Article Text

Abstract
Objective To investigate changes in incidence of admissions for schizophrenia and related non-affective psychoses in North Wales.
Design Data from two epidemiologically complete cohorts of patients presenting for the first time to mental health services in North Wales between 1875–1924 and 1994–2010 are used in this study to map the incidence of hospital admissions for schizophrenia and non-affective psychoses.
Setting The North Wales Asylum Denbigh (archived patient case notes) and the North West Wales District General Hospital psychiatric unit.
Population 3168 patients admitted to the North Wales Asylum Denbigh between 1875 and 1924 and 355 patients admitted to the District General Hospital psychiatric unit between 1994 and 2010.
Results There was an increasing admission incidence for schizophrenia between 1875 and 1900, a higher admission rate in the 1990s for men, followed by a drop in rates of admission for both genders since 2006. Admission incidences switch from parity between the sexes in the historical period to a doubling of the admission rates for men compared with women in the modern period. This admission pattern differs from the admission patterns for affective psychoses or organic disorders.
Conclusion There have been changes in the incidence of admissions for schizophrenia in North Wales.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
This article investigates the incidence of schizophrenia and related psychoses in the 19th, 20th and 21st centuries.
It is a first report covering both historical and contemporary data drawn from one geographical area, with comprehensive patient ascertainment.
The data address longstanding questions concerning the incidence of schizophrenia in historical and contemporary periods.
Key messages
This article is the first to report a specific rise in the admission incidence of schizophrenia in the 19th century. It reports a specific drop in the admission incidence of schizophrenia in the 21st century.
It demonstrates a switch in gender ratios for this illness in cohorts drawn from the same ethnic group and geographical area.
Strengths and limitations
This study has unique access to 19th and early 20th centuries asylum records.
The late 20th and early 21st century diagnosis are drawn from clinical consensus rather than administrative databases.
It is unlikely that the historical arm of this study can be replicated elsewhere. Confirmation of the findings will hinge on studies of 21st century incidence rates.
This is a study of hospital admission incidence and is therefore one step removed from the true incidence.
Introduction
In the 19th century, as British asylum beds filled, asylum superintendents and others regularly worried that the incidence of insanity was increasing.1 In the late 20th century, the issue of whether there had been an absolute increase in insanity in the 19th century came to the fore when Torrey,2 Hare3 and others argued that the unquestioned increase in admissions pointed to a true increase, postulating that this might indicate that schizophrenia or other non-affective psychoses were triggered by infections or other toxic processes. Others such as Scull4 drew attention to the capacity of, and interests of, medical systems to fill beds and suggested that increases in hospital populations need not reflect an increase in the incidence of the disorder.
Shortly thereafter, a series of articles5–9 provided data consistent with a possible decline in the incidence of schizophrenia in the late 20th century, but more recent studies have not found any decline in rates of psychosis.10–12
The conflicting results in the modern studies have drawn attention to a range of methodological confounders from changing diagnostic criteria to the unreliability of administrative case registers, issues of age standardisation, the changing ethnic mix of populations and shifts in patterns of care.13 Many of these factors can be controlled for in contemporary populations.
In contrast, on the issue of whether there was an increase in insanity in the 19th century, the available data for the most part do not permit distinctions between increases in insanity in general and increases in specific diagnoses such as schizophrenia.
The task of pinpointing aetiological factors contributing to schizophrenia is likely to be somewhat easier if any periods of increase or decrease can be established. In North West Wales, we have access to two case registers that while posing their own methodological issues overcome some of the difficulties of other studies. These have been explored to shed light on the incidence of admissions for all non-affective psychoses and for schizophrenia in particular.
Methods
We have used two data sets to look at admission rates for schizophrenia and other non-affective psychoses drawn from the periods 1875–1924 and 1994–2010. In North West Wales, geographical and financial constraints ensured that there was nowhere else for 19th century patients to go other than the asylum at Denbigh, and today, there are no private facilities or alternate public facilities for patients other than the District General Hospital (DGH) unit in Bangor. Patients from North West Wales furthermore getting sick elsewhere in both periods have been returned to the area for treatment.
