Article Text

Abstract
Objective To quantify general practitioners’ (GPs) sensitivity to anxiety disorders (ADs) when confronted with the range of symptoms common to children with ADs. Also, to explore GPs’ conscious preferences and implicit tendencies for referral of children with ADs to mental healthcare.
Design and setting In a cross-sectional vignette-based survey, all attendees of a Dutch continuing medical education conference for primary care physicians were presented with subtitled audio fragments of five vignettes that we constructed to mimic symptom presentation of children with ADs in general practice. We asked attendees to select per vignette the most plausible diagnoses and most adequate referral option, and for their general referral preferences when they suspect each of the most common mental health problems.
Participants A sample of 229 GPs, resulting in a total of 1128 vignette evaluations.
Main outcome measure GPs’ selection rate of ADs in the five vignettes compared with a benchmark provided by mental health professionals (MHPs).
Results Overall, recognition of ADs was less likely in GPs compared with MHPs (OR=0.26, 95% CI 0.15 to 0.46). GPs varied in their recognition of anxiety, with 44.1% not once selecting anxiety as the probable presenting problem. When asked explicitly, 63.9% of the GPs reported that they would refer a child to mental healthcare when they suspect probable ADs. By contrast, only 12.0% of the GPs who recognised anxiety in the vignettes actually selected that referral option.
Conclusion A significant fraction of GPs did not notice the depicted symptoms as anxiety. Despite the widespread prevalence of ADs, GPs seem to overlook anxiety already in their early diagnostic opinion. Improving GPs’ familiarity with initial symptom presentation, ADs’ base-rate, relevance and impact yields potential for timely recognition.
- primary care
- mental health
- anxiety disorders
- psychiatry
- child & adolescent psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study relating general practitioners’ (GPs) interpretation of the broad range of presenting problems in daily practice to the timely recognition of anxiety disorders in children.
The vignette-based design enabled exclusion of putative external effects of the complex clinical reality, and the presentation of the vignettes through subtitled audio fragments the isolation of GPs’ sensitivity to pick up on the signs of anxiety.
While the verbal presentation of five vignettes to every participant in the same order was substantial to investigate overall recognition, the results are only exploratory on the level of the individual vignettes and various symptoms.
The predefined response options limited access to GPs’ considerations; mixed-methods studies might enhance in-depth understanding of their interpretations and decision-making process.
Introduction
Unnoticed anxiety disorders (ADs) have an important impact on human development and well-being. Only one in ten children with ADs, including those with subthreshold levels of severity, will be free of any mental health problem later in life.1–7 With estimated prevalence rates of up to one in four, ADs are the most common mental health issue over the lifespan.8–10 Fortunately, treatment helps to mitigate risks and adversities.11–14 Based on their gate-keeper role, approachability and their continuous care relationship with families, general practitioners (GPs) are in a unique position to recognise ADs characterised by an early age of onset, a chronic or relapsing-remitting course, somatic manifestations and comorbidities.15–20 Although around 70% of children and adolescents consult their GP more than twice a year,21–24 studies in primary healthcare indicate that over two-thirds of children with ADs go unnoticed.25–28
Recognition is especially problematic in early onset, less severe and less explicit disorders.28–31 Interestingly, those factors are inherent to anxiety, including the covert nature of its core symptoms, its gradual development, fluctuating course and the wide variety of accompanying symptoms that are not prototypic for anxiety.3 ADs are tied to problems as temper tantrums, control neediness, withdrawn behaviour, difficulties in connecting with others, poor concentration and physical complaints.32 Each of these indicators are seemingly unrelated and may not equally impact a child’s situation, increasing the chances that professionals fail to appreciate them as a relevant or important sign. These symptoms also mimic and co-occur with other mental health disorders and contextual problems. Parents and teachers show differences in recognition of various symptoms and tend to underdetect or misattribute some more than the others.33–36
Given the limited time available to understand and act on the breadth of disclosed problems, a GP’s first interpretation of the presented problems might be pivotal in successfully navigating a consultation and recognising anxiety in children. The decision-making literature highlights the importance of the first diagnostic opinion and suggests that amendments after this point are often insufficient (‘anchoring bias’).37 However, studies that relate recognition to the variety of symptoms are scarce, and to our knowledge, no study has investigated in how far physicians even consider anxiety as the probable factor underlying the reason of consult. To address this, we presented GPs with mixed-anxiety vignettes. That is, vignettes that capture the variety and indefinite nature of early symptom presentation in general practice and do not solely describe specific mental health disorders as demarcated in psychiatric nosologies. Notwithstanding that we created the vignettes to suggest a probable AD, we hypothesised that GPs would not proportionately cite anxiety as the underlying cause of the presented symptoms. In addition to the question how GPs would interpret and refer the described cases, we also asked how they generally tend to manage cases when they suspect specific mental health problems in practice. Based on literature suggesting that ADs might be evaluated as relatively benign,38 we hypothesised that GPs would be less likely to report that they refer children with suspected anxiety to mental healthcare (MHC) than children with suspected developmental, behavioural or mood problems.
