Article Text

Abstract
Objective Whether care group participation by general practitioners improves delivery of diabetes care is unknown. Using ‘monitoring of biomedical and lifestyle target indicators as recommended by professional guidelines’ as an operationalisation for quality of care, we explored whether (1) in new practices monitoring as recommended improved a year after initial care group participation (aim 1); (2) new practices and experienced practices differed regarding monitoring (aim 2).
Design Observational, real-life cohort study.
Setting Primary care registry data from Eerstelijns Zorggroep Haaglanden (ELZHA) care group.
Participants Aim 1: From six new practices (n=538 people with diabetes) that joined care group ELZHA in January 2014, two practices (n=211 people) were excluded because of missing baseline data; four practices (n=182 people) were included. Aim 2: From all six new practices (n=538 people), 295 individuals were included. From 145 experienced practices (n=21 465 people), 13 744 individuals were included.
Exposure Care group participation includes support by staff nurses on protocolised diabetes care implementation and availability of a system providing individual monitoring information. ‘Monitoring as recommended’ represented minimally one annual registration of each biomedical (HbA1c, systolic blood pressure, low-density lipoprotein) and lifestyle-related target indicator (body mass index, smoking behaviour, physical exercise).
Primary outcome measures Aim 1: In new practices, odds of people being monitored as recommended in 2014 were compared with baseline (2013). Aim 2: Odds of monitoring as recommended in new and experienced practices in 2014 were compared.
Results Aim 1: After 1-year care group participation, odds of being monitored as recommended increased threefold (OR 3.00, 95% CI 1.84 to 4.88, p<0.001). Aim 2: Compared with new practices, no significant differences in the odds of monitoring as recommended were found in experienced practices (OR 1.21, 95% CI 0.18 to 8.37, p=0.844).
Conclusions We observed a sharp increase concerning biomedical and lifestyle monitoring as recommended after 1-year care group participation, and subsequently no significant difference between new and experienced practices—indicating that providing diabetes care within a collective approach rapidly improves registration of care.
- general diabetes
- protocols & guidelines
- quality in health care
- primary care
- organisation of health services
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- general diabetes
- protocols & guidelines
- quality in health care
- primary care
- organisation of health services
Strengths and limitations of this study
Due to the observational real-life design of this study, interference with daily routines of general practitioner (GP) practices was avoided, thus contributing to reliability and representativeness of our findings
Because the outcome measure ‘monitoring as re-commended’ is rooted in current professional GP guidelines and is associated with significant better HbA1c outcomes, our results are valuable for clinical practice
Considering that for the first analysis, two practices missing baseline data had to be excluded—which might reflect at most limited registration of target indicators—the associations we found in the first analysis might be underestimated.
Although the diabetes protocol is targeted to structural and enduring care for adult people of any age, monitoring recommendations are determined for people younger than 80 years—in accordance with these recommendations, people younger than 80 years were included in our study.
Since people participating less than a year and people older than 80 years or without registration of age were excluded, the generalisability of our findings is limited to people registered within this age range and being exposed minimally 1 year to the care protocol.
Introduction
In the last decades, the worldwide prevalence of type 2 diabetes has increased rapidly.1 This trend is also reported in the Netherlands where, in 2016, approximately 1.1 million people (constituting 6.4% of the entire population) had a diagnosis of type 2 diabetes.2 Although health systems may vary on a local level, organisational challenges regarding the implementation of effective diabetes care are internationally frequently reported. A recent review identified several barriers to the delivery of diabetes primary care in general practice, including a heavy workload, time pressure and lack of information technology (IT).3 In addition, general practitioners (GPs) and nurse practitioners have difficulty in keeping up to date with diabetes-related knowledge and skills.
To strengthen primary diabetes care, internationally, several programmes have been initiated, in which GP practices, generally supported by payment structures, restructure the delivery of diabetes care. For example, in the UK, the Diabetes Integrated Care Initiative has been launched,4 aiming to integrate primary, secondary and community diabetes care. In the USA, the Comprehensive Primary Care (CPC) and, successively, the CPC+ programme have been introduced. The CPC and CPC+ provide practices with a robust learning system, including actionable data feedback to guide their decision-making.5 Since it is widely known that adequate monitoring of diabetes-related health outcomes is tremendously important to reduce the risk of diabetes complications6–8 both CPC and CPC+ support monitoring of people with type 2 diabetes through health technology data.