The first data set consists of all admissions from North West Wales to the asylum at Denbigh between 1875 and 1924. The asylum records offered five sets of information relevant to diagnosis: medical and legal certificates outlining the circumstances of detention; standard demographic data including age, sex, educational, employment and marital status, family history of mental illness, prior mental or physical illness and possible triggers; standard assessments of dangerousness, suicidality, seizure proneness, along with food refusal and a range of clinical features; descriptions of patients' mental and physical states on admission and case notes covering patients' stays in hospital until discharge or death.14 We could retrieve the records of prior admissions back to 1865 or subsequent admissions through to 1965.
The term schizophrenia was not used in asylum records until after 1924. Throughout the historical period, psychotic patients were primarily diagnosed as having mania.15 Accordingly, a panel of clinicians covering the clinical patches these patients would now come from reviewed records from all admissions for each patient14 and made retrospective diagnoses according to the International Classification of Diseases (ICD)-10 criteria.
A diagnosis of non-affective psychosis was made if there was clear evidence of delusions, hallucinations or thought disorder in the clinical record, an absence of affective symptoms and a clinical course consistent with the diagnosis. All diagnoses were made before this study began. In the case of the psychoses, five diagnoses were given: schizophrenia (F20), schizoaffective disorder (F25), delusional disorder (F22), acute and transient psychoses (F23) and catatonia (F0.61). Other patients who were difficult to classify were coded as unspecified non-organic psychosis (F29). The schizoaffective group were primarily schizophrenic rather than affective in features and were a small group (N=26).
One coauthor (SCL) reviewed all affective and non-affective diagnoses covering eight randomly picked years from the whole sample. The agreement concerning the schizophrenic diagnoses (F20) between the initial rater and SCL was 96.5%. To take account of the number of agreements expected by chance, we used Cohen's κ coefficient,16 a statistical measure of inter-rater agreement for categorical items. The κ coefficient (781 cases, two raters, schizophrenia vs all other diagnoses) was 86.4%.
The second data set is drawn from an ongoing study of the incidence of service utilisation for non-affective and affective psychoses from North West Wales. From this, we have assembled all first admissions to the sole DGH unit accessible from the area between 1 January 1994 and 31 December 2010 or to the regional medium secure facility or to any other unit to which patients could be admitted. The catchment area for the modern cohort is the same as that for the historical cohort. Patients were included in this study if they were native to or resident in the North West Wales area prior to and following their initial episode. We have not included patients who became ill after coming from elsewhere as students to the local university and who have since left the area. In similar fashion in the contemporary and historical cohorts, we have excluded patients who came from out of area and returned to their place of origin but who had a first episode of mental illness while in North West Wales. We have included patients admitted solely for the purpose of instituting treatment with clozapine.
Diagnoses in the contemporary cohort were made according to ICD-10 codes, but they were not made on the basis of administrative coding by ward clerks of individual admissions. In the case of all patients, the diagnoses came from medical and nursing staff on the treating team. Case records were checked on several occasions and following all subsequent admissions to confirm the presence of clinical details consistent with the diagnosis. These diagnoses therefore take clinical course into account, and not unexpectedly, only 49% of those diagnosed as having schizophrenia were given that diagnosis on first discharge.
The population of North West Wales has remained roughly the same over a century, but there are differences in numbers of younger subjects and in those over the age of 55. Using census data from 1881, 1891, 1901 and 1911, we have accordingly standardised our incidence figures for the contemporary sample to the rates observed for the historical sample. (Much of the 1921 census data were destroyed in a fire.) Population data for the period 1875–1924 came from the Register General Annual Reviews 1881–1921 obtainable from the Office of National Statistics.17 Data for the contemporary sample came from the Office of National Statistics.