Methods
Setting and design
The study was conducted during the yearly 2-day continuing medical education conference ‘Boerhaave Progress and Practice’39 for primary healthcare physicians (Leiden, The Netherlands, 14 December 2018). Each year, a range of somatic and mental health topics are covered by specialists within 25 min time slots. During one of those slots, we presented the survey supported by PowerPoint slides that additionally carried embedded subtitled audio fragments of the vignettes (60–64 s each). A total of 275 GPs were registered. Attendees were seated with a device that digitally recorded their anonymous responses. As such, data collection was not subject to Dutch law governing medical research involving human subjects, nor to European law on general data protection and privacy.
Procedure and measurement
Attendees were introduced with (1) that they would hear five case descriptions of children with psychosocial problems in the form of a report resulting from a few consultations, and would see three recurring questions that reflect their daily reality concerning what the condition might be and what could be done about it. (2) They were asked to base their considerations on the available information only. We aimed to use gender-neutral names for the vignettes to prevent that gender confounds decision-making. In an independent coding of 25 gender-neutral names by six coders, at most three names were labelled by half of the coders as gender-neutral. Given this low agreement and taking into account discrepancies in literature on gender differences and recognition,29 36 we mentioned (3) that the named cases were intentionally gender-neutral. Attendees were also informed (4) that by responding they voluntarily and anonymously agreed to analysis of their responses for scientific purposes. Preceding the first vignette, the recurring questions were verbally introduced and shown (table 1). Thereafter, the questions were shown sequentially, each with a progress bar displaying the response time set to a maximum of 10s.
Survey items as shown and verbally introduced
Vignette development
In order to quantify to what extend GPs consider anxiety in their early diagnostic opinion, we constructed vignettes that capture various symptoms (online supplementary file A). Guided by knowledge of the clinical presentation of ADs and the prevalence of common mental health disorders, we had decided to build five vignettes around the combined presentation of anxiety with, respectively, physical complaints, difficult behaviour, mood, developmental and school attendance problems. On the level of the key aspect mixed-anxiety, each vignette represented symptoms related mostly to one of these domains while also depicting symptoms of anxiety that do not overlap with these mental health problems.
Supplemental material
To theoretically support the process, we first consulted clinical handbooks and questionnaires.40–42 Relevant symptom expressions and idioms were obtained from actual clinical referral letters written by GPs of children and adolescents diagnosed in specialised MHC. This linked text-data enabled working back and forth from children’s complaints mentioned by their GPs and their descriptive diagnoses, and hence facilitated a controlled development of vignettes that are also natural. The extracted descriptions were grouped into the five domains and an initial set of 11 vignettes (as advised)43 was formed. In an iterative process five vignettes were selected, further refined and for readability purposes named as V1-Somatic, V2-Behavioural, V3-Mood, V4-Developmental, V5-School Attendance. In each vignette, more cues were given for anxiety compared with any other specific disorder group (eg, in V2-Behavioural vignette, we counted the total number of cues as 13, with eight cues that could be related to anxiety, five to behavioural problems, three to attention-hyperactivity and trauma, two to somatic and one to autism). To mimic actual consultations, the vignettes also included contextual factors43 such as academic or home functioning or background information about the GP–child relationship. Case age and vignette length had a limited range (10–12 years, 165–172 words) to avoid possible confounding effects.43
During the final stage of vignette development, GPs affiliated with Leiden University Medical Centre were invited to participate in an individual pilot interview (six interviews held in November 2018). GPs were asked to think aloud and provide verbal feedback while reading the transcript of each vignette and answering the identification and referral questions. We also asked GPs about the realism of the vignettes: they responded positively and felt that the descriptions corresponded to their practice. The pilot led to minor changes, most concerning the ‘contextual aspects’,43 for example, initially we alternated mothers and fathers as the parent who went along to the consultation. Several GPs evaluated this as odd, hence we changed it to ‘mother’.