In the Netherlands, a national primary care diabetes programme was introduced in 2007. To facilitate the implementation of this programme in terms of logistic support and quality control, various Dutch GPs joined together in local ‘care group’ collectives. These care groups provide a multidisciplinary care approach in which GP practices collaborate with allied health disciplines such as dieticians, podotherapists and optometrists.9
Because the use of a computerised clinical decision support system (CCDSS) is associated with improvements in the monitoring of diabetes-related health outcomes,10 many care groups provide a CCDSS. In addition to a CCDSS, care groups offer continuing professional development training and other IT facilities. Moreover, care groups negotiate with local healthcare insurance companies about integrated reimbursements and annual care targets regarding the proportion of individuals with type 2 diabetes having at least one measure of biomedical indicators, such as haemoglobin A1c (HbA1c), systolic blood pressure and low-density lipoprotein (LDL) profile. At the end of each year, the GP practices get feedback on the adequacy of monitoring, which may result in tariff adjustment. In addition, during the individual practice coaching and professional development trainings, GP practices are systematically encouraged to pay sufficient attention to lifestyle-related factors.
According to professional GP guidelines in the Netherlands,11 HbA1c, systolic blood pressure, LDL cholesterol profile and lifestyle factors such as body mass index (BMI), smoking behaviour and physical exercise can be considered ‘diabetes target indicators’. These guidelines recommend to frequently monitor people with type 2 diabetes on these indicators, that is, at least once each year.
Previous studies showed that structured primary diabetes care and systematic monitoring of diabetes target indicators are associated with improved diabetes-related health outcomes, including HbA1c levels,12 13 which in turn affects the risk of fatal and non-fatal myocardial infarctions.14 Thus, monitoring of diabetes target indicators might be perceived as a measure of quality of diabetes care. However, little is known about the effects of providing protocolised primary diabetes care within a care group setting on the monitoring of individuals. Therefore, we aimed to explore whether providing protocolised primary diabetes care within a care group is associated with an increase in recommended monitoring of biomedical and lifestyle-related target indicators in individuals after 1 year (aim 1). In addition, we aimed to evaluate the impact of GP practices’ experience with providing protocolised primary diabetes care (aim 2) by comparing recommended monitoring of people with type 2 diabetes in GP practices participating in the care group since 1 year with GP practices that participated in a care group for at least 3 years.
Methods
Study design and population
In this observational Eerstelijns Zorggroep Haaglanden (ELZHA) real-life Dutch cohort study, based on primary care registry data from 2013 to 2015, the monitoring of diabetes target indicators in individuals with type 2 diabetes was analysed. Data were obtained from Hadoks, formerly known as ELZHA, a care group collective in the western part of the Netherlands. In 2015, the care group numbered 168 practices, of whom six had been participating since 2014, and 146 had been participating for at least 3 years (since 2012). In February 2017, after pseudonymisation of the individual data, all GP practices were invited to participate in the present study based on an opt-out procedure.
Inclusion and exclusion of participating practices and people
For the first aim, all six GP practices that joined the collective in 2014 (‘new’ practices) were selected. GP practices were excluded if baseline data were missing, that is, data of people related to calendar year 2013. People who were registered with type 2 diabetes in January 2014 and who had received within the care group approach continuously primary diabetes care during the previous 12 months were included in this study. Because Dutch national GP guidelines concerning the monitoring of systolic blood pressure and LDL are specifically defined for people aged younger than 80 years, all individuals aged ≥80 years were—in accordance with these guidelines—excluded. In addition, individuals’ missing data on essential characteristics for any diabetes treatment—age, gender and duration of time since the diagnosis of diabetes—were excluded.
For our second aim, new practices were compared with practices that had participated in the care group for at least 3 years (‘experienced’ practices). Practices which were taken over or left the care group between 2013 and 2015 were excluded. In both groups of practices, individuals were included in January 2015 if they were aged younger than 80 years and if they had received care group-supported diabetes care for at least 12 months.
