Article Text

Abstract
Objectives To investigate the complications and survival of elderly patients with end-stage renal disease (ESRD) who received urgent-start peritoneal dialysis (USPD) or urgent-start haemodialysis (USHD), and to explore the value of peritoneal dialysis (PD) as the emergent dialysis method for elderly patients with ESRD.
Design Retrospective cohort study.
Setting Two tertiary care hospitals in Shanghai, China.
Participants Chinese patients (n=542) >65 years of age with estimated glomerular filtration rate ≤15 mL/min/m2 who received urgent-start dialysis between 1 January 2005 and 31 December 2015, and with at least 3 months of treatment. Patients who converted to other dialysis methods, regardless of the initial dialysis method, were excluded, as well as those with comorbidities that could significantly affect their dialysis outcomes.
Primary and secondary outcome measures Dialysis-related complications and survival were compared. Patients were followed until death, stopped PD, transfer to other dialysis centres, loss to follow-up or 31 December 2016.
Results There were 309 patients in the USPD group and 233 in the USHD group. The rate of dialysis-related complications within 30 days after catheter implantation was significantly lower in the USPD group compared with the USHD group (4.5% vs 10.7%, p=0.031). The 6-month and 1, 2 and 3-year survival rates were 95.3%, 91.4%, 86.6% and 64.8% in the USPD group, and 92.2%, 85.7%, 70.2% and 57.8% in the USHD group, respectively (p=0.023). The multivariable Cox regression analysis showed that USHD (HR=2.220, 95% CI 1.298 to 3.790; p=0.004), age (HR=1.025, 95% CI 1.013 to 1.043, p<0.001) and hypokalaemia (HR=0.678, 95% CI 0.487 to 0.970; p=0.032) were independently associated with death.
Conclusions USPD was associated with slightly better survival compared with USHD. USPD was associated with fewer complications and better survival than USHD in elderly patients with ESRD.
- peritoneal dialysis
- prognosis
- elderly
- end-stage renal disease
- haemodialysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Relatively small sample size from only two hospitals.
Retrospective study, with all the inherent biases.
The data were limited to those available from the medical charts.
A strength of this study is the relatively long follow-up.
Introduction
End-stage renal disease (ESRD) is the end stage of chronic kidney disease, which is an important public health problem worldwide with high incidence, poor prognosis, high healthcare costs and high socioeconomic burden.1–10 With the overall ageing of the population, the prevalence of ESRD is on the rise worldwide. Dialysis often needs to be performed urgently in patients with ESRD due to silent disease, low health awareness and late referral.11–14 According to USRDS data reports, in 2010, 43% of the patients had been referred to a nephrologist for the first time at the time of initiating dialysis. Therefore, 30%–50% of patients needing dialysis start the procedure urgently, despite planned dialysis known as an ideal dialysis modality.12
The elderly represents a special population for dialysis. In addition to having the highest prevalence of dialysis among all age groups,15 16 the elderly with ESRD can have dramatic consequences because of frailty, comorbidities and less resistance to health issues, complicating the management of ESRD.17 In addition, the haemodynamic stability of elderly individuals is relatively poor.17 Previous studies showed that using peritoneal dialysis (PD) as the first dialysis method does not increase the risk of short-term complications in elderly patients with ESRD; in addition, the survival rate of the patients is also not evidently affected.18–20
Urgent-start PD (USPD) refers to the initiation of PD treatment within 2 weeks after catheter implantation.21 USPD is commonly applied by physicians in China.22 USPD avoids temporary central venous catheter (CVC) and vascular access surgery in urgent-start haemodialysis (USHD), and thus reduces the risks of USHD and simplifies the treatment processes. The comparison between USPD and USHD has shown that the risks of bacteraemia and death are higher in the patients receiving USHD than in those receiving USPD.23 24 Nevertheless, there is a lack of such comparison for elderly patients.
Therefore, the aim of the present study was to investigate the complications and survival of elderly patients with ESRD who received USPD or USHD and to explore the value of PD as the emergent dialysis method for elderly patients with ESRD.
Patients and methods
Study design and patients
This was a retrospective cohort study of patients >65 years of age who received urgent-start dialysis at the Shanghai Changzheng Hospital and Songjiang District Central Hospital between 1 January 2005 and 31 December 2015.
ESRD was defined as an estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2.15 USPD was defined as PD that started within 2 weeks after catheter implantation. USHD was defined as dialysis that started without the establishment of long-term dialysis access or within 30 days after the establishment of long-term dialysis.
The inclusion criteria were: (1) >65 years of age; (2) eGFR ≤15 mL/min/m2; and (3) received haemodialysis (HD) or PD for ≥3 months. The exclusion criteria were: (1) <65 years of age; (2) died within 3 months of dialysis or lost to follow-up; (3) converted to other dialysis methods, regardless of the initial dialysis method; or (4) combined with severe respiratory diseases, severe acute heart failure, severe hyperkalaemia (serum potassium levels >6.5 mmol/L) or severe acidosis (bicarbonate radical levels <12 mmol/L).
