Article Text

Abstract
Objective To assess the efficacy and harms of adding medical cannabis to prescription opioids among people living with chronic pain.
Design Systematic review.
Data sources CENTRAL, EMBASE and MEDLINE.
Main outcomes and measures Opioid dose reduction, pain relief, sleep disturbance, physical and emotional functioning and adverse events.
Study selection criteria and methods We included studies that enrolled patients with chronic pain receiving prescription opioids and explored the impact of adding medical cannabis. We used Grading of Recommendations Assessment, Development and Evaluation to assess the certainty of evidence for each outcome.
Results Eligible studies included five randomised trials (all enrolling chronic cancer-pain patients) and 12 observational studies. All randomised trials instructed participants to maintain their opioid dose, which resulted in a very low certainty evidence that adding cannabis has little or no impact on opioid use (weighted mean difference (WMD) −3.4 milligram morphine equivalent (MME); 95% CI (CI) −12.7 to 5.8). Randomised trials provided high certainty evidence that cannabis addition had little or no effect on pain relief (WMD −0.18 cm; 95% CI −0.38 to 0.02; on a 10 cm Visual Analogue Scale (VAS) for pain) or sleep disturbance (WMD −0.22 cm; 95% CI −0.4 to −0.06; on a 10 cm VAS for sleep disturbance; minimally important difference is 1 cm) among chronic cancer pain patients. Addition of cannabis likely increases nausea (relative risk (RR) 1.43; 95% CI 1.04 to 1.96; risk difference (RD) 4%, 95% CI 0% to 7%) and vomiting (RR 1.5; 95% CI 1.01 to 2.24; RD 3%; 95% CI 0% to 6%) (both moderate certainty) and may have no effect on constipation (RR 0.85; 95% CI 0.54 to 1.35; RD −1%; 95% CI −4% to 2%) (low certainty). Eight observational studies provided very low certainty evidence that adding cannabis reduced opioid use (WMD −22.5 MME; 95% CI −43.06 to −1.97).
Conclusion Opioid-sparing effects of medical cannabis for chronic pain remain uncertain due to very low certainty evidence.
PROSPERO registration number
CRD42018091098.
- pain management
- cancer pain
- general medicine (see internal medicine)
Data availability statement
Data are available on reasonable request to the corresponding author at: bussejw@mcmaster.ca.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first meta-analysis to pool the results of randomised controlled trials and observational studies exploring the opioid-sparing effects of medical cannabis among people living with chronic pain.
We conducted a comprehensive search for eligible studies, appraised the risk of bias of included studies and evaluated the certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation approach.
Most observational studies incorporated inadequate adjustment for confounding, and all randomised trials, despite reporting this outcome, were not designed to address the effect of medical cannabis on opioid use.
Introduction
Chronic pain affects approximately one in five adults and is a common reason for seeking medical care.1 2 Opioids are commonly prescribed for this condition, particularly in North America;3 however, they only provide benefit to a minority of patients. A 2018 systematic review of 96 trials found high certainty evidence that, versus placebo, opioids provide important pain relief (≥1 cm improvement on a 10 cm Visual Analogue Scale (VAS) for pain) to 12% of patients for whom they are prescribed.4 Moreover, opioids are associated with harms such as overdose and death,5 6 which are dose dependent.7–10 As a result, there is considerable interest in therapies that may allow patients with chronic pain using opioid therapy to reduce their opioid intake.
One promising approach is adding cannabis therapy, which low certainty evidence suggests may be similarly effective to opioids for reducing pain and improving physical functioning among people living with chronic pain.4 Experimental studies have shown that opioids and cannabis have similar signal transduction systems,11 and observational studies in the USA demonstrated that the rates of opioid-related mortality reduced after cannabis was legalised.12–14 Between 64% and 77% of patients with chronic pain responding to cross-sectional surveys reported a reduction in long-term opioid use after adding medical cannabis to their treatment.15 16 A 2017 systematic review concluded that preclinical studies provided robust evidence for the opioid-sparing effects of cannabis.17 To clarify the issue, we undertook a systematic review of randomised controlled trials (RCT) and observational studies to explore the impact of adding medical cannabis on opioid dose, other patient-important outcomes and related harms in patients with chronic pain using prescribed opioid therapy.