Validation of vignettes
To validate the recognisability of anxiety, 24 MHPs were invited to participate in a pilot presentation, of whom 11, all with extensive clinical experience (median 15–19 years), agreed to participate. All MHPs were employed at Curium-LUMC, a university-affiliated inpatient and outpatient psychiatric clinic for children and adolescents. We surveyed MHPs using the same procedure as in the GP-survey, with the exception of written responses and two additional questions regarding their psychiatric specialisation. The presentation resulted in 55 answers concerning the first identification question, and 53 answers on the second identification question. In line with our aim to develop mixed-anxiety vignettes, MHPs selected different disorder groups: anxiety (n=22), mood (n=19), attention-hyperactivity (n=14), behavioural (n=12) and somatic (n=10) problems were selected frequently, and typical development was not selected (online supplementary file A). Anxiety was the most or second most frequently selected disorder group in V1-Somatic, V2-Behavioural and V4-Developmental, and the third most frequently selected in V3-Mood and V5-School Attendance.
Outcome definition and analysis
Recognition rate was defined as the ratio of the total number of times anxiety was selected and the total number of times anxiety could have been selected. GPs’ and MHPs’ recognition was compared following Newcombe’s method 1044 using the Epi package45 in the R-statistics environment. This method tests for independence as in the χ2 test, yet provides a robust method to estimate CIs. GPs’ selection rate of the different disorder categories and the referral indications they made for the vignettes were analysed using descriptive statistics. Whether the likelihood of an MHC referral was lower when anxiety was recognised in a vignette was tested in a logistic multilevel regression using the lme4 package.46 That GPs would report an MHC referral for ADs less often compared with referral for behavioural, developmental and mood problems was also tested in a logistic multilevel regression, with disorder groups (anxiety vs behaviour, development and mood problems) as the repeated measures. Respondents with missing responses on more than half of the survey were excluded from all analyses. Data were visualised using the ggplot2 package.47
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Results
Participants
A total of 299 attendees answered at least one survey question. Of these, 239 reported being a GP. Data from 10 GPs were excluded due to missing responses. As a missing response on both identification questions of a vignette occurred 17 times, the number of times anxiety could have been selected was 1128 (229*5–17).
The distribution of the sample’s gender and years of experience was similar to the national population48 (table 2).
These demographics showed no association with the number of times anxiety was recognised, the referral indications GPs made for each vignette, or with their reported referral preferences for ADs (online supplementary file B).
Demographics of the study sample and the national population
Recognition
By selecting 167 times anxiety in the 1128 possibilities to opt for a specific disorder group, GPs reached a recognition rate of 14.8%. GPs were less likely to recognise anxiety compared with MHPs (OR=0.26, 95% CI 0.15 to 0.46, figure 1). Whereas 55.9% (n=128) of the GPs labelled one or more vignette as anxiety-related, over two-fifths did not in any. On average, GPs often selected behavioural, mood, developmental and trauma-related problems, and typical development (table 3). GPs and MHPs did not differ in their selection rate of these disorder groups (online supplementary file B).

