Article Text

Abstract
Objective To investigate the effect of intensified lifestyle counselling targeting infants' mothers on offspring weight development during the first 4 years of life.
Design and setting Follow-up of a cluster-randomised controlled trial in primary care child health clinics during 2004–2006 in Finland. Participants received a follow-up survey during 2010 concerning weight and height measurements of their offspring. Number of clusters was six and the response rate to the follow-up 71.9% (N=64/89).
Participants The participants (N=89) were mothers of infants aged 2–10 months.
Intervention The intervention included individual counselling on diet and physical activity when the infant was 2–10 months of age and an option to attend supervised group exercise sessions.
Primary and secondary outcome measures The authors analysed the secondary outcome of the intervention study: the weight development of the offspring. The primary outcome was the proportion of women returning to their prepregnancy weight by 10 months post partum, reported earlier.
Results Multilevel mixed effect non-linear regression models included group, age of the child and interaction between group and age of the child. The increase of BMI z-score between 24 and 48 months was slower among the intervention group offspring (−0.034 to −0.002, p=0.028) as compared with control group. Z-scores for weight-for-length/height did not differ between groups when the period 0–48 months was analysed (p=0.23) but for the period of 24–48 months, between-group differences were significant (p=0.012).
Conclusions Lifestyle counselling targeting mothers during the child's first year may be effective in slowing offspring weight gain until 4 years of age. However, larger studies are needed to confirm the findings which may have the potential in combatting the obesity epidemic.
Trial registration number Current Controlled Trials ISRCTN21512277.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
Rapid preschool weight gain is known to increase risk for later obesity.
There is lack of intervention studies targeting child's first year with follow-up of their weight gain.
Key message
Results suggested that intensive lifestyle counselling targeting mother during child's first year may slower child's weight gain until 48 months of age.
Strengths and limitations of this study
A feasible counselling method was used as well as a controlled trial setting and reliable growth data based on repeated measurements by nurses in primary child healthcare. We also utilised the recently updated growth data on Finnish children by using z-scores of weight-for-length/height and BMI-for-age described in that growth data.
Since the study was a pilot study, number of participants and clusters was low. Also a longer follow-up period could reveal more clear influence of intervention on offspring weight development.
Introduction
The prevalence of childhood overweight and obesity has increased during the past three decades in the developed world and also in the developing world.1–3 However, recent evidence suggests that the increase in childhood obesity prevalence may be abating.4 Obesity has detrimental short- and long-term consequences to health, and successful treatment of obesity is difficult even in childhood. Effective preventive means are therefore needed.4–6 Because overweight tends to begin during preschool years, early primary preventive interventions are thought to be the most effective means to combat the obesity epidemic. However, only few randomised, controlled primary prevention lifestyle counselling trials have been reported targeting families during offspring's first year of life, to our knowledge none targeting only mothers and including both diet and physical activity counselling. Some of them have shown slightly positive effects on child's weight development, but evidence of effective preventive means to reduce childhood obesity is still insufficient.7–9
Obesity is partly a result of genetic susceptibility, but an obesity epidemic is mainly attributable to societal and environmental changes, with changes in lifestyle.4 Pregnant mothers are also more often obese, and prenatally, a child may meet an obesinogenic environment.10 11 Mother's prepregnancy BMI and weight gain during pregnancy correlate with the offspring's risk for subsequent overweight and obesity, and mother's glucose intolerance has been shown to increase the offspring's birth weight.11–13 In some studies, higher birth weight seems to increase the child's risk for overweight and obesity, but the evidence is weak.14 15 Children with rapid weight gain during their preschool years and children who reach their BMI rebound earlier are prone to obesity.16–20 Modification of diet in infancy appears to reduce subsequent obesity risk.21 22 Since excessive weight gain begins already during preschool years, preventive interventions should start early, before pregnancy, and include pregnancy and infancy.23 So far, only few such intervention studies have been published.4 7–9
The aim of this study was to investigate whether individual counselling on diet and physical activity targeting first-time mothers with infants aged 2–10 months affects offspring weight gain by the age of 4 years.