USPD or USHD was selected according to the willingness of the patients and the decision of the physicians at the Nephrology Department according to the condition of the patients (vital signs, cardiac functions and biochemical indexes). The patients were categorised into the USPD and USHD groups.
Dialysis methods
For the patients in the USPD group, a PD catheter was used as access. All catheters were implanted by trained physicians after local anaesthesia (5–10 mL of 1% lidocaine hydrochloride was applied layer by layer). After the catheter was implanted, the time of the dialysis initiation was decided by the physicians according to the clinical manifestations (vital signs, cardiac functions and biochemical indexes). For all patients on PD, a swan-neck straight catheter was implanted, and glucose-based dialysate was used in all patients. All patients in the USPD group received continuous ambulatory PD, four bags/day, 2 L/bag.
For the patients in the HD group, CVC was used as access. All CVCs were implanted into the internal jugular vein or femoral vein by trained physicians. The patients in the USHD group received HD (4 hours/time, volume of blood flow was 250–300 mL/min) or continuous renal replacement treatment (CRRT; 6–8 hours/time, volume of blood flow was 180–300 mL/min).
Data collection
All the included patients were followed until loss to follow-up, death or 31 December 2016. The demographic characteristics (sex, age, primary disease and complications), residual renal function before dialysis and clinical and biochemical indexes of patients were collected. The date of catheter implantation, time of dialysis initiation and dialysis-related complications, including infection-related complications (such as catheter-related infection and peritonitis) and non-infection-related complications (leakage, bleeding, catheter malposition, embolism, catheter obstruction and hernia), were recorded. The outcomes (including death, conversion to HD, kidney transplantation and transferred to other treatment centres), time of the outcomes, causes of the outcomes, time of the first peritonitis, time of peritonitis and the catheter dysfunction events that required surgical interventions or conversion to HD within 3 months after the operation were recorded.
Statistical analysis
SPSS V.19.0 (IBM) was used for statistical analysis. Continuous data with normal distribution are presented as means±SD, while continuous data without normal distribution are described as percentiles (P25, P75). The Mann-Whitney test or the Student’s t-test was used, as appropriate. The Kaplan-Meier method and the log-rank test were used to analyse the survival of the patients. The factors that have been widely acknowledged to affect the survival of the patients, as well as the factors that were significantly different between the two groups at baseline, were entered in a multivariable model (logistic regression and Cox models); the results are presented as OR and 95% CI. P<0.05 was considered statistically significant.
Patient and public involvement
The patients and the public were not involved in the design of this study, in the selection of the outcomes, in the conduct of the study or in result dissemination.
Results
Characteristics of the patients
Finally, 542 patients (283 males and 259 females) were included, 309 in the USPD group and 233 in the USHD group. The mean age of the patients was 73.1±5.6 years. The patients in the USPD accounted for 57% of all the dialysis patients, and the median time from catheter implantation to the start of dialysis was 4 (2−6) days. The patients in the USHD group received dialysis on the day of or the day after catheter implantation. Age, sex and primary diseases were not significantly different between the two groups. The numbers of patients with coronary artery-related events or heart failure (New York Heart Association III, grade IV) were not significantly different between the two groups. The Charlson Comorbidity Index was also not significantly different between the two groups (table 1). The duration of HD was longer than that of PD (24.6±5.2 months vs 22.9±5.1 months, p<0.001). The eGFR, serum calcium levels, serum phosphorus levels, serum intact parathyroid hormone and blood lipid levels before dialysis were not significantly different between the two groups (table 2).
Comparisons of the baseline data
Comparisons of the baseline biochemical indexes
Complications
Compared with the USHD group, the rate of dialysis-related complications within 30 days after catheter implantation was significantly lower in the USPD group (4.5% vs 10.7%, p=0.031). The rates of dialysis-related complications requiring recatheterisation (1.6% vs 9.4%; p<0.001) and bacteraemia (1.2% vs 5.5%; p=0.006) were significantly lower in the USPD group than in the USHD group (table 3). Logistic regression showed that after adjusting for demographic characteristics and baseline data, USHD was an independent risk factor for dialysis-related complications compared with USPD (OR=2.121, 95% CI 1.058 to 4.273, p=0.031).