The upper figure depicts MHPs’ and GPs’ recognition rate of anxiety. MHPs selected anxiety in nine of their 55 responses on the first identification question and in 13 of their 53 responses on the second identification question. GPs selected anxiety in 84 of their 1060 responses on the first identification question and in 83 of their 1067 responses on the second identification question. Differences between the two groups were statistically significant overall (OR=0.26, 95% CI 0.15 to 0.46), in the first identification question (OR=0.44, 95% CI 0.21 to 0.93), and in the second identification question (OR=0.26, 95% CI 0.13 to 0.50). The lower figure depicts the percentage of GPs and MHPs that recognised anxiety in none, one, two, three, four or all five vignettes. The difference between GPs’ and MHPs’ recognition frequency was statistically significant, χ2(5, 240)=42.94, p<0.001. GPs, general practitioners; MHPs, mental health professionals.
GPs’ selection rate of each disorder category
Exploration of recognition per vignette revealed a major difference between GPs and MHPs for V1-Somatic (GPs: 5.7%, MHPs: 54.5%). Differences were not statistically significant for V2-Behavioural (GPs: 33.8%, MHPs: 45.5%), and for V3-Mood (GPs: 13.7%, MHPs: 18.2%). GPs recognised anxiety significantly less often than MHPs in V4-Developmental (GPs: 9.0%, MHPs: 36.4%) and in V5-School Attendance (GPs: 11.9%, MHPs: 45.5%).
Referral
When asked how they would refer a child with a similar profile to the vignettes, the majority responded that they would keep the child in general practice (practice nurse=40%, figure 2). GPs who indicated that they would refer most often chose primary healthcare (local youth teams=24%, primary MHC=13%). The vignette which most often triggered referral to MHC was V3-Mood.
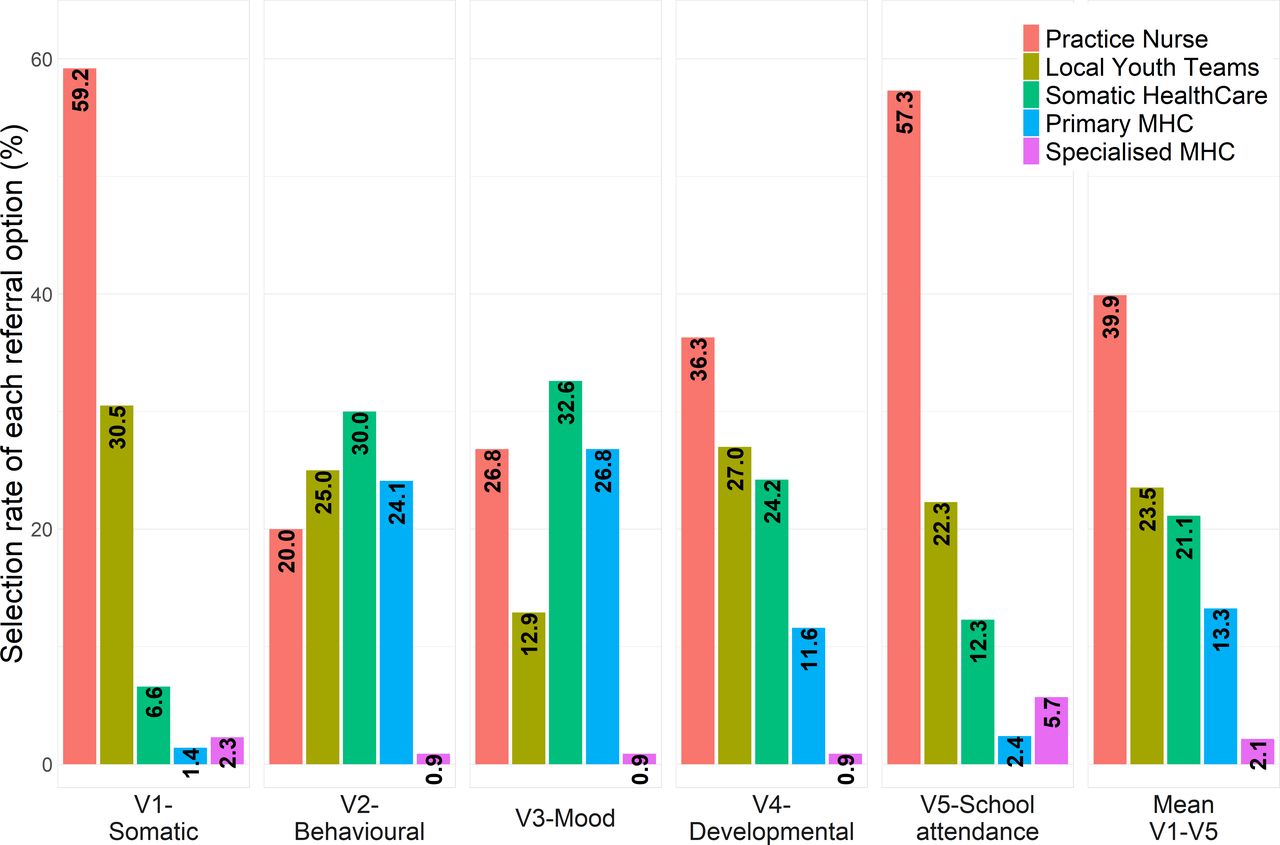
GPs’ referral decisions following each of the five vignettes. Sample size was as follows in V1-Somatic=213, V2-Behavioral=220, V3-Mood=224, V4-Developmental=215, V5-School Attendance=211. GPs, general practitioners; MHPs, mental health professionals.
