Article Text

Abstract
Objective To evaluate oral anticoagulant (OAC) prescribing trends in type 2 diabetes mellitus (T2DM) in the UK from 2001 to 2015.
Design A cross-sectional drug utilisation study.
Setting Electronic health records from The Health Improvement Network primary care database in the UK.
Participants Individuals with T2DM who received a record of OAC prescription.
Outcome measures The prescribing trends of OAC medications in individuals with T2DM were examined from 2001 to 2015, stratified by age, gender and therapeutic classifications.
Results A total of 361 635 individuals with T2DM were identified, of whom 36 570 were prescribed OAC from 2001 to 2015. The prevalence of OAC prescribing increased by 50.0%, from 1781 individuals receiving OAC prescriptions (IROACP) (4.4 (95% CI 4.2 to 4.6) per 100 persons) in 2001, to 17 070 IROACP (6.6 (95% CI 6.5 to 6.7) per 100 persons) in 2015. The prevalence of warfarin prescribing decreased by 14.0%, from 1761 individuals receiving warfarin prescriptions (IRWP) (98.9 (95% CI 98.4 to 99.4) per 100 persons) in 2001, to 14 533 IRWP (85.1 (95% CI 84.6 to 85.7) per 100 persons) in 2015. This corresponded with increased prescribing of direct oral anticoagulants (DOACs), from 18 individuals receiving DOAC prescriptions (IRDOACP) (0.1 (95% CI 0.08 to 0.23) per 100 persons) in 2010, to 3016 IRDOACP (17.6 (95% CI 17.1 to 18.2) per 100 persons) in 2015, during the same period.
Conclusions Prescribing of OACs in individuals with T2DM increased from 2001 to 2015. Since the introduction of DOACs, there has been a clear shift in prescribing towards these agents. Future studies are needed to assess the safety of coadministration of OAC medications and antidiabetic therapy with T2DM.
- epidemiology
- diabetes & endocrinology
- anticoagulation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, this is the first study that examined the overall and stratified trend of oral anticoagulant (OAC) medication prescribing in individuals with type 2 diabetes mellitus over a 15-year period.
This study used a clinical record primary care research database which was representative of the UK general population.
Underestimation of OAC prescribing could be a limitation of this study as The Health Improvement Network (THIN) database only contains information from the primary care setting, and therefore it was not possible to include individuals treated in different healthcare settings (secondary, tertiary, private), and this can create gaps in the data recorded by THIN on the treatment of individuals.
Introduction
Type 2 diabetes mellitus (T2DM) is one of the most common chronic diseases worldwide and has become a major global public health concern.1 According to the International Diabetes Federation report in 2017, it was estimated that 425 million people worldwide are living with diabetes, compared with 30 million in the year 1985, of whom 90% were diagnosed with T2DM.1 In the UK, the prevalence of diabetes has doubled over the last three decades.2 3 Using a national health database in the UK, Zghebi et al4 estimated that the prevalence of diabetes increased from 3.2% in 2004 to 5.2% in 2014.
T2DM and cardiovascular diseases often coexist in many individuals with T2DM experiencing cardiovascular complications.5 6 Cardiovascular diseases, including cardiac arrhythmias, venous thromboembolism and ischaemic heart disease, are among the leading causes of mortality worldwide in individuals with T2DM.7 Anticoagulants are widely prescribed for the prevention and treatment of atrial fibrillation (AF), stroke, and venous and arterial thrombosis. When prescribed for venous thromboembolism, oral anticoagulant (OAC) treatment is typically of short duration, but it can be a lifelong treatment when prescribed for AF.8
T2DM is one of the main risk factors that contribute to CHA2DS2 score (Congestive heart failure, Hypertension, Age≥75 years, Diabetes mellitus, previous Stroke/transient ischaemic attack (TIA) (2 points)), which predicts the risk of stroke and guides optimisation of management in individuals with AF.9 In 2010, CHA2DS2-VASc (Congestive heart failure (CHF)/left ventriculardysfunction, Hypertension, Age≥75 (2 points), Diabetes, Stroke (2 points) –Vascular disease, Age 65–74 and Sex category (female)) was adapted from the previous score,10 and it is now recommended by most of the current guidelines,8 11 12 in which individuals with AF are likely to be prescribed OAC if they score 2 or more in the total score. In addition, since the introduction of direct oral anticoagulants (DOACs) in 2011, several guidelines have recommended their use for indications such as AF.8 11 12 DOACs have much more predictable pharmacokinetics and pharmacodynamics, and are less prone to drug interactions when compared with warfarin.13 However, OAC use in individuals with T2DM remains unclear, with limited studies focused on their use in individuals with T2DM.14 15
Previous studies have demonstrated that the prevalence of AF in individuals with T2DM ranges from 8% to 14.9%,16 17 and that individuals with T2DM have 40% higher risk of developing AF compared with individuals without T2DM.18 Investigating OAC use in individuals with T2DM is important due to the high number of individuals, the possibility of drug–drug interactions, and the potential association with serious adverse events such as bleeding and hypoglycaemia.19 20 This was highlighted in particular among individuals with T2DM in previous large-scale epidemiological studies and in multiple case reports where warfarin was associated with an increased risk of hypoglycaemia. It has been suggested that displaced plasma protein and cytochrome P450 hepatic metabolic pathway could be potential mechanisms for the increased risk of hypoglycaemia.21–24
Given the recent update in the guidelines for OAC prescribing and the limited research on their use in individuals with T2DM, this research aimed to describe the prescribing patterns of OAC medications in individuals with T2DM in the UK population, as an important step in investigating its safety within this high-risk population.