Complications within 30 days after catheter implantation
Survival
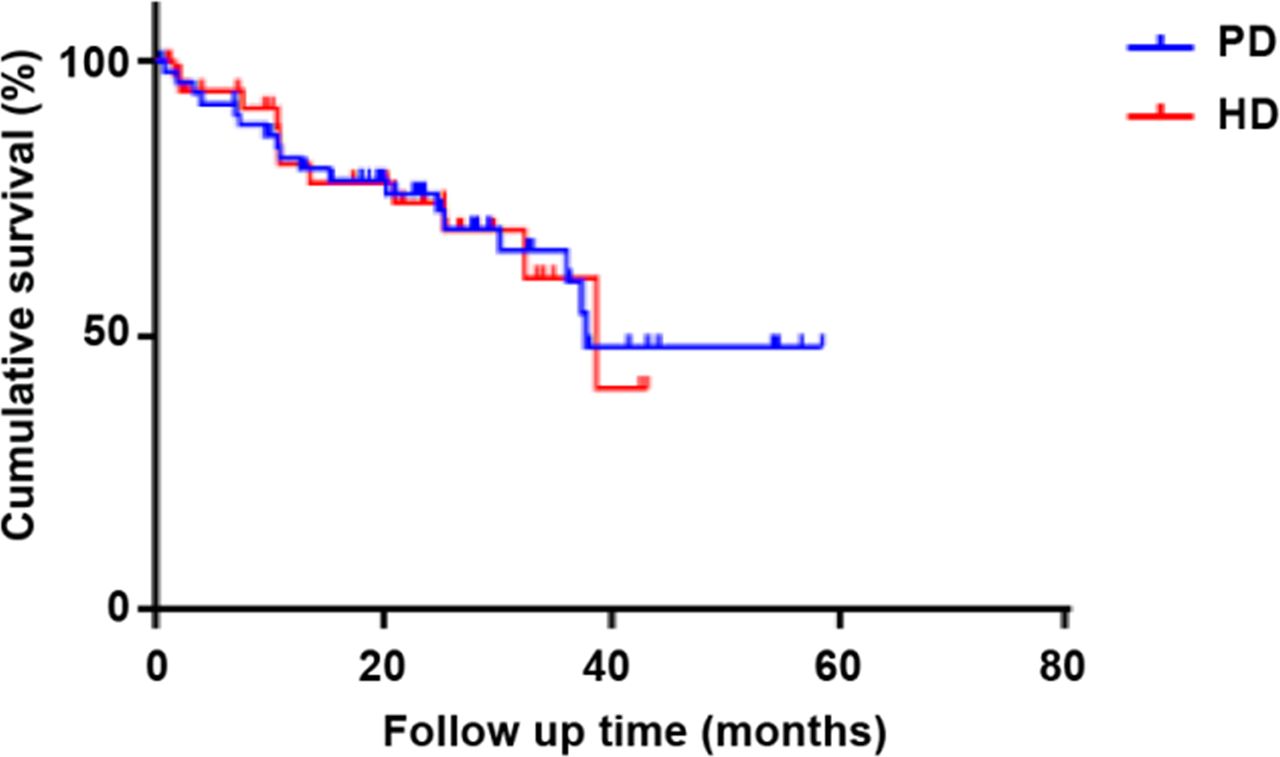
The 6-month and 1, 2 and 3-year survival rates were 95.3%, 91.4%, 86.6% and 64.8% in the USPD group, and 92.2%, 85.7%, 70.2% and 57.8% in the USHD group, respectively (p=0.023) (figure 1). The multivariable Cox regression analysis showed that after adjusting for demographic characteristics and baseline data, USHD was an independent risk factor of death compared with USPD (HR=2.220, 95% CI 1.298 to 3.790; p=0.004). In addition, age (HR=1.025, 95% CI 1.013 to 1.043, p<0.001) and hypokalaemia (HR=0.678, 95% CI 0.487 to 0.970; p=0.032) were also independently associated with death (table 4). A subgroup analysis showed that USHD had a worse prognosis than USPD in elderly patients with diabetes (HR=2.81, 95% CI 1.09 to 7.33, p=0.03) (table 5).
{kind=link}
Survival rates of the patients in the peritoneal dialysis and haemodialysis groups. Kaplan-Meier survival analysis. HD, haemodialysis; PD, peritoneal dialysis.
Multivariable Cox analysis of the independent factors for survival
Multivariable Cox analysis of the independent factors for survival in elderly patients with diabetes
Discussion
Studies suggest that USPD is associated with better patient outcomes than USHD,23 24 but there is a lack of comparison between USPD and USHD for elderly patients with ESRD. Therefore, this study aimed to investigate the complications and survival of elderly patients with ESRD who received USPD or USHD and to explore the value of PD as the emergent dialysis method for elderly patients with ESRD. The results strongly suggest that USPD was associated with slightly better survival compared with USHD. USPD was associated with fewer complications and better survival than USHD in elderly patients with ESRD.