Methods
Study design, participants and methods
A controlled trial was conducted in six maternity and child health clinics in Finland in the cities of Tampere and Hämeenlinna between the years 2004 and 2006. Aim of the trial was to evaluate the feasibility and effects of a lifestyle intervention designed to prevent excessive gestational weight gain and postpartum weight retention. The study protocol was implemented during five visits to maternity or child healthcare clinics (figure 1). The prenatal intervention study will be reported elsewhere. Feasibility of the study protocol and other details have been reported earlier.24–27

Original sample and the follow-up of the offspring, respondents and non-respondents.
The intervention study was conducted in six maternity and childcare centers, three of which volunteered to be intervention clinics and the remaining clinics were treated as control clinics. The allocation was performed at clinic level. The clinics were a convenience sample of the clinics in Tampere and Hämeenlinna as they were selected based on the clinics' administrative personnel's suggestion for suitable clinics. The participants consisted of postpartum primiparous women. The exclusion criteria were age under 18 years, type 1 or type 2 diabetes mellitus (but not gestational diabetes mellitus), twin pregnancy, physical disability preventing exercising, otherwise problematic pregnancy (determined by a physician), substance abuse, treatment or clinical history for any psychiatric illness, inadequate language skills in Finnish and intention to change residence within 3 months. The nurses recruited postpartum women when visiting their home after delivery or at their first visit to the childcare center. The eligibility of all potential participants was assessed, and all eligible women were asked to participate in the study. All participants provided written informed consent for participation. The aim was to recruit at least 40 postpartum participants in the intervention and in the control clinics form August to October 2004.
For the original trial power calculations, we used assumptions from previous literature resulting at 90% power and significance level α=0.05, which suggested 82 women per group, in total 164.28 In addition, a conservative estimation of the sample size would be at least 1.5-fold compared with this calculation because cluster randomisation was applied. The estimated dropout rate (25%) was also taken into account in the sample size calculations. With these requirements, at least 300–350 women should be recruited to the original intervention study. However, statistical significance of the results was not a priority in a pilot study and we aimed to recruit at least 60 postpartum women. Of these women, approximately 15 postpartum women were assumed to discontinue the study because of spontaneous abortion, pregnancy complications or for other reasons.
Intervention
The intervention included individual counselling on physical activity and diet when the child was 2–10 months old and an option to attend supervised group exercise sessions once a week. The content of the intervention is described in greater detail elsewhere.25 The purpose of the intervention was to promote leisure time physical activity and healthy dietary habits, thereby supporting participants' return to their prepregnancy weight during the study. In the control clinics, the nurses continued their usual counselling practices on physical activity and diet.26
Outcomes
In this study, we analysed the secondary outcome of the intervention study, namely the weight development of the offspring. The primary outcomes of the study have been reported earlier: the proportion of women returning to their prepregnancy weight by 10 months post partum. Dietary outcomes were changes in meal patterns, overall intake of vegetables, fruit and berries, use of high-fibre bread and intake of high-sugar snacks. Physical activity outcomes were MET (metabolic equivalent) minutes.25 27
Follow-up data collection
In 2010, mothers participating in the trial received a postal questionnaire on their offspring's weight development. This questionnaire was chosen for data gathering as direct access to the child health clinic records would have entailed maternal permission, and mothers have the same information on their offspring's growth as the child health clinic records. Finnish children attend child healthcare clinics several times in their first year and once a year thereafter. Children's weight was measured to the nearest 0.1 kg on a standard electronic scale. Children under 2 years were measured in recumbent position and thereafter in standing position to the nearest millimetre with a standard stadiometer. A nurse enters the height and weight measurements in the child's own health booklet for the mothers. The mothers entered these measurements in the postal questionnaire. The mothers were also asked whether their children had any long-term illnesses affecting growth (allergies or other chronic diseases), duration of breast feeding and child's age when starting solid foods.
Statistical methods
Characteristics of the study participants were described using means and SDs or frequencies and proportions. Observed weight trajectories by gender are shown in figure 2. The child's size during follow-up was analysed using weight and length/height converted to BMI (weight (kg)/height (m2))-for-age and weight-for-length/height and their SDs (z-scores) according to the recently updated Finnish growth reference.29–31 Exact age of the child was used in all analyses.

