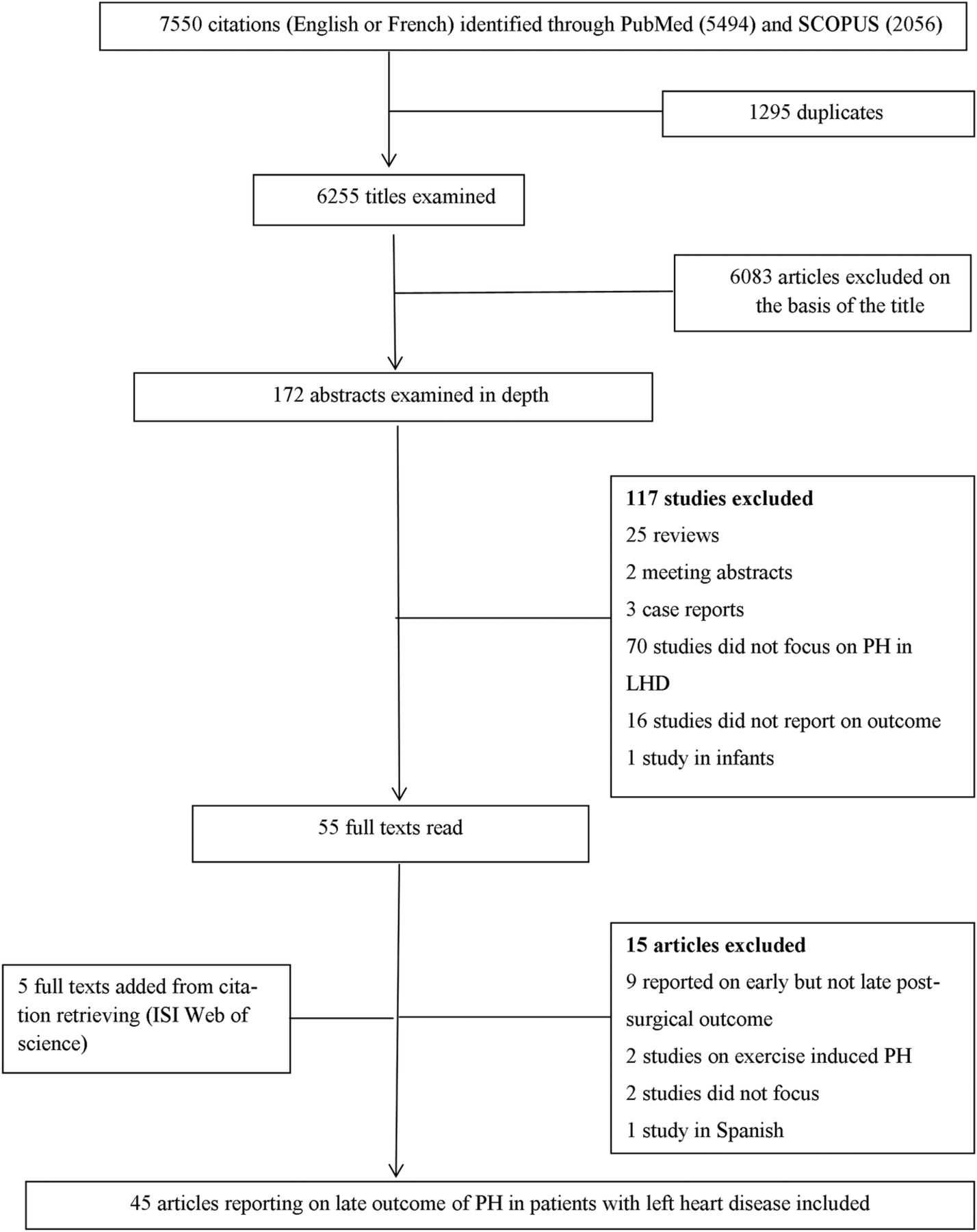
Figure 1 presents a flow diagram for the study selection process. Of the 7550 citations identified through searches, 6255 titles were examined and 6083 were excluded on the basis of the title scanning. The remaining 172 abstracts were examined and 55 articles were screened by full text of which 15 were excluded for various reasons (figure 1). Five studies were identified via citation search. Therefore, 45 articles were included in the final review among which 86.7% were published between 2003 and 2013 (see online supplementary figure S1).

{kind=link}
Flow diagram of literature search process. LHD, left heart disease; PH, pulmonary hypertension.