This systematic review is part of the BMJ Rapid Recommendations project, a collaborative effort from the MAGIC Evidence Ecosystem Foundation (www.magicevidnece.org) and BMJ. This systematic review informed a parallel guideline published on BMJ.com18 and MAGICapp (https://app.magicapp.org/#/guideline/jMMYPj).
Methods
We followed standards for Meta-analysis Of Observational Studies in Epidemiology19 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.20
Eligibility criteria
We included RCTs and observational studies, including cohort studies and case–control studies, in any language, that explored the impact of adding medical cannabis (ie, phytocannabinoids, endocannabinoids or synthetic cannabinoids) on the use of prescription opioids among people living with chronic pain. We defined pain as chronic if patients reported that symptoms had persisted for ≥3 months.21 We excluded editorials, letters to the editor, preclinical studies, conference abstracts, case reports, case series, cross-sectional studies and studies with less than 2 weeks follow-up. We also excluded studies of recreational cannabis use as these products typically contain much higher amounts of the psychotropic cannabinoid tetrahydrocannabinol (THC) than would be administered for therapeutic purposes.22 23 We classified observational study designs according to recommendations by the Cochrane Observational Studies Methods Group.24
Literature search and study selection
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), EMBASE and MEDLINE from inception to March 2020 with no restriction on language of publication. An experienced medical librarian (RJC) developed our database-specific search strategies (online supplemental appendix A). We also searched the ClinicalTrials.gov registry to identify ongoing trials, and reference lists of all eligible studies and related systematic reviews for additional eligible studies. Two teams of paired reviewers independently screened titles, abstracts and full-text studies for eligibility using online systematic review software (Rayyan QCRI, Qatar Computing Research Institute). Reviewers resolved disagreements through discussion.
Supplemental material
Data collection
Using standardised forms and a detailed instruction manual, pairs of reviewers independently abstracted data from each eligible study, including study and patient characteristics, and details of treatment (eg, dose, formulation and duration of cannabis add-on therapy). Our primary outcome was opioid dose. We also captured all patient-important outcomes, as guided by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials,25 including pain relief, sleep disturbance, physical and emotional functioning. Regarding adverse events, we focused on vomiting, nausea and constipation as a systematic review of values and preferences26 demonstrated that patients living with chronic pain experience gastrointestinal complaints as the most important opioid-induced adverse events. We contacted authors to obtain unpublished data.
Risk of bias assessment
Following training and calibration exercises two independent reviewers used a modified Cochrane risk of bias tool27 28 to assess the risk of bias among eligible RCTs according to the following domains: allocation concealment, blinding of participants, study personnel, outcome assessors and data analyst, and lost to follow-up (≥20% missing data were assigned high risk of bias). Response options for each item were 'definitely or probably yes' (assigned a low risk of bias) and ‘definitely or probably no’ (assigned a high risk of bias) (online supplemental table 1). We used criteria suggested by the CLARITY group29 to assess the risk of bias of observational studies including selection bias, confidence that all patients had the condition of interest, control for confounding variables, validity of outcome assessment(s), and infrequent missing data (<20%) (details available at www.evidencepartners.com/resources/methodological-resources/). (online supplemental tables 2–3).
Data analysis
We calculated inter-rater agreement regarding the eligibility of full-text studies using an adjusted kappa (κ) statistic.30 We conducted separate analyses for RCTs and observational studies. All continuous measures for pain intensity and sleep disturbance were converted to a 10 cm VAS; the minimally important difference (MID) for both was 1 cm.31 32 All continuous outcomes that were reported by more than one study were pooled to derive the weighted mean difference (WMD) and associated 95% CI. We pooled binary outcomes (adverse events) as relative risks (RRs) and risk differences (RDs) and their associated 95% CIs. We conducted all meta-analyses with random-effects models and the DerSimonian-Laird method.33
When studies reported effects on continuous outcomes as the median and IQR, we derived the mean and SD using the method presented by Wan et al.34 We also converted medians to means using the approach recommended by the Cochrane Handbook as a sensitivity analysis. When authors failed to report a measure of precision associated with mean differences, we imputed the SD from eligible studies that reported these measures (online supplemental technical appendix).35 We included each comparison reported by multiarm studies and calculated a correction factor to account for the unit of analysis error (ie, when information from a treatment arm is used more than once in the same meta-analysis).36 We explored the consistency of association between our pooled results and studies reporting the same outcome domains that were not possible to pool. We used Stata (StataCorp, Release V.15.1) for all analyses.Comparisons were two tailed using a threshold of p≤0.05.