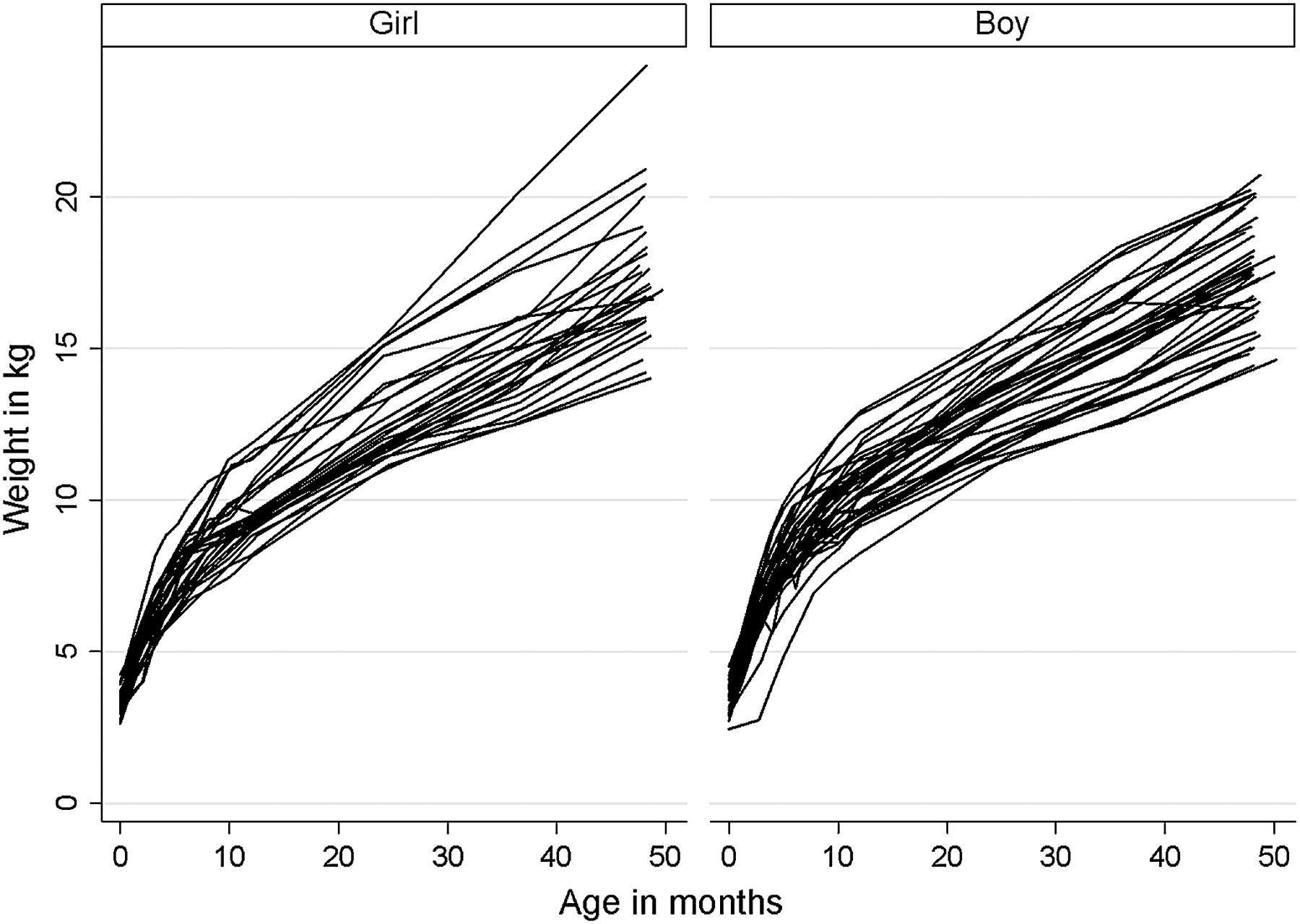
Growth trajectories by gender, exact age of the child and weight from birth to age of 48 months.