Study characteristics and methodological quality
The characteristics and methodological quality of the 45 included studies are described in table 1. The overall quality score ranged from 29.5 to 72.5 points with a median of 63.5. Based on the cut-offs of ≥60 and ≥45 points, respectively, we classified 34 articles as being of high quality, 7 as moderate-to-high quality and four as low-quality studies (table 1). Studies of high quality were recent and scored well on patient selection, outcome measurement, statistical analysis and presentation. Studies classified as moderate/low quality scored relatively well on patient selection, but poorly on study attrition, statistical analysis and presentation. Twenty-four (53.3%) studies were from the USA, 12 (26.6%) from Europe (four from UK, three from Italy and one each from Spain, Germany, Denmark, France and Sweden), 6 (13.3%) from Asia (two from Japan, one each from India, China, Korea and Australia) and 1 from South Africa. One study was multicentric across Europe and the USA40 and another one was multicentric across the USA and Canada.30 Only three population-based cohorts were reported including two prospective13 ,29 and one retrospective study.14 For the remaining 42 hospital-based cohort studies, 20 had a retrospective design. The number of participants ranged from 46 to 2385 in hospital-based and from 244 to 1049 in population-based studies. The proportion of men ranged from 21% to 91%, and mean/median age from 63 to 82 years. Twenty-six studies were in patients with heart failure (HF) and cardiomyopathies (two in heart failure with preserved ejection fraction (HFpEF)) and 19 in patients with valve disease.
Twelve studies defined PH using RHC and 32 studies using DE. One study defined PH using both RHC and DE. Studies applied variable definitions of PH using both RHC (based on mPAP >25 or 30 mm Hg, or on systolic pulmonary artery pressure (sPAP) >50 mm Hg, or sPAP >40 mm Hg, or on pulmonary vascular resistance (PVR) >2.5 wood units (WU)) and DE (based on RVSP with cut-offs varying from 35 to 50 mm Hg, or based on a mPAP >25 mm Hg8 or on a right ventricular tricuspid gradient (RVTG) >25 mm Hg).25 Prevalence of PH in HF ranged from 22% to 83.3% overall, 22–83.3% in studies of PH based on DE and 23–76% in studies of PH based on RHC (see online supplementary figure S2).
Outcome of PH
Admissions for heart failure
The duration of follow-up ranged from 6 to 87.6 months overall, 6–69.6 months in studies of PH based on RHC definition and 6–87.6 months in studies of PH based on DE definition. Readmission rates, when reported, ranged from 9.2% to 75% overall and 9.2–75% in studies of PH based on DE definition. Only one study with PH definition based on RHC reported a readmission rate of 27% (table 2). Admissions or readmissions for HF were reported in nine studies all based on DE definition among which seven reported HRs or ORs for admission/readmission in relation with PH. Effect estimates for six of the seven studies were statistically significant.
Mortality
Mortality was reported in all studies (table 2); however, not all studies provided multivariable-adjusted effect estimates of mortality risk associated with PH. PH was associated with increased all-cause mortality in 24 of 26 studies of HF, among which 6 studies were of PH based on RHC definition, while two studies failed to report an association between PH and all-cause mortality at 6 months. Of these two studies, one used PH definition based on RHC and was a multicentric trial of HF that reported effect estimates for mortality risk from PH (HR=0.89 (95% CI 0.66 to 1.20));30 while the other one32 did not. When reported, mortality rates at 12 months ranged from 0% to 32% overall, 0% to 32% in studies of PH based on DE and 2.9% to 18% in studies of PH based on RHC (see online supplementary figure S3). As summarised in table 3, over 35 potential predictors of mortality were tested across studies with variable and often inconsistent effects on the outcome of interest. Age was associated with mortality in 14 studies (among which 11 studies of PH were based on DE), male gender in 3/11 studies (all based on DE), LVEF in 6/10 studies, right ventricular (RV) function in 3/3 studies and renal disease (rising creatinine, decreasing glomerular filtration rate (GFR) or dialysis) in 6/17 studies (all based on DE), functional class (New York Heart Association (NYHA) or WHO) in 7/12 studies (five based on DE) while the 6 min walking distance was tested in only one study but was not integrated in the multivariable analysis for outcome risk.32
Other prognostic factors associated with mortality in patients with pulmonary hypertension associated with left heart disease
Discussion
An increasing number of studies have assessed the risk of readmission and mortality in patients with LHD-related PH over the last decade, and mostly in North America and Europe. Available studies are mostly consistent on the adverse effect of PH (whether assessed using DE or RHC) on mortality risk in patients with heart failure as well as those with mitral valve disease, but less unanimous in those with aortic valve disease. The consistent adverse effect of PH in this population highlights the importance of early diagnosis of PH to reduce mortality. While available studies have been overall of acceptable quality, substantial heterogeneity in the study population, PH definition and measurement, outcome definitions as well as other prognostic factors limit direct comparisons across studies. Information on readmission for heart failure was limited and the assessment of other prognostic factors in an integrated multivariable model was very heterogeneous.