Those GPs who recognised anxiety reported referral of a child to MHC slightly less often compared with those who did not recognise anxiety (table 1, online supplementary file B). However, multilevel analysis revealed that the likelihood of a referral to MHC was not significantly related to the recognition of anxiety (OR=0.70, 95% CI 0.42 to 1.18) (table 4).
Referral to mental healthcare by those GPs who recognised anxiety and those who did not
When asked about their general referral preferences, a majority reported a tendency to refer children with suspected ADs to primary MHC (figure 3). More GPs reported treatment of suspected anxiety in MHC (OR=1.79, 95% CI 1.35 to 2.37) compared with suspected developmental, behavioural or mood problems (OR=0.53, 95% CI 0.39 to 0.72). Analysis per disorder group revealed that GPs’ reported referral preferences for anxiety, did not differ from their preferences for mood problems. A referral to MHC was reported less often for difficult behaviour, problems related to autism, attention-hyperactivity and (psycho-)somatic problems and more often for eating problems and trauma (online supplementary file B).

{kind=link}
{kind=link}
{kind=link}
GPs’ reported referral preferences for each of the eight disorder groups. Excluding cases with missing responses left the following sample sizes: anxiety n=224, trauma n=217, mood n=220, somatic n=212, eating problems n=219, autism n=213, attention-hyperactivity n=214, difficult behaviour n=216. GPs, general practitioners; MHC, mental health care.
Discussion
To investigate GPs’ sensitivity towards ADs, we presented vignettes describing the mixture of problems that might be disclosed during consultations. GPs noticed anxiety sufficiently in the vignette that depicted a prototypic sign (‘fears’) but infrequently when the depicted symptoms were less explicit. Possible alternative mental health problems were recognised also by MHPs who helped to validate the vignettes but they differed from GPs only in their better recognition of anxiety. Whether a GP indicated a referral to MHC for a given vignette showed no significant association with recognition of anxiety in that vignette. MHC was selected by GPs as the appropriate referral option in less than one-fifth of these vignettes depicting problems of mild severity. Interestingly, when asked about their general referral preferences for children with suspected ADs, over two-thirds of the GPs reported a preference for intervention in MHC.