The primary objective of this study was to examine the prescribing trends of OAC medications in individuals with T2DM from 2001 to 2015, stratified by age, gender and therapeutic classifications. The secondary objective was to compare the trend in OAC use in individuals with AF, with and without T2DM, given that AF is the main indication for OAC use.
Methods
Data sources
This was a retrospective drug utilisation study using primary care data in The Health Improvement Network (THIN), a UK primary care database containing anonymised administrative, clinical and prescribing data from over 587 practices with more than 13 million individuals.25 26 THIN is one of the largest sources for primary care data in the UK and has been validated for epidemiological research purposes.25–27 In addition, it has been used by our team to study prescribing of OAC and various psychotropic medications.28–32 It holds data on personal information, health-related behaviours and diagnoses information, which are recorded and identified using Read codes.25 26 Read codes, which are also known as clinical terms, are clinical terminologies used to describe the care, diagnosis of diseases and treatments of individuals. It is used to manage primary care data in electronic health records.33 The database also has prescribing information that is linked with the British National Formulary. THIN contains records of prescriptions issued only by general practitioners and recorded in individuals’ records.
Study population
Data from practices that met the acceptable mortality reporting (AMR) measures of quality assurance for THIN data were used in this study. The AMR date is the year that data reporting is deemed to be complete, based on information derived from the Office for National Statistics.34 The start date was defined as the date of the first record for T2DM diagnosis. Individuals were included only if they had an observation period of at least 12 months prior to their start date and were registered with the general practice during the study period. The end date was the date were individuals left the practice, died or transferred out. Individuals with T2DM aged >18 and registered with the THIN database between 2001 and 2015 (of which data were only available up to) were identified based on the following criteria: (1) a diagnostic code for T2DM (using Read codes) or (2) a diagnostic code for any type of diabetes and a record of any oral hypoglycaemic agent prescription, and the start date for these individuals was defined as the date of the first record for diabetes. Individuals who had a diagnostic code for T2DM accounted for 92.7% of the entire cohort, while the remaining were of criteria 2. Individuals with a non-specific code for T2DM and who only had records for insulin prescription were excluded because they may have type 1 diabetes mellitus (T1DM), although their age at first event is taken into account. T2DM is typically diagnosed over the age of 30 years; however, the rate of young-onset T2DM is increasing.35 We therefore only excluded children (less than 18 years old) who were more likely to have T1DM. Individuals with T2DM receiving at least one prescription of OAC medication were identified. OAC medications were consigned into three categories: warfarin, DOACs (apixaban, rivaroxaban, dabigatran and edoxaban) and other anticoagulant medications (acenocoumarol, pentosan polysulfate and phenindione). Furthermore, individuals with AF aged >18 years and registered with THIN were identified using Read codes. The prescribing of OAC medications in individuals with AF with and without T2DM involved a two-step cohort identification (online supplementary figure S1). The first step was designed to identify individuals with AF with coexisting T2DM, and the latest first record between AF and diabetes mellitus was counted as the start date (coexistence of both diseases) for this cohort. The second step involved identifying individuals with AF without a diagnosis of T2DM, and the start date for these individuals was the first recorded AF diagnosis. Individuals who developed AF first and T2DM later contributed to the AF only cohort and then to the AF and T2DM cohort. For baseline characteristics, chronic comorbidities were measured over the 12-month period preceding the first OAC prescription. However, medication use was assessed over the 6-month period preceding the first OAC prescription.