Mixed-effects linear regression models were constructed to analyse the association of weight-for-length/height z-score and BMI z-score over time by group (intervention/control). Three-level mixed-effects models consisted of fixed effects (group, child's age in months, non-linear effects AgeInMonths2 and AgeInMonths3 and interactions between group and age) and random effects (measurements within child within centre). These models allow for a difference between groups at baseline, linear changes of z-score over time and the difference of improvement between groups, which can be viewed as the intervention effect (ie, interaction term). A likelihood ratio test was used for model selection. The parameter estimates were presented with 95% CI and p values. The goodness-of-fit of the models was evaluated visually by normal probability and residual plots and also tested by the normality of the residuals (Kolmogorov–Smirnov test). All analyses were performed using STATA software (V.12.0 for Windows), StataCorp LP.
Response rate to the follow-up questionnaire was 71.9% (N=64/89). We also performed an analysis to compare mothers lost to follow-up and respondents. According to the loss-of-follow-up analysis, mothers participating in the intervention and responding to the follow-up questionnaire reported significantly lower weight before pregnancy than non-responders (61.1 vs 66.3 kg, p=0.04). There were no differences in age, employment status or smoking before pregnancy, but the responding mothers tended to be more highly educated than non-respondents (highest education group 58.7% vs 33.3%, p=0.07).
We also estimated the power for the future studies using the current sample. With a multi-level structure, the ordinary sample size estimates need to be inflated by the design effect (1+(n−1) ρ), where n is the average cluster size and ρ is the estimated intracluster correlation coefficient. When we have repeated measurements on the same child, the child is considered as the cluster. We applied the design effect after calculating a sample size (STATA, sampclus). New power estimates are shown in the Results section.
The study was approved by the Ethics Committee of the Pirkanmaa Hospital District.
Results
Mothers in the intervention group who responded to the questionnaire were slightly older than the control mothers (mean age 29.6 vs 28.4 years, p=0.195). There were no obese mothers (BMI ≥30 kg/m2) in the control group, whereas in the intervention group, there were two mothers who were obese before pregnancy, but mean prepregnancy BMI did not differ between groups (p=0.40) (table 1). Smoking during pregnancy or duration of breast feeding did not differ significantly between groups (table 1). Number of mothers reporting children's allergies (two in intervention group, one in control group) or any chronic diseases (four children in intervention and five in control group) was low and did not result to exclusion of these children. Proportion of missing mother–child dyads due to non-response was similar among intervention (N=14) and control (N=11) groups (figure 1).
Baseline characteristics of the trial groups (mean ± SD or frequency and %, difference between the groups and 95% CI)
Observed weight trajectories were slightly wider among girls than among boys until age of 48 months (figure 2). The weight gain from birth to 48 months of child's age measured as weight-for-length/height was no significantly different between the groups (figure 3).