Intervention
The care group approach is characterised by three cornerstones with regard to implementation of structured care in clinical practice: (1) Intensive support to GPs and nurse practitioners by specialised staff nurses with regard to implementation and delivery of structured diabetes care. All GP practices are frequently visited and coached by specialised staff nurses. These visits aim to give GP practices tailored feedback on the monitoring and health outcomes of individuals with diabetes, and to support GPs with the implementation and organisation of the primary diabetes care programme. (2) Availability of a CCDSS to improve oversight of the diabetes population and recent monitoring outcomes. Since January 2013, a CCDSS has been used to monitor and improve the care process and outcomes. Based on the diabetes-related electronic GP information system, this system presents an overview of all individuals with diabetes, including the history of their diabetes registrations each quarter. As a result, the CCDSS provides GPs with up-to-date insight into the monitoring of people with diabetes, which makes it easier to manage this monitoring. (3) A programme of vocational courses for GPs and nurse practitioners to keep diabetes-related skills and knowledge up to date. The care group offers GPs and nurse practitioners each year mandatory courses on diabetes to keep their knowledge and skills up to date. Thus, from care group perspective, the aim is to realise tailored counselling and education for staff people, fitting their needs and preferences. Furthermore, to join the care group, presence of a nurse practitioner in the practice team is necessary. For individuals with diabetes, the approach consists of a quarterly invitation to consult their GP practice, in which diabetes-related blood indicators are checked and lifestyle education is provided, combined with allied healthcare such as an annual foot examination, fundus screening and dietician’s counselling.
Outcomes
Registration of the six diabetes target indicators (HbA1c, systolic blood pressure, LDL profile, BMI, smoking behaviour and physical exercise) was measured at the end of each quarter. In correspondence with the GP guidelines,11 monitoring targets were based on proportions of people with minimal one registration of each indicator during the calendar year. For the present study, people were regarded ‘being monitored as recommended’ when there was at least one registration for each of the six target indicators in the previous calendar year on 1 January of the subsequent year. If one or more target indicators were not registered in this time frame, people were defined as ‘not being monitored as recommended’.
Analysis
For the baseline characteristics, categorical variables were reported as numbers and percentages. Continuous variables which were non-normally distributed were reported as medians with IQRs. In addition, for all measurement moments, the sum of the registered indicators was determined.
For the first aim, the recommended monitoring of people in the calendar year 2013 (baseline measure) was compared with the calendar year 2014 (follow-up measure). To investigate the second aim, the recommended monitoring in new practices was compared with experienced practices in the calendar year 2014. For both aims, multilevel logistic analyses were conducted, which allowed to adjust the individual observations (level 1) for variation at the level of GP practice (level 2). In addition, both analyses were adjusted for age, duration of diabetes and gender, which are relevant confounders regarding diabetes monitoring.15–19
Descriptive statistics were analysed using SPSS V.24.0. Multilevel analyses were performed using MLwiN (V.2.28; Centre for Multilevel Modelling, University of Bristol, UK).
Patient and public involvement
Since this study was targeted on a GP supporting approach of structured primary diabetes care, patients were not actively involved.
Ethical considerations
Based on an opt-out procedure, informed consent was obtained from the GP practices. Since the pseudonymised individual data only contained age and gender, the data could easily be aggregated without enabling investigators to reduce them to individual persons. Also, taking into account the large number of people, individual informed consent was not required. The study protocol was approved by the Medical Ethical Committee of the Leiden University Medical Center (code G16.102).
Results
Regarding our first aim, since none of the six new practices objected to participation in this study, all practices were included. Because baseline data from 2013 were missing in two practices, data of four practices were used (n=327 individuals). In these latter practices, 182 individuals met the inclusion criteria (figure 1).

Flow chart of the practices (individuals) in the first analysis.
Regarding our second aim, out of the 146 experienced practices, 145 did not object to participate in this study (n=21 465 individuals) and were thus included. Concerning the study population, respectively 295 individuals in the six new practices and 13 744 individuals in the experienced practices fulfilled the study criteria (figure 2).

Flow chart of the practices (individuals) in the second analysis.
Aim 1: association between care group participation and recommended monitoring of people
Baseline characteristics are presented in table 1. In the new practices that joined the care group collective in January 2014, at baseline the percentage of people being monitored as recommended was 25% (n=45). The total number of registered indicators at baseline and at follow-up is presented in figure 3. The unadjusted analysis showed that after 1-year care group participation, the proportion of people being monitored as recommended increased to 51% (n=93) with an unadjusted OR of 3.18 (95% CI 2.04 to 4.96) compared with baseline (table 2). Adjustment for duration of diabetes, age and gender resulted in a similar association (OR 3.00, 95% CI 1.84 to 4.88). A detailed overview of the adjusted model is presented in online supplementary appendix 1.