Mortality in patients with PH and heart failure with reduced ejection fraction
While PH was an independent prognostic factor for mortality in fatal-outcome studies, the prevalence of PH and effects on mortality varied according to LVEF. Differences in the prevalence of PH could be explained at least in part by population heterogeneity (age, level of HF, HF centres or community study) and differences in the criteria used to define PH across studies with a variety of cut-off values. Regardless of the prevalence of PH in HFrEF, there seems to be no uniformity in the association between the magnitude of reduction in LVEF, and the presence or absence of PH and the effects of PH on mortality risk. It is possible that the small size of studies and the short duration of follow-up precluded the accumulation of a substantial number of events to allow the detection of a relationship, if any. Furthermore, although the precise haemodynamic threshold beyond which RVSP is invariably associated with mortality is subject to debate; the risk of death associated with PH seems to increase with higher RVSP.6 ,12 ,13 ,16 A possible pathophysiological explanation is that early and higher vascular remodelling occurs in patients with HF and severe PH, causing a reactive or ‘postcapillary PH with a precapillary component’, which in turn has a greater impact on the RV function. Equally, RV systolic function has been shown to be highly influenced by pressure overload and by vascular resistance in the pulmonary region50; and RV function assessed using RHC or echocardiography has been shown to be associated with mortality.30 ,31 ,33 It is, however, remarkable that one study30 reported no interaction between PH and RV function, with both variables being independently associated with mortality. This highlights the fact that RV function in HF does not only depend on pulmonary pressure but may also reflect intrinsic myocardial disease. As suggested by Vachiery et al6 there might be a spectrum of clinical phenotypes of RV failing in PH-LHD that might evolve from one to the other, from isolated postcapillary PH with little effect on the RV to more advanced disease where the failing RV is the key determinant of outcome.
Mortality in patients with PH and heart failure with preserved ejection fraction
Over the past decades, the increasing prevalence of HFpEF51 has been paralleled by an increasing presence of PH in patients with HFpEF.5 ,6 When compared to heart failure with reduced ejection fraction (HFrEF), patients with HFpEF have their subset of risk factors; but finally, PH conveys similar morbidity and mortality risk in the two subgroups of patients.13 ,17 The current incomplete understanding of HFpEF limits our ability to explain why these patients develop PH. However, it is estimated that over time left atrium and ventricular filling pressure from compromised left ventricle and, in some, left atrium relaxation and distensibility can lead to elevated pulmonary venous pressure, triggering vasoconstriction and arterial remodelling.4 ,5 In total, the finding of PH as an independent prognostic factor for mortality in patients with HF tends to support the suggestion that PH should be considered as a potential therapeutic target at least in the group of patients with HF who exhibit persisting PH after optimisation of HF therapy. In this line, targeting both pulmonary vasculature and the heart would probably be more beneficial.
Mortality in patients with PH related to valvular heart disease
PH due to valvular heart disease (VHD) was not always related to mortality risk,38 ,39 ,45 which is in contrast with PH in patients with heart failure. A simple explanation of this difference could be that the prevalence and severity of PH correlates with the severity and type of VHD. Although mitral stenosis (MS) has been the classical disease associated with PH-LHD and reactive PH was initially described in these patients4; it is, however, noticeable that PH due to MS has received little attention over the last decade, probably because of the progressive decline in RHD in Western countries. Interestingly, the two studies included showed that surgery was safe and improved survival in patients with PH due to MS35 ,48 with PH regressing to normal levels over 6–12 months after successful Mitral Balloon Valvotomy (MBV).35 In mitral regurgitation (MR), nearly all cohort studies on outcomes of severe PH reported increased mortality.38 ,39 ,40 ,46 ,49 The relevance of this finding is that PH can serve both as an indication for proceeding to surgical or catheter-based interventions, and also as an operative risk factor for mitral valve interventions.54 By contrast, PH is not as common in the aortic valve surgical cohort. Mortality rates in different studies of patients with VHD depends on comorbidities, exclusion criteria and definition for PH. Studies that also evaluated changes in PH following valve surgery showed a decline in pulmonary pressures following surgery.35 ,45 ,50 ,55 It is worth noting that the pathophysiology of the pulmonary vasculature in PH due to VHD is similar to that in patients with HF.1
Hospitalisations and other prognostic factors
The paucity of information on the effect of PH-LHD on hospitalisations or rehospitalisations as has been shown in this study highlights the need for more evidence on this outcome. Such information is important to fully characterise and quantify the contribution of PH-LHD to the global burden of disease, and assess future improvement from treating the underlying LHD and/or controlling PH in patients with LHD.