{kind=link}
{kind=link}
{kind=link}
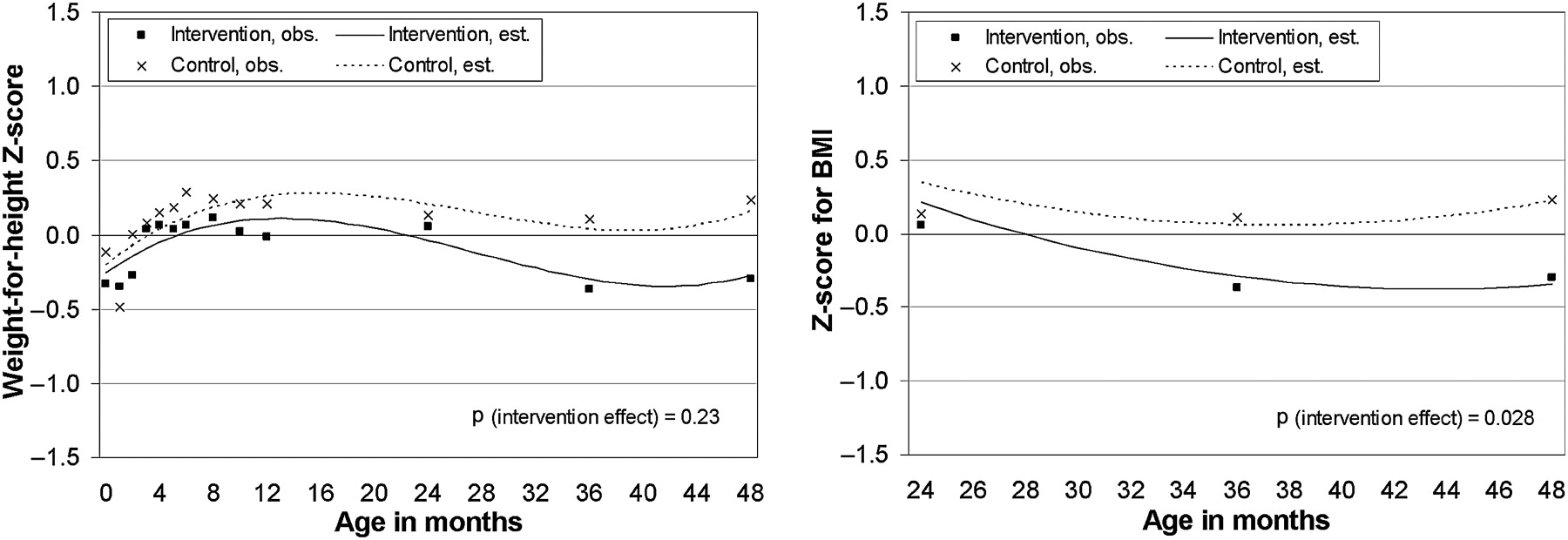
Weight-for-height from 0 to 48 months and BMI z-scores from 24 to 48 months. p Values denote for the significance of intervention effects (interaction between group and child's age at months). Non-linear model including age of the child and interaction between group × age. Obs., observed; est., estimated.
Multilevel mixed effect non-linear regression models included group, age of the child and interaction between group and age of the child. The increase of BMI z-score between 24 and 48 months was slower among the intervention group offspring (−0.034 to −0.002, p=0.028) as compared with control group. Z-scores for weight-for-length/height did not differ between groups when the period 0–48 months was analysed (p=0.23), but for the period of 24–48 months between-group differences were significant (p=0.012) (table 2 and figure 3).
Estimates and 95% CIs for z-scores for weight-for-length/height and body mass index
Based on the current data, we also estimated the sample size of the study which should be needed to achieve sufficient power for the study. From the current sample, we assume group means (SDs) of −0.3 (1.1) vs 0.2 (1.2) and intracluster correlation coefficient of 0.63 for z-score on weight for height. For future studies, 730 observations are needed, divided by the number of observations per child, 730/13=56.2, 57 children per group.
Discussion
The main finding of our study was that the offspring of the mothers receiving intensified lifestyle counselling during the period from 2 to 10 months of infant's age may have slower weight gain measured as BMI z-scores between 24 and 48 months than the children in the control group. The STRIP Study showed that children overweight at 13 years had a steeper weight gain starting at 2 or 3 years.18 Thus, our result suggests that the lifestyle intervention might reduce the risk for obesity.
Since the unfavourable health consequences of obesity already begin during childhood and the treatment of childhood obesity tends not to lead to permanent results, early preventive measures are needed.4–6 23 One of the early determinants for obesity, type 2 diabetes and cardiovascular disease is rapid growth in early childhood.16 18 19 32 33 Most of the evidence published so far on rapid early growth and subsequent increased risk for obesity has concerned infants, but there is also similar evidence regarding later preschool years.18 19 34 35 To the best of our knowledge, no previous controlled intervention trials have targeted only mothers during child's first year and included both diet and physical activity counselling.8 9 Our study was follow-up of a cluster-randomised trial conducted in child health clinics. The participants were first-time mothers without specifically sought risk determinants for having overweight offspring. There were no statistically significant differences between the groups regarding mother's age before pregnancy, prepregnancy BMI, gestational weight gain, education, smoking during pregnancy or duration of breast feeding. In the intervention clinics, the mothers received individual counselling on diet and physical activity and the option to attend supervised group exercise sessions once a week during the first 10 months of infant's life. The control group received conventional healthcare counselling.
The strengths of our study include a feasible counselling method, controlled trial setting and reliable growth data based on repeated measurements by nurses in primary child healthcare.25 26 We also utilised the recently updated growth data on Finnish children by using z-scores of weight-for-length/height and BMI-for-age described in that growth data.29 Our sample included healthy first-time mothers thereby constituting a more homogeneous group than mothers with earlier deliveries. We were also able to take account of confounding factors on childhood growth, such as mothers' smoking and prepregnancy BMI. We have shown earlier that intensified counselling both during pregnancy and postpartum results in changes in mother's dietary and physical activity behaviour.24–27 36 Therefore, the beneficial sequelae in offspring weight gain found in this study are more probable than without an effective counselling method.
The weaknesses of our study include the relatively small number of participants and clusters. In spite of this, clinic level was taken into account in the models. The respondents were also more often highly educated and had lower prepregnancy weight than the non-respondents. Therefore, selective response may have influenced the result, and the abovementioned selection may have diminished the intervention effect. The possibility of Hawthorne effect cannot be denied either. Another reason for the small observed differences between groups may be that the participant mothers as a group had no special risk characteristics of having overweight children, such as obesity or low social class.4 The proportion of overweight children tends to increase with age, and longer follow-up time might have revealed increasing differences between the groups.4 37 38
Power of the study was insufficient, but the primary aim of the original trial was to evaluate the feasibility of the counselling protocol. According to our estimates based on the current sample, at least 57 children are needed per group for future intervention studies concerning childhood obesity prevention.
The positive intervention effect on offspring weight gain is probably mediated by the healthier diet and increased physical activity adopted by the intervention mothers. The role of parents is vital in facilitating sustainable lifestyle behaviour in their offspring, and early childhood is a critical period in the acquisition of food preferences and physical activity habits.23 39 The impact of the intervention via mother and her breast milk on infant's early nutrition could partly explain the effect of the lifestyle intervention on offspring weight gain: infants have been shown to acquire a flavour bridge through breast milk, which is influenced by mother's diet, making it easier for a child to accept these flavours in her diet.40
Conclusions
In our study, the intensified lifestyle intervention targeting mothers during child's first year may reduce weight gain in the offspring until 4 years of age. By slowing the weight gain, such an intervention targeting this crucial growth period could be one means of combating the obesity epidemic. To break this intergenerational circle of obesity and its complications, initiating early prevention programmes targeting mothers before, during and after pregnancy is essential, likewise community-based preventive actions.4 5 23 Larger randomised controlled trials are needed to gather more evidence for selecting the most effective preventive programmes.
Acknowledgments
We thank Tarja I Kinnunen and Minna Aittasalo for planning the physical activity and diet counselling of the trial, we thank Ms Päivi Viitanen of the UKK Institute for Health Promotion who participated in data collection and coding; Kirsi Mansikkamäki, MSc; Mrs Ulla Hakala; Mrs Ulla Honkanen; Mrs Taru Helenius and Mrs Sirke Rasinperä of the UKK Institute laboratory participated in data collection. We gratefully acknowledge the participating parents and children and nurses in maternity and child healthcare in the six clinics in Tampere and Hämeenlinna.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
To cite: Mustila T, Raitanen J, Keskinen P, et al. Lifestyle counselling targeting infant's mother during the child's first year and offspring weight development until 4 years of age: a follow-up study of a cluster RCT. BMJ Open 2012;2:e000624. doi:10.1136/bmjopen-2011-000624
Funding This project was funded by the Competitive Research Funding of the Tampere University Hospital (Dr Riitta Luoto, grant 9G042, Dr Päivi Keskinen), Medical Research Fund of Vaasa Hospital District (Dr Taina Mustila), this project was funded by the UKK Institute for Health Promotion (Tampere, Finland), the Ministry of Health and Welfare, the Academy of Finland and the Foundation of Pediatric Research (Finland).
Competing interests None.
Ethics approval The study was approved by the Ethics Committee of the Pirkanmaa Hospital District.
Contributors RL is the guarantor of the study. TM, PK and RL planned the follow-up questionnaire to the mothers. TM coded the data together with a research assistant. AS produced the BMI-for-age statistics and participated in the interpretation of the BMI-for-age results. JR performed the statistical analyses. All contributors participated in drafting the manuscript and approved the final manuscript. All authors had full access to all data (including statistical reports and tables) in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix, statistical codes and data set available from the authors at email riitta.luoto{at}uta.fi. Consent for data sharing was obtained from the participants.