Subgroup analyses and meta-regression
We examined heterogeneity among pooled RCTs using the I2 statistic, and through visual inspection of forest plots for pooled observational data, because statistical tests of heterogeneity can be misleading when sample sizes are large and associated confidence intervals are therefore narrow.37 When we had at least two studies in each subgroup, we explored sources of heterogeneity with five prespecified subgroup hypotheses, assuming greater benefits with: (1) shorter versus longer duration of follow-up; (2) higher versus lower risk of bias; (3) enriched versus non-enriched study design; (4) chronic non-cancer versus chronic cancer-related pain and (5) higher versus lower THC content. We assumed similar directions of subgroup effects for harms, except for study design and THC content in which we expected greater harms with non-enriched trials and higher THC content. However, apart from item two (risk of bias), studies did not report sufficient data to undertake subgroup analyses.
The certainty of the evidence
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to assess the certainty of evidence on an outcome-by-outcome basis as high, moderate, low or very low.38 With GRADE, RCTs begin as high-certainty evidence, but can be rated down because of risk of bias, imprecision, inconsistency, indirectness or publication bias. We rated down for imprecision if the 95% CI associated with a pooled continuous outcome included half the MID, or if the estimate of precision associated with the RR for binary outcomes included no effect. We considered an I2 value between 75% and 100% to represent considerable inconsistency.39 We rated down the certainty of evidence for indirectness if there were important differences between our research question and the patients enrolled, intervention tested or outcomes reported among studies contributing to our meta-analyses.40
Using GRADE, observational studies begin as low certainty evidence, and while they can be rated down further for the same reasons as RCTs, they can also be rated up in the presence of a large magnitude of the effect, a dose–response gradient or consideration of plausible confounders or other biases that increase confidence in the estimated effect.41 We only reported the pooling results of observational studies when they resulted in the same or higher certainty of evidence than evidence from RCTs. When there were at least 10 studies for meta-analysis, we explored for small-study effects by visual assessment of funnel plot asymmetry and Egger’s statistical test.42
Patients and public involvement
Patients and public were not involved in this research.
Results
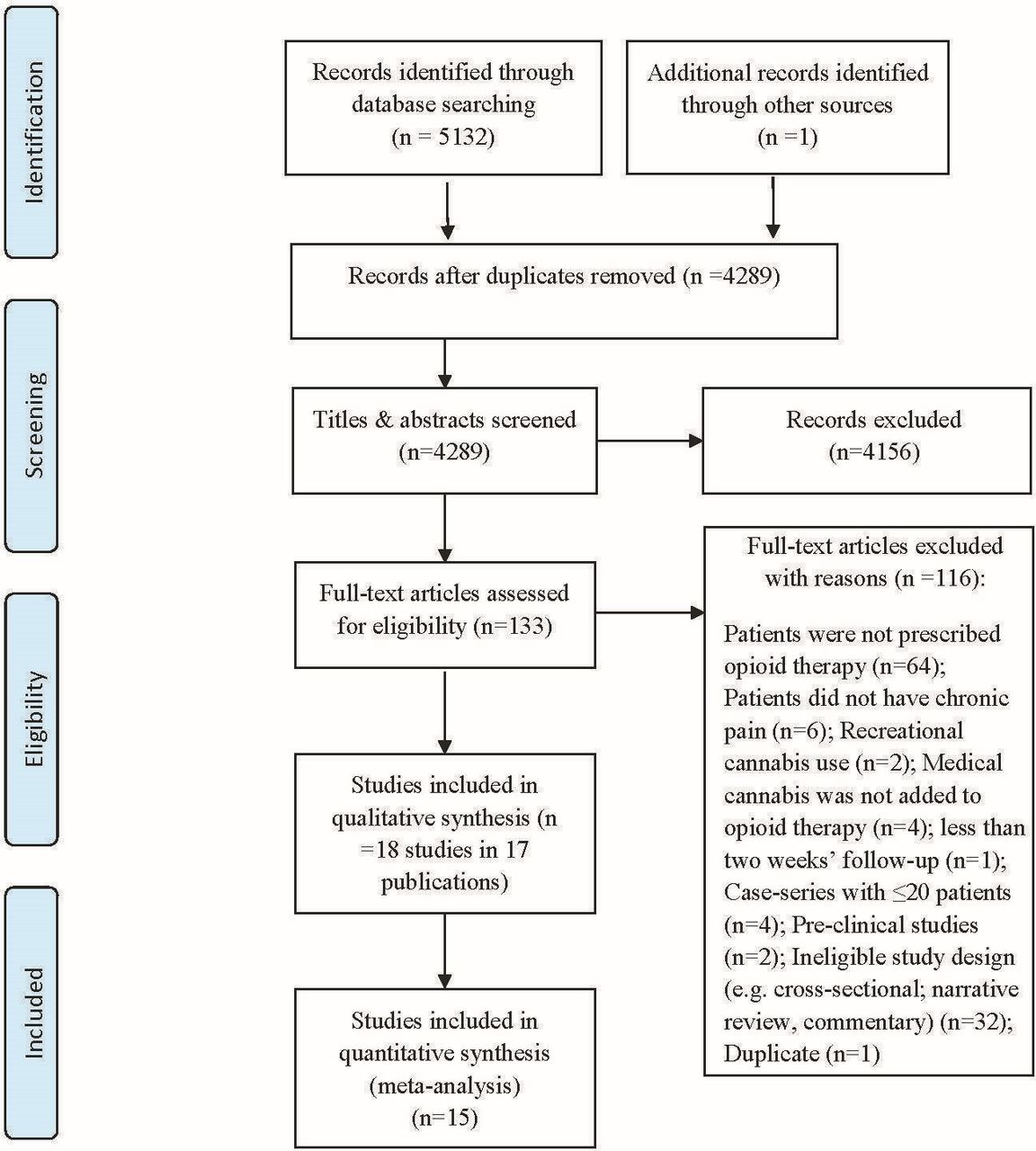