Supplemental material
Statistical analysis
Descriptive statistics were used to describe individuals’ demographics and comorbidities. Continuous data were reported as mean±SD, and categorical data were reported as percentages (frequencies). The prevalence of OAC medications presented per 100 persons with 95% CIs was calculated on an annual basis by dividing the number of all individuals prescribed OAC medications in a particular year over the midyear population of individuals with T2DM in the same calendar year, stratified by age, gender and therapeutic classifications. For the secondary objective, the trend in OAC use in AF individuals with T2DM was calculated on an annual basis by dividing the number of AF individuals with T2DM prescribed OAC medications in a particular year over the midyear population of AF individuals with T2DM in the same calendar year. The trend in OAC use in individuals with AF and without T2DM was calculated by dividing the number of AF individuals without T2DM prescribed OAC medications in a particular year over the midyear population of AF individuals without T2DM in the same calendar year. The prescribing trend of OAC medications was assessed using Poisson model. All analyses were performed using SAS V.9.4.
The research was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement (online supplementary table S1).
Supplemental material
Patient and public involvement
We used anonymised administrative data, and it was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Demographics and characteristics
During the study period of 2001 and 2015, a total of 361 635 individuals with T2DM were identified, of whom 36 570 received a prescription for OAC. The characteristics of the entire cohort included in our study are presented at the time of first OAC prescription. The average age of individuals at the time of first OAC prescription was 72 (SD, 10.2) years old, and the majority of individuals were male (59.9%). Around 64.6% of individuals were diagnosed with AF and 22.2% were diagnosed with venous thromboembolism diseases. The baseline demographics of the study sample are described in table 1.
Characteristics of the study sample at the time of first OAC prescription
Trends in prescribing prevalence of OAC medications in T2DM
Between 2001 and 2015, the prescribing prevalence of OACs in individuals with T2DM increased by 50.0%, from 1781 individuals receiving OAC prescriptions (IROACP) (4.4 (95% CI 4.2 to 4.6) per 100 persons) in 2001, to 17 070 IROACP (6.6 (95% CI 6.5 to 6.7) per 100 persons) in 2015 (p<0.001), with an average increase of 3.2% per year (figure 1).

Prescribing prevalence of OAC medications in individuals with T2DM stratified by gender. OAC, oral anticoagulant; T2DM, type 2 diabetes mellitus.
The changes in prevalence of OAC prescribing between 2001 and 2015 stratified by gender are shown in figure 1. The prescribing prevalence of OAC medications among men increased by 54.3%, from 4.6 (95% CI 4.3 to 4.9) to 7.1 (95% CI 6.9 to 7.2) per 100 persons with T2DM, while the prescribing prevalence of OAC medications among women increased from 4.0 (95% CI 3.8 to 4.4) to 5.9 (95% CI 5.8 to 6.1) per 100 persons with T2DM, with an overall increase of 47.5%.
Similarly, the prescribing prevalence of OAC medications varied among individuals from the different age groups. The prevalence of OAC medications among individuals aged 75 years or above increased from 7.1 (95% CI 6.6 to 7.6) in 2001 to 11.6 (95% CI 11.4 to 11.9) in 2015 per 100 persons with T2DM. However, it was clearly lower among younger individuals, which increased from 5.7 (95% CI 5.2 to 6.1) in 2001 to 6.5 (95% CI 6.3 to 6.6) in 2015 per 100 persons with T2DM for individuals aged between 65 and 74 years, and from 2.0 (95% CI 1.8 to 2.2) in 2001 to 2.2 (95% CI 2.1 to 2.3) in 2015 per 100 persons with T2DM for individuals aged below 65 years (figure 2).

Prescribing prevalence of OAC medications in individuals with T2DM stratified by age. OAC, oral anticoagulant; T2DM, type 2 diabetes mellitus.