Supplemental material
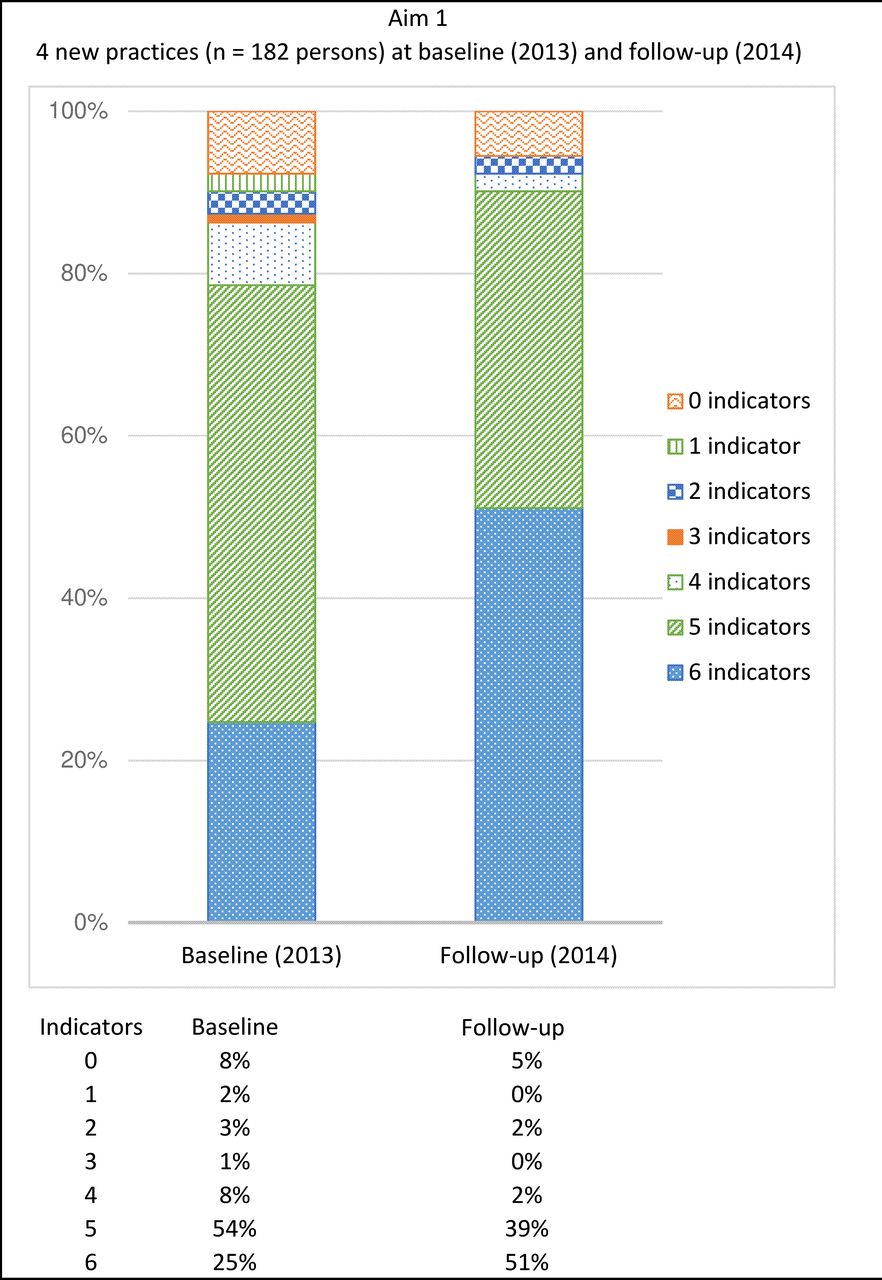
Overview of registered type 2 diabetes mellitus indicators for aim 1.
Characteristics of individuals in the first and second analyses
Overview of difference in monitoring as recommended (aim 1 and aim 2)
Aim 2: association between care group experience and recommended monitoring of people
Table 1 presents the characteristics of individuals in the new and experienced practices; the two groups were comparable regarding duration of diabetes, age and gender. The proportion of people being monitored as recommended was 62% (n=8563) in the experienced group versus 61% (n=180) in the new group. In the unadjusted analysis (table 2), experienced practices showed no significant difference from new practices in people being monitored as recommended (OR 1.06, 95% CI 0.83 to 1.34; p=0.65). Multilevel analysis adjusting for practice level and additionally for age, duration of diabetes and gender revealed similar findings (OR 1.21, 95% CI 0.18 to 8.37; p=0.844). A detailed overview of the adjusted model is presented in online supplementary appendix 2. For both groups, the sum of registered indicators is presented in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overview of registered type 2 diabetes mellitus indicators for aim 2.