Strengths and limitations of the study
To the best of our knowledge, this is the first study to investigate GPs’ interpretations of the various problems typical in children with ADs. We surveyed a large sample but we do not have insight into the representativeness of the attending GPs. Nevertheless, the years of experience and gender distribution of the sample were similar to the national GP population, these demographics did not show an association with the outcome measures.32 Also, literature is inconclusive in whether GPs’ attitudes influence decision-making.30 31 The presentation of the vignettes to all participants at once yielded a risk of carryover effects. It also incited a game aspect that may have decreased observer effects and improved access to participants’ honest and direct considerations.43 A limitation is the small number of MHPs and the multiple statistical comparisons made between GPs and MHPs. Notwithstanding the explorative nature of the study on the level of the individual vignettes, we applied conservative Bonferroni corrections to avoid false positives. MHPs selected anxiety infrequently in the mixed anxiety-depression vignette. This low recognition rate might be a consequence of similar number of cues for anxiety (8) and depression (7) in this vignette, the large conceptual overlap between anxiety and depression and that MHPs might also be more attuned towards depression.49 GPs could not indicate watchful waiting for the vignettes in this study overestimating the likelihood that GPs take any action when presented with children similar to the vignettes. In conversations with GPs. we had found that in case of any ambiguity they would make the rational decision for further enquiry. Given our aim to gain insight in their tendencies, we decided to prevent selection of this safe option. Nevertheless, it is unlikely that addition of this option would change the results considering referral to MHC. Those who would have selected watchful waiting now probably selected the practice nurse. A related caveat is the interpretation of the findings as representing recognition and referral in everyday practice. Decision-making in general practice is shaped by a complex interplay of multiple individual and systemic factors over time. With this novel approach, we aimed to isolate the extent to which GPs mind anxiety in their early diagnostic opinion. In this regard, a major strength of the study was the use of actual patient medical records to create the vignettes. This enabled wording similar to that of GPs, improving the construct and external validity of the case descriptions and diminishing uncontrollable variability.50
Comparison with other studies
Overall recognition of anxiety was within the lower range of what is found in literature (9%–60%).27 28 51 This might be a consequence of the mild severity portrayed in the vignettes, a factor limiting recognition of all disorder groups.32 This design, however, does not explain why GPs selected the other mental health problems yet failed to recognise anxiety proportionately. In V1-Somatic depicting a consultation for recurring earaches, for example, GPs picked up on the probability of behavioural, somatic or autism spectrum-related problems. They were also sensitive to whether typical development was depicted. Nonetheless, the portrayal should have also raised the prospect of an AD, a possibility that was recognised by very few GPs. GPs recognised anxiety sufficiently in one vignette. This being the vignette that literally mentioned the core feature of anxiety (‘fears’) supports that unfamiliarity with symptom presentation might be the driving factor behind the low recognition rates.
The recognition rate was realised by just over half of GPs. Others did not select anxiety in any vignette. A question is what underlies these individual differences. Previous studies also found no association of recognition with gender or experience of the professional, and literature is not one-sided about the role of attitude.31 Observations we made during the pilot with six GPs suggest that differences might be caused by how they ‘perceive, read and interpret’37 presenting symptoms. For instance, all GPs commented about the word ‘temperamental’, yet many neglected ‘timid’ although both words were in the same sentence. GPs also varied in the problem areas they gave attention to. Most GPs expressed a focus on school and home burden (eg, ‘School is a benchmark for me and that is going well. If it wasn’t alarm bells would be going off’). By contrast, many did not reveal a need to enquire further with children themselves or about leisure activities and social relations. If a GP tends to piece out some symptom-profiles and neglect others based on context,52 53 this might be of particular consequence for the recognition of ADs characterised by a covert and less disruptive profile.
An important finding concerned the final vignette which portrayed a child with social AD. In response to this vignette, GPs frequently selected typical development and the mildest referral options. Although a similar response pattern was obtained for the first vignette, both the vignette developers and MHPs evaluated the final vignette as a more severe case description. This finding is in line with studies suggesting low recognition of social anxiety.29 35 54 Recognition of social anxiety by professionals is of particular importance since these patients are known to under-report symptoms, and since diagnosis-specific interventions are advised in clinical guidelines.55
Contrary to hypothesis, GPs did not prove less likely to prefer intervention in MHC for ADs compared with problems related to difficult behaviour, developmental disorders or depression. Results of this normative part of the study contrasts with clinical studies demonstrating that a substantial proportion of children with ADs are unlikely to be referred to MHC.25 30 56 This disparity with clinical practice might be related to factors other than GPs’ conscious evaluations, such as strain on parents and their treatment desires that differ between disorders.57 Another explanation might be a discrepancy in GPs conscious evaluations on the one hand, and their skills and implicit decision-making tendencies on the other hand. Our data support this explanation to some extent, although to our knowledge, no previous study examined the evaluations and implicit tendencies GPs hold towards treatment of children with ADs. We found a discrepancy in GPs’ responses in that the majority of the GPs reported to consider a referral when they suspect ADs, but generally chose management in primary healthcare rather than referral to MHC in the vignettes. This comparison of reported referral preferences to the referral indications made for the vignettes might be invalid if GPs assumed a higher severity when asked about referral preferences versus the mild severity depicted in the vignettes. However, in both, we emphasised that the survey considers probable mental health problems, including subthreshold levels of severity. The variations in GPs’ answers between disorder groups supports that they understood the question as it was meant. Also, GPs were inclined to refer the vignette scenario with symptoms that overlapped with mood problems to MHC, in agreement with their reported normal practice. This leaves open whether their threshold to evaluate anxiety as an AD differs from when they consider mood problems as depression,54 yet supports our hypothesis that differences in the likelihood of a referral may depend on symptom presentation. Notably, during the individual pilot interviews, we observed a focus on symptoms related to depression ‘because you would not want to leave it untreated’ and varying heuristics GPs used when evaluating the relevance of symptoms.