Of 5133 records identified, we reviewed 133 articles in full text, and 18 studies reported in 17 publications proved eligible (figure 1, online supplemental appendix B); five RCTs in four publications43–46 and 13 observational studies.47–59 One study enrolled a mixed group of opioid and non-opioid users50; however, our attempts to contact the authors to acquire pain intensity data for the subgroup of patients prescribed opioids proved unsuccessful. All five RCTs43–46 and three observational studies51 54 55 enrolled patients with chronic cancer-related pain; the remaining 10 observational studies explored adding cannabis to opioids for patients with chronic non-cancer pain (eg, chronic low back pain, fibromyalgia, painful chronic pancreatitis),47 52 53 57–59 or a mix of cancer and non-cancer pain (table 1).48–50 56

{kind=link}
Study selection process in review of opioid-sparing effects of cannabis in chronic pain.
Characteristics of included studies (n=18)
Among the 18 included studies, the percentage of female participants was 48% (median of individual trials 48%, IQR 43%–58%), and the median of the mean age was 56.3 (IQR 51.2–59.9). Follow-up ranged from 2 to 5 weeks among RCTs, and from 4 weeks to 6.4 years for observational studies. Only one RCT43 used an enrichment design (following the open-label phase, patients with at least 15% improvement in pain were randomised to the intervention and control groups) and all RCTs advised patients to maintain stable doses of all other prescribed pain medications, including opioids, during the study period (table 1). All included RCTs, and three of the observational studies48 51 52 administered synthetic cannabis products (ie, nabilone, dronabinol and nabiximole), five observational studies49 50 56 58 59 reported different combinations of THC:Cannabidiol (CBD) products, and six other observational studies47 53–55 57 did not provide details on the type of cannabis or cannabinoids provided (table 1, online supplemental table 4). Ten studies reported receiving industry funding,43–46 49 51 52 57 58 five studies50 53–56 reported no-industry funding and three studies47 48 59 did not report funding information (table 1).
Risk of bias of included studies
All included RCTs reported adequate allocation concealment and blinding of patients and healthcare providers; however, three trials43 45 46 were at risk of bias due to high lost to follow-up (online supplemental table 5). Each RCT specified that they employed an intention-to-treat analysis. All observational studies were at high risk of bias, typically due to lack of confidence in the assessment of exposure, non-representative samples and insufficient control for confounding (online supplemental file 6–7).