Trends in prevalence of OAC prescribing stratified by medication
Although warfarin was the most common OAC prescribed during the entire study period (86.3%), its use declined by 14.0%, from 1761 individuals receiving warfarin prescriptions (IRWP) (98.9 (95% CI 98.4 to 99.4) per 100 persons) in 2001, to 14 533 IRWP (85.1 (95% CI 84.6 to 85.7) per 100 persons) in 2015. In contrast, there was a corresponding increase in the proportion of individuals who used DOACs, from 18 individuals receiving DOAC prescriptions (IRDOACP) (0.1 (95% CI 0.08 to 0.23) per 100 persons) in 2010, to 3016 IRDOACP (17.6 (95% CI 17.1 to 18.2) per 100 persons) in 2015. Other OACs, including acenocoumarol and phenindione, were less likely to be prescribed during the entire study period (0.03%); their prescribing rate decreased from 1.1 (95% CI 0.7 to 1.7) in 2001 to 0.4 (95% CI 0.3 to 0.5) in 2015 per 100 persons with T2DM (figure 3). In addition, a small percentage of individuals with T2DM using OAC were prescribed different OAC classes during the same year, ranging from less than 1% in 2010 to 3% in 2015.
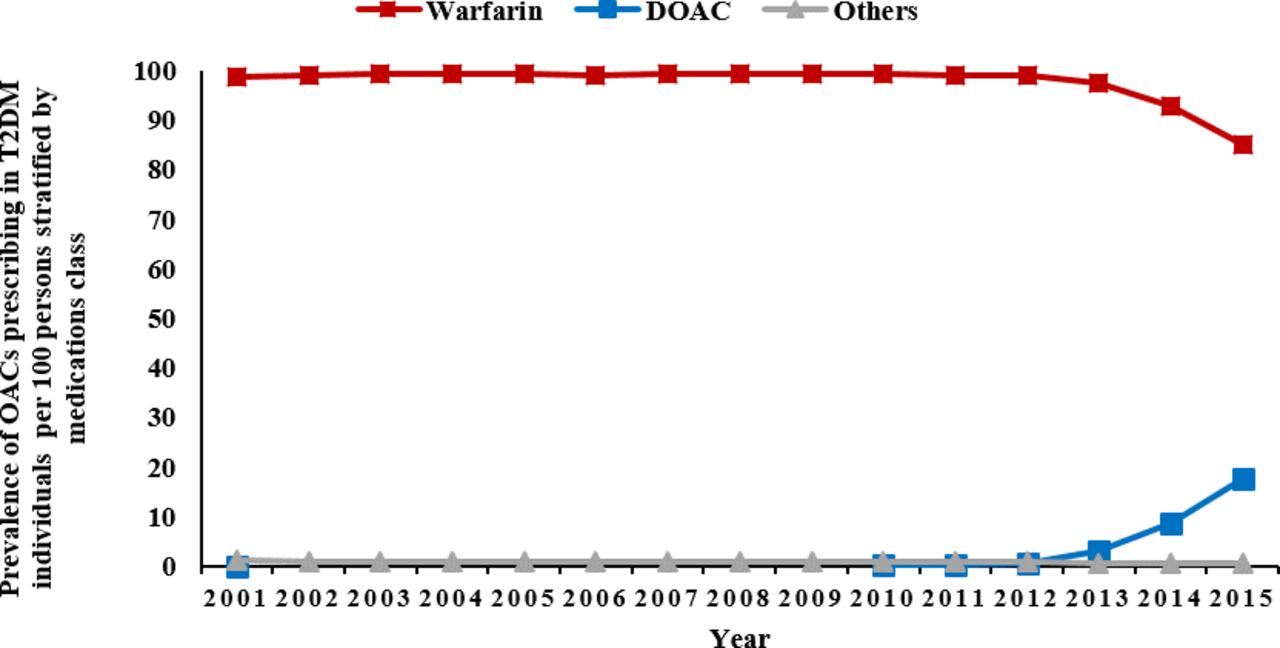
Prescribing prevalence of OAC medications in individuals with T2DM stratified by medication class. DOAC, direct oral anticoagulants; OAC, oral anticoagulant; T2DM, type 2 diabetes mellitus.