Meaning of the study
Moving beyond sensitivity as the endpoint of diagnostic accuracy, the results suggest that the repeatedly found underrecognition of anxiety goes back to the initial considerations GPs make. Our findings confirm the conjecture that recognition of ADs is often confounded by their overlap with other common and well-known mental health problems and similarity with typical developmental variations.26 However, this finding per se does not distinguish between the alternate possibilities that GPs prioritise other disorder groups or lack sufficient knowledge of the presentation and prevalence of child anxiety. In fact, it has been suggested that there might be a prioritisation issue given the seemingly low burden and impact of ADs.38 In the current study, the presentation of the vignettes using subtitled audio fragments precluded the possibility of rereading and elaborate evaluation. By verbally presenting vignettes that do not indicate a distinctive mental health disorder, we aimed to circumvent knowledge of diagnostic criteria and the question of a primary or differential diagnosis. The study results therefore imply that, even before rational prioritisation, there could be a significant bottleneck in first interpretation that might have otherwise led to early recognition. Anxiety might not resonate sufficiently as the likely problem when GPs encounter children with ADs. Leaving aside the discussion of whether it is a GP’s task to assess the specifics of a child’s mental health problem, we argue that it is worthwhile to improve knowledge of early symptom presentation in children with problems that are relatively poorly recognised by parents and teachers. GPs face the difficult task to recognise mental health problems in a limited amount of consult time, yet report difficulties with the use of structured assessment methods in clinical practice.58 To avail the benefits of their unguided decision-making, it is necessary that they become more attuned and aware of the prevalence, the breadth and relevance of typical signs of anxiety. Understanding how professionals comprehend and act on presenting symptoms is important, even more so in light of the high base-rate of ADs,8 their early age of onset (11 years)18 and risk of persistence into adulthood.1–3 The finding that majority of the GPs reported to prefer an MHC referral indicates that they do acknowledge anxiety as a treatment demanding problem, and leaves opportunity for targeted improvements.
Unanswered questions and future research
Why did some GPs recognise anxiety in multiple vignettes whereas others did not? Another open question concerns how GPs would have responded had the referral option ‘no action needed’ been available for the vignettes. Causal inferences as regards symptom presentation and subsequent recognition and referral could be made if the many symptoms associated with ADs could be systematically varied using a factorial vignette design.43 If combined with qualitative methods, future studies could further enhance our understanding of the decision-making process.
Acknowledgments
We gratefully acknowledge the organisers and participants of the 14 December 2018 Boerhaave Symposium, the participants of the 27 November 2018 validation meeting with mental health professionals at Curium-LUMC Leiden, Umut Can Yildiz for his technical advices in embedding the vignette transcripts as subtitles into the audio fragments, and Dr Elise Dusseldorp for her advices regarding the multilevel analyses.
References
Footnotes
Contributors SA analysed clinical referral letters of children, created the vignette drafts and drafted the manuscript. MC, PMW, BMS and MEN provided feedback to the vignette drafts during the iterative vignette development process. MC, MW and BMS contributed to the interpretation of the data. SA, MC, BMS, RRJV, MEN and PMW designed the study, critically revised and gave final approval for the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. No additional data are available for this study in repositories. Inquiries concerning the data may be made to the corresponding author.