Outcomes for medical cannabis add-on therapy
Opioid dose reduction
The primary limitation of RCTs was that all investigators instructed patients to not alter their dose of opioids. This represents a very serious indirectness of the findings regarding the research question, warranting rating down two levels, and was the primary reason for very low certainty evidence from the 1176 patients.43–45 Their results raised the possibility that adding medical cannabis may not be associated with a reduction in opioid use among patients living with chronic cancer pain (WMD −3.4 milligram morphine equivalent (MME); 95% CI −12.7 to 5.9; table 2; online supplemental figure 1). There were no differences in effect based on the lost to follow-up (online supplemental figure 2); test of interaction p=0.758).
GRADE evidence profile of medical cannabis or cannabinoids for patients with chronic pain prescribed long-term opioid therapy
Very-low certainty evidence from eight observational studies (seven of which enrolled people with chronic non-cancer pain)47 48 50 51 53–55 58 raised the possibility that adding medical cannabis may reduce the use of opioids among patients with predominantly chronic non-cancer pain (WMD −22.5 MME; 95% CI −43.06 to −1.97; table 2; online supplemental figure 3). Three observational studies that could not be pooled, as they only reported opioid reduction as a percentage, also found that providing medical cannabis allowed patients to decrease their opioid dose. The first study assessed the impact of providing medical cannabis to 61 patients with chronic low back pain who were prescribed opioid therapy (median opioid dose was 21 mg MME/day) and reported that 52% of patients (32 of 61) stopped all use of opioids at a median follow-up of 6.4 years.57 The second study49 reported that of 94 patients with chronic pain (both cancer and non-cancer pain) who began using CBD hemp extract, 53% were able to decrease their use of prescription opioids at 8 weeks. A third study56 included 600 patients with chronic pain who indicated willingness to taper their opioid dose and were administered 0.5 g daily of medicinal cannabis for each 10% reduction in opioid dose. After 6 months follow-up, 55% of patients reported a 30% reduction in opioid dose on average and 26% of them discontinued opioid use.
Pain relief
High-certainty evidence from five RCTs43–46 demonstrated that adding medical cannabis to opioid therapy resulted in trivial or no difference in cancer-related pain (WMD −0.18 cm; 95% CI −0.38 to 0.02 on the 10 cm VAS for pain; MID 1 cm; table 2; online supplemental figure 4). Results did not differ depending on lost to follow-up (online supplemental figure 5, a test of interaction p=0.623). Very low certainty evidence from observational studies suggested a large decrease in pain when medical cannabis was added to opioids (online supplemental figure 6).
Sleep disturbance
Five RCTs43–46 provided high certainty evidence that adding medical cannabis to prescription opioids results in a trivial improvement in sleep disturbance in people living with cancer-related chronic pain (WMD −0.22 cm; 95% CI −0.4 to −0.06 on the 10 cm VAS for sleep disturbance; MID 1 cm; table 2; online supplemental figure 7). Results did not differ between trials reporting the low and high lost to follow-up (online supplemental figure 8, a test of interaction p=0.93). Very low certainty evidence from observational studies suggested an improvement in sleep disturbance when medical cannabis was added to opioids (online supplemental table 8).
Other reported outcomes
A single RCT44 reported moderate certainty evidence that adding cannabis likely has little or no effect on emotional and physical functioning (online supplemental tables 9–10).
Adverse events
Nausea, vomiting or constipation
Four RCTs43–46 provided moderate certainty evidence that adding medical cannabis to opioid therapy likely increases the incidence of nausea (RR 1.43, 95% CI 1.04 to 1.96; RD 4%, 95% CI 0% to 7%; online supplemental figures 9–10) and vomiting (RR 1.50; 95% CI 1.01 to 2.24; RD 3%; 95% CI 0% to 6%; online supplemental figures 11–12) in patients with cancer-related chronic pain prescribed opioid therapy. Three RCTs43 45 46 provided low certainty evidence that adding medical cannabis to opioid therapy may not increase constipation (RR 0.85, 95% CI 0.54 to 1.35; RD −1%; 95% CI −4% to 2%; online supplemental figures 13–14). Online supplemental table 11 summarises adverse events reported in observational studies.