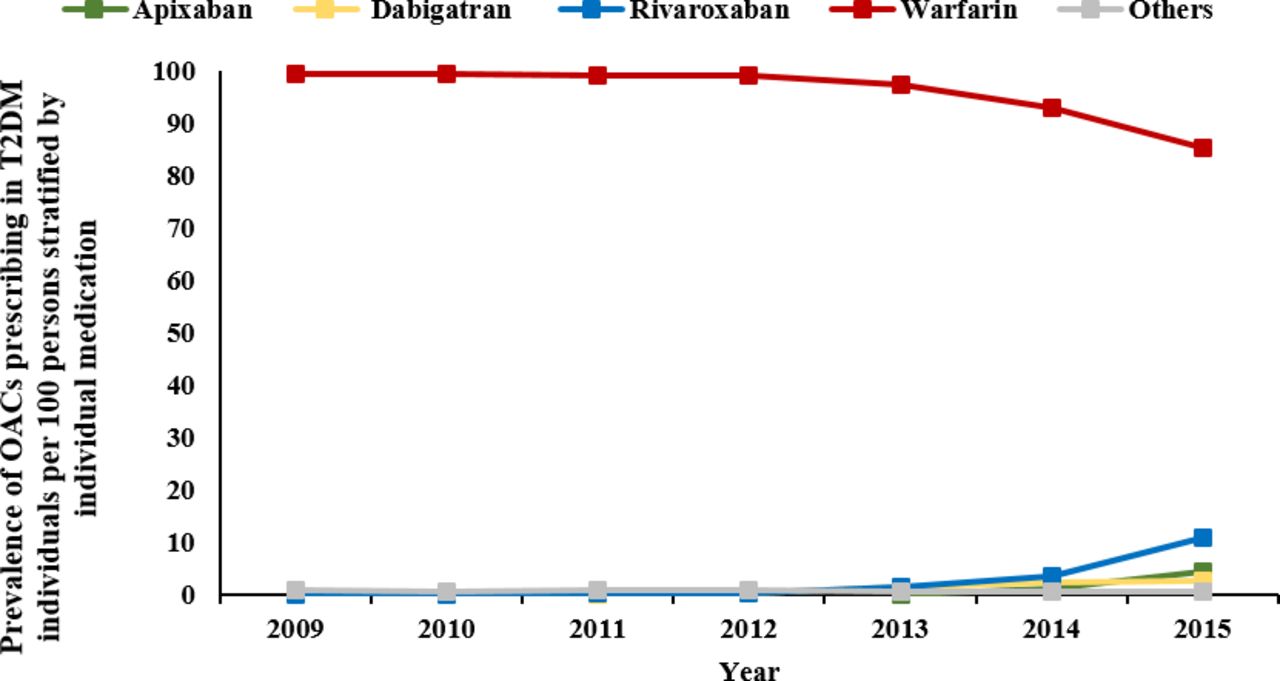
Further stratification by individual OAC drug treatment showed that the prescribing prevalence of rivaroxaban markedly increased, from 0.1 (95% CI 0.05 to 0.2) in 2010 to 10.9 (95% CI 10.5 to 11.4) in 2015 per 100 persons with T2DM, while the prescribing prevalence of dabigatran increased to a lesser degree, from 0.03 (95% CI 0.001 to 0.07) in 2010 to 2.7 (95% CI 2.5 to 2.9) in 2015 per 100 persons with T2DM. In addition, the prescribing prevalence of apixaban increased from 0.05 (95% CI 0.01 to 0.08) in 2010 to 4.36 (95% CI 4.1 to 4.6) in 2015 per 100 persons with T2DM (figure 4).

Prescribing prevalence of OAC medications in individuals with T2DM stratified by individual medication. OAC, oral anticoagulant; T2DM, type 2 diabetes mellitus.