Of the 35 other potential prognostic factors of mortality in patients with PH that were tested in multivariable models across studies, investigations on echocardiographic parameters suggested that PH >60 mm Hg was associated with worse mortality in seven of the nine studies. Similarly, a greater degree of MR, deceleration time when reported26 and RV function were almost constantly associated with adverse outcome while LVEF was associated with adverse outcome in 6 of the 10 studies. In the evolution of LHD, RV dysfunction usually occurs as a turning point. It shall be noted that PH incorporates information on diastolic function, MR and pulmonary vascular disease, and this might explain the pivotal role of PH in gauging the prognosis of patients with HF.
Strengths and limitations of the studies included in the review
The first limitation of the studies included in our review is the possibility of study population bias. The majority of studies originated from Western countries and included predominantly Caucasians and reported mostly on PH-LHD in a population with high prevalence of ischaemic heart disease. This precludes the generalisability of our findings to developing countries where aetiologies of LHDs are less of ischaemic origin and are more dominated by systemic hypertension, dilated cardiomyopathies and RHD in a younger population.56 Therefore, PH-LHD may have a different prognosis in developing countries. Second, studies included in this review were defined PH based either on DE or RHC. RHC remains the gold standard to diagnose and confirm PH, but performing RHC on all patients with dyspnoea would bear excessive risks and be impractical in resource-limited settings. DE on the other hand is widely available, safe and relatively cheap for diagnosing PH, although the reproducibility of the approach in some circumstances has been questioned. However, a systematic review on the diagnostic accuracy of DE in PH by Janda et al57 has shown that the correlation of pulmonary artery systolic pressure by DE compared to RHC was good with a pooled correlation coefficient of 0.70 (95% CI 0.67 to 0.73). However, studies to date examining the prognostic impact of PH in LHD have been performed in heterogeneous populations, using variable definitions of PH based both on RHC and echocardiography parameters, thus limiting any possibility of pooling. Finally, readmissions were not frequently reported and multivariable analysis when performed was characterised by a great heterogeneity in the number and range of candidate predictors included in the models, thus limiting interpretation and generalisability. Therefore, findings on these other prognostic factors must be interpreted with caution. For studies that performed only univariate analysis, we cannot rule out the possibility that the reported factors may not preserve a significant association with the outcome once adjusted for the effect of other extraneous factors. In spite of these limitations, the majority of studies included were recent and all reported on the relation of PH-LHD with all-cause mortality, making the conclusions on this relation appropriate for contemporary Western populations.
Strengths and limitations of the review
First, by restricting our search strategy to full-report articles published in English and French, and in journals available in the used electronic databases, we cannot rule out the possibility of language or publication bias. Second, we used the QUIPS instrument, designed for prognosis studies, to address common sources of bias. The QUIPS, however, lacks discriminative power; we addressed this by using the scoring algorithm suggested by de Jonge et al.6 This scoring algorithm can still be subject to criticisms, especially because the cut-off points used to determine the quality of the studies are quite arbitrary. Third, because of important heterogeneity in the included studies, we were not able to pool data to perform a meta-analysis or to stratify data by clinically important subgroups (such as mild, moderate or severe PH). However, to the best of our knowledge, this is the first systematic review on determinants of hospitalisations and mortality in patients with PH-LHD, and the search strategy used allowed us to present the results of several recent and high-quality publications on the topic.
Conclusion
The majority of studies included in this review showed that PH is an independent predictor of mortality in patients with LHD, with the more consistent evidence being in those with HF and MR. Information on readmission for heart failure was somehow very limited. The majority of this information derives from studies in Western and developed countries, and may not apply to populations in other settings. All together, these findings suggest that the hypothesis of targeting PH to improve the outcomes of patients with LHD s should be actively investigated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
Footnotes
-
Contributors AD and APK conceived and designed the protocol. AD, APK and KS performed the literature search, selection and quality assessment of the articles and extraction of the data. AD, APK, FT and KS interpreted the data. AQ wrote the first draft of the manuscript. AD, APK, KS and FT contributed to the writing of the manuscript and agreed with manuscript results and conclusions. All authors read and approved the final manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.