Discussion
This study explored whether offering protocolised primary diabetes care in a care group is related to improvement of people with type 2 diabetes being monitored as recommended. We found that after 1 year of collectively organised and facilitated primary diabetes care, monitoring of people in line with GP recommendations increased substantially. In addition, we found in experienced practices, participating at least 3 years in the care group, no significant differences in recommended monitoring as compared with new practices, participating for 1 year. These findings indicate that participating in a care group has a rapid and enduring effect on the quality of monitoring of people with type 2 diabetes.
To our knowledge, this is the first study in Europe to explore the relationship between care group participation and registration concerning monitoring of essential biomedical and lifestyle diabetes indicators. As demonstrated by previous work,12 appropriate registration of diabetes monitoring is associated with significantly better HbA1c levels. Similarly, a meta-analysis established that appropriate self-monitoring of blood glucose was associated with better HbA1c levels.20 Thus, in our view, adequate monitoring is clinically relevant. Our findings underpin the outcomes of a longitudinal evaluation regarding the first Dutch initiative on collectively supported implementation and delivery of structured primary diabetes care. This study revealed a trend reflecting improved measure of indicators such as systolic blood pressure and LDL.21 In addition, our results support the conclusions of previous annual national benchmarks which were based on aggregated data of care groups between 2011 and 201322 and which suggested that monitoring of people in line with professional GP guidelines has improved. Furthermore, our findings are confirmed by a British evaluation of GP support by diabetologists and nurse specialist concerning diabetes care, which showed that the number of appropriate referrals to secondary care increased significantly.23 In the USA, the CPC initiative has key characteristics in common with the Dutch care group approach. Our findings show a greater increase in monitoring than found in the evaluation of the first year CPC24–26 which detected only small improvements in monitoring. This difference might be explained by the recent introduction of the CPC programme, since an in-depth evaluation of US practices participating in the CPC programme revealed that practice staff appreciated advice adjusted to their job roles and practice organisation, and the electronic health record system and other digital systems used in their practice27—indicating that a quality transition had been initiated. In addition, an evaluation of the first year of the Dutch care group approach reported much room for improvement of individual monitoring, hardly any significant improvement of diabetes-related health outcomes and missing data due to registration problems28; also, in an evaluation of the second and third years, only modest improvements in monitoring were found.29 In other words, the better outcomes of our study might be explained by a broader experience with the care group approach.
In our view, one important strength of this study is the design. In general, a randomised clinical trial (RCT) might be useful to eliminate bias. However, in RCTs achieving adequate powering is a common problem. In contrast, observational studies generally allow inclusion of large-scale study populations. To illustrate, in the case of our study, meeting the powered study population within an RCT design would have been severely hindered by logistical barriers. That is, finding sufficient practices that were willing to be assigned to a randomisation procedure concerning care group participation or a control condition would virtually have been impossible. This problem can be avoided with an observational design. Thus, when using an observational design in this field, barriers with regard to the external generalisability of the findings might be alleviated.30 In addition, since our design typically does not interfere with the daily organisation of GP practices, adequate reliability of our findings can be assumed. Moreover, in our study, the observational real-life setting reflects the reality of diabetes monitoring in this specific study population. The design we used is in line with other studies that also used a pragmatic design to conduct diabetes-related studies in primary care.31–35
Nevertheless, some limitations warrant discussion. First of all, our findings are only generalisable to people younger than 80 years participating minimally 1 year in the care protocol. Second, the number of new practices was relatively low, which might have influenced our findings on the effect of care group participation. For example, two new practices lacked baseline data, indicating weak registration of diabetes monitoring, and were thus excluded for our first research analysis; in addition, in the new practices, a considerable number of people were excluded because of missing information on essential personal data (age, gender and diabetes duration). Missing data are a common challenge when using routine registry data.36 This implies that our results on the effect of care group participation are primarily applicable to people with registration of elementary diabetes-related information. Second, since no control group could be included, we cannot proof a causal relation between the observed increase in the monitoring of people and participation in a care group. In addition, it should be noted that given the observational design, our findings might be affected by residual confounding. Third, concerning the second analysis, different groups that varied in size were compared. Therefore, our findings might have been influenced by other factors (eg, size and organisation of the GP practice, or characteristics of the practice population) even though we did correct our analyses for the level of GP practice and additionally for age, duration of diabetes and gender of the individuals.