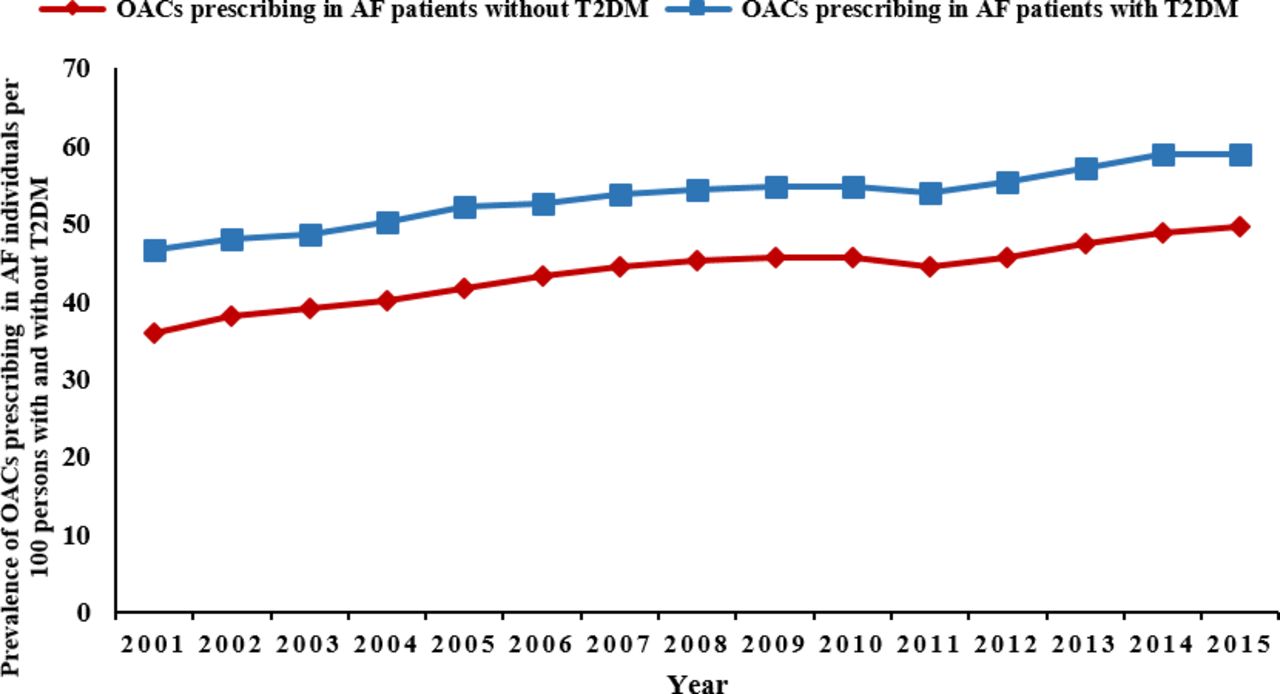
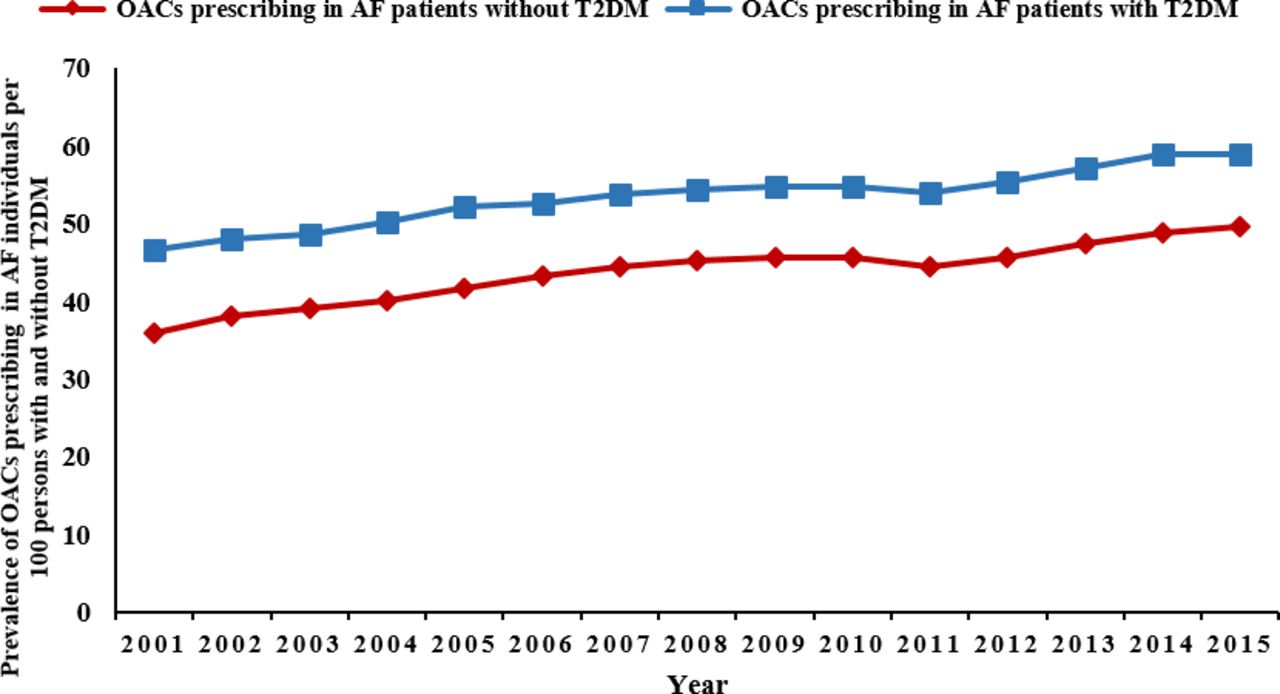
Trends in prescribing prevalence of OACs in AF individuals with and without T2DM
The prescribing prevalence of OACs in AF individuals with and without coexisting T2DM maintained a parallel increase. Individuals with AF and T2DM had a higher rate of OAC medications prescribing compared with those without T2DM (38.2% vs 26.4%, respectively). The prevalence of prescribing ranged from 46.6 (95% CI 43.5 to 49.7) in 2001 to 59.0 (95% CI 58.3 to 60.0) in 2015 per 100 persons for individuals with AF and T2DM, and from 36.0 (95% CI 35.1 to 36.7) to 49.7 (95% CI 49.4 to 50.0) per 100 persons between 2001 and 2015 for individuals with AF without T2DM (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prescribing prevalence of OAC medications in individuals with AF with and without T2DM. AF, atrial fibrillation; OAC, oral anticoagulant; T2DM, type 2 diabetes mellitus.