Discussion
Very low certainty evidence from randomised trials and observational studies was conflicting and leaves uncertain whether the addition of medical cannabis affects the use of prescribed opioids among people living with chronic pain. Compared with long-term opioid therapy for chronic cancer pain without medical cannabis, high certainty evidence showed that adding medical cannabis had little or no effect on pain or sleep disturbance. Results provided moderate certainty evidence that adding cannabis therapy to opioids likely increases both nausea (RR 1.43, 95% CI 1.04 to 1.96) and vomiting (RR 1.50; 95% CI 1.01 to 2.24) and low certainty evidence suggested no effect on constipation (RR 0.85, 95% CI 0.54 to 1.35).
Strengths of our review include a comprehensive search for eligible randomised and observational studies, appraisal of the risk of bias among individual studies, and use of the GRADE approach to rate the certainty of evidence. Our review has limitations, primarily due to features of primary studies eligible for review, which failed to report all recommended outcomes that have been established as important for people living with chronic pain. Most observational studies incorporated inadequate adjustment for confounding. All randomised trials, despite reporting this outcome, were not designed to address the effect of medical cannabis on opioid use. All eligible RCTs enrolled patients with chronic cancer-related pain, and the generalisability to non-cancer chronic pain is uncertain. Specifically, substitution effects of medical cannabis for prescription opioids may also differ between chronic cancer and non-cancer pain; however, lack of variability among studies eligible for our review precluded exploration of this subgroup effect. Studies included in our review administered different formulations of cannabis and cannabinoid products; however, pooled effects of outcomes reported in RCTs showed no important heterogeneity.
A meta-analysis of preclinical studies,17 a narrative systematic review,60 and several cross-sectional and case studies have reported an apparent reduction in opioid use with addition of cannabis therapy.9 10 61–65 In a national US population-based survey66 of 2774 cannabis users (both medical and non-medical use) 36% of respondents reported substituting cannabis for prescription opioids (discontinued opioid use). In this survey, the 60% of participants who identified as medical cannabis users were much more likely to substitute cannabis for prescription drugs than recreational users (OR 4.59; 95% CI 3.87 to 5.43). Another US survey67 that included 841 patients prescribed long-term opioid therapy for chronic pain reported that 61% used medical cannabis, and 97% of this subgroup reported coincident reduction of their opioid use. Consistent with these findings, very low certainty evidence from observational studies in our review also suggests that adding medical cannabis allows patients predominantly with chronic non-cancer pain to reduce their use of opioids. Although RCT results do not support reduction in opioid dose by adding medical cannabis for opioids, the evidence is also very low certainty, primarily because investigators instructed patients to maintain their current opioid dose. This is a critical limitation, despite the 2019 National Institute for Health and Care Excellence guideline having concluded that providing medical cannabis for chronic pain does not reduce opioid use on the basis of these trials.68 Future trials should randomise chronic pain patients who voluntarily agree to engage in a trial of opioid tapering to receive medical cannabis or placebo and report all patient-important outcomes.69 Forced opioid tapering is ineffective70 and may cause harm.71
Conclusion
The opioid-sparing effects of medical cannabis for chronic pain remain uncertain. Based on moderate-to-high certainty evidence, adding medical cannabis to opioid therapy among chronic cancer pain patients had little or no effect on neither pain relief nor sleep disturbance and likely increases the risk of nausea and vomiting. The accompanying BMJ Rapid Recommendation18 provides contextualised guidance based on this evidence, as well as three other systematic reviews on benefits,72 harms73 and patients’ values and preferences.74
Data availability statement
Data are available on reasonable request to the corresponding author at: bussejw@mcmaster.ca.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JasonWBusse
Contributors JWB, AN and GHG conceived and designed the study. RJC performed the literature search. AN, AM, YS, VA and YR selected the studies, extracted the relevant information, and assessed the risk of bias of selected studies. AN synthesised the data. AN wrote the first draft of the paper. AN, JWB, GHG and TA critically revised the manuscript for important intellectual content. AN, JWB, LT, GHG, MB and DNB interpreted the findings. JWB, LT and GHG provided methodological support. All authors reviewed the paper and approved the final version. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.