Elderly patients with ESRD have several special features, including delayed initiation of dialysis, more complications, poor nutritional status, cognitive impairment and relatively low quality of life, which could lead to difficulties in the management of ESRD.17 The mortality rate in elderly patients with ESRD is higher than in relatively younger patients receiving dialysis; in addition, the mortality rate is increasing with the increase of age.6 17 A previous study has already reported that the mortality rate increases by about 1.7-fold with every 10 years’ increase of the age in Chinese patients.6 Previous studies have compared the mortality rates of elderly patients on HD or PD, but the results are inconsistent. Collins et al 25 compared the data of patients on HD (n=99 048) and PD (n=18 110), and they observed that the survival of the patients >55 years old was significantly higher among those on PD compared with HD, after stratification for age and diabetes. The data in the 2009 USRDS database showed that after adjusting for age, gender, ethnicity and comorbidities, the 1, 3 and-5 year survival rates of patients on PD were significantly higher than those on HD.26
Several studies have demonstrated that PD could be used for emergent dialysis in patients with ESRD.27–29 Early PD involves high risks of leakage, bleeding and peritonitis within a short time after catheter implantation, which limits the application of PD in emergent dialysis. Nevertheless, the PD techniques have advanced greatly in recent years with the development of the Tenckhoff catheter, closed liquid supply system with Y-type connection, advancement of catheterisation methods and application of automatic PD.30 ,31 Recent studies have shown that PD is safe and applicable as the emergent dialysis for patients with ESRD.32–37
In the present study, the results showed that the occurrence of complications in the USPD group was significantly lower than in the USHD group. After adjustment for demographic characteristics and clinical data, USHD was independently associated with dialysis-related complications, compared with USPD. Using USPD in elderly patients with ESRD could effectively reduce the risk of dialysis-related complications within 2 weeks after catheter implantation. No serious complications such as major bleeding, leakage or organ rupture were found in the PD group, suggesting that the catheter implantation for USPD conducted by trained physicians was probably safe, but additional studies should be performed for confirmation.
Some previous studies showed that compared with USHD, the survival rate of patients on USPD is not significantly different.18 38 Lobbedez et al 18 observed that survival and rehospitalisation rates were not significantly different between USPD and USHD. In the present study, USPD was associated with a slightly better overall survival at 3 years compared with USHD. In addition, the present study showed that USHD had a worse prognosis than USPD in elderly patients with diabetes. More complications within 30 days after catheter implantation in HD than in PD might be a part of the explanation. Previous studies reported conflicting results concerning the mortality of HD versus PD. Indeed, a study showed that mortality was lower for PD than for HD in non-diabetics, men <55 years of age and in diabetics <55 years of age, but higher in diabetic women >55 years of age.25 Lukowsky et al 39 reported that PD led to better survival than HD in those patients, while a number of studies reported no significant survival difference between HD and PD.40–46 On the other hand, a meta-analysis suggested that elderly patients with diabetes might benefit more from HD than PD.47 There is still controversy in this area. Additional studies are necessary to examine this issue, especially since the present study specifically examined USPD and USHD, while those previous studies examined all patients.
This study has limitations. The sample size was relatively small and from only two hospitals. The study was retrospective, with all the inherent biases, and the data were limited to those available in the medical charts. Because of the retrospective nature of the study, and the regulations in China, the exact cause of death can be known only if written in the patient chart. Otherwise, such data might be available on request to the central state database, but access to those data requires special authorisation. As of now, the exact cause of death is missing for most patients. The patients on CRRT were included, but those patients are known to have high mortality rates, probably affecting the results. Furthermore, the usual rate of catheter dysfunction depends on the method of implantation and is usually around 5%–8%.48 We agree that this rate is low, but not so far than that of a study that reported a rate of 5.9% before a continuous quality improvement programme and 1.5% after the programme.49 In our hospitals, even there is no official continuous quality improvement programme, a strict protocol is followed, which could explain the low rate. Finally, as a retrospective study, no causality relationship could be established between the type of dialysis and the outcomes. These limitations might account, at least in part, for the differences observed between the present study and previous ones. Prospective trials could be necessary to determine the exact benefits of USPD versus USHD.
In conclusion, USPD was associated with slightly better survival compared with USHD. USPD was associated with fewer complications and better survival than USHD in elderly patients with ESRD.
References
Footnotes
Contributors XZ, XD, LL and CM carried out the studies, participated in collecting data and drafted the manuscript. LL and CM performed the statistical analysis and participated in its design. All authors read and approved the final manuscript.
Funding This study was supported by the Shanghai Top Priority Key Clinical Disciplines Construction Project (2017ZZ02009; 2017ZZ02009), the National Key Research and Development Program of China (2016YFC0901502), the Shanghai Science and Technology Commission Foundation (15411971200) and the Shanghai Integration of Chinese and Western Medicine Foundation (SH201737).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committees of the Shanghai Changzheng Hospital and Songjiang District Central Hospital (No 2019SL005).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.