Discussion
This study investigated the drug utilisation pattern of OAC medications in individuals with T2DM, and in individuals with AF with and without T2DM. The following are the key findings: (1) The prescribing prevalence of OACs in individuals with T2DM has increased markedly between 2001 and 2015. (2) The increase in the prescribing prevalence of OACs was not consistent across individuals of different genders and age groups; men and individuals aged 75 years and above had a higher prescribing prevalence compared with women and individuals younger than 75 years. (3) The prescribing of DOACs is clearly replacing the prescribing of warfarin since their introduction to the UK market in 2011.
Previous studies investigating the trend of OAC prescribing in individuals with T2DM are limited. A previous study by Hamada and Gulliford.15 examined the trend of cardiovascular medication prescribing in individuals with diabetes aged 80 years or above in the UK between 1990 and 2010 concluding that the prescribing of OACs in individuals with T2DM had increased from 5% in 1999 to 19% in 2010. These results showed similar trends to our study in the increase of OAC prescriptions in T2DM. However, our results showed that OAC prescriptions increased less sharply, which is explicable by restriction of their population to include only individuals aged 80 years and older. Despite this, age is considered a risk factor for many conditions for which OACs are indicated, and our results showed an increased rate of OAC prescribing among individuals aged 75 years and above, which was also similar to a previous study that used primary care data in the UK.36 Furthermore, an increasing prescribing prevalence of DOACs in the last few years has been reported in several studies that examined the trend of OACs in the general population or in individuals with AF across different countries.36–38 Alalwan et al,37 using data from MarketScan Medicare, reported that DOACs increased from 1.39% (95% CI 1.34% to 1.44%) in 2010 to 28.33% (95% CI 28.14% to 28.52%) in 2014. Similarly, Loo et al36 found that the rate of initiation of DOAC increased significantly, particularly from 2012 onwards, with a 17-fold increase from 2012 to 2015 (relative risk (RR) 17.68; 95% CI 12.16 to 25.71). The findings presented in our study, and specifically related to DOACs’ prescribing trend, are in line with previous findings; however, it is important to highlight that those studies concerned the general population and were not specific to T2DM.36–38
This study showed that since the introduction of DOACs, individuals with T2DM using OACs were prescribed different classes of OAC, possibly due to individuals switching from one class to another. DOACs have been reported to be non-inferior to warfarin in the prevention of major strokes and embolic events in different clinical trials and observational studies.39–43 Evidence from meta-analyses showing better efficacy and non-inferior safety when comparing DOACs and warfarin could be a reason for the paradigm shift in favouring the prescribing of DOACs.44 45 This led to a change in the UK National Institute for Health and Care Excellence (NICE) guidance for the management of AF,8 and as of 2014 DOACs have been recommended as first-line therapy for AF.46 However, it is crucial to recognise that older people with comorbidities were excluded or under-represented in the pivotal clinical trials of DOACs, and therefore DOACs should be prescribed with caution and there should be strict monitoring in this population.47 Another major issue with warfarin is that it is more prone to several drug–food and drug–drug interactions,20–22 48 which could explain why DOACs are being prescribed more favourably in the recent years compared with warfarin, especially accounting for elements such as ageing and polypharmacy. Nonetheless, a major advantage of DOACs is their wider therapeutic index and that they do not require regular monitoring during intake for international normalised ratio compared with warfarin.49–51
The results of this study highlighted that individuals with T2DM receiving OACs have a high-risk profile of cardiovascular comorbidities including hypertension, coronary heart disease, heart failure, peripheral vascular diseases and hyperlipidaemia (table 1), where it could be associated with the initiation of OAC prescribing.14 However, due to the nature of this descriptive study, it is difficult to draw this conclusion and we urge for further studies to investigate this association.