Our study shows that providing protocolised primary diabetes care in a care group context is associated with a rapid increase in monitoring of individuals with type 2 diabetes. This might be explained by the three cornerstones of the care group support. First, in the context of a high workload and competing priorities in daily GP practice,3 the support provided to GPs and nurse practitioners with regard to implementation and delivery of a diabetes care protocol might encourage essential organisational changes in individual practices. This is supported by a Canadian study showing that in the view of GPs, supporting access of GPs to other health professionals in primary care such as nurse practitioners facilitates interprofessional collaboration and improves diabetes care.37 To illustrate, although the collaboration process between GPs and nurse practitioners in daily practice is sometimes perceived as challenging,29 within care groups, different stakeholder groups report clarity about one another’s expertise, roles and tasks.38 Accordingly, process coaching by an experienced staff nurse might ameliorate the functioning of the GP team and subsequently care delivery. More effective functioning of the GP team and improved care delivery might result in development of a team-based approach to realise timely invitation of people for diabetes consultations at ward or a team-based approach to reduce no shows.
Second, effective use of a CCDSS enables systematic and appropriate monitoring of diabetes-related health outcomes. Because the accessibility of IT systems is known to be a barrier in primary diabetes care,3 39 appropriate coaching concerning the use of these systems is required.40 Care group-related support with regard to the use of a CCDSS stimulates up-to-date oversight of individual monitoring, thus contributing to a higher number of people being monitored as recommended. Third, the mandatory educational diabetes courses enable GPs and nurse practitioners to keep their knowledge and skills up to date. As a result, optimal benefits from the collective approach might be derived.
In other words, the care group approach tackles several internationally reported barriers on the delivery of diabetes care and thus contributed to improvement of care quality. Therefore, the benefits of collectively organised logistic and quality support might also be relevant for other protocolised diabetes care settings, such as the CPC+ programme in the USA.
From the perspective of individuals with type 2 diabetes, quarterly consultation in a care group setting, which is characterised by systematic and ongoing attention for diabetes-related self-management and lifestyle support, is associated with an increase in being monitored as recommended, although for certain subgroups of people, a more flexible ‘care protocol’ might be sufficient.41
For future research, further examination of factors that might affect relations between care group participation and outcomes within participating practices—such as local geographical and socioeconomic characteristics or practice organisation—is needed to gain a better understanding of the association between care group participation and monitoring of people. To add, previous studies have shown that structured primary diabetes care and structured monitoring of diabetes target indicators are associated with improved diabetes-related health outcomes, including HbA1c,12 13 which in turn affects the risk of fatal and non-fatal myocardial infarctions.14 42 However, more detailed exploration of the relationship between monitoring of individual diabetes indicators in line with professional recommendations, diabetes-related changes in treatment and health outcomes (eg, meeting treatment targets, cardiovascular complications, hospital admissions) might enhance our understanding of adequate, collectively supported primary diabetes care. Next, evaluating the financial costs and benefits of this diabetes care approach might be interesting for policymakers. Finally, although we found that protocolised primary diabetes care with collective support is associated with better monitoring, little is known about the personal perspective of the individuals themselves with regard to participation in a structured care protocol.
To summarise, in practices that started with protocolised primary diabetes care within a care group setting, the monitoring of people as recommended increased considerably after 1 year. In experienced practices, the odds of being monitored in line with professional guidelines did not significantly differ from new practices participating 1 year in the care group. Thus, collectively organised logistic and quality support of GP practices is associated with improvement of primary diabetes care monitoring. The association between care group participation and diabetes health outcomes needs further research. More insights into the personal perspective of the stakeholders (GPs, nurse practitioners and individuals with diabetes) are recommended.
Acknowledgments
The authors thank the general practitioners and individuals with type 2 diabetes of Hadoks, formerly known as the ELZHA care group, for the use of their data for this study.
References
Footnotes
Twitter @tbonten, @@NHChavannes, @@MattijsNumans
Contributors SvB analysed data and wrote the manuscript. SR analysed data and reviewed the manuscript. TNB reviewed the manuscript. NC reviewed the manuscript and contributed to the discussion. MEN is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. MJK reviewed and edited the manuscript and contributed to the discussion.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Medical Ethical Committee of the Leiden University Medical Center (code G16.102).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request to the corresponding author.