We have collected data from 1875, when we are confident that there are no gaps in the admission record. Hospital documents from 1876 to 1877 make it clear that there was pressure on beds pending the opening of a new unit in 1881.18 There was similar correspondence in 1895. These documents point to unexpected rates of incarceration and complicate annual figures. We are therefore providing all the data from the period 1875 to 1924 for analysis.
In comparing modern and historical samples, we have calculated a standardised psychosis rate for the period 1885–1924. This choice of period offers a lower estimate of the standard admission rate than would have been derived from using the period 1900–1924. Against the background of this standardised psychosis rate, we compared the incidence rates for schizophrenia and other psychoses for the periods 1875–1924 and 1994–2010.
The number of all psychoses for the period 1885–1924 was tabulated for each year, sex and age (0–14, 15–24, 25–34, 35–44, 45–54, 55–64 and 65+) combination. The population at risk in each year was taken to be the population from the nearest census year for the same age and sex combinations. From these figures, an average psychosis rate over the historical period can be calculated. This rate was then applied to the population in each age and sex combination for the 2001 census. This gives the expected number of psychoses for each year between 1994 and 2010. A standardised psychosis ratio (SPR) is calculated by dividing the observed number of cases with that expected and multiplying by 100. CIs for the SPR were calculated using the exact method detailed in Estève et al.19 This method was used to calculate an SPR for all psychoses as well as successively a diagnosis of schizophrenia (F20, F25 and F0.61) including and not including F22, F29 and F23 cases.
Results
In the historical sample, there were 3168 patients admitted between 1875 and 1924. Of these patients, 1074 were retrospectively diagnosed as having a non-affective psychosis, of whom, 605 (56%) had schizophrenia (F20) or schizoaffective disorder (F25), 143 (13%) had delusional disorder (F22), 143 (13%) an acute and transient psychosis (F23), 135 (13%) had other non-organic psychoses (F29) and 48 (4.5%) had a catatonic disorder (F0.61).
These 1074 patients had 1372 admissions between them over their lifetime. Five hundred and fifty-eight (52%) patients were women and 516 (48%) were men. Six hundred and forty-nine patients (60%) were single, 319 (30%) were married, 85 (8%) were widowed, 7 (0.6%) were separated or divorced and for 14 patients, marital status was not recorded. The gender ratios and median age at first hospitalisation for all diagnostic groups in both the contemporary and historical samples are given in table 1.
Median age at first hospitalisation by diagnosis and sex in historical and contemporary cohorts
The contemporary sample consists of 355 patients, of whom, 227 (64%) had schizophrenia or schizoaffective disorder, 66 (19%) an acute and transient psychosis, 48 (14%) delusional disorder, and 14 (4%) patients were non-organic psychoses (F29). We have not included 27 drug-induced psychoses (F19)—disorders lasting 24–72 h accompanied by clear evidence of drug intake that resolved once the drug cleared the patient's system and with no further psychotic episodes. We have included patients with psychoses whose admissions were linked to drug intake and patients with a first admission for drug-induced psychosis who later developed schizophrenia.
Of these 355 patients, 137 (38%) were women and 218 (62%) were men. No data regarding marital status were available for the contemporary sample. Of the patients given a definitive diagnosis of schizophrenia (F20 and F25), 49% were given this diagnosis on admission. Of those later diagnosed as having schizophrenia, 12% were initially diagnosed as having an acute and transient psychosis (F23), 11% as having a drug-induced disorder, 10% as having a delusional disorder (F22) or unspecified psychosis (F29), 10% as having a mood disorder and 7% with other diagnoses. Of the delusional disorder (F22) and acute and transient (F23) patients, 56% and 58%, respectively, had this diagnosis on first admission.
The data presented in table 2 and figures 1–5 point to an increasing rate of first admissions for non-affective psychoses through to approximately 1900. In the modern period, they show a divergence in rates of admissions for men and women with contemporary rates for women at or below the SPR, while rates for men substantially exceeded the SPR until quite recently. It should be noted that the visual representation, utilising a conservative SPR, tends to minimise appearances of an increase in the 19th century and a decline in the 21st century.
All admissions by year, diagnosis and sex: historical and contemporary cohorts
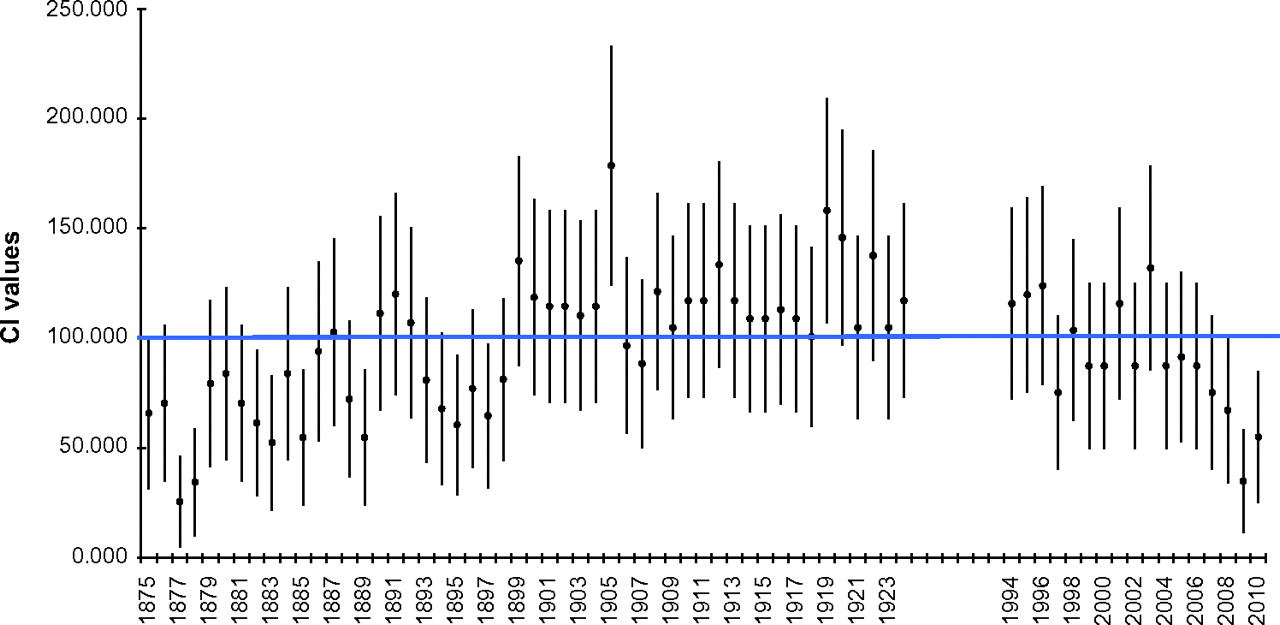
Admission incidence for all psychoses (including F23) between the periods 1875–1924 and 1994–2010.

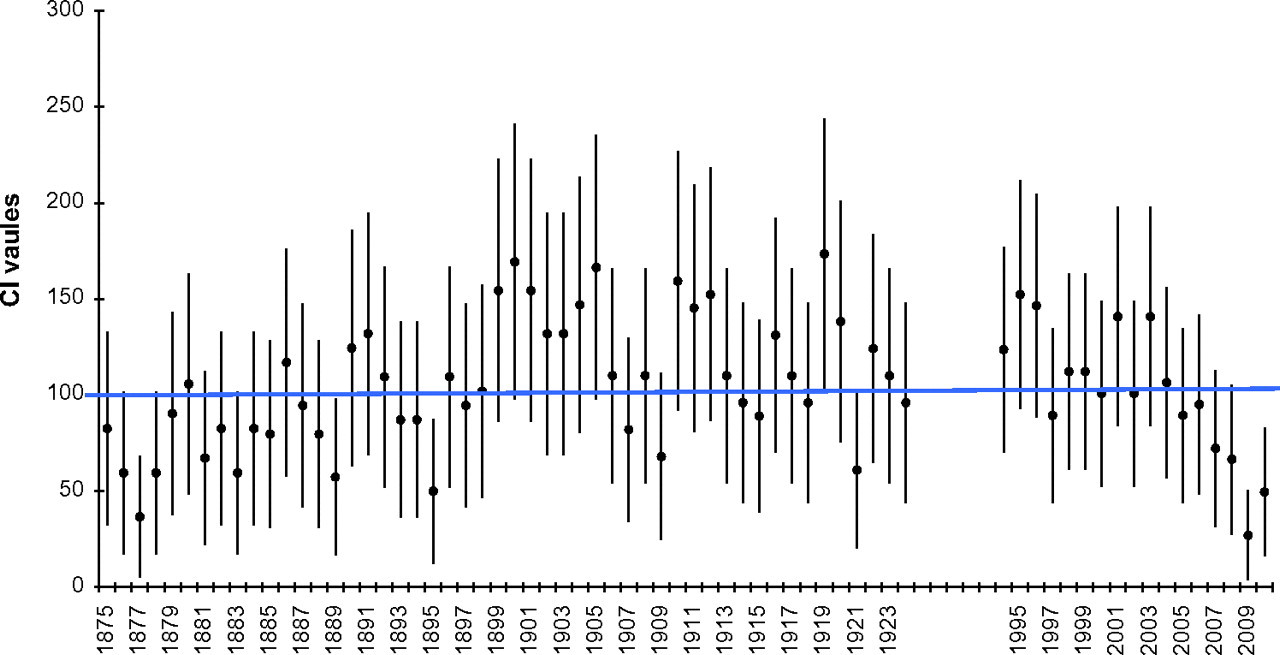
Admission incidence for all psychoses (excluding F23) between the periods 1875–1924 and 1994–2010.
Admission incidence for schizophrenic psychoses (F20, F25 and F06.1) between the periods 1875–1924 and 1994–2010.

Admission incidence for schizophrenic psychoses (F20, F25 and F06.1)—men 1875–1924 and 1994–2010.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Admission incidence for schizophrenic psychoses (F20, F25 and F06.1)—women 1875–1924 and 1994–2010.
The contemporary period shows a reduced rate of F29 diagnoses. This is an artefact, in that, F29 is a default diagnosis for ambiguous cases and in the case of the historical sample deficiencies in the records contributed to a greater difficulty in being certain of the diagnosis in a small minority of cases.
Accordingly in analysing the data, we have successively compared contemporary rates of hospitalisation for all non-affective psychoses (F20–29), for schizophrenia (F20, 25 and F0.61), for schizophrenia with delusional disorder (F20, F22 and F25) and for schizophrenia with both delusional disorder and other non-organic psychoses (F29) (excluding F23) with the respective standardised psychosis rates for these diagnostic groupings from the historical period. This sensitivity analysis shows that the increase in admissions for psychosis in the historical period and decline in admissions in the modern period holds whether a broad diagnosis such as psychosis or narrow diagnosis such as schizophrenia is adopted.
In other studies, we have looked at year of first admission for admissions in the historical database for all affective psychoses, as well as for organic and neurotic disorders, and, as discussed below, can rule out the possibility of diagnostic leakage as an explanation for the data reported here.
Discussion
Establishing temporal or geographical variations in the incidence of a disorder can contribute to a discovery of aetiological factors, especially if both increases and decreases in incidence can be pinpointed.
For 30 years, there has been an inconclusive debate about possible increases in rates of schizophrenia in the historical record. The material available has not permitted an analysis that might distinguish between competing explanations. There have also been claims and counterclaims about the incidence of schizophrenia and related psychoses in modern times. A drop in the contemporary incidence of admissions without evidence of an increase at some point in time would lead to a different set of hypotheses regarding contributory factors than evidence of both increases and decreases.
This study gives unique data on the incidence rates of hospital admission for schizophrenia and related psychoses compared with other disorders in the 19th and early 20th centuries along with data from the same catchment area for the later years of the 20th century and early years of the 21st century. The data point to a possible increase in admission incidence for schizophrenia in the 19th century and a possible recent decline in admission incidence.
Unlike other studies that employ historical data, we have been able to go behind the data to get some indication as to the contribution made by specific diagnostic groups to changing rates of admission. In addition to being more diagnostically specific, our data on this issue offer admission incidence rather than admission prevalence rates.
Thus, our published figures for first admissions for depressive psychoses in North West Wales show no rise in the historical period but show a reduced rate of admissions in the contemporary period without the more recent decline.20 Our unpublished figures for bipolar disorder in North West Wales show no rise in incidence rate in the historical period, no change in incidence rate in the modern period and no difference between historical and modern periods. The bipolar admission rate moreover is only 10% of the admission rate of schizophrenia and related psychoses. Hence, the findings for non-affective psychoses reported here cannot be explained by shifting diagnostic fashions between affective and non-affective groups.
In addition to the above, we tracked admissions for neuroses, personality disorders, organic disorders (including General Paralysis of the Insane (GPI) and epilepsy), dementias, mental handicap, and alcohol-related disorders across the historical period. There is a constant rate of first admissions for these groups except for GPI and epilepsy which show a rise in the 1890s, so that admissions from 1890 to 1924 run at double the pre-1890 rates (16 vs 8 cases/year).
Given these data, the following points can be made about the historical period. First, there was some increase in all diagnoses due to an expanding population that is not present when the population is standardised by age. Second, if there was a ‘warehousing’ of patients with mental disorders, this appears to have applied across all diagnostic groups. Third, there was a specific increase in admissions for schizophrenia not found for other disorders.
Admissions for schizophrenia and other non-affective psychoses ran at 35% of the total number of admissions in the historical cohort. Admissions for organic disorders including dementia and mental handicap also ran at 35% of the total. Admissions for mood disorders were 26% of the total, and admissions for neurotic and related disorders were 4%. The population with schizophrenia appears therefore sufficiently large for increases from this source to have fuelled a debate in the 19th century that could not be readily resolved in the absence of specific diagnostic criteria as to whether the observed increase could be entirely explained in terms of increases in the population or a warehousing of patients.
This increase in a condition that proved resistant to ‘moral treatment’ might also explain to some extent the confounded expectations of asylum builders and medical personnel who found later 19th century recovery rates compared unfavourably with earlier 19th century rates.21 In contrast to schizophrenia, patients with manic-depressive illness, acute and transient psychoses and melancholia did recover and leave hospital in line with the expectations of asylum builders, and indeed for melancholia, there were reduced rates of readmission than are found for severe unipolar depression today.20
As regards the changing data between 1875 and 1924, there are a number of notable peaks and troughs in admission incidence for non-affective psychoses. The low rate of admissions in the mid-1870s is linked to letters from the hospital administrators to local magistrates, doctors and relieving officers telling them the asylum was full and that patients could not be guaranteed an admission.18 22 There were similar letters in the mid-1890s. But these letters do not coincide with any drop in admissions for affective psychoses or organic disorders at these times, suggesting that the lower rate of admission for schizophrenia in the 1870s compared with later does not stem from this source.
There are in contrast peaks in admission rates for non-affective psychoses at 1905 and again in 1919 and 1920. Analysis of admissions at these points shows that the increase in 1905 stemmed from an increase in acute and transient psychoses linked to the Welsh religious revival of 1904–1905.23 There is another peak in admissions for acute and transient psychoses the year after the end of the World War and the influenza epidemic of 1918. These latter admissions are not attributed as directly to social dislocation as were the admissions of 1905 but they share many of the formal characteristics of the 1905 set of admissions and the increase is primarily in diagnoses of acute and transient psychoses (F23).
Acute and transient psychoses share many clinical features in common with schizophrenia and would at many times and in many settings have been diagnosed as benign prognosis schizophrenia. We have shown, however, that these cases display a different phenomenology and follow a different clinical trajectory to cases of schizophrenia.23 It is a moot point whether these cases are better regarded as reactive psychoses distinct from schizophrenia rather than good prognosis schizophrenia. Their importance for this study is that they open up the prospect that short-lived changes in the incidence of these conditions can lead to significant changes in the overall incidence of psychosis, and for this reason, it is important to analyse all psychoses together but also to separate the enduring psychoses from acute and transient psychoses or other psychoses of less certain character. This combination of peaks and troughs also points to the hazards in basing conclusions on relatively brief time spans, such as the period from 2005 to 2010.
Before considering the contemporary cohort, it is worth noting that this is not a comparative study of admission incidence in a historical and contemporary cohort and can only study the ‘true’ incidence of the illness by proxy. The probability of an admission for schizophrenia in the two periods may not ever be something that can be established. But the first point to make is the contemporary decline in admissions for psychosis in this service is against a background of a greatly increased admission prevalence for the service compared with the late 19th century.14 There are now 15 times more admissions than a century ago to the North West Wales service, seven times more admissions for psychotic disorders than before and a threefold greater rate of compulsory detention than before. Compared with a century ago, there is no evidence for a bias against admission. All patients with schizophrenia in the historical period were admitted compulsorily. In the modern period while many patients were admitted informally, 94% of the patients with schizophrenia recorded here have had more than admission, at least one of which was compulsory.
In the historical cohort, we began collecting data 28 years after the asylum opened in part to minimise any bias against admission. Given that dangerousness was the key criterion for admission to the asylum in the historical period, one might expect a greater incidence of male admissions if significant numbers of patients were left unadmitted. The equivalent rates of admission in men and women in the 19th century suggest that comparatively few patients with schizophrenia were left unadmitted or the alternate explanation that schizophrenia was once dramatically more prevalent among women than now. If it is still thought that there were more unadmitted patients with schizophrenia historically, this would make the pronounced decline in contemporary period even more significant.
The apparent decline in admission incidence in the contemporary period is relatively brief but there are aspects to the data that suggest it should be taken seriously. First, the admission rate has dropped to a historically unprecedented level. Second, there is a changing gender ratio, which is specific to schizophrenia. In the data from 1875 to 1924, the rates were almost identical in both sexes (52% female). By 1994, this had changed so that in the years from 1994 to 2005, the incidence of male admissions for first episode psychosis is double that of female admissions. The 2:1 ratio of male-to-female admissions maps onto other data from British studies in the present day period,24 while the historical data are in accordance with perceptions of an equal gender ratio formerly.
Thus, while overall admission rates for all psychoses and for schizophrenia were almost indistinguishable between the 1885–1924 and 1994–2010 cohorts, these rates conceal an increased rate of male admissions for schizophrenia and a decline in female admissions for schizophrenia possibly antedating the 1990s. This finding is consistent with data reported by Waddington and Youssef9 that point to an even earlier decline in female admissions.
No one has collected data on the admission incidence rates for psychosis in North West Wales in the seven decades between 1925 and 1993. This is a period in which others have reported an increase in admission incidence rates for schizophrenia elsewhere.12 Such increases are not inconsistent with our data, especially the data for males.
In the contemporary period, the most salient finding is a decline in admission incidence for schizophrenia from 2005. This cannot be explained in terms of administrative coding procedures or in terms of service changes. In North West Wales during this period, there were no bed shortages; the DGH unit ran at approximately 85% bed occupancy. There was no change in service delivery—community mental health teams were well established before this study began. No service innovations were put in place such as early intervention services or home treatment or assertive outreach teams. The medical staff have remained the same throughout or been replaced by their trainees, and so diagnostic patterns are likely to have been more stable than average. The ethnic mix in the local population is unchanged.
If the recent drop in incidence rates reflects a true decline rather than the consequence of some administrative change, what candidates might be responsible for this change? There is a widespread perception that schizophrenia involves neurodevelopmental disturbances. If this is the case, then factors contributing to a decline in rates from 2005 onwards should be operative around the period 1975–1985, as 25 is the median age of first admission for schizophrenia today.
The most parsimonious explanation should account for both a 19th century increase and a 21st century decline. One possibility is increasing exposure to lead during the 19th century and a reduced exposure since the mid-1970s. A second is the emergence of anaesthesia with a consequent increased use of forceps and other measures in the 19th century and an increased turn to caesarean sections from the mid-1970s onwards.
A more general point needs to be made. There is something of a bias against thinking that mental illnesses can emerge and disappear. Using this database, however, we have also reported a near disappearance of postpartum psychoses in North West Wales during this same period.25 This disappearance does not involve administrative sleight of hand; it has led to a closure of mother and baby units across North Wales,25 just as falls in the incidence of tuberculosis in the 1950s led to the closure of tuberculosis beds.
We have also in this database found a contemporary decline in admission rates of depressive psychoses.20 While the present data offer specific incidence rates for schizophrenia, the combination of changes in postpartum, affective and non-affective psychoses point to the possibility that what is changing is a propensity to psychosis rather than to a specific disorder.
There are a few other points to note about the data. We have sufficient numbers to break down the psychoses into broad groupings. But within the schizophrenia group, there traditionally have been hebephrenic, catatonic and paranoid groups.26 The data are not sufficient to offer numerically definitive statements about cases of hebephrenia, but no cases were coded in the contemporary sample, while there were a number of cases in the historical record consistent with such a diagnosis.
In a separate study, we have demonstrated a disappearance of frank catatonia, although elements of the condition remain as common as ever.27 The change in presentations seems most likely to be linked to the use of benzodiazepines which given coincidentally reduce the likelihood of such states evolving.
In conclusion, data we have reported earlier on postpartum psychoses demonstrate that specific psychoses can in fact disappear. Having made this point, it is almost inconceivable that all psychoses could disappear in that a range of brain-damaging conditions from head injuries to chromosomal conditions contribute to the development of psychoses, and such contributions will almost certainly continue. Against this background, changes in the apparent incidence of what has been termed schizophrenia may point to a drop in certain conditions that predispose to specific psychotic presentations, especially psychoses that run a chronic course. In the next few years, other conditions such as better survival for premature babies may lead to an increase in chronic psychoses or to somewhat different psychosyndromes to the disorders hitherto termed schizophrenic. In the meantime, the data here call for an explanation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
All authors had full access to all the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
To cite: Healy D, Le Noury J, Linden SC, et al. The incidence of admissions for schizophrenia and related psychoses in two cohorts: 1875–1924 and 1994–2010. BMJ Open 2012;2:e000447. doi:10.1136/bmjopen-2011-000447
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Ethics approval This study was approved by the North West Wales Acute Hospitals Trust Ethics Committee.
Contributors DH, MH and JLN conceived the study. DH, MH, JLN, AP, DL and SCL contributed to the data collection. AP, DL and SCL contributed to the diagnostic process. MH, JLN, DB and CW analysed all the data. All authors contributed to the design of the article, to the interpretation of the results and to the review of the literature. DH wrote the first draft of the manuscript and all authors reviewed and commented on the original and successive drafts and all approved the final version.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We are happy to share our data but will need to be advised about patient confidentiality issues.