As expected, our results showed that AF was the main indication for OAC prescriptions among individuals with T2DM. Several international guidelines, including those from the USA,52 Europe11 and the UK,8 have recommended the use of OACs in individuals with AF based on CHADS29 and CHA2DS2-VASc score.10 This was also in line with our results, which showed that individuals with AF and coexisting T2DM had a higher rate of OAC prescribing compared with AF individuals without T2DM. However, our results showed a higher prescribing rate of OAC among men compared with women, which is similar to other studies that highlighted the higher prevalence of OAC prescribing among men.53 54
Strengths and limitations
To the best of our knowledge, this is the first study that examined the overall and stratified trend of OAC medication prescribing in individuals with T2DM over a 15-year period. This study used a clinical record primary care research database which was representative of the UK general population.
However, this study has some limitations. First, OAC prescribing may be underestimated as THIN database only contains information from the primary care setting, and therefore it was not possible to include individuals treated in different healthcare settings (secondary, tertiary, private), and this can create gaps in the data recorded by THIN on the treatment of individuals. However, the UK National Health Service heavily subsidises the treatment of chronic illness, and the majority of individuals with chronic illness are looked after by primary care; therefore, our results should not be affected significantly. Second, individuals were identified using relevant Read code lists and algorithms. Codes were selected with reference to clinicians’ comments and previously published studies. However, as described in the Methods section, there is a possibility of misclassification in identifying individuals with T2DM. This may have led to overestimation of T2DM diagnoses in the study; however, it is also important to mention that individuals who had a diagnostic code for T2DM contributed to over 92% of the study cohort. Therefore, it is reasonable to assume that this did not have a major impact on our findings. THIN is a medical record database and therefore similar to other clinical databases. It was not possible to confirm if individuals were adherent. Furthermore, in the secondary objective of this study, we did not adjust for CHA2DS2-VASc in the comparison between the trend in OAC use in AF individuals with and without T2DM. However, CHA2DS2-VASc was introduced in 201010 and was only implemented in the NICE guidelines in 20148; considering that our study end date was 2015, the practice will not be reflected in our study period.
Future studies are warranted to investigate the safety of the concurrent use of antidiabetic medications and OAC medications for possible drug–drug interactions, especially when warfarin is the drug of choice. However, with DOACs being relatively new to the market and rapidly replacing warfarin, it is imperative to investigate the effect of concomitant use of this class of medication and the risk of hypoglycaemia or bleeding. This will identify medications that are associated with higher risk, and thus improve the safety of OAC use in individuals with T2DM.
Conclusions
This study highlights a clear change in prescribing pattern towards DOAC use compared with warfarin since its introduction to the UK market, which is consistent with the UK guidelines. However, there is a lack of studies examining their safety when used in individuals with T2DM. Further studies are warranted to investigate the safety of the concurrent use of antidiabetic and OAC medications for possible drug–drug interactions.
Acknowledgments
The authors thank Lisa Lam for her contribution in preparing the publication of this manuscript.
References
Footnotes
Twitter @KennethKCMan
Contributors HA, LW and ICKW had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. HA, LW and ICKW contributed to the study design. HA, LW, KKCM and PM contributed to the statistical analysis. HA, LW and ICKW were involved in the interpretation of data. HA wrote the first draft of the article. HA, LW, AYN, JSB, JI, GT, GF and ICKW made substantial contributions to the drafts, reviewed the manuscript for important intellectual content and provided final approval of the version to be published. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding JSB, LW, ICKW, GF and JI received PharmAlliance project grant to conduct collaborative research between UCL, Monash and UNC. HA's PhD project was supported by a scholarship from the Saudi Arabian Ministry of Higher Education.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The present study is based on anonymised and unidentifiable THIN data; thus, the need for informed consent was waived by the THIN scientific review committee (SRC). This study was reviewed and scientific approval was obtained by THIN SRC in 2018 (18